

Healthier Dietary Patterns Are Associated with Better Sleep Quality among Shanghai Suburban Adults: A Cross-Sectional Study

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire and Anthropometric Measurements
2.3. Sleep Quality
2.4. A Priori Dietary Pattern Scores
2.5. A Posteriori Dietary Pattern Scores
2.6. Considered Covariates
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
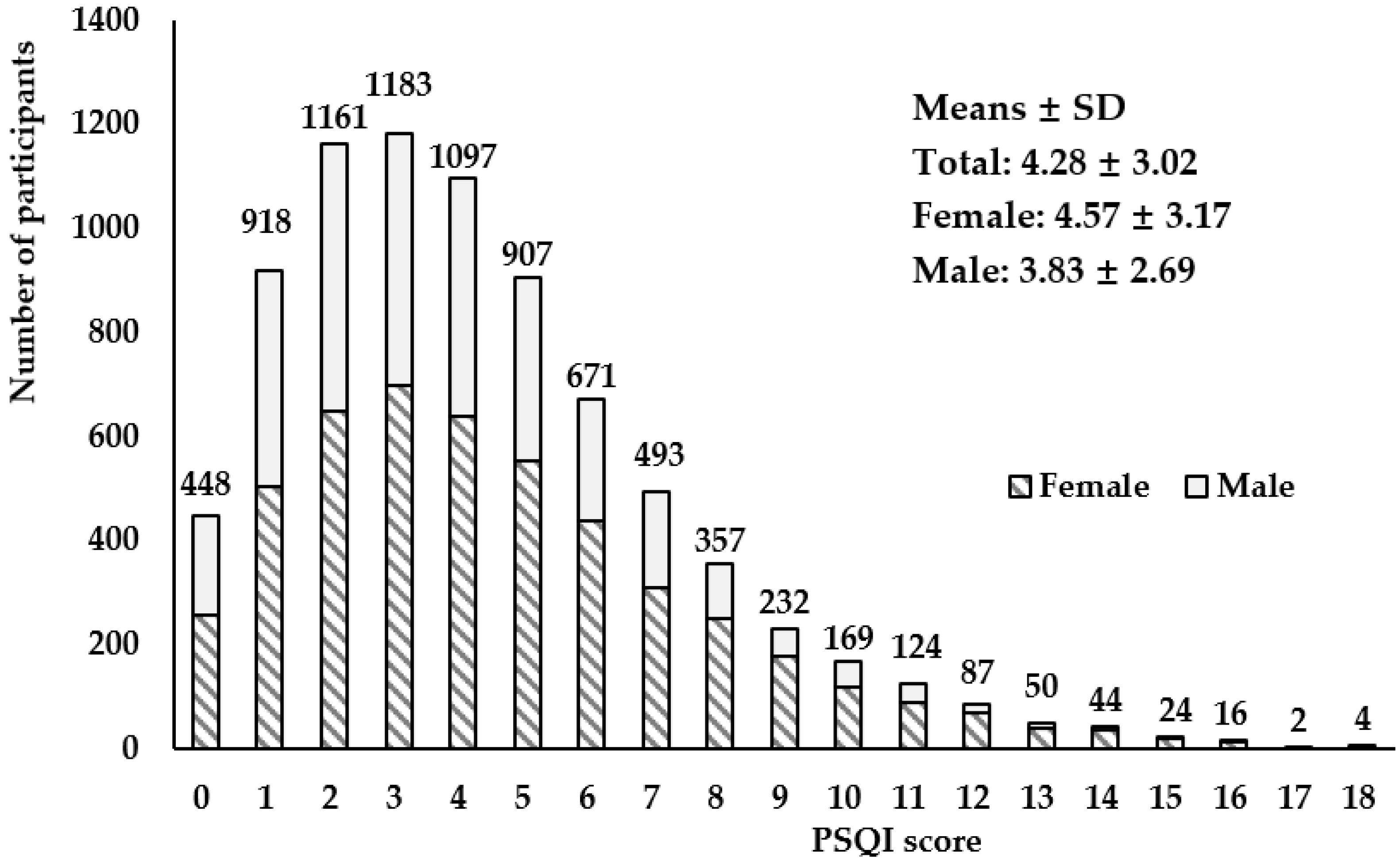
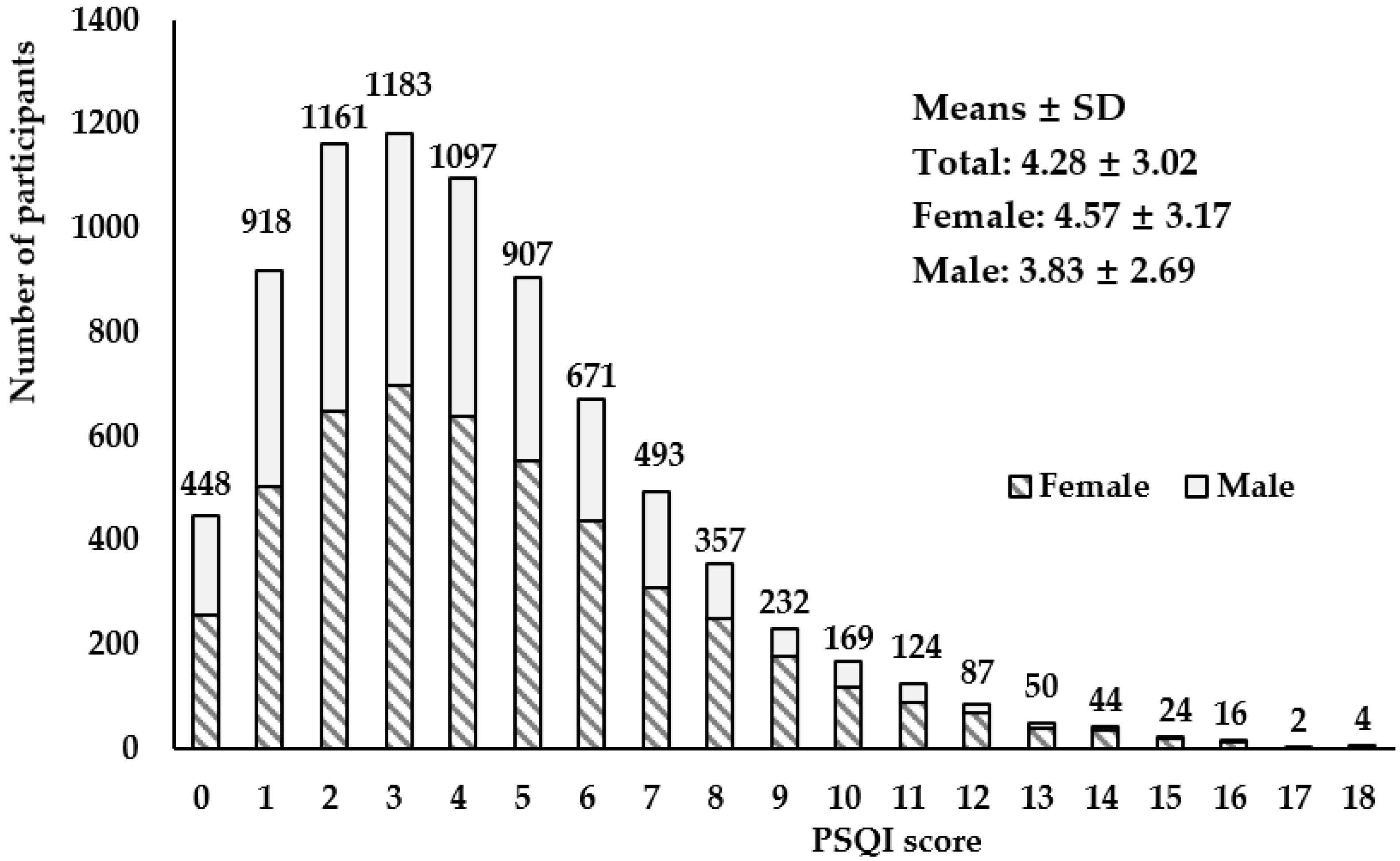
3.2. Pittsburgh Sleep Quality Index Scores for Study Participants
3.3. Dietary Pattern Scores of the Participants
3.4. Associations between Dietary Pattern Scores and Sleep Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chattu, V.K.; Manzar, M.D.; Kumary, S.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The global problem of insufficient sleep and its serious public health implications. Healthcare 2018, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.P.; Li, H.B. Influence of shift work on rest-activity rhythms, sleep quality, and fatigue of female nurses. Chronobiol. Int. 2022, 39, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lee, Y. Influence of sleep characteristic changes on nurses’ quality of life during their transition to practice: A prospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 573. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.J.; Kim, Y.; Kwak, Y. Influence of smartphone addiction and poor sleep quality on attention-deficit hyperactivity disorder symptoms in university students: A cross-sectional study. J. Am. Coll. Health 2022, 70, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Nistor, P.; Chang-Kit, B.; Nicholson, K.; Anderson, K.K.; Stranges, S. The relationship between sleep health and multimorbidity in community dwelling populations: Systematic review and global perspectives. Sleep Med. 2023, 109, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Hale, L.; Troxel, W.; Buysse, D.J. Sleep health: An opportunity for public health to address health equity. Annu. Rev. Public Health 2020, 41, 81–99. [Google Scholar] [CrossRef] [PubMed]
- Cable, J.; Schernhammer, E.; Hanlon, E.C.; Vetter, C.; Cedernaes, J.; Makarem, N.; Dashti, H.S.; Shechter, A.; Depner, C.; Ingiosi, A.; et al. Sleep and circadian rhythms: Pillars of health—A keystone symposia report. Ann. N. Y. Acad. Sci. 2021, 1506, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Tuo, H.; Wang, S.; Zhao, L. The effects of dietary nutrition on sleep and sleep disorders. Mediat. Inflamm. 2020, 2020, 3142874. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Mikic, A.; Pietrolungo, C.E. Effects of diet on sleep quality. Adv. Nutr. 2016, 7, 938–949. [Google Scholar] [CrossRef]
- Ward, A.L.; Reynolds, A.N.; Kuroko, S.; Fangupo, L.J.; Galland, B.C.; Taylor, R.W. Bidirectional associations between sleep and dietary intake in 0–5 year old children: A systematic review with evidence mapping. Sleep Med. Rev. 2020, 49, 101231. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between diet and sleep quality: A systematic review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef]
