
The Anxiety Burden in Patients with Chronic Intestinal Failure on Long-Term Parenteral Nutrition and in Their Caregivers

 , ,
, ,
Abstract
1. Introduction
2. Aims of the Study
3. Patients and Methods
3.1. Study Population
3.2. Inclusion Criteria
- -
- CIF patients and caregivers aged between 18 and 70;
- -
- CIF patients on HPN from at least 1 month;
- -
- Signed informed consent.
3.3. Exclusion Criteria
- -
- Drug addiction or abuse;
- -
- Psychosis or personality disorders classified according to the DSM-V criteria;
- -
- Acute medical complications requiring hospitalization.
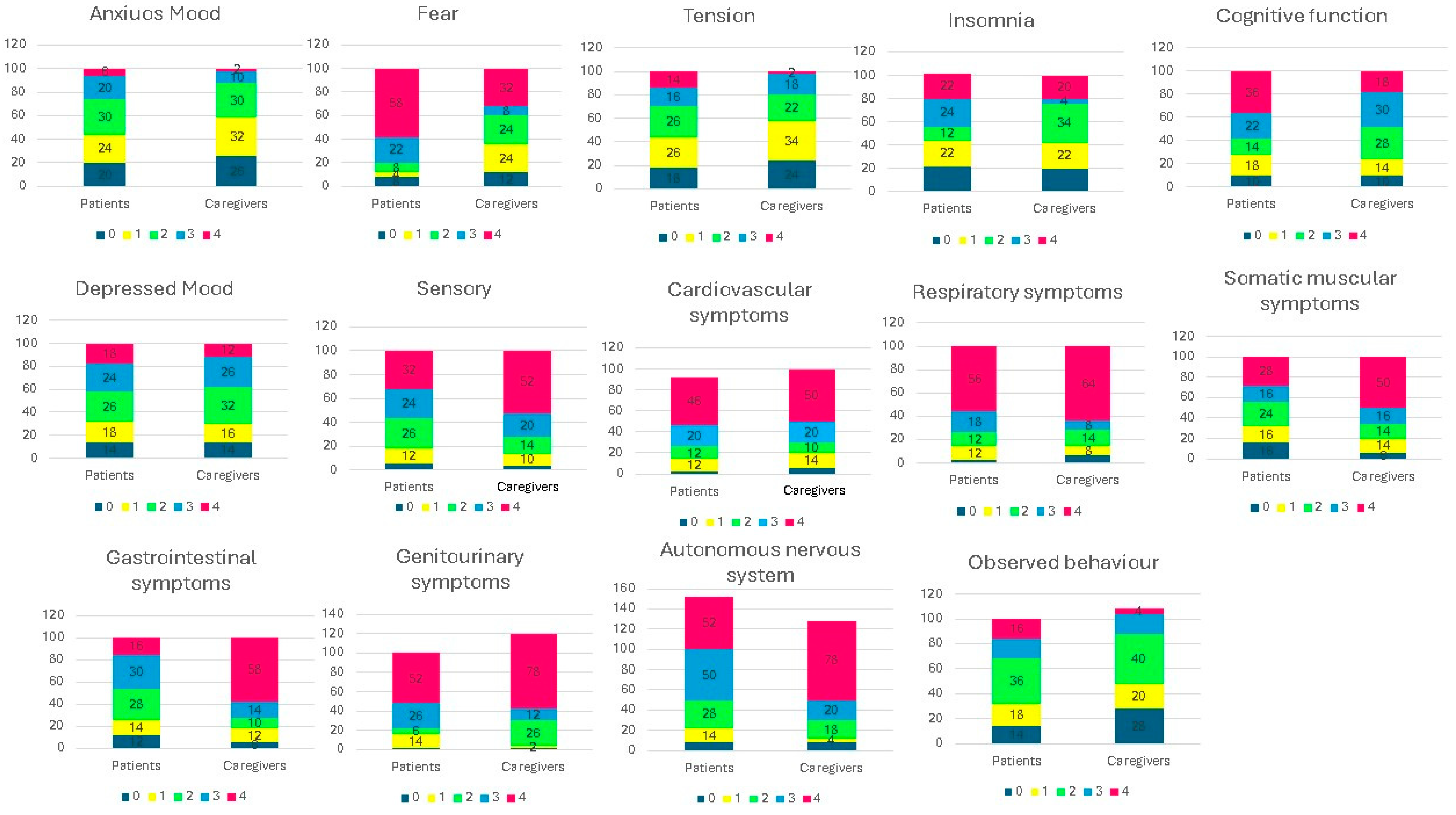
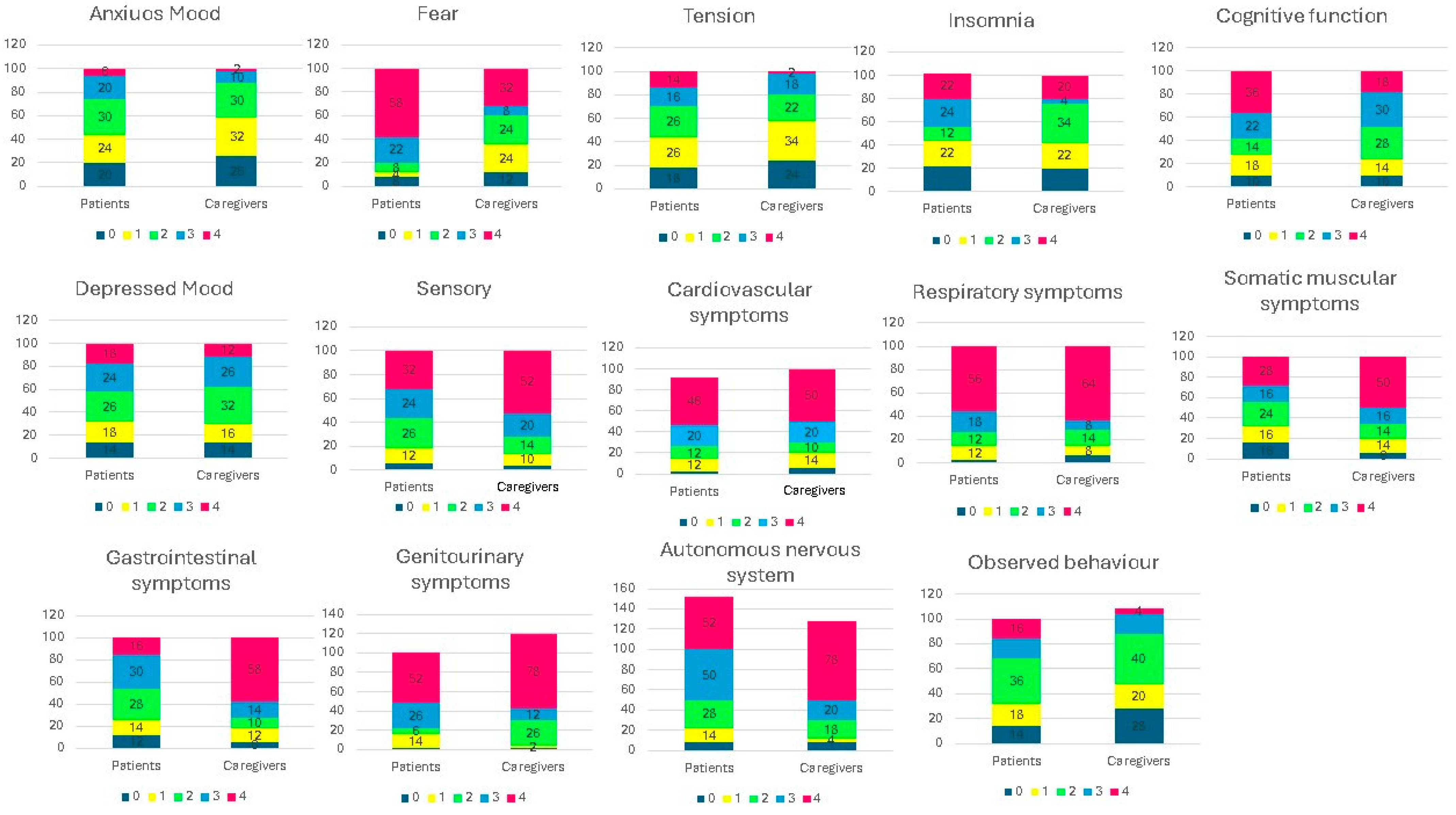
3.4. The Hamilton Anxiety Rating Scale (HAM-A)
- Anxious mood (worries, fear of the worst, irritability);
- Tension (startle response, fatigability, restlessness, easy tearing, trembling, inability to relax);
- Fear (of the dark/traffic/crowds, of being left alone);
- Insomnia (difficulty in falling asleep, broken sleep, unsatisfying sleep and fatigue on waking, dreams, nightmares, night terrors);
- Cognitive functions (poor memory and difficulty in concentration);
- Depressed mood (loss of interest, lack of pleasure in hobbies, depression, shifting moods);
- Somatic muscular symptoms (aches and pains, stiffness, bruxism, twitching, myoclonic jerks, teeth grinding, unsteady voice, increased muscular tone);
- Sensory (tinnitus, blurred vision, hot and cold flushes, feelings of weakness, pricking sensation);
- Cardiovascular (tachycardia, extrasystoles, palpitations, chest pain, vessel throbbing, faint feeling);
- Respiratory (chest tightness, choking pressure, sighing, dyspnoea);
