
A Personalized Approach to Vitamin D Supplementation in Cardiovascular Health Beyond the Bone: An Expert Consensus by the Italian National Institute for Cardiovascular Research

 , , ,
, , ,  , , , , , ,
, , , , , ,  ,
,  , , ,
, , ,  ,
,  , , , ,
, , , ,
Abstract
1. Introduction
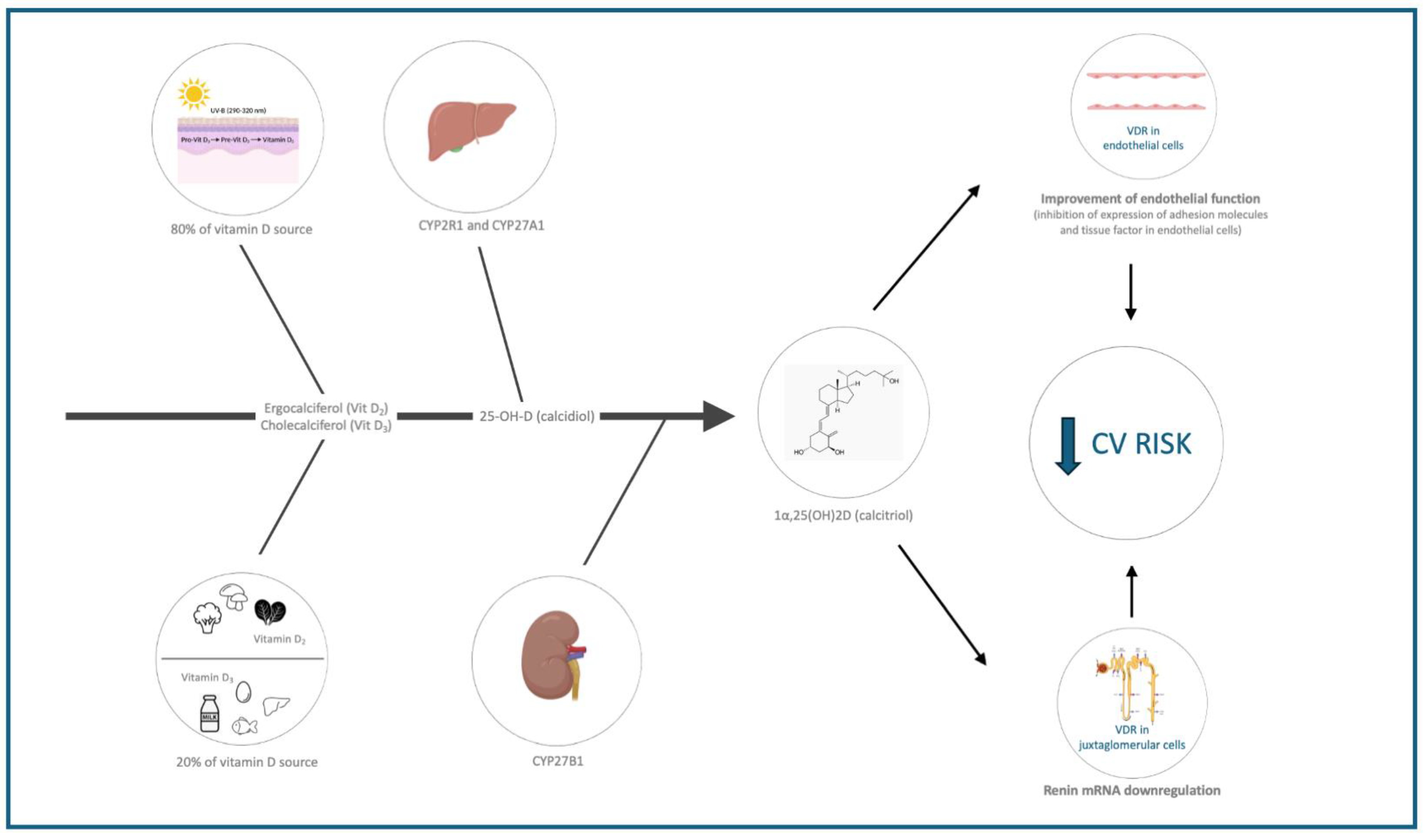
1.1. Vitamin D Synthesis and Function
1.2. Vitamin D as a Hormone

{kind=link}
| Vitamin D Status | Serum 25(OH) D (ng/mL) In the General Population | Serum 25(OH)D (ng/mL) In Population at Risk (Including Patients at High Cardiovascular Risk) |
|---|---|---|
| Deficiency | <10 | <10 |
| Moderate deficiency | <20 | <30 |
| Optimal | 20–50 | 30–50 |
1.2.1. Endothelial and Vascular Smooth Muscle Cell Function and Inflammation
1.2.2. Cardiac Cells
1.2.3. Renin–Angiotensin–Aldosterone System (RAAS)
1.2.4. Lipid Metabolism
1.2.5. Glucose Metabolism
2. Observational and Interventional Insights into Vitamin D and Cardiovascular Health
2.1. Cohort and Cross-Sectional Studies, Observational Studies
2.2. Interventional Studies and Randomized Controlled Trials (RCTs)
2.2.1. Interventional Studies
2.2.2. Randomized Controlled Trials (RCTs)
2.3. Meta-Analyses and Systematic Reviews
3. Potential Reasons for Inconsistent Findings
3.1. Baseline Vitamin D Status
3.1.1. Threshold Effects
3.1.2. Greater Potential for Correction
3.1.3. Biological Compensation
3.2. Dosage and Duration
3.3. Heterogeneity of Populations Included in Studies
3.3.1. Age
3.3.2. Sex
3.3.3. Physical Activity
3.3.4. Diabetes
3.3.5. Hypertension
3.3.6. Frailty
3.3.7. Possible Interactions of Vitamin D with Other Factors
3.4. Endpoints
3.5. Clinical Implications and Future Directions
- Stratification: To accurately assess the effects of vitamin D supplementation, it is essential to stratify participants based on age, sex, baseline vitamin D levels, health status, and comorbidities. This allows for a clearer understanding of how different subgroups respond to supplementation.
- Customized Dosing: Different populations may require different dosages of vitamin D. For example, older adults or those with severe deficiency might need higher doses compared to younger, healthier individuals.
