
Reproducibility and Relative Validity of a Short Food Frequency Questionnaire for Chinese Older Adults in Hong Kong
 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Dietary Assessments
2.4. Statistical Analyses
3. Results
3.1. Demographic Characteristics
3.2. Dietary Intakes of the Included Participants
3.3. Reproducibility of the Short FFQ and Its Relative Validity with Three-Day Dietary Records
3.3.1. Reproducibility of the Short FFQ
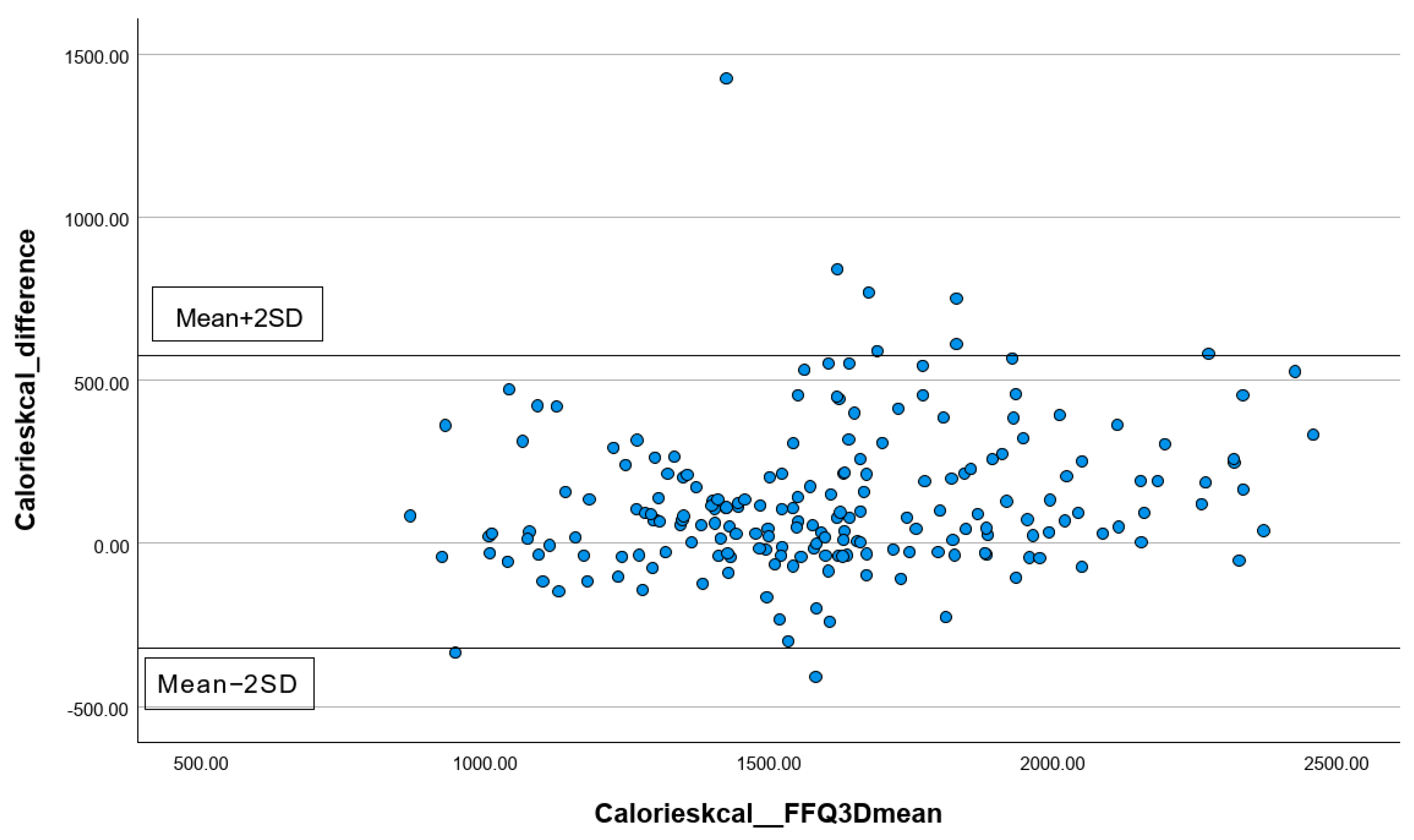