- Gastrointestinal (irritable bowel syndrome-type symptoms, abdominal colicky pain, burning sensations, abdominal fullness, swallowing difficulty, nausea, vomiting, borborygmi, looseness of bowels/constipation, weight loss);
- Genitourinary (urinary frequency or urgency, amenorrhea, menorrhagia, frigidity, premature ejaculation, loss of libido, impotence);
- Autonomic (dry mouth, tension headache, flushing, sweating, giddiness, goose bumps);
- Observed behaviour at interview (fidgeting, restlessness or pacing, tremor of hands, furrowed brow, strained face, sighing or rapid respiration, pallor, swallowing, etc.).
3.5. Statistical Analysis
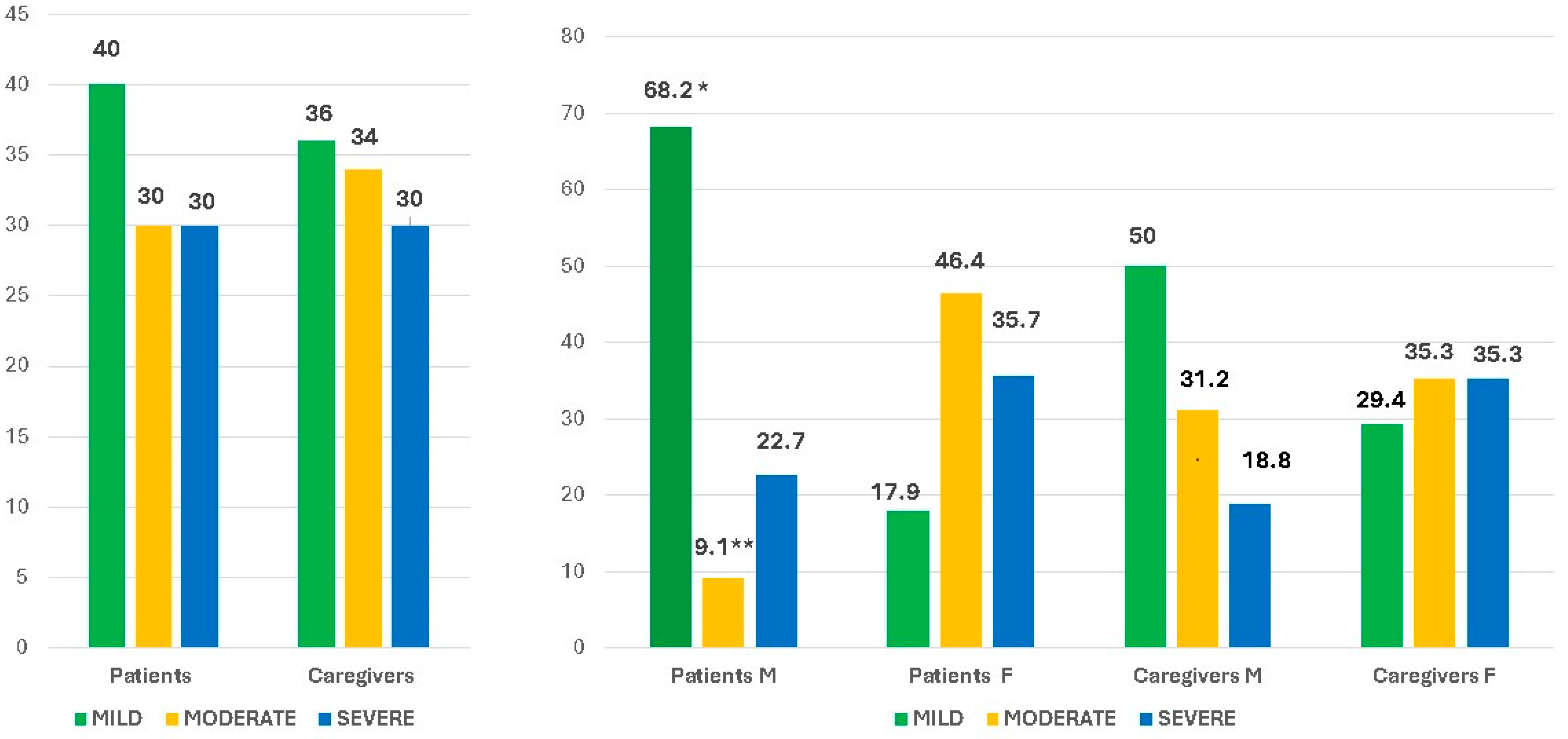
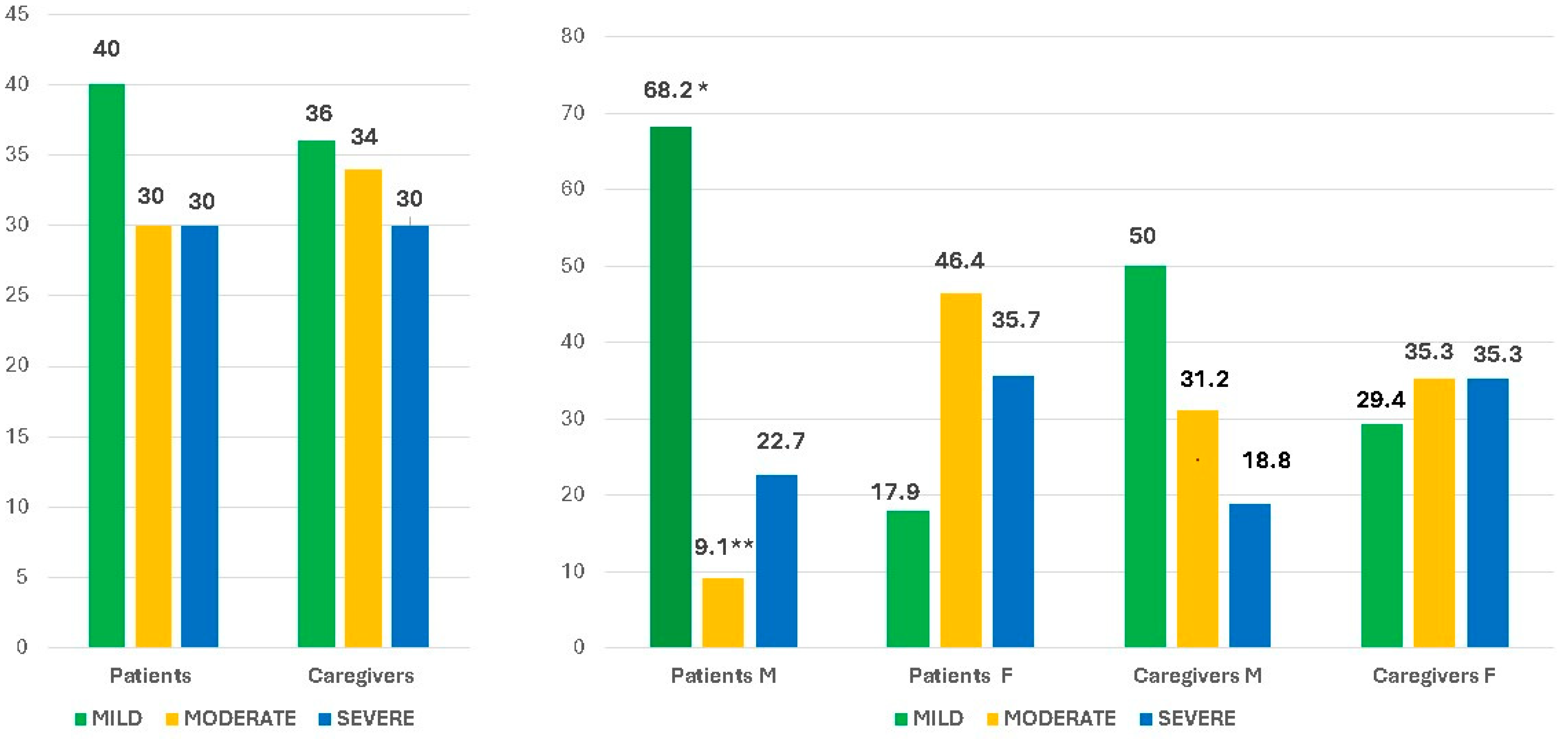
4. Results
5. Discussion
6. Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sowerbutts, A.M.; Panter, C.; Dickie, G.; Bennett, B.; Ablett, J.; Burden, S.; Lal, S. Short bowel syndrome and the impact on patients and their families: A qualitative study. J. Hum. Nutr. Diet. 2020, 33, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Carroll, R.E.; Benedetti, E.; Schowalter, J.P.; Buchman, A.L. Management and Complications of Short Bowel Syndrome: An Updated Review. Curr. Gastroenterol. Rep. 2016, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Burden, S.T.; Jones, D.J.; Gittins, M.; Ablett, J.; Taylor, M.; Mountford, C.; Tyrrell-Price, J.; Donnellan, C.; Leslie, F.; Bowling, T.; et al. Needs-based quality of life in adults dependent on home parenteral nutrition. Clin. Nutr. 2019, 38, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Wilburn, J.; McKenna, S.P.; Heaney, A.; Rouse, M.; Taylor, M.; Culkin, A.; Gabe, S.; Burden, S.; Lal, S. Development and validation of the Parenteral Nutrition Impact Questionnaire (PNIQ), a patient-centric outcome measure for Home Parenteral Nutrition. Clin. Nutr. 2018, 37, 978–983. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, P.B.; Shahraz, S.; Hopkins, T.; Worsfold, A.; Genestin, E. Impact of intestinal failure and parenteral support on adult patients with short-bowel syndrome: A multinational, noninterventional, cross-sectional survey. JEPN J. Parenter. Enteral Nutr. 2022, 46, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Heaney, A.; McKenna, S.P.; Wilburn, J.; Rouse, M.; Taylor, M.; Burden, S.; Lal, S. The impact of home parenteral nutrition on the lives of adults with type 3 intestinal failure. Clin. Nutr. ESPEN 2018, 24, 35–40. [Google Scholar] [CrossRef]
- Gulledge, A.D.; Gipson, W.T.; Steiger, E.; Hooley, R.; Srp, F. Home parenteral nutrition for the short bowel syndrome. Psychological issues. Gen. Hosp. Psychiatry 1980, 2, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Sowerbutts, A.M.; Jones, D.; Lal, S.; Burden, S. Quality of life in patients and in family members of those receiving home parenteral support with intestinal failure: A systematic review. Clin. Nutr. 2021, 40, 3210–3220. [Google Scholar] [CrossRef]
- Winkler, M.F.; Smith, C.E. Clinical, social, and economic impacts of home parenteral nutrition dependence in short bowel syndrome. J. Parenter. Enter. Nutr. 2014, 38 (Suppl. S1), 32Se7S. [Google Scholar] [CrossRef]
- Kumpf, V.J. Challenges and obstacles of long-term home parenteral nutrition. Nutr. Clin. Pract. 2019, 34, 196–203. [Google Scholar] [CrossRef]
- Messing, B.; Crenn, P.; Beau, P.; Boutron-Ruault, M.C.; Rambaud, J.-C.; Matuchansky, C. Long-term survival and parenteral nutrition dependence in adult patients with the short bowel syndrome. Gastroenterology 1999, 117, 1043.e50. [Google Scholar] [CrossRef] [PubMed]