- Knowlden, A.P.; Hackman, C.L.; Sharma, M. Systematic review of dietary interventions targeting sleep behavior. J. Altern. Complemen. Med. 2016, 22, 349–362. [Google Scholar] [CrossRef]
- Schulz, C.A.; Oluwagbemigun, K.; Nothlings, U. Advances in dietary pattern analysis in nutritional epidemiology. Eur. J. Nutr. 2021, 60, 4115–4130. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Martinez-Gonzalez, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. BMJ-Br. Med. J. 2018, 361, k2396. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Scoditti, E.; Tumolo, M.R.; Garbarino, S. Mediterranean diet on sleep: A health alliance. Nutrients 2022, 14, 2998. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Ferri, R.; Caraci, F.; Cosentino, F.; Castellano, S.; Galvano, F.; Grosso, G. Adherence to the mediterranean diet is associated with better sleep quality in Italian adults. Nutrients 2019, 11, 976. [Google Scholar] [CrossRef]
- Mamalaki, E.; Anastasiou, C.A.; Ntanasi, E.; Tsapanou, A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Associations between the mediterranean diet and sleep in older adults: Results from the hellenic longitudinal investigation of aging and diet study. Geriatr. Gerontol. Int. 2018, 18, 1543–1548. [Google Scholar] [CrossRef] [PubMed]
- Zuraikat, F.M.; Makarem, N.; St-Onge, M.P.; Xi, H.; Akkapeddi, A.; Aggarwal, B. A mediterranean dietary pattern predicts better sleep quality in us women from the American heart association go red for women strategically focused research network. Nutrients 2020, 12, 2830. [Google Scholar] [CrossRef]
- Liang, H.; Beydoun, H.A.; Hossain, S.; Maldonado, A.; Zonderman, A.B.; Fanelli-Kuczmarski, M.T.; Beydoun, M.A. Dietary approaches to stop hypertension (dash) score and its association with sleep quality in a national survey of middle-aged and older men and women. Nutrients 2020, 12, 1510. [Google Scholar] [CrossRef]
- Gonzalez-Trevino, I.M.; Arrona-Palacios, A.; Nunez-Rocha, G.M.; Jansen, E.C. Association between self-reported sleep duration and dietary quality in Mexican school-aged children. Appetite 2022, 178, 106177. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.C.; Prather, A.; Leung, C.W. Associations between sleep duration and dietary quality: Results from a nationally-representative survey of us adults. Appetite 2020, 153, 104748. [Google Scholar] [CrossRef] [PubMed]
- Behbahani, H.B.; Borazjani, F.; Sheikhi, L.; Amiri, R.; Angali, K.A.; Nejad, S.B.; Samadani, M. The association between diet quality scores with sleep quality among employees: A cross-sectional study. Ethiop. J. Health Sci. 2022, 32, 145–154. [Google Scholar] [PubMed]