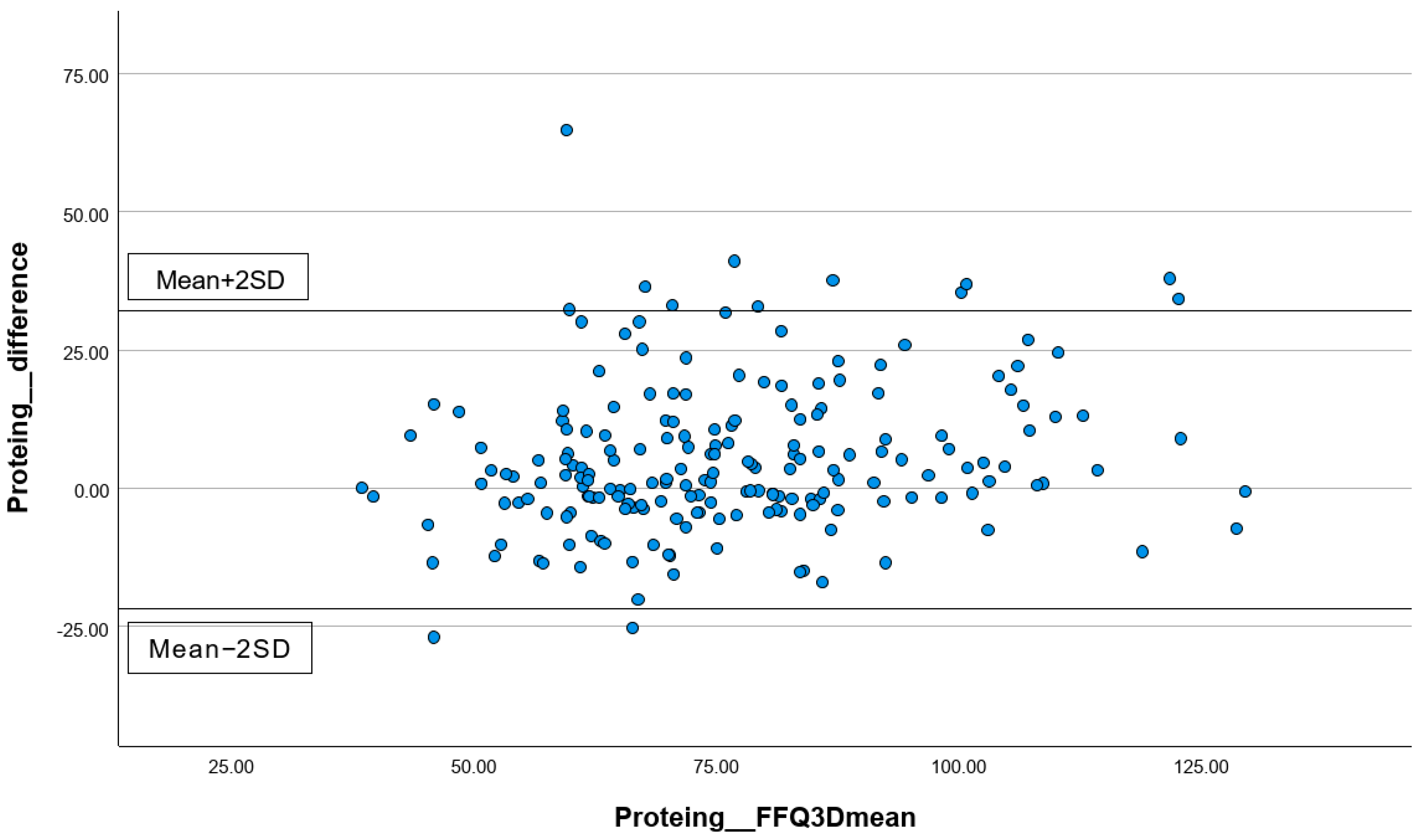
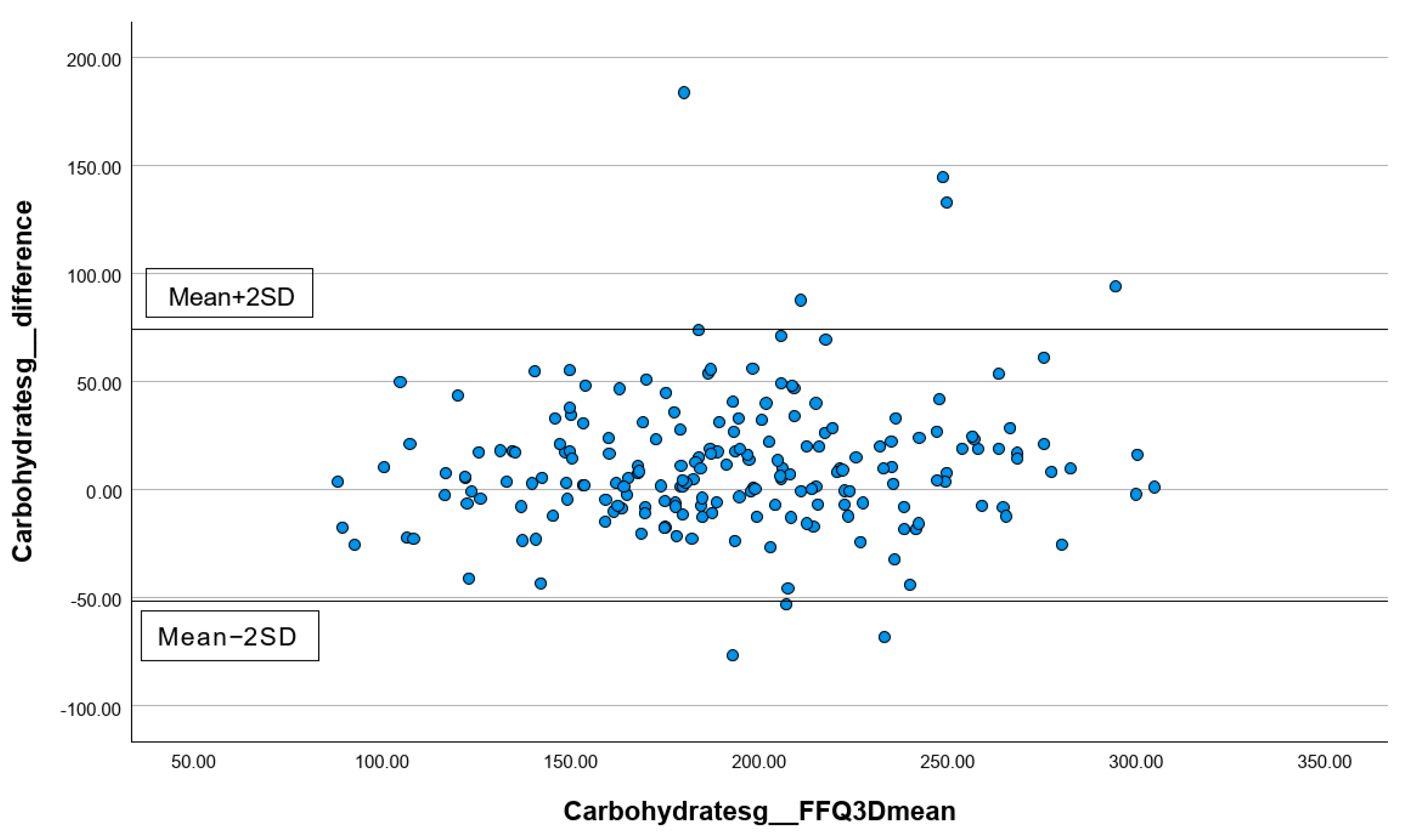
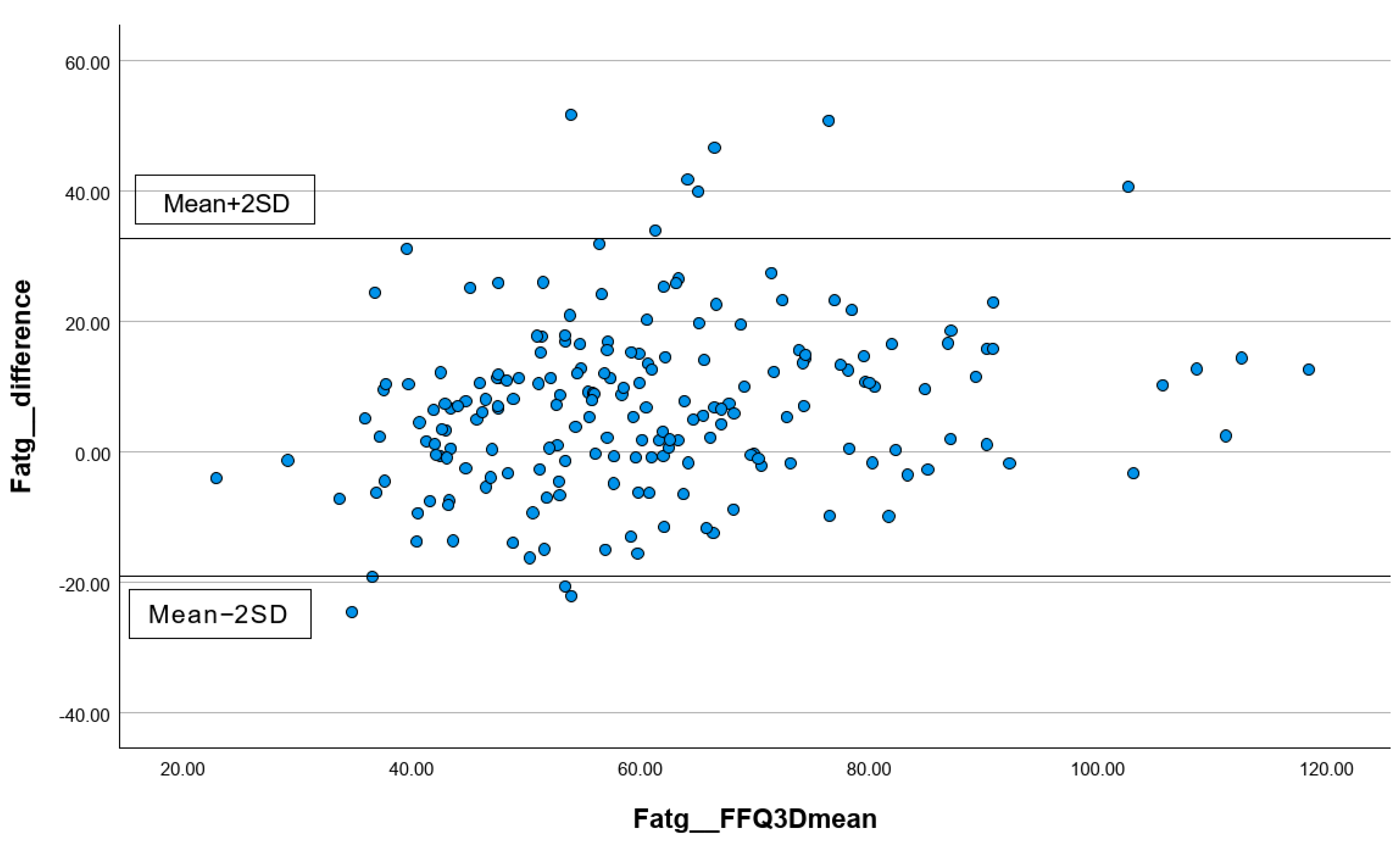
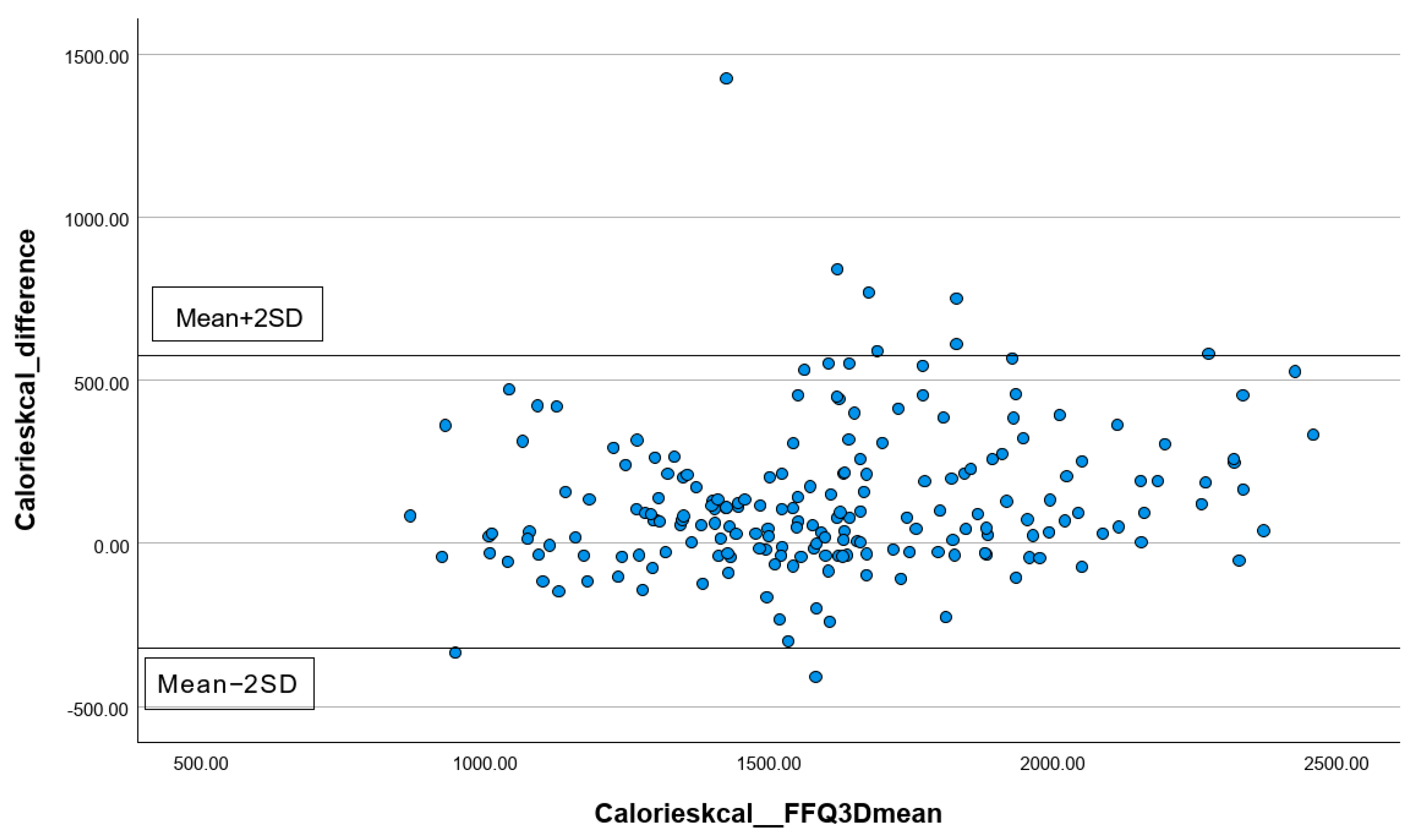
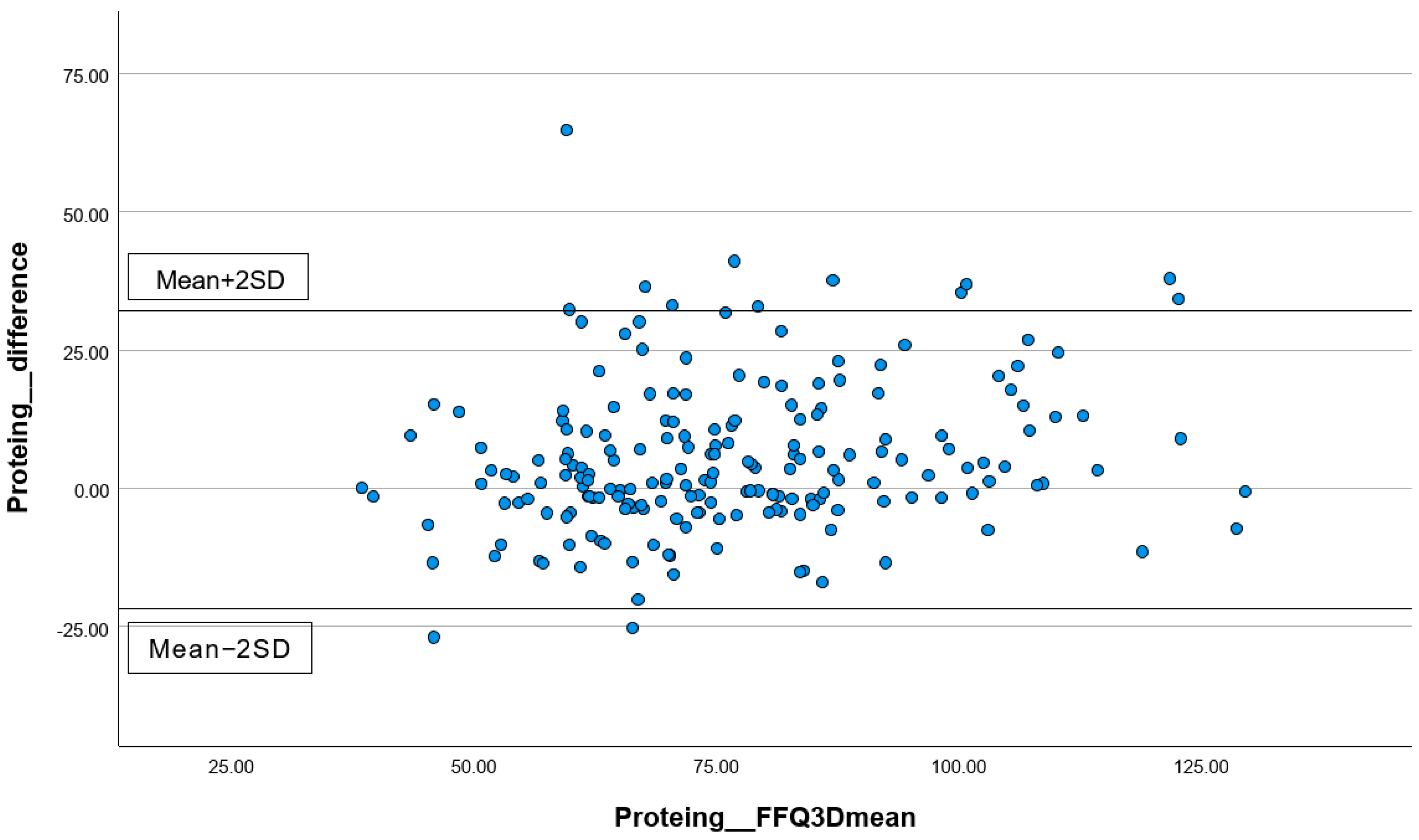
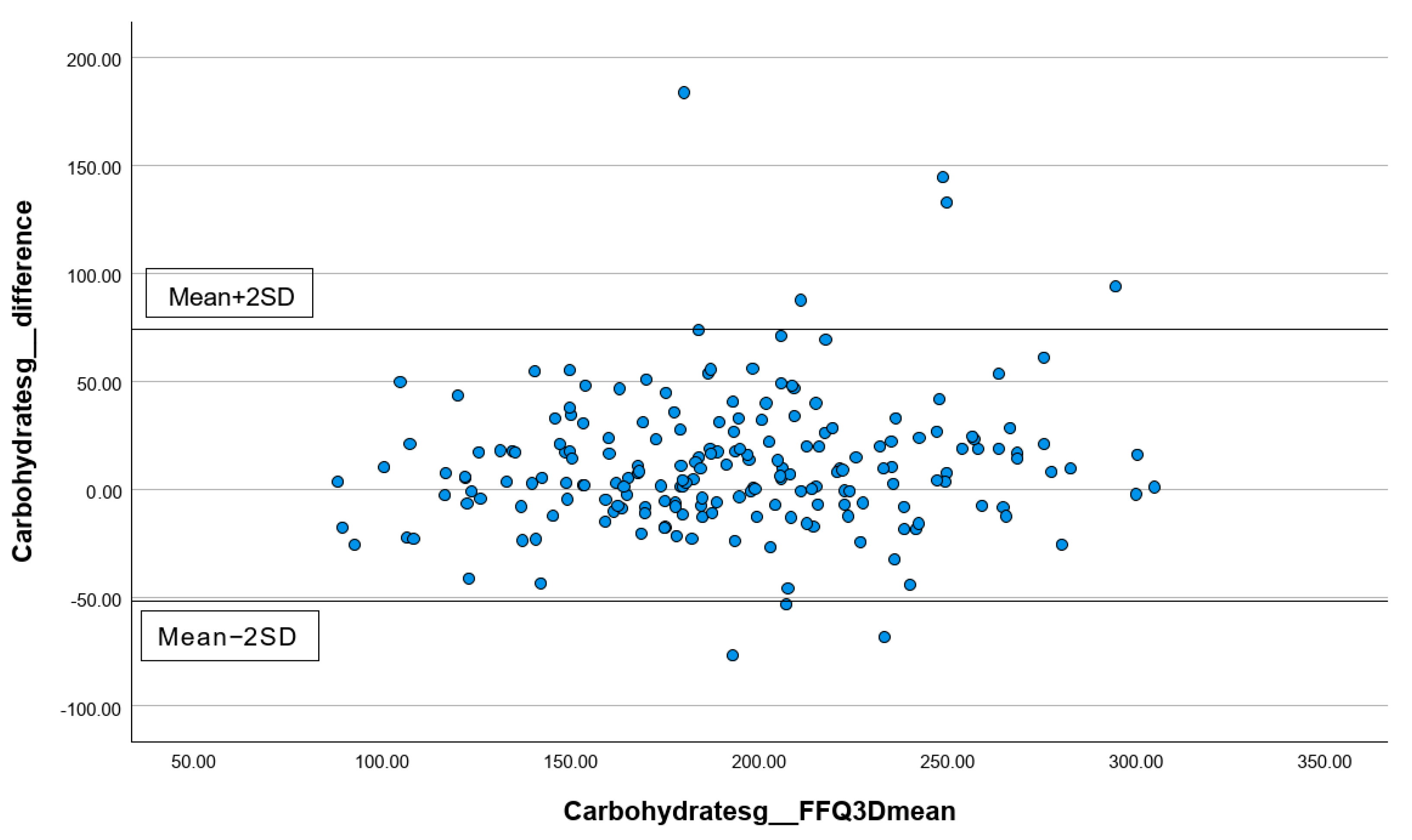
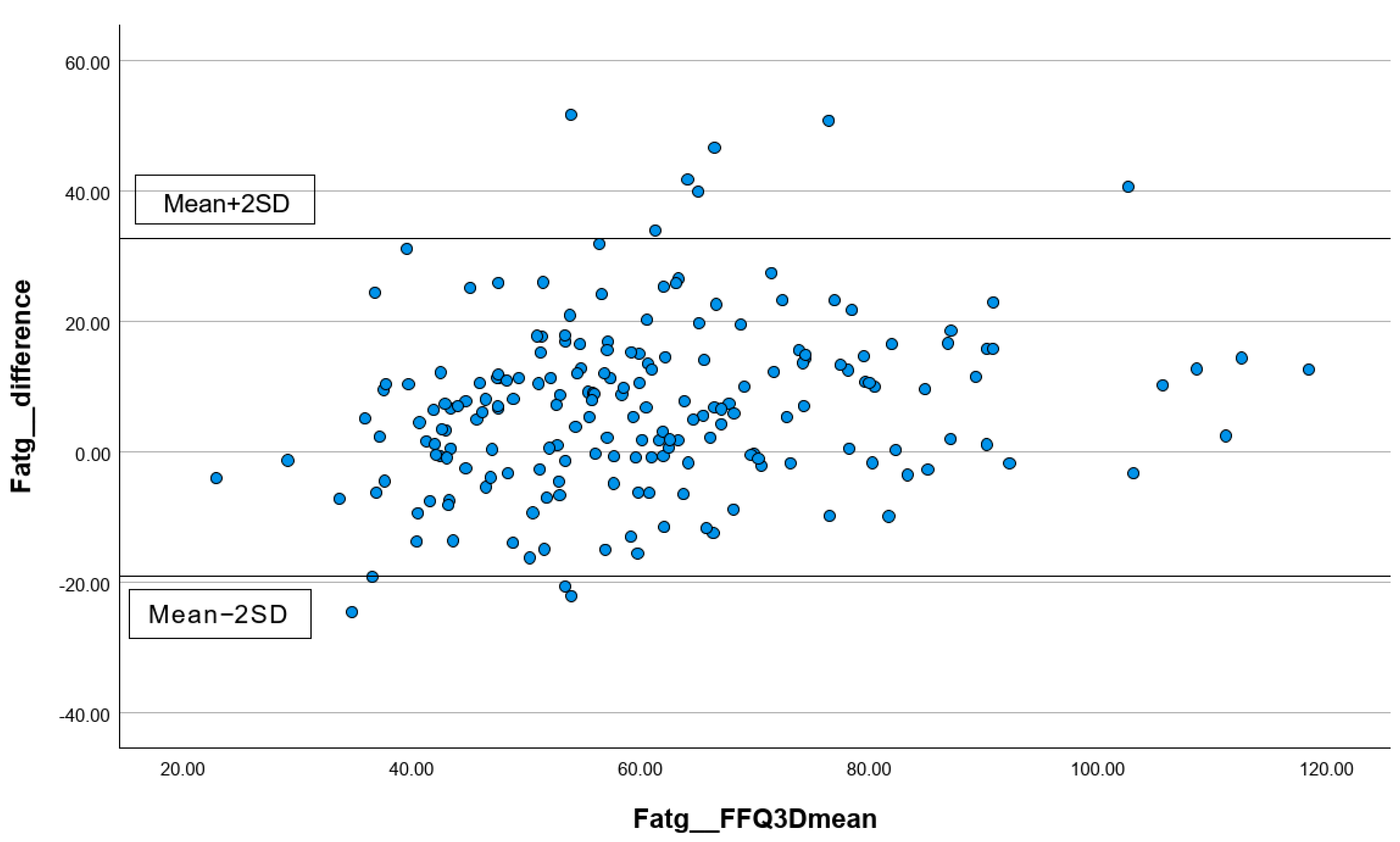
3.3.2. Analyzing the Consistency of Dietary Data Reported by FFQs and Three-Day Dietary Records Using Bland–Altman Plots
3.3.3. Correlations between the Short FFQ1 and Three-Day Dietary Records