- Baxter, J.P.; Fayers, P.M.; McKinlay, A.W. A review of the quality of life of adult patients treated with long-term parenteral nutrition. Clin. Nutr. 2006, 25, 543–553. [Google Scholar] [CrossRef] [PubMed]
- French, C.; Lal, S.; Jones, D.; Sowerbutts, A.M.; Brundrett, D.; Burch, N.; Calvert, C.; Cooper, S.C.; Donnellan, C.; Forbes, A.; et al. Impact of home parenteral nutrition on family members: A national multi-centre cross-sectional study. Clin. Nutr. 2022, 41, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Jeppesen, P.B.; Chen, K.; Murphy, R.; Shahraz, S.; Goodwin, B. Impact on caregivers of adult patients receiving parenteral support for short-bowel syndrome with intestinal failure: A multinational, cross-sectional survey. J. Parenter. Enter. Nutr. 2022, 46, 905–914. [Google Scholar] [CrossRef] [PubMed]
- Dibb, M.; Soop, M.; Teubner, A.; Shaffer, J.; Abraham, A.; Carlson, G.; Lal, S. Survival and nutritional dependence on home parenteral nutrition: Three decades of experience from a single referral centre. Clin. Nutr. 2017, 36, 570.e6. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E. Hamilton Rating Scale for Anxiety (HAM-A). Occup. Med. 2015, 65, 601. [Google Scholar] [CrossRef] [PubMed]
- Donzuso, G.; Cerasa, A.; Gioia, M.C.; Caracciolo, M.; Quattrone, A. The neuroanatomical correlates of anxiety in a healthy population: Differences between the State-Trait Anxiety Inventory and the Hamilton Anxiety Rating Scale. Brain Behav. 2014, 4, 504–514. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A. Relationship between the Beck Anxiety inventory and the Hamilton Anxiety Rating Scale with anxious outpatients. J. Anx. Disord. 1991, 5, 213–223. [Google Scholar] [CrossRef]