- Van Lee, L.; Chia, A.R.; Loy, S.L.; Colega, M.; Tham, E.; Cai, S.; Yap, F.; Godfrey, K.M.; Teoh, O.H.; Goh, D.; et al. Sleep and dietary patterns in pregnancy: Findings from the gusto cohort. Int. J. Environ. Res. Public Health 2017, 14, 1409. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.C.; Stern, D.; Monge, A.; O’Brien, L.M.; Lajous, M.; Peterson, K.E.; Lopez-Ridaura, R. Healthier dietary patterns are associated with better sleep quality among midlife Mexican women. J. Clin. Sleep Med. 2020, 16, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Velazquez-Kronen, R.; Millen, A.E.; Ochs-Balcom, H.M.; Mnatsakanova, A.; Gu, J.K.; Andrew, M.; Violanti, J. Sleep quality and dietary patterns in an occupational cohort of police officers. Behav. Sleep Med. 2022, 20, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, R.; Asakura, K.; Kobayashi, S.; Suga, H.; Sasaki, S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. J. Occup. Health 2014, 56, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Shi, Z.; Lv, J.; Guo, Y.; Bian, Z.; Du, H.; Chen, Y.; Tao, R.; Huang, Y.; Chen, J.; et al. Dietary patterns and insomnia symptoms in Chinese adults: The China Kadoorie biobank. Nutrients 2017, 9, 232. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Zhao, A.; Szeto, I.M.; Wang, Y.; Meng, L.; Li, T.; Zhang, J.; Wang, M.; Tian, Z.; Zhang, Y. Diet quality, consumption of seafood and eggs are associated with sleep quality among Chinese urban adults: A cross-sectional study in eight cities of China. Food Sci. Nutr. 2019, 7, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Li, H.; Xu, G.; Ying, Y.; Gong, Q.; Zhao, J.; Zhang, X.; Zhang, L.; Liu, S.; Han, L. Association of dietary behaviors and sleep quality: Results from the adults chronic diseases and risk factors survey of 2015 in Ningbo, China. Int. J. Environ. Res. Public Health 2018, 15, 1823. [Google Scholar] [CrossRef]
- Zhao, Q.; Chen, B.; Wang, R.; Zhu, M.; Shao, Y.; Wang, N.; Liu, X.; Zhang, T.; Jiang, F.; Wang, W.; et al. Cohort profile: Protocol and baseline survey for the shanghai suburban adult cohort and biobank (ssacb) study. BMJ Open 2020, 10, e035430. [Google Scholar] [CrossRef] [PubMed]
- Banna, J.C.; McCrory, M.A.; Fialkowski, M.K.; Boushey, C. Examining Plausibility of Self-Reported Energy Intake Data: Considerations for Method Selection. Front. Nutr. 2017, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Fan, J.; Dong, R.; Zhang, M.; Jiang, Y.; Zhao, Q.; Zhao, G.; Chen, B.; Li, J.; Liu, S. The effect of dietary pattern on metabolic syndrome in a suburban population in shanghai, China. Nutrients 2023, 15, 2185. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Huang, Y.; Wu, H.; He, G.; Li, S.; Chen, B. Association between dietary patterns and frailty prevalence in shanghai suburban elders: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 10852. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.R.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Fabbri, M.; Beracci, A.; Martoni, M.; Meneo, D.; Tonetti, L.; Natale, V. Measuring subjective sleep quality: A review. Int. J. Environ. Res. Public Health 2021, 18, 1082. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhang, H.; Zhao, M.; Li, Z.; Cook, C.E.; Buysse, D.J.; Zhao, Y.; Yao, Y. Reliability, validity, and factor structure of pittsburgh sleep quality index in community-based centenarians. Front. Psychiatry 2020, 11, 573530. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.Q.; Bloom, M.S.; Wu, Q.Z.; He, Z.Z.; Qian, Z.; Stamatakis, K.A.; Liu, E.; Vaughn, M.; Lawrence, W.R.; Yang, M.; et al. Association between depressive symptoms and poor sleep quality among han and manchu ethnicities in a large, rural, Chinese population. PLoS ONE 2019, 14, e0226562. [Google Scholar] [CrossRef] [PubMed]