- Outcome Measures: Selecting appropriate outcome measures that reflect the specific benefits relevant to different subgroups is crucial. For instance, bone density measures might be more relevant for older women, while immune function might be a key outcome for individuals with autoimmune conditions.
- Generalizability: Understanding how population differences affect study outcomes helps in generalizing the findings to broader populations. Without considering these factors, the study’s applicability to diverse groups is limited.
- Dual Measurement Approach: For patients with CVD, especially those with comorbid conditions, such as CKD, diabetes, or metabolic syndrome, measuring both 25(OH)D and 1,25(OH)2D could help tailor treatment more precisely. This dual approach can reveal discrepancies between stored and active vitamin D, allowing for better-informed therapeutic interventions.
- 1.
- Assessment of Vitamin D Levels in Cardiovascular Patients.
- 2.
- Vitamin D Deficiency and Cardiovascular Risk.
- 3.
- Hypertension Management
- 4.
- Prediabetes and Diabetes and Cardiovascular Risk
- 5.
- Obesity and Cardiovascular Risk
- 6.
- Heart Failure and Vitamin D
- 7.
- Frail Patients and Rehabilitation
4. Adverse Effects of Vitamin D Overdosing
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cosentino, N.; Campodonico, J.; Milazzo, V.; De Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.E.; Powell, J.T. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; März, W.; Pilz, S. Vitamin D and Cardiovascular Disease: An Updated Narrative Review. Int. J. Mol. Sci. 2021, 22, 2896. [Google Scholar] [CrossRef]
- Dirks, N.F.; Cavalier, E.; Heijboer, A.C. Vitamin D: Marker, measurand & measurement. Endocr. Connect. 2023, 12, e220269. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Christakos, S.; Li, S.; De La Cruz, J.; Bikle, D.D. New developments in our understanding of vitamin D metabolism, action and treatment. Metab. Clin. Exp. 2019, 98, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Demay, M.B.; Pittas, A.G.; Bikle, D.D.; Diab, D.L.; E Kiely, M.; Lazaretti-Castro, M.; Lips, P.; Mitchell, D.M.; Murad, M.H.; Powers, S.; et al. Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2024, 109, 1907–1947. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Meyer, M.B. Fundamentals of vitamin D hormone-regulated gene expression. J. Steroid Biochem. Mol. Biol. 2014, 144 (Pt A), 5–11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Żmijewski, M.A. Nongenomic Activities of Vitamin D. Nutrients 2022, 14, 5104. [Google Scholar] [CrossRef]
- IGreiller, C.L.; Martineau, A.R. Modulation of the immune response to respiratory viruses by vitamin D. Nutrients 2015, 7, 4240–4270. [Google Scholar] [CrossRef] [PubMed]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef]
- Zanini, G.; Selleri, V.; Roncati, L.; Coppi, F.; Nasi, M.; Farinetti, A.; Manenti, A.; Pinti, M.; Mattioli, A.V. Vascular “Long COVID”: A New Vessel Disease? Angiology 2023, 18, 33197231153204. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zanini, G.; Selleri, V.; Domenech, S.L.; Malerba, M.; Nasi, M.; Mattioli, A.V.; Pinti, M. Mitochondrial DNA as inflammatory DAMP: A warning of an aging immune system? Biochem. Soc. Trans. 2023, 51, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Uberti, F.; Lattuada, D.; Morsanuto, V.; Nava, U.; Bolis, G.; Vacca, G.; Squarzanti, D.F.; Cisari, C.; Molinari, C. Vitamin D protects human endothelial cells from oxidative stress through the autophagic and survival pathways. J. Clin. Endocrinol. Metab. 2014, 99, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Coronelli, M.M.; Coppi, F.; Mattioli, A.V. Inflammation, atherosclerosis and hypertension: The impact of depression and stress on their complex relationship. Futur. Cardiol. 2024, 20, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Bertoldo, F.; Cianferotti, L.; Di Monaco, M.; Falchetti, A.; Fassio, A.; Gatti, D.; Gennari, L.; Giannini, S.; Girasole, G.; Gonnelli, S.; et al. Definition, Assessment, and Management of Vitamin D Inadequacy: Suggestions, Recommendations, and Warnings from the Italian Society for Osteoporosis, Mineral Metabolism and Bone Diseases (SIOMMMS). Nutrients 2022, 14, 4148. [Google Scholar] [CrossRef]
- Janubová, M.; Žitňanová, I. The effects of vitamin D on different types of cells. Steroids 2024, 202, 109350. [Google Scholar] [CrossRef] [PubMed]
- D’ascenzi, F.; Sciaccaluga, C.; Cameli, M.; Cecere, A.; Ciccone, M.M.; Di Francesco, S.; Ganau, A.; Imbalzano, E.; Liga, R.; Palermo, P.; et al. When should cardiovascular prevention begin? The importance of antenatal, perinatal and primordial prevention. Eur. J. Prev. Cardiol. 2021, 28, 361–369. [Google Scholar] [CrossRef]
- Molinari, C.; Rizzi, M.; Squarzanti, D.F.; Pittarella, P.; Vacca, G.; Renò, F. 1α,25-Dihydroxycholecalciferol (Vitamin D3) induces NO-dependent endothelial cell proliferation and migration in a three-dimensional matrix. Cell. Physiol. Biochem. 2013, 31, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Pittarella, P.; Squarzanti, D.F.; Molinari, C.; Invernizzi, M.; Uberti, F.; Renò, F. NO-dependent proliferation and migration induced by Vitamin D in HUVEC. J. Steroid Biochem. Mol. Biol. 2015, 149, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Laera, N.; Malerba, P.; Vacanti, G.; Nardin, S.; Pagnesi, M.; Nardin, M. Impact of Immunity on Coronary Artery Disease: An Updated Pathogenic Interplay and Potential Therapeutic Strategies. Life 2023, 13, 2128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, Y.; Lyons, C.J.; Ayu, C.; O’brien, T. Recent advances in endothelial colony-forming cells: From the transcriptomic perspective. J. Transl. Med. 2024, 22, 313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tukaj, S.; Trzonkowski, P.; Tukaj, C. Regulatory effects of 1,25-dihydroxyvitamin D3 on vascular smooth muscle cells. Acta Biochim. Pol. 2012, 59, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Law, C.S.; Grigsby, C.L.; Olsen, K.; Gardner, D.G. A role for the cell cycle phosphatase Cdc25a in vitamin D-dependent inhibition of adult rat vascular smooth muscle cell proliferation. J. Steroid Biochem. Mol. Biol. 2010, 122, 326–332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Molinuevo, M.S.; Fernández, J.M.; Cortizo, A.M.; McCarthy, A.D.; Schurman, L.; Sedlinsky, C. Advanced glycation end products and strontium ranelate promote osteogenic differentiation of vascular smooth muscle cells in vitro: Preventive role of vitamin D. Mol. Cell. Endocrinol. 