- Cummings, J.H.; James, W.P.; Wiggins, H.S. Role of the colon in ileal-resection diarrhoea. Lancet 1973, 1, 344–347. [Google Scholar] [CrossRef]
- Neumann, M.L.; Allen, J.Y.; Ladner, A.; Kakani, S.; Weaver, M.S.; Mercer, D.F. Exploring the impact of pediatric short bowel syndrome on parent well-being using a disease-specific pilot survey. Nutr. Clin. Pract. 2023, 39, 154–167. [Google Scholar] [CrossRef]
- Belza, C.; Avitzur, Y.; Ungar, W.J.; Stremler, R.; Fehlings, D.; Wales, P.W. Stress, anxiety, depression, and health-related quality of life in caregivers of children with intestinal failure receiving parenteral nutrition: A cross-sectional survey study. JEPN J. Parenter. Enteral Nutr. 2023, 47, 342–353. [Google Scholar] [CrossRef] [PubMed]
- van Oers, H.A.; Haverman, L.; Olieman, J.F.; Neelis, E.G.; Jonkers-Schuitema, C.F.; Grootenhuis, M.A.; Tabbers, M.M. Health-related quality of life, anxiety, depression and distress of mothers and fathers of children on Home parenteral nutrition. Clin. Nutr. 2019, 38, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Selvi, K.; Parling, T.; Ljótsson, B.; Welch, E.; Ghaderi, A. Two randomized controlled trials of the efficacy of acceptance and commitment therapy-based educational course for body shape dissatisfaction. Scand. J. Psychol. 2021, 62, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Castinel, J.; Pellet, G.; Laharie, D.; Zerbib, F.; Silvain, C.; Wilsius, E.; Kerlogot, L.; Rivière, P.; Poullenot, F. Male gender is associated with informal caregiver burden in patients with chronic intestinal failure treated with home parenteral nutrition. JEPN J. Parenter. Enteral Nutr. 2022, 46, 1593–1601. [Google Scholar] [CrossRef]