- Ding, K.R.; Wang, S.B.; Xu, W.Q.; Lin, L.H.; Liao, D.D.; Chen, H.B.; Tan, W.Y.; Huang, J.H.; Hou, C.L.; Jia, F.J. Low mental health literacy and its association with depression, anxiety and poor sleep quality in Chinese elderly. Asia-Pac. Psychiatry 2022, 14, e12520. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, L.; Wang, K.; Han, X.; Cong, L.; Wang, Y.; Zhang, L.; Yan, Z.; Tang, S.; Du, Y. Prevalence and associated factors of poor sleep quality among Chinese older adults living in a rural area: A population-based study. Aging Clin. Exp. Res. 2020, 32, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Hu, Z.; Nie, Y.; Zhu, T.; Chiwanda, K.A.; Yu, Y.; Xu, H. The prevalence of poor sleep quality and associated risk factors among Chinese elderly adults in nursing homes: A cross-sectional study. PLoS ONE 2020, 15, e0232834. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Jiang, Y.; Wang, N.; Zhu, M.; Liu, X.; Jiang, F.; Zhao, G.; Zhao, Q. Sleep quality of Shanghai residents: Population-based cross-sectional study. Qual. Life Res. 2020, 29, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.Q.; Li, F.; Wu, H.; Wang, Y.C.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. Evaluation of the validity and reliability of the Chinese healthy eating index. Nutrients 2018, 10, 114. [Google Scholar] [CrossRef]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary approaches to stop hypertension (dash) diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Roberts, A.; Shechter, A.; Choudhury, A.R. Fiber and saturated fat are associated with sleep arousals and slow wave sleep. J. Clin. Sleep Med. 2016, 12, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Karbasi, S.; Azaryan, E.; Zangooie, A.; Zarban, A.; Bahrami, A. Association between adherence to the dietary approaches to stop hypertension (dash) diet and maternal and infant sleep disorders. BMC Nutr. 2022, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, C.; Tan, S.; Zhang, Y.; Zhang, K.; Wang, B.; Zuo, H. Association of dietary approaches to stop hypertension (dash) diet with self-reported sleep-disordered breathing (sdb): A cross-sectional study from China. Br. J. Nutr. 2023, 130, 1806–1813. [Google Scholar] [CrossRef] [PubMed]
- Mohd, F.T.N.; Norsham, J.; Nadhra, A.; Dalila, A.; Nursyafiqa; Nasuha, S.I.; Das, S. Chrononutrition behaviors, sugar-sweetened beverage consumption, sleep quality and the association with body mass index among malaysian women. Chronobiol. Int. 2023, 40, 1487–1499. [Google Scholar] [CrossRef] [PubMed]