2017, 450, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Valcheva, P.; Cardus, A.; Panizo, S.; Parisi, E.; Bozic, M.; Novoa, J.M.L.; Dusso, A.; Fernández, E.; Valdivielso, J.M. Lack of vitamin D receptor causes stress-induced premature senescence in vascular smooth muscle cells through enhanced local angiotensin-II signals. Atherosclerosis 2014, 235, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Lin, H.; Liu, J.; Wang, D.; Li, D.; Jiang, C.; Tang, Y.; Wang, J.; Zhang, T.; Li, Y.; et al. 1,25-Dihydroxyvitamin D attenuates diabetic cardiac autophagy and damage by vitamin D receptor-mediated suppression of FoxO1 translocation. J. Nutr. Biochem. 2020, 80, 108380. [Google Scholar] [CrossRef] [PubMed]
- Jahanifar, F.; Astani, A.; Shekarforoosh, S.; Jamhiri, M.; Safari, F.; Zarei, F.; Safari, F. 1.25 Dihydroxyvitamin D3 Attenuates Hypertrophy Markers in Cardiomyoblast H9c2 Cells: Evaluation of Sirtuin3 mRNA and Protein Level. Int. J. Vitam. Nutr. Res. 2019, 89, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Pacini, S.; Morucci, G.; Branca, J.J.V.; Aterini, S.; Amato, M.; Gulisano, M.; Ruggiero, M. Effects of Vitamin D3 and Paricalcitol on immature cardiomyocytes: A novel role for vitamin D analogs in the prevention of cardiovascular diseases. Nutrients 2013, 5, 2076–2092. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mansournia, M.A.; Ostadmohammadi, V.; Doosti-Irani, A.; Ghayour-Mobarhan, M.; Ferns, G.; Akbari, H.; Ghaderi, A.; Talari, H.R.; Asemi, Z. The Effects of Vitamin D Supplementation on Biomarkers of Inflammation and Oxidative Stress in Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm. Metab. Res. 2018, 50, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Moslemi, E.; Musazadeh, V.; Kavyani, Z.; Naghsh, N.; Shoura, S.M.S.; Dehghan, P. Efficacy of vitamin D supplementation as an adjunct therapy for improving inflammatory and oxidative stress biomarkers: An umbrella meta-analysis. Pharmacol. Res. 2022, 186, 106484. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Viglione, F.; Boggio, A.; Stefani, D.; Panarotto, N.; Malabaila, A.; Rolla, R.; Soldà, P.L.; Stecco, A.; Carriero, A.; et al. Relationship between vitamin D and cholesterol levels in STEMI patients undergoing primary percutaneous coronary intervention. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Legarth, C.; Grimm, D.; Wehland, M.; Bauer, J.; Krüger, M. The Impact of Vitamin D in the Treatment of Essential Hypertension. Int. J. Mol. Sci. 2018, 19, 455. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cameli, M.; Lembo, M.; Sciaccaluga, C.; Bandera, F.; Ciccone, M.M.; D’andrea, A.; D’ascenzi, F.; Esposito, R.; Evola, V.; Liga, R.; et al. Identification of cardiac organ damage in arterial hypertension: Insights by echocardiography for a comprehensive assessment. J. Hypertens. 2020, 38, 588–598. [Google Scholar] [CrossRef] [PubMed]
- Pastore, M.C.; Cavigli, L.; Olivoni, G.; Morrone, F.; Amati, F.; Imbalzano, E.; Rinaldi, A.; Liga, R.; Mattioli, A.V.; Scicchitano, P.; et al. Physical exercise in hypertensive heart disease: From the differential diagnosis to the complementary role of exercise. Int. J. Cardiol. 2024, 410, 132232. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Xu, X.-J.; Zhang, J.-S.; Liu, H.-M. Association between Vitamin D Deficiency and Levels of Renin and Angiotensin in Essential Hypertension. Int. J. Clin. Pract. 2022, 2022, 8975396. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nardin, M.; Verdoia, M.; Nardin, S.; Cao, D.; Chiarito, M.; Kedhi, E.; Galasso, G.; Condorelli, G.; De Luca, G. Vitamin D and Cardiovascular Diseases: From Physiology to Pathophysiology and Outcomes. Biomedicines 2024, 12, 768. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Khanolkar, S.; Hirani, S.; Mishra, A.; Vardhan, S.; Hirani, S.; Prasad, R.; Wanjari, M. Exploring the Role of Vitamin D in Atherosclerosis and Its Impact on Cardiovascular Events: A Comprehensive Review. Cureus 2023, 15, e42470. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, Y.; Li, X.; Wang, M.; Ning, H.; A, L.; Li, Y.; Sun, C. Lipoprotein lipase links vitamin D, insulin resistance, and type 2 diabetes: A cross-sectional epidemiological study. Cardiovasc. Diabetol. 2013, 12, 17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Inomata, S.; Kadowaki, S.; Yamatani, T.; Fukase, M.; Fujita, T. Effect of 1 alpha (OH)-vitamin D3 on insulin secretion in diabetes mellitus. Bone Miner. 1986, 1, 187–192. [Google Scholar] [PubMed]
- Maestro, B.; Dávila, N.; Carranza, M.; Calle, C. Identification of a Vitamin D response element in the human insulin receptor gene promoter. J. Steroid Biochem. Mol. Biol. 2003, 84, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Atkins, A.; Downes, M.; Wei, Z. Vitamin D in Diabetes: Uncovering the Sunshine Hormone’s Role in Glucose Metabolism and Beyond. Nutrients 2023, 15, 1997. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeitz, U.; Weber, K.; Soegiarto, D.W.; Wolf, E.; Balling, R.; Erben, R.G. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB J. 2003, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wolden-Kirk, H.; Overbergh, L.; Gysemans, C.; Brusgaard, K.; Naamane, N.; Van Lommel, L.; Schuit, F.; Eizirik, D.; Christesen, H.; Mathieu, C. Unraveling the effects of 1,25OH2D3 on global gene expression in pancreatic islets. J. Steroid Biochem. Mol. Biol. 2013, 136, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Sergeev, I.N.; Rhoten, W.B. 1,25-Dihydroxyvitamin D3 evokes oscillations of intracellular calcium in a pancreatic beta-cell line. Endocrinology 1995, 136, 2852–2861. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Grant, W.B.; Della Casa, S.; Orio, F.; Pontecorvi, A.; Colao, A.; Sarno, G.; Muscogiuri, G. Vitamin D and pancreas: The role of sunshine vitamin in the pathogenesis of diabetes mellitus and pancreatic cancer. Crit. Rev. Food Sci. Nutr. 2017, 57, 3472–3488. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Grande, J.P.; Roche, P.C.; Kumar, R. Immunohistochemical localization of the 1,25(OH)2D3 receptor and calbindin D28k in human and rat pancreas. Am. J. Physiol. Metab. 1994, 267 Pt 1, E356–E360. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Qiu, S.; Wang, Z.; Hu, Y. Vitamin D levels and five cardiovascular diseases: A Mendelian randomization study. Heliyon 2023, 10, e23674. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hung, M.; Hung, M.; Birmingham, W.C.; Birmingham, W.C.; Ocampo, M.; Ocampo, M.; Mohajeri, A.; Mohajeri, A. The Role of Vitamin D in Cardiovascular Diseases. Nutrients 2023, 15, 3547. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, X.; Chen, X.; Liu, S.; Deng, Y.; Wang, Y.; Lu, Q.; Li, R.; Ou, Y.; Tian, Q.; Liao, Y.; et al. Associations of Serum 25(OH)D With Risk of Recurrent Cardiovascular Events in Individuals With Coronary Heart Disease. J. Clin. Endocrinol. Metab. 2023, 108, e1712–e1719. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Chen, J.; Shi, Y.; Hou, L. Association between serum 25(OH)D and risk of all-cause mortality in adults with prior cardiovascular disease: A cohort study from NHANES 2007–2018. BMC Cardiovasc. Disord. 2023, 23, 240. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, Y.; Jiang, M.; Sun, J.-Y.; Cheng, C.; Shen, H.; Sun, W.; Kong, X.-Q. The Association Between Vitamin D Levels and the 10-Year Risk of Atherosclerotic Cardiovascular Disease: A Population-Based Study. J. Cardiovasc. Nurs. 2022, 38, E178–E186. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Dong, Y.; Naugler, C.T.; de Koning, L. Serum 25-hydroxyvitamin D, cardiovascular risk markers, and incident cardiovascular disease in a high risk community population. Clin. Biochem. 2021, 93, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Soh, V.; Tan, S.J.X.; Sehgal, R.; Shirke, M.M.; Ashry, A.; Harky, A. The Relationship Between Vitamin D Status and Cardiovascular Diseases. Curr. Probl. Cardiol. 2021, 46, 100836. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the Third National Health and Nutrition Examination Survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Michos, E.D.; Post, W.; Astor, B. Astor B. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch. Intern. Med. 2008, 168, 1629–1637. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Desouza, C.; Chatterjee, R.; Vickery, E.M.; Nelson, J.; Johnson, K.C.; Kashyap, S.R.; Lewis, M.R.; Margolis, K.; Pratley, R.; Rasouli, N.; et al. The effect of vitamin D supplementation on cardiovascular risk in patients with prediabetes: A secondary analysis of the D2d study. J. Diabetes Its Complicat. 2022, 36, 108230. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Adams, F.; McSwiggan, S.; Kennedy, G.; Kabir, G.; Belch, J.; Khan, F. Effect of intermittent vitamin D3 on vascular function and symptoms in chronic fatigue syndrome—A randomised controlled trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Witte, K.K.; Byrom, R.; Gierula, J.; Paton, M.F.; Jamil, H.A.; Lowry, J.E.; Gillott, R.G.; Barnes, S.A.; Chumun, H.; Kearney, L.C.; et al. Effects of Vitamin D on Cardiac Function in Patients With Chronic HF: The VINDICATE Study. J Am Coll Cardiol. 2016, 67, 2593–2603. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Manson, J.E.; Bassuk, S.S.; Buring, J.E.; VITAL Research Group. Principal results of the VITamin D and OmegA-3 TriaL (VITAL) and updated meta-analyses of relevant vitamin D trials. J. Steroid Biochem. Mol. Biol. 2020, 198, 105522. [Google Scholar] [CrossRef]
- Scragg, R. The Vitamin D Assessment (ViDA) study—Design and main findings. J. Steroid Biochem. Mol. Biol. 2020, 198, 105562. [Google Scholar] [CrossRef] [PubMed]
- Sluyter, J.D.; Camargo, C.A.; Stewart, A.W.; Waayer, D.; Lawes, C.M.M.; Toop, L.; Khaw, K.; Thom, S.A.M.; Hametner, B.; Wassertheurer, S.; et al. Effect of Monthly, High-Dose, Long-Term Vitamin D Supplementation on Central Blood Pressure Parameters: A Randomized Controlled Trial Substudy. J. Am. Heart Assoc. 2017, 6, e006802. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Prentice, R.L.; Pettinger, M.B.; Jackson, R.D.; Wactawski-Wende, J.; LaCroix, A.Z.; Anderson, G.L.; Chlebowski, R.T.; Manson, J.E.; Van Horn, L.; Vitolins, M.Z.; et al. Health risks and benefits from calcium and vitamin D supplementation: Women’s Health Initiative clinical trial and cohort study. Osteoporos. Int. 2013, 24, 567–580. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thadhani, R.; Appelbaum, E.; Pritchett, Y.; Chang, Y.; Wenger, J.; Tamez, H.; Bhan, I.; Agarwal, R.; Zoccali, C.; Wanner, C.; et al. Vitamin D Therapy and Cardiac Structure and Function in Patients With Chronic Kidney Disease: The PRIMO Randomized Controlled Trial. JAMA 2012, 307, 674–684. [Google Scholar] [CrossRef]