3.3.4. Cross-Classification of Dietary Intakes between FFQ1 and Three-Day Dietary Records
3.3.5. One-Sample t-Tests and Linear Regression Analyses for FFQ1 and Three-Day Dietary Records
4. Discussion
4.1. Summary of Main Findings
4.2. Dietary Intakes of the Included Participants
4.3. Reproducibility and Relative Validity of the Short FFQ
4.4. Comparison between the Previous and Current Short FFQs Used in the Hong Kong Community
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Pilgrim, A.L.; Robinson, S.M.; Sayer, A.A.; Roberts, H.C. An overview of appetite decline in older people. Nurs. Older People 2015, 27, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.M.H.; So, W.K.W.; Choi, K.C.; Cheung, R.; Chan, H.Y.L.; Sit, J.W.H.; Ho, B.; Li, F.; Lee, T.Y.; Chair, S.Y. Malnutrition risks and their associated factors among home-living older Chinese adults in Hong Kong: Hidden problems in an affluent Chinese community. BMC Geriatr. 2019, 19, 138. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, S.S.; Wang, J.W.; Liu, S.H.; Chen, S.M.; Li, X.H.; Yang, S.S.; Liu, M.; He, Y. Prevalence of malnutrition among elderly in the community of China: A Meta-analysis. Zhonghua Liu Xing Bing. Xue Za Zhi 2022, 43, 915–921. [Google Scholar] [CrossRef]
- Malnutrition. Available online: https://www.who.int/news-room/questions-and-answers/item/malnutrition (accessed on 19 March 2024).
- Lopez-Jaramillo, P.; Gomez-Arbelaez, D.; Sotomayor-Rubio, A.; Mantilla-Garcia, D.; Lopez-Lopez, J. Maternal undernutrition and cardiometabolic disease: A Latin American perspective. BMC Med. 2015, 13, 41. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, D.; Büyükkoyuncu Pekel, N.; Kiliç, A.K.; Tolgay, E.N.; Tufan, F. Malnutrition is associated with dementia severity and geriatric syndromes in patients with Alzheimer disease. Turk. J. Med. Sci. 2015, 45, 1078–1081. [Google Scholar] [CrossRef] [PubMed]
- Zahangir, M.S.; Hasan, M.M.; Richardson, A.; Tabassum, S. Malnutrition and non-communicable diseases among Bangladeshi women: An urban-rural comparison. Nutr. Diabetes 2017, 7, e250. [Google Scholar] [CrossRef] [PubMed]
- Hurrle, S.; Hsu, W.H. The etiology of oxidative stress in insulin resistance. Biomed. J. 2017, 40, 257–262. [Google Scholar] [CrossRef]
- The Government of the Hong Kong Special Administrative Region. Towards 2025: Strategy and Action Plan to Prevent and Control Non-Communicable Diseases in Hong Kong. Available online: https://www.chp.gov.hk/files/pdf/saptowards2025_fullreport_en.pdf (accessed on 8 April 2024).