- Zuraikat, F.M.; Wood, R.A.; Barragan, R.; St-Onge, M.P. Sleep and diet: Mounting evidence of a cyclical relationship. Annu. Rev. Nutr. 2021, 41, 309–332. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Zuraikat, F.M. Reciprocal roles of sleep and diet in cardiovascular health: A review of recent evidence and a potential mechanism. Curr. Atheroscleros. Rep. 2019, 21, 11. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Rodriguez, A.; Rubio-Arias, J.A.; Ramos-Campo, D.J.; Reche-Garcia, C.; Leyva-Vela, B.; Nadal-Nicolas, Y. Psychological and sleep effects of tryptophan and magnesium-enriched mediterranean diet in women with fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 2227. [Google Scholar] [CrossRef]
- Frank, S.; Gonzalez, K.; Lee-Ang, L.; Young, M.C.; Tamez, M.; Mattei, J. Diet and sleep physiology: Public health and clinical implications. Front. Neurol. 2017, 8, 393. [Google Scholar] [CrossRef] [PubMed]
- Pepin, A.; Stanhope, K.L.; Imbeault, P. Are fruit juices healthier than sugar-sweetened beverages? A review. Nutrients 2019, 11, 1006. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, C.; Xu, Y.; Wang, Y.; Zhang, Y.; Jiang, T.; Zhang, Q. The relationship between sugar-sweetened beverages, sleep disorders, and diabesity. Front. Endocrinol. 2022, 13, 1041977. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Food Groups | Dietary Patterns b | |||
|---|---|---|---|---|
| Factor 1: “Protein-Rich and Vegetables” | Factor 2: “Dairy and Fruits” | Factor 3: “Snacks, Salted Food and Nuts” | Factor 4: “Beverages” | |
| Meat | 0.707 | −0.086 | 0.108 | 0.115 |
| Fish and seafood | 0.676 | 0.105 | 0.135 | −0.056 |
| Poultry | 0.659 | −0.064 | 0.087 | 0.156 |
| Vegetables | 0.572 | 0.104 | −0.076 | −0.102 |
| Soybeans and soy products | 0.457 | 0.206 | 0.117 | 0.233 |
| Dairy and dairy products | 0.153 | 0.664 | 0.064 | 0.116 |
| Fruits | 0.282 | 0.549 | −0.035 | 0.052 |
| Snacks | 0.007 | 0.059 | 0.650 | 0.109 |
| Salted food | −0.036 | −0.305 | 0.590 | 0.094 |
| Nuts and seeds | 0.169 | 0.160 | 0.460 | −0.111 |
| Sugar-sweetened beverages | 0.063 | −0.054 | 0.056 | 0.777 |
| Juice | 0.050 | 0.278 | −0.027 | 0.664 |
| Eggs | 0.306 | 0.054 | 0.370 | −0.013 |
| Grain and tubers | 0.303 | −0.440 | 0.025 | −0.122 |
| Whole grain and mixed beans | 0.290 | 0.241 | 0.256 | −0.174 |
| Alcohol | 0.259 | −0.359 | −0.270 | 0.111 |
| Characteristics | Total | Good Sleeper (PQIS < 5) | Poor Sleeper (PQIS ≥ 5) | p Value a | |
|---|---|---|---|---|---|
| Age (years) | 53.19 ± 13.47 | 52.55 ± 13.85 | 54.79 ± 12.32 | <0.001 | |
| BMI (kg/m2) | 23.68 ± 4.91 | 23.70 ± 4.95 | 23.64 ± 4.90 | 0.615 | |
| Energy intake (kcal/day) | 1745.35 ± 683.70 | 1757.95 ± 685.15 | 1713.67 ± 679.15 | 0.009 | |
| Total, N (%) | 7987 (100) | 5714 (71.54) | 2273 (28.46) | ||
| Sex | |||||
| Male | 3117 (39.03) | 2417 (77.54) | 700 (22.46) | <0.001 | |
| Female | 4870 (60.97) | 3297 (67.70) | 1573 (32.30) | ||
| Age | |||||
| <40 years | 1610 (20.16) | 1283 (79.69) | 327 (20.31) | <0.001 | |
| 40–60 years | 3910 (48.95) | 2682 (68.59) | 1228 (31.41) | ||
| 60–74 years | 2467 (30.89) | 1749 (70.90) | 718 (29.10) | ||
| BMI | |||||
| Underweight | 467 (5.85) | 322 (68.95) | 145 (31.05) | 0.592 | |
| Normal | 3615 (45.26) | 2602 (71.98) | 1013 (28.02) | ||
| Overweight | 2853 (35.72) | 2037 (71.40) | 816 (28.60) | ||
| Obese | 1052 (13.17) | 753 (71.58) | 299 (28.42) | ||