- Parker, J.; Hashmi, O.; Dutton, D.; Mavrodaris, A.; Stranges, S.; Kandala, N.-B.; Clarke, A.; Franco, O.H. Levels of vitamin D and cardiometabolic disorders: Systematic review and meta-analysis. Maturitas 2010, 65, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Ball, D.; Gellert, C.; Brenner, H. Serum 25-hydroxyvitamin D levels and overall mortality. A systematic review and meta-analysis of prospective cohort studies. Ageing Res. Rev. 2013, 12, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Iodice, S.; Pilz, S.; Grant, W.B.; Bagnardi, V.; Gandini, S. Vitamin D deficiency and mortality risk in the general population: A meta-analysis of prospective cohort studies. Am. J. Clin. Nutr. 2012, 95, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Gaksch, M.; Jorde, R.; Grimnes, G.; Joakimsen, R.; Schirmer, H.; Wilsgaard, T.; Mathiesen, E.B.; Njølstad, I.; Løchen, M.-L.; März, W.; et al. Vitamin D and mortality: Individual participant data meta-analysis of standardized 25-hydroxyvitamin D in 26916 individuals from a European consortium. PLoS ONE 2017, 12, e0170791. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2014, 2014, CD007470. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83 000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776, Erratum in JAMA Cardiol. 2020, 5, 112. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pei, Y.-Y.; Zhang, Y.; Peng, X.-C.; Liu, Z.-R.; Xu, P.; Fang, F. Association of Vitamin D Supplementation with Cardiovascular Events: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rasouli, M.A.; Darvishzadehdaledari, S.; Alizadeh, Z.; Moradi, G.; Gholami, F.; Mahmoudian, A. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 134000 Individuals in 29 Randomized Clinical Trials and 157000 Individuals in 30 Prospective Cohort Studies: An Updated Systematic Review and Meta-analysis. J. Res. Health Sci. 2023, 23, e00594. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sousa, P.V.d.L.; Nascimento, L.M.; de Oliveira, A.F.M.; dos Santos, G.M.; Moura, A.R.d.S.; Primo, M.G.S.; Paiva, A.d.A.; Freitas, B.d.J.e.S.d.A.; de Carvalho, C.M.R.G.; Martins, M.D.C.d.C.e.; et al. Effects of Vitamin D Levels on Cardiovascular Diseases: A Systematic Review. Curr. Nutr. Food Sci. 2022, 18, 642–648. [Google Scholar] [CrossRef]
- de la Guía-Galipienso, F.; Martínez-Ferran, M.; Vallecillo, N.; Lavie, C.J.; Sanchis-Gomar, F.; Pareja-Galeano, H. Vitamin D and cardiovascular health. Clin. Nutr. 2020, 40, 2946–2957. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ostadmohammadi, V.; Milajerdi, A.; Ghayour-Mobarhan, M.; Ferns, G.; Taghizadeh, M.; Badehnoosh, B.; Mirzaei, H.; Asemi, Z. The Effects of Vitamin D Supplementation on Glycemic Control, Lipid Profiles and C-Reactive Protein Among Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr. Pharm. Des. 2019, 25, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Rai, V.; Agrawal, D.K. Role of Vitamin D in Cardiovascular Diseases. Endocrinol. Metab. Clin. N. Am. 2017, 46, 1039–1059. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luo, W.; Xu, D.; Zhang, J.; Zhou, Y.; Yang, Q.; Lv, Q.; Qu, Z. Low serum 25-hydroxyvitamin D levels are associated with increased cardiovascular morbidity and mortality. Postgrad. Med. 2023, 135, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Kunutsor, S.; Vitezova, A.; Oliver-Williams, C.; Chowdhury, S.; Kiefte-De-Jong, J.C.; Khan, H.; Baena, C.P.; Prabhakaran, D.; Hoshen, M.B.; et al. Vitamin D and risk of cause specific death: Systematic review and meta-analysis of observational cohort and randomised intervention studies. BMJ 2014, 348, g1903. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kuwabara, A.; Tsugawa, N.; Mizuno, K.; Ogasawara, H.; Watanabe, Y.; Tanaka, K. A simple questionnaire for the prediction of vitamin D deficiency in Japanese adults (Vitaimn D Deficiency questionnaire for Japanese: VDDQ-J). J. Bone Miner. Metab. 2019, 37, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Sohl, E.; Heymans, M.W.; de Jongh, R.T.; Heijer, M.D.; Visser, M.; Merlijn, T.; Lips, P.; van Schoor, N.M. Prediction of vitamin D deficiency by simple patient characteristics. Am. J. Clin. Nutr. 2014, 99, 1089–1095. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Khazai, N.; Judd, S.E.; Tangpricha, V. Calcium and vitamin D: Skeletal and extraskeletal health. Curr. Rheumatol. Rep. 2008, 10, 110–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bishop, E.L.; Ismailova, A.; Dimeloe, S.K.; Hewison, M.; White, J.H. Vitamin D and immune regulation: Antibacterial, antiviral, anti-inflammatory. JBMR Plus 2020, 5, e10405. [Google Scholar] [CrossRef]
- Chiu, S.-K.; Tsai, K.-W.; Wu, C.-C.; Zheng, C.-M.; Yang, C.-H.; Hu, W.-C.; Hou, Y.-C.; Lu, K.-C.; Chao, Y.-C. Putative Role of Vitamin D for COVID-19 Vaccination. Int. J. Mol. Sci. 2021, 22, 8988. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mattioli, A.V.; Coppi, F.; Nasi, M.; Gallina, S. Stress and cardiovascular risk burden after the pandemic: Current status and future prospects. Expert Rev. Cardiovasc. Ther. 2022, 20, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Dobnig, H.; Pilz, S.; Scharnagl, H.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Kinkeldei, J.; Boehm, B.O.; Weihrauch, G.; Maerz, W. Independent association of low serum 25-hydroxyvitamin d and 1,25-dihydroxyvitamin d levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 2008, 168, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Wang, J.; Gu, L.; Wang, L.; Yuan, W. Vitamin D supplements in chronic kidney disease. Ren. Fail. 2015, 37, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Selleri, V.; Zanini, G.; Nasi, M.; Pinti, M.; Stefanelli, C.; Fedele, F.; Gallina, S. Physical Activity and Diet in Older Women: A Narrative Review. J. Clin. Med. 2023, 12, 81. [Google Scholar] [CrossRef]
- Shi, J.-W.; Wu, J.-N.; Zhu, X.-Y.; Zhou, W.-H.; Yang, J.-Y.; Li, M.-Q. Association of serum 25-hydroxyvitamin D levels with all-cause and cause-specific mortality among postmenopausal females: Results from NHANES. J. Transl. Med. 2023, 21, 629. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Moscucci, F.; Sciomer, S.; Maffei, S.; Nasi, M.; Pinti, M.; Bucciarelli, V.; Cas, A.D.; Parati, G.; Ciccone, M.M.; et al. Cardiovascular prevention in women: Un update By the Italian Society of Cardiology Working Group On “Prevention, Hypertension and peripheral disease”. J. Cardiovasc. Med. 2023, 24, e147–e155. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Control Policy Contributors. Position Statement-Risks and Benefits of Sun Exposure, National Cancer Control Policy. Available online: https://www.assc.org.au/wp-content/uploads/2023/01/Sun-Exposure-Summit-PositionStatement_V1.9.pdf (accessed on 28 December 2024).