- Silva, R.; Guerra, P.; Rocha, A.; Correia, M.; Ferreira, R.; Fonseca, J.; Lima, E.; Oliveira, A.; Gomes, M.V.; Ramos, D.; et al. Clinical, Economic, and Humanistic Impact of Short-Bowel Syndrome/Chronic Intestinal Failure in Portugal (PARENTERAL Study). GE Port. J. Gastroenterol. 2022, 30, 293–304. [Google Scholar] [CrossRef]
- Kurita, G.P.; Eidemak, I.; Larsen, S.; Jeppesen, P.B.; Antonsen, L.B.; Molsted, S.; Liem, Y.S.; Pressler, T.; Sjøgren, P. The impact of caring on caregivers of patients with life-threatening organ failure. Palliat. Support. Care 2023, 1–7. [Google Scholar] [CrossRef]
- Smith, C.E.; Yadrich, D.; Wright, S.; Ridder, L.; Werkowitch, M.; Bruce, A.; Bonar, J.R.M. Themes of Stressors, Emotional Fatigue, and Communication Challenges Found in Mobile Care Discussion Sessions With Patients Requiring Lifelong Home Parenteral Nutrition Infusions. JEPN J. Parenter. Enteral Nutr. 2021, 45, 499–506. [Google Scholar] [CrossRef]
- Marchese, F.; Bonanno, B.; Borinato, D.; Burgio, S.; Mangiapane, D.; Matranga, M.; Saputo, E.; La Barbera, D. Psychosis, symbol, affectivity 2: Another perspective on the treatment of psychotic disorder. J. Anal. Psychol. 2021, 66, 200–220. [Google Scholar] [CrossRef]
- Santarpia, L.; Bozzetti, F. Acute impact of home parenteral nutrition in patients with late-stage cancer on family caregivers: Preliminary data. Support. Care Cancer 2018, 26, 667.e71. [Google Scholar] [CrossRef]
- Osse, B.H.; Vernooij-Dassen, M.J.; Schade, E.; Grol, R.P. Problems experienced by the informal caregivers of cancer patients and their needs for support. Cancer Nurs. 2006, 29, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Beurskens-Meijerink, J.; Huisman-de Waal, G.; Wanten, G. Evaluation of quality of life and caregiver burden in home parenteral nutrition patients: A cross sectional study. Clin. Nutr. ESPEN 2020, 37, 50.e7. [Google Scholar] [CrossRef] [PubMed]