| Education | |||||
| Primary school or below | 2726 (34.13) | 1845 (67.68) | 881 (32.32) | <0.001 | |
| Secondary school or above | 5261 (65.87) | 3869(73.54) | 1392 (26.46) | ||
| Marital status | |||||
| Married | 7384 (92.45) | 5300 (71.78) | 2084 (28.22) | 0.103 | |
| Other b | 603 (7.55) | 414 (68.66) | 189 (31.34) | ||
| Lifestyle variables | |||||
| Current smoker c | Yes | 1669 (20.90) | 1258 (75.37) | 411 (24.63) | <0.001 |
| No | 6318 (79.10) | 4456 (70.53) | 1862 (29.47) | ||
| Current alcohol user d | Yes | 787 (9.85) | 490 (62.26) | 297 (37.74) | <0.001 |
| No | 7200 (90.15) | 5224 (72.56) | 1976 (27.44) | ||
| Physical exercise e | Yes | 2304 (28.85) | 1715 (74.44) | 589 (25.56) | <0.001 |
| No | 5683 (71.15) | 3999 (70.37) | 1684 (29.63) | ||
| Being sedentary > 6 h/day | Yes | 1877 (23.50) | 1359 (72.40) | 518 (27.60) | 0.344 |
| No | 6110 (76.50) | 4355 (71.28) | 1755 (28.72) | ||
| Related diseases | |||||
| Hypertension | Yes | 2424 (30.35) | 1632 (67.33) | 792 (32.67) | <0.001 |
| No | 5563 (69.65) | 4082 (73.38) | 1481 (26.62) | ||
| Hyperlipidemia | Yes | 944 (11.82) | 724 (76.69) | 220 (23.31) | <0.001 |
| No | 7043 (99.18) | 4990 (70.85) | 2053 (29.15) | ||
| Diabetes | Yes | 575 (7.20) | 393 (68.35) | 182 (31.65) | 0.078 |
| No | 7412 (92.80) | 5321 (71.79) | 2091 (28.21) | ||
| Coronary heart disease | Yes | 430 (5.38) | 238 (55.35) | 192 (44.65) | <0.001 |
| No | 7557 (94.62) | 5476 (72.46) | 2081 (27.54) | ||
| Stroke | Yes | 142 (1.78) | 86 (60.56) | 56 (39.44) | 0.003 |
| No | 7845 (98.22) | 5628 (71.74) | 2217 (28.26) | ||
| Urarthritis | Yes | 413 (5.17) | 235 (56.90) | 178 (43.10) | <0.001 |
| No | 7574 (94.83) | 372 (48.75) | 362 (47.44) | ||
| Chronic bronchitis | Yes | 513 (6.42) | 311 (60.62) | 202 (39.38) | <0.001 |
| No | 7474 (93.58) | 5403 (72.29) | 2071 (27.71) | ||
| Asthma | Yes | 166 (2.08) | 94 (56.63) | 72 (43.37) | <0.001 |
| No | 7821 (97.92) | 5620 (71.86) | 2201 (28.14) | ||
| Kidney disease | Yes | 981 (12.28) | 592 (60.35) | 389 (39.65) | <0.001 |
| No | 7006 (87.72) | 5122 (73.11) | 1884 (26.89) | ||
| Cancer | Yes | 57 (0.71) | 31 (54.39) | 26 (45.61) | <0.001 |
| No | 7930 (99.29) | 5683 (71.66) | 2247 (28.34) | ||
| Schizophrenia | Yes | 22 (0.28) | 11 (50.00) | 11 (50.00) | 0.025 |
| No | 7965 (99.72) | 5703 (71.60) | 2262 (28.40) | ||
| Parkinson’s disease | Yes | 46 (0.58) | 22 (47.83) | 24 (52.17) | <0.001 |
| No | 7941 (99.42) | 5692 (71.68) | 2249 (28.32) | ||
| Alzheimer’s disease | Yes | 20 (0.25) | 13 (65.00) | 7 (35.00) | 0.516 |
| No | 7967 (99.75) | 5701 (71.56) | 2266 (28.44) | ||
| Depressive disorder | Yes | 31 (0.39) | 10 (32.26) | 21 (67.74) | <0.001 |
| No | 7956 (99.61) | 5704 (71.69) | 2252 (28.31) | ||
| Dietary Pattern Score | Minimum | Quartiles | Maximum | ||
|---|---|---|---|---|---|
| 25th Percentile | Median | 75th Percentile | |||
| CHEI | 20.85 | 49.7 | 57.33 | 64.85 | 84.09 |
| DASH | 9.50 | 21.50 | 24.50 | 27.50 | 37.50 |
| MDS | 0.00 | 4.00 | 5.00 | 6.00 | 9.00 |
| Factor 1: Protein-rich and vegetables | −2.71 | −0.71 | −0.22 | 0.5 | 7.62 |