- Fernandes, M.R.; Junior, W.d.R.B. Association between physical activity and vitamin D: A narrative literature review. Front. Public Health 2017, 63, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.T.; Ebeling, M.; Shary, J.R.; Forestieri, N.; Wagner, C.L. The relationship between physical activity and vitamin D status in postpartum lactating and formula-feeding women. J. Steroid Biochem. Mol. Biol. 2018, 177, 261–265. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farrell, S.W.; Meyer, K.J.; Leonard, D.; Shuval, K.; Barlow, C.E.; Pavlovic, A.; DeFina, L.; Haskell, W.L. Physical Activity, Adiposity, and Serum Vitamin D Levels in Healthy Women: The Cooper Center Longitudinal Study. J. Women’s Health 2022, 31, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Prusik, K.; Kortas, J.; Prusik, K.; Mieszkowski, J.; Jaworska, J.; Skrobot, W.; Lipinski, M.; Ziemann, E.; Antosiewicz, J. Nordic Walking Training Causes a Decrease in Blood Cholesterol in Elderly Women Supplemented with Vitamin D. Front. Endocrinol. 2018, 9, 42. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Irandoust, K.; Taheri, M. The Effect of Vitamin D supplement and Indoor Vs Outdoor Physical Activity on Depression of Obese Depressed Women. Asian J. Sports Med. 2017, 8, e13311. [Google Scholar] [CrossRef]
- Khan, S.; Claeson, M.; Khan, A.; Neale, R. The effect of physical activity on vitamin D: A systematic review and meta-analysis of intervention studies in humans. Public Health Pract. 2024, 7, 100495. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, J.; Cao, Z.-B. Exercise: A Possibly Effective Way to Improve Vitamin D Nutritional Status. Nutrients 2022, 14, 2652. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bucciarelli, V.; Mattioli, A.V.; Sciomer, S.; Moscucci, F.; Renda, G.; Gallina, S. The Impact of Physical Activity and Inactivity on Cardiovascular Risk across Women’s Lifespan: An Updated Review. J. Clin. Med. 2023, 12, 4347. [Google Scholar] [CrossRef]
- Da Silva, A.C.M.; Cureau, F.V.; De Oliveira, C.L.; Giannini, D.T.; Bloch, K.V.; Kuschnir, M.C.C.; Dutra, E.S.; Schaan, B.D.; de Carvalho, K.M.B. Physical activity but not sedentary time is associated with vitamin D status in adolescents: Study of cardiovascular risk in adolescents (ERICA). Eur. J. Clin. Nutr. 2018, 73, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Orces, C.H. Association between leisure-time aerobic physical activity and vitamin D concentrations among US older adults: The NHANES 2007–2012. Aging Clin. Exp. Res. 2019, 31, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Ceolin, G.; Confortin, S.C.; da Silva, A.A.M.; Rech, C.R.; D’Orsi, E.; Rieger, D.K.; Moreira, J.D. Association between physical activity and vitamin D is partially mediated by adiposity in older adults: EpiFloripa Aging Cohort Study. Nutr. Res. 2022, 103, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Farag, H.A.M.; Hosseinzadeh-Attar, M.J.; Muhammad, B.A.; Esmaillzadeh, A.; el Bilbeisi, A.H. Effects of vitamin D supplementation along with endurance physical activity on lipid profile in metabolic syndrome patients: A randomized controlled trial. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Stankiewicz, B.; Mieszkowski, J.; Kochanowicz, A.; Brzezińska, P.; Niespodziński, B.; Kowalik, T.; Waldziński, T.; Kowalski, K.; Borkowska, A.; Reczkowicz, J.; et al. Effect of Single High-Dose Vitamin D3 Supplementation on Post-Ultra Mountain Running Heart Damage and Iron Metabolism Changes: A Double-Blind Randomized Controlled Trial. Nutrients 2024, 16, 2479. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Klausen, T.; Breum, L.; Sørensen, H.A.; Schifter, S.; Sonne, B. Plasma levels of parathyroid hormone, vitamin D, calcitonin, and calcium in association with endurance exercise. Calcif. Tissue Int. 1993, 52, 205–208. [Google Scholar] [CrossRef]
- Sun, X.; Cao, Z.-B.; Tanisawa, K.; Taniguchi, H.; Kubo, T.; Higuchi, M. Effects of chronic endurance exercise training on serum 25(OH)D concentrations in elderly Japanese men. Endocrine 2018, 59, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Malandish, A.; Tartibian, B.; Sheikhlou, Z.; Afsargharehbagh, R.; Rahmati, M. The effects of short-term moderate intensity aerobic exercise and long-term detraining on electrocardiogram indices and cardiac biomarkers in postmenopausal women. J. Electrocardiol. 2020, 60, 15–22. [Google Scholar] [CrossRef]
- Mudjanarko, S.W.; Irawati, A.; Tinduh, D. Effects of aerobic exercise on adiponectin levels potentially mediated by vitamin D in type 2 diabetic patients. Endocr. Regul. 2022, 56, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Podsiadło, S.; Skiba, A.; Kałuża, A.; Ptaszek, B.; Stożek, J.; Skiba, A.; Marchewka, A. Influence of Nordic Walking Training on Vitamin D Level in the Blood and Quality of Life among Women Aged 65–74. Healthcare 2021, 9, 1146. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Skalska, M.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.J.; Radzimiński; Jastrzębska, J.; Kaczmarczyk, M.; Myśliwiec, A.; Dragos, P.; López-Sánchez, G.F.; et al. Vitamin D Supplementation and Physical Activity of Young Soccer Players during High-Intensity Training. Nutrients 2019, 11, 349. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rahimpour, Z.; Hoseini, R.; Behpour, N. Alterations of liver enzymes and lipid profile in response to exhaustive eccentric exercise: Vitamin D supplementation trial in overweight females with non-alcoholic fatty liver disease. BMC Gastroenterol. 2022, 22, 372. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ghasemi, E.; Nayebifar, S. Benefits of 10 weeks of high-intensity interval training and green tea supplementation on cardiovascular risk factors and VO2max in overweight women. J. Res. Med. Sci. 2019, 24, 79. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aschauer, R.; Unterberger, S.; Zöhrer, P.A.; Draxler, A.; Franzke, B.; Strasser, E.-M.; Wagner, K.-H.; Wessner, B. Effects of vitamin D3 supplementation and resistance training on 25-hydroxyvitamin D status and functional performance of older adults: A randomized placebo-controlled trial. Nutrients 2021, 14, 86. [Google Scholar] [CrossRef]