- Sowerbutts, A.M.; Lal, S.; Sremanakova, J.; Clamp, A.R.; Jayson, G.C.; Teubner, A.; Hardy, L.; Todd, C.; Raftery, A.-M.; Sutton, E.; et al. Palliative home parenteral nutrition in patients with ovarian cancer and malignant bowel obstruction: Experiences of women and family caregivers. BMC Palliat. Care 2019, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Riffin, C.; Wolff, J.L.; Estill, M.; Prabhu, S.; Pillemer, K.A. Caregiver needs assessment in primary care: Views of clinicians, staff, patients, and caregivers. J. Am. Geriatr. Soc. 2020, 68, 1262.e70. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Patients (n. 50) | Caregivers (n. 50) | p | |
|---|---|---|---|
| Age (years) | 48.4 ± 15.0; median 52 (18–69) | 50.7 ± 13.3; median 54 (21–71) | n.s |
| Gender | 28 F/22 M | 34 F/16 M | n.s |
| Disease duration (yrs) | 6.5 ± 5.38; median 7 (0.5–22) | - | - |
| Primary disease | |||
| Intestinal infarction | 17 | ||
| Crohn’s disease | 15 | ||
| Intestinal volvulus | 5 | ||
| Intestinal adhesions | 4 | ||
| Intestinal pseudobstruction | 3 | ||
| Bariatric surgery | 2 | ||
| Mucosal disease | 2 | ||
| Radiation enteritis | 2 | ||
| Residual small bowel length, cm median (range) | 7 no resections in 43: median 108 cm (15–300) | ||
| Presence of stoma (yes/no) | 12/38 | ||
| Presence of ileocecal valve (yes/no) | 7/43 | ||
| Colon in continuity (yes/no) | 38/12 | ||
| Percentage of colon in continuity according to Cummings’ classification median (range) | 70 (0–100) | ||
| PN dependency duration (yrs) | 6.5 ± 5.38; median 7 (0.5–22) | ||
| Days of infusion per week | 5 (3–7) | ||
| Weight (kg) | 55.9 ± 10.5 (35–80) | - | - |