| Factor 2: Dairy and fruits | −8.84 | −0.59 | −0.1 | 0.51 | 7.97 |
| Factor 3: Snacks, salted food and nuts | −8.02 | −0.64 | −0.23 | 0.39 | 10.86 |
| Factor 4: Beverages | −3.71 | −0.45 | −0.23 | 0.08 | 13.20 |
| Dietary Pattern Score | Q1 | Q2 | Q3 | Q4 | p Value a |
|---|---|---|---|---|---|
| CHEI, Medians | 44.56 | 53.52 | 61.01 | 69.53 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1339 (67.0) | 1423 (71.3) | 1456 (72.9) | 1496 (74.9) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 659 (33.0) | 572 (28.7) | 542 (27.1) | 500 (25.1) | <0.001 |
| DASH, Medians | 20.50 | 23.50 | 26.50 | 29.50 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1534 (68.6) | 1579 (71.2) | 1462 (73.2) | 1139 (74.2) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 702 (31.4) | 640 (28.8) | 534 (26.8) | 397 (25.8) | <0.001 |
| MDS, Medians | 3.00 | 5.00 | 6.00 | 7.00 | |
| Good Sleep Quality (PQIS < 5), n (%) | 2406 (68.1) | 1146 (72.7) | 1128 (75.2) | 1034 (75.0) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 1125 (31.9) | 431 (27.3) | 372 (24.8) | 345 (25.0) | <0.001 |
| Factor 1: Protein-rich and vegetables, Medians | −0.97 | −0.47 | 0.08 | 1.12 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1368 (68.5) | 1417 (70.9) | 1458 (73.0) | 1471 (73.7) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 628 (31.5) | 581 (29.1) | 538 (27.0) | 526 (26.3) | <0.001 |
| Factor 2: Dairy and fruits, Medians | −0.96 | −0.33 | 0.17 | 1.08 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1440 (72.1) | 1365 (68.4) | 1455 (72.8) | 1454 (72.8) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 556 (27.9) | 632 (31.6) | 543 (27.2) | 542 (27.2) | 0.003 |
| Factor 3: Snacks, salted food and nuts, Medians | −0.85 | −0.44 | 0.04 | 1.32 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1442 (72.2) | 1417 (70.9) | 1417 (71.0) | 1438 (72.0) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 554 (27.8) | 581 (29.1) | 579 (29.0) | 559 (28.0) | 0.712 |
| Factor 4: Beverages, Medians | −0.63 | −0.33 | −0.11 | 1.16 | |
| Good Sleep Quality (PQIS < 5), n (%) | 1452 (72.7) | 1405 (70.4) | 1409 (70.6) | 1448 (72.5) | |
| Poor Sleep Quality (PQIS ≥ 5), n (%) | 545 (27.3) | 592 (29.6) | 588 (29.4) | 548 (27.5) | 0.199 |
| Dietary Pattern Score | Model 1 a | Model 2 b | Model 3 c | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| CHEI | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 0.817 | 0.714–0.934 | 0.003 | 0.896 | 0.781–1.029 | 0.121 | 0.933 | 0.810–1.074 | 0.331 |
| Q3 | 0.756 | 0.660–0.866 | <0.001 | 0.83 | 0.720–0.956 | 0.010 | 0.875 | 0.757–1.011 | 0.069 |
| Q4 | 0.679 | 0.592–0.779 | <0.001 | 0.742 | 0.640–0.860 | <0.001 | 0.811 | 0.696–0.945 | 0.007 |
| DASH | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 0.886 | 0.779–1.007 | 0.063 | 0.817 | 0.717–0.932 | 0.003 | 0.833 | 0.729–0.952 | 0.007 |
| Q3 | 0.798 | 0.698–0.912 | 0.001 | 0.721 | 0.628–0.828 | <0.001 | 0.758 | 0.659–0.873 | <0.001 |
| Q4 | 0.762 | 0.659–0.880 | <0.001 | 0.667 | 0.574–0.776 | <0.001 | 0.704 | 0.603–0.823 | <0.001 |