- Timpmann, S.; Rips, L.; Olveti, I.; Mooses, M.; Mölder, H.; Varblane, A.; Lille, H.-R.; Gapeyeva, H.; Ööpik, V. Seasonal Variation in Vitamin D Status Does Not Interfere with Improvements in Aerobic and Muscular Endurance in Conscripts during Basic Military Training. Nutrients 2024, 16, 1306. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, C.; Coppi, F.; Farinetti, A.; Mattioli, A.V. Cardiovascular disease prevention and therapy in women with Type 2 diabetes. Future Cardiol. 2021, 17, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Vijay, G.S.; Ghonge, S.; Vajjala, S.M.; Palal, D. Prevalence of Vitamin D Deficiency in Type 2 Diabetes Mellitus Patients: A Cross-Sectional Study. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2023, 15, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Marrone, E.; Di Palermo, C.; Iommi, C.; Ruggirello, R.; Caffarelli, C.; Gonnelli, S.; Barbagallo, M. Vitamin D and Risk of Incident Type 2 Diabetes in Older Adults: An Updated Systematic Review and Meta-Analysis. Nutrients 2024, 16, 1561. [Google Scholar] [CrossRef] [PubMed]
- Pittas, A.G.; Dawson-Hughes, B.; Li, T.; Van Dam, R.M.; Willett, W.C.; Manson, J.E.; Hu, F.B. Vitamin D and calcium intake in relation to type 2 diabetes in women. Diabetes Care 2006, 29, 650–656. [Google Scholar] [CrossRef]
- Pittas, A.G.; Dawson-Hughes, B.; Sheehan, P.; Ware, J.H.; Knowler, W.C.; Aroda, V.R.; Brodsky, I.; Ceglia, L.; Chadha, C.; Chatterjee, R.; et al. Vitamin D Supplementation and Prevention of Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B.; Staten, M.A.; Knowler, W.C.; Nelson, J.; Vickery, E.M.; LeBlanc, E.S.; Neff, L.M.; Park, J.; Pittas, A.G. Intratrial Exposure to Vitamin D and New-Onset Diabetes Among Adults With Prediabetes: A Secondary Analysis From the Vitamin D and Type 2 Diabetes (D2d) Study. Diabetes Care 2020, 43, 2916–2922. [Google Scholar] [CrossRef]
- Lu, Q.; Liang, Q.; Xi, Y. The effects of vitamin D supplementation on serum lipid profiles in people with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Front. Nutr. 2024, 11, 1419747. [Google Scholar] [CrossRef] [PubMed]
- Jayedi, A.; Daneshvar, M.; Jibril, A.T.; Sluyter, J.D.; Waterhouse, M.; Romero, B.D.; Neale, R.E.; Manson, J.E.; Shab-Bidar, S. Serum 25(OH)D Concentration, Vitamin D Supplementation, and Risk of Cardiovascular Disease and Mortality in Patients with Type 2 Diabetes or Prediabetes: A Systematic Review and Dose–Response Meta-Analysis. Am. J. Clin. Nutr. 2023, 118, 697–707. [Google Scholar] [CrossRef]
- Wan, Z.; Geng, T.; Li, R.; Chen, X.; Lu, Q.; Lin, X.; Chen, L.; Guo, Y.; Liu, L.; Shan, Z.; et al. Vitamin D status, genetic factors, and risks of cardiovascular disease among individuals with type 2 diabetes: A prospective study. Am. J. Clin. Nutr. 2022, 116, 1389–1399. [Google Scholar] [CrossRef] [PubMed]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D Deficiency: Consequence or Cause of Obesity? Medicina 2019, 55, 541. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, H.J.C.B.; da Silva, M.M.; de Castro, R.M.; da Silva, L.K.T.M.; Calado, C.M.S.d.S.; Araújo, E.R.d.S.; Silva, M.d.A.C.; Toscano, A.E. Vitamin D supplementation does not alter inflammatory markers in overweight and obese individuals: A systematic review and meta-analysis of randomized controlled trials. Nutr. Res. 2024, 128, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Che, J.; Tong, J.; Kuang, X.; Zheng, C.; Zhou, R.; Song, J.; Zhan, X.; Liu, Z. Relationship between serum 25-hydroxyvitamin D concentrations and blood pressure among US adults without a previous diagnosis of hypertension: Evidence from NHANES 2005–2018. Front. Nutr. 2023, 10, 1265662. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Apekey, T.A.; Steur, M. Vitamin D and risk of future hypertension: Meta-analysis of 283,537 participants. Eur. J. Epidemiol. 2013, 28, 205–221. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Burgess, S.; Munroe, P.B.; Khan, H. Vitamin D and high blood pressure: Causal association or epiphenomenon? Eur. J. Epidemiol. 2014, 29, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Nadir, M.A.; Struthers, A.D. Effect of vitamin D on blood pressure: A systematic review and meta-analysis. J. Hypertens. 2009, 27, 1948–1954. [Google Scholar] [CrossRef]
- Scragg, R.; Rahman, J.; Thornley, S. Association of sun and UV exposure with blood pressure and cardiovascular disease: A systematic review. J. Steroid Biochem. Mol. Biol. 2019, 187, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Verheyen, N.; Grübler, M.R.; Tomaschitz, A.; März, W. Vitamin D and cardiovascular disease prevention. Nat. Rev. Cardiol. 2016, 13, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Karunananthan, S.; Eisenberg, M.J.; Alexander, K.P.; Bergman, H. Role of Frailty in Patients With Cardiovascular Disease. Am. J. Cardiol. 2009, 103, 1616–1621. [Google Scholar] [CrossRef]
- Tsushima, Y.; Hatipoglu, B. Statin Intolerance: A Review and Update. Endocr. Pract. 2023, 29, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Yavuz, B.; Ertugrul, D.T. Statins and vitamin D: A hot topic that will be discussed for a long time. Dermato-endocrinology 2012, 4, 8–9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riche, K.D.; Arnall, J.; Rieser, K.; East, H.E.; Riche, D.M. Impact of vitamin D status on statin-induced myopathy. J. Clin. Transl. Endocrinol. 2016, 6, 56–59. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davidson, Z.E.; Walker, K.Z.; Truby, H. Do Glucocorticosteroids Alter Vitamin D Status? A Systematic Review with Meta-Analyses of Observational Studies. J. Clin. Endocrinol. Metab. 2012, 97, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Saket, S.; Varasteh, N.; Asl, A.A.H.; Saneifard, H. How Antiepileptics May Change the Serum Level of Vitamin D, Calcium, and Phosphorus in Children with Epilepsy. Iran. J. Child Neurol. 2021; 15, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Vitamin D: Fact Sheet for Health Professionals NIH Site. Available online: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/ (accessed on 26 December 2024).