| BMI (kg/m2) | 20.7 ± 3.2 (12.5–25.5) | - | - |
| Degree of kinship | |||
| Husband | 16 | 14 | |
| Wife | 15 | 16 | |
| Son/daughter | 11 | 6 | |
| Mother/father | 6 | 11 | |
| Brother/sister | 3 | 3 | |
| Education | |||
| Primary school license | 5 | 3 | |
| Secondary school license | 17 | 18 | |
| High school license | 23 | 23 | |
| University degree | 5 | 4 | |
| Employment | 19 remunerated | 23 remunerated | |
| 26 non remunerated | 23 non remunerated | ||
| 5 retired | 4 retired | ||
| Total HAM-A score | 20.94 ± 10.72 (3–42) | 21.94 ± 10.85 (7–52) | n.s |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santarpia, L.; Orefice, R.; Alfonsi, L.; Marra, M.; Contaldo, F.; Pasanisi, F. The Anxiety Burden in Patients with Chronic Intestinal Failure on Long-Term Parenteral Nutrition and in Their Caregivers. Nutrients 2024, 16, 1168. https://doi.org/10.3390/nu16081168
Santarpia L, Orefice R, Alfonsi L, Marra M, Contaldo F, Pasanisi F. The Anxiety Burden in Patients with Chronic Intestinal Failure on Long-Term Parenteral Nutrition and in Their Caregivers. Nutrients. 2024; 16(8):1168. https://doi.org/10.3390/nu16081168
Chicago/Turabian StyleSantarpia, Lidia, Raffaella Orefice, Lucia Alfonsi, Maurizio Marra, Franco Contaldo, and Fabrizio Pasanisi. 2024. "The Anxiety Burden in Patients with Chronic Intestinal Failure on Long-Term Parenteral Nutrition and in Their Caregivers" Nutrients 16, no. 8: 1168. https://doi.org/10.3390/nu16081168
APA StyleSantarpia, L., Orefice, R., Alfonsi, L., Marra, M., Contaldo, F., & Pasanisi, F. (2024). The Anxiety Burden in Patients with Chronic Intestinal Failure on Long-Term Parenteral Nutrition and in Their Caregivers. Nutrients, 16(8), 1168. https://doi.org/10.3390/nu16081168