| MDS | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 0.804 | 0.705–0.917 | 0.001 | 0.796 | 0.695–0.910 | 0.001 | 0.819 | 0.714–0.938 | 0.004 |
| Q3 | 0.705 | 0.615–0.809 | <0.001 | 0.710 | 0.616–0.818 | <0.001 | 0.744 | 0.644–0.859 | <0.001 |
| Q4 | 0.714 | 0.620–0.822 | <0.001 | 0.705 | 0.609–0.817 | <0.001 | 0.747 | 0.643–0.867 | <0.001 |
| Factor 1: Protein-rich and vegetables | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 0.893 | 0.780–1.022 | 0.101 | 1.012 | 0.881–1.163 | 0.865 | 1.073 | 0.931–1.236 | 0.329 |
| Q3 | 0.804 | 0.701–0.922 | 0.002 | 0.947 | 0.822–1.091 | 0.447 | 1.014 | 0.877–1.172 | 0.854 |
| Q4 | 0.779 | 0.679–0.894 | <0.001 | 1.000 | 0.864–1.158 | 0.999 | 1.061 | 0.913–1.232 | 0.44 |
| Factor 2: Dairy and fruits | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 1.036 | 0.901–1.190 | 0.62 | 1.072 | 0.932–1.233 | 0.332 | 1.048 | 0.907–1.210 | 0.527 |
| Q3 | 1.242 | 1.084–1.424 | 0.002 | 0.859 | 0.741–0.996 | 0.045 | 0.875 | 0.752–1.019 | 0.086 |
| Q4 | 1.001 | 0.871–1.151 | 0.987 | 0.868 | 0.745–1.011 | 0.069 | 0.913 | 0.780–1.069 | 0.259 |
| Factor 3: Snacks, salted food and nuts | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 1.067 | 0.930–1.225 | 0.354 | 1.056 | 0.919–1.213 | 0.446 | 1.071 | 0.930–1.233 | 0.342 |
| Q3 | 1.064 | 0.927–1.221 | 0.38 | 1.040 | 0.905–1.195 | 0.584 | 1.06 | 0.921–1.222 | 0.416 |
| Q4 | 1.012 | 0.881–1.162 | 0.868 | 0.936 | 0.813–1.077 | 0.354 | 0.972 | 0.843–1.121 | 0.696 |
| Factor 4: Beverages | |||||||||
| Q1 | Reference | Reference | Reference | ||||||
| Q2 | 1.123 | 0.978–1.288 | 0.099 | 1.097 | 0.955–1.261 | 0.189 | 1.083 | 0.940–1.247 | 0.27 |
| Q3 | 1.112 | 0.969–1.276 | 0.131 | 1.048 | 0.912–1.205 | 0.508 | 1.046 | 0.907–1.206 | 0.538 |
| Q4 | 1.008 | 0.877–1.159 | 0.907 | 1.165 | 1.010–1.345 | 0.037 | 1.180 | 1.020–1.266 | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.; Jiang, Y.; Sun, Z.; Wu, Y.; Yao, C.; Yang, L.; Tang, M.; Wang, W.; Lei, N.; He, G.; et al. Healthier Dietary Patterns Are Associated with Better Sleep Quality among Shanghai Suburban Adults: A Cross-Sectional Study. Nutrients 2024, 16, 1165. https://doi.org/10.3390/nu16081165
Huang L, Jiang Y, Sun Z, Wu Y, Yao C, Yang L, Tang M, Wang W, Lei N, He G, et al. Healthier Dietary Patterns Are Associated with Better Sleep Quality among Shanghai Suburban Adults: A Cross-Sectional Study. Nutrients. 2024; 16(8):1165. https://doi.org/10.3390/nu16081165
Chicago/Turabian StyleHuang, Li, Yonggen Jiang, Zhongxing Sun, Yiling Wu, Chunxia Yao, Lihua Yang, Minhua Tang, Wei Wang, Nian Lei, Gengsheng He, and et al. 2024. "Healthier Dietary Patterns Are Associated with Better Sleep Quality among Shanghai Suburban Adults: A Cross-Sectional Study" Nutrients 16, no. 8: 1165. https://doi.org/10.3390/nu16081165
APA StyleHuang, L., Jiang, Y., Sun, Z., Wu, Y., Yao, C., Yang, L., Tang, M., Wang, W., Lei, N., He, G., Chen, B., Huang, Y., & Zhao, G. (2024). Healthier Dietary Patterns Are Associated with Better Sleep Quality among Shanghai Suburban Adults: A Cross-Sectional Study. Nutrients, 16(8), 1165. https://doi.org/10.3390/nu16081165