- Mavar, M.; Sorić, T.; Bagarić, E.; Sarić, A.; Sarić, M.M. The Power of Vitamin D: Is the Future in Precision Nutrition through Personalized Supplementation Plans? Nutrients 2024, 16, 1176. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Francesca, C.; Mario, M.; Alberto, F. Fruit and vegetables in hypertensive women with asymptomatic peripheral arterial disease. Clin. Nutr. ESPEN 2018, 27, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Reddy, P.; Edwards, L.R. Magnesium Supplementation in Vitamin D Deficiency. Am. J. Ther. 2019, 26, e124–e132. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, C.; Pepe, J.; Piemonte, S.; Colangelo, L.; Cilli, M.; Minisola, S. Vitamin d and its relationship with obesity and muscle. Int. J. Endocrinol. 2014, 2014, 841248. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mattioli, A.V.; Coppi, F.; Nasi, M.; Pinti, M.; Gallina, S. Long COVID: A New Challenge for Prevention of Obesity in Women. Am. J. Lifestyle Med. 2022, 17, 164–168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haider, F.; Ghafoor, H.; Farooqui, K.; Khair, A.O.M.B.; Shoaib, F.; Hassan, O.F.H. Vitamin D and Cardiovascular Diseases: An Update. Cureus 2023, 15, e49734. [Google Scholar] [CrossRef] [PubMed Central]
- Wimalawansa, S.J.; Weiss, S.T.; Hollis, B.W. Integrating Endocrine, Genomic, and Extra-Skeletal Benefits of Vitamin D into National and Regional Clinical Guidelines. Nutrients 2024, 16, 3969. [Google Scholar] [CrossRef] [PubMed]
- Marcinowska-Suchowierska, E.; Kupisz-Urbańska, M.; Łukaszkiewicz, J.; Płudowski, P.; Jones, G. Vitamin D Toxicity–A Clinical Perspective. Front. Endocrinol. 2018, 9, 550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Galior, K.; Grebe, S.; Singh, R. Development of Vitamin D Toxicity from Overcorrection of Vitamin D Deficiency: A Review of Case Reports. Nutrients 2018, 10, 953. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Brandenburg, V.M.; Vervloet, M.G.; Marx, N. The role of vitamin D in cardiovascular disease: From present evidence to future perspectives. Atherosclerosis 2012, 225, 253–263. [Google Scholar] [CrossRef] [PubMed]
| Mechanism | Explanation |
|---|---|
| Anti-Inflammatory Effects |
|
| Glucose Metabolism |
|
| Lipid Metabolism |
|
| Vascular Calcification |
|
| Regulation of Blood Pressure |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattioli, A.V.; Coppi, F.; Severino, P.; Penna, C.; Pagliaro, P.; Dei Cas, A.; Bucciarelli, V.; Madonna, R.; Tarperi, C.; Schena, F.; et al. A Personalized Approach to Vitamin D Supplementation in Cardiovascular Health Beyond the Bone: An Expert Consensus by the Italian National Institute for Cardiovascular Research. Nutrients 2025, 17, 115. https://doi.org/10.3390/nu17010115
Mattioli AV, Coppi F, Severino P, Penna C, Pagliaro P, Dei Cas A, Bucciarelli V, Madonna R, Tarperi C, Schena F, et al. A Personalized Approach to Vitamin D Supplementation in Cardiovascular Health Beyond the Bone: An Expert Consensus by the Italian National Institute for Cardiovascular Research. Nutrients. 2025; 17(1):115. https://doi.org/10.3390/nu17010115
Chicago/Turabian StyleMattioli, Anna Vittoria, Francesca Coppi, Paolo Severino, Claudia Penna, Pasquale Pagliaro, Alessandra Dei Cas, Valentina Bucciarelli, Rosalinda Madonna, Cantor Tarperi, Federico Schena, and et al. 2025. "A Personalized Approach to Vitamin D Supplementation in Cardiovascular Health Beyond the Bone: An Expert Consensus by the Italian National Institute for Cardiovascular Research" Nutrients 17, no. 1: 115. https://doi.org/10.3390/nu17010115
APA StyleMattioli, A. V., Coppi, F., Severino, P., Penna, C., Pagliaro, P., Dei Cas, A., Bucciarelli, V., Madonna, R., Tarperi, C., Schena, F., Cetrullo, S., Angelone, T., Rocca, C., Parenti, A., Palazzuoli, A., Margonato, A., Paolillo, S., Perrone Filardi, P., Barillà, F., ... on behalf of the Italian National Institute for Cardiovascular Research (INRC). (2025). A Personalized Approach to Vitamin D Supplementation in Cardiovascular Health Beyond the Bone: An Expert Consensus by the Italian National Institute for Cardiovascular Research. Nutrients, 17(1), 115. https://doi.org/10.3390/nu17010115