- Your Health, Your Life: Report on First Stage Public Consultation on Healthcare Reform. Available online: https://www.healthbureau.gov.hk/beStrong/files/consultation/HCR_Report_eng.pdf (accessed on 4 March 2024).
- Eysteinsdottir, T.; Thorsdottir, I.; Gunnarsdottir, I.; Steingrimsdottir, L. Assessing validity of a short food frequency questionnaire on present dietary intake of elderly Icelanders. Nutr. J. 2012, 11, 12. [Google Scholar] [CrossRef]
- Chan, V.W.; Chan, C.Y.; Hoi, B.P.; Chan, J.H.; Li, L.; Li, M.Y.; Chung, E.S.; Sin, H.H.; Wong, E.L.; Lo, K.K. Relative Validity of a Short Food Frequency Questionnaire for Disadvantaged Families in Hong Kong. Nutrients 2023, 15, 2668. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Y.; Hoi, B.P.; Wong, E.L. Lay health worker intervention in pre-diabetes management: Study protocol of a pragmatic randomized controlled trial for Chinese families living in inadequate houses. Front. Public Health 2022, 10, 957754. [Google Scholar] [CrossRef]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef]
- Nielsen, D.E.; Boucher, B.A.; Da Costa, L.A.; Jenkins, D.J.A.; El-Sohemy, A. Reproducibility and validity of the Toronto-modified Harvard food frequency questionnaire in a multi-ethnic sample of young adults. Eur. J. Clin. Nutr. 2023, 77, 246–254. [Google Scholar] [CrossRef]
- Syauqy, A.; Afifah, D.N.; Purwanti, R.; Nissa, C.; Fitranti, D.Y.; Chao, J.C. Reproducibility and Validity of a Food Frequency Questionnaire (FFQ) Developed for Middle-Aged and Older Adults in Semarang, Indonesia. Nutrients 2021, 13, 4163. [Google Scholar] [CrossRef]
- Vioque, J.; Gimenez-Monzo, D.; Navarrete-Muñoz, E.M.; Garcia-de-la-Hera, M.; Gonzalez-Palacios, S.; Rebagliato, M.; Ballester, F.; Murcia, M.; Iñiguez, C.; Granado, F. Reproducibility and Validity of a Food Frequency Questionnaire Designed to Assess Diet in Children Aged 4–5 Years. PLoS ONE 2016, 11, e0167338. [Google Scholar] [CrossRef]
- Luo, H.; Wong, G.H.; Lum, T.Y.; Luo, M.; Gong, C.H.; Kendig, H. Health Expectancies in Adults Aged 50 Years or Older in China. J. Aging Health 2016, 28, 758–774. [Google Scholar] [CrossRef]
- Woo, J.; Chan, R.; Ong, S.; Bragt, M.; Bos, R.; Parikh, P.; de Groot, L.C. Randomized Controlled Trial of Exercise and Nutrition Supplementation on Physical and Cognitive Function in Older Chinese Adults Aged 50 Years and Older. J. Am. Med. Dir. Assoc. 2020, 21, 395–403. [Google Scholar] [CrossRef]
- Wu, F.; Guo, Y.; Kowal, P.; Jiang, Y.; Yu, M.; Li, X.; Zheng, Y.; Xu, J. Prevalence of major chronic conditions among older Chinese adults: The Study on Global AGEing and adult health (SAGE) wave 1. PLoS ONE 2013, 8, e74176. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Use of Electronic Informed Consent Questions and Answers. 2016. Available online: https://www.fda.gov/media/116850/download (accessed on 8 April 2024).
- Nicol, G.E.; Piccirillo, J.F.; Mulsant, B.H.; Lenze, E.J. Action at a Distance: Geriatric Research during a Pandemic. J. Am. Geriatr. Soc. 2020, 68, 922–925. [Google Scholar] [CrossRef] [PubMed]
- Skelton, E.; Drey, N.; Rutherford, M.; Ayers, S.; Malamateniou, C. Electronic consenting for conducting research remotely: A review of current practice and key recommendations for using e-consenting. Int. J. Med. Inform. 2020, 143, 104271. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Leung, S.S.F.; Ho, S.C.; Lam, T.H.; Janus, E.D. A food frequency questionnaire for use in the Chinese population in Hong Kong: Description and examination of validity. Nutr. Res. 1997, 17, 1633–1641. [Google Scholar] [CrossRef]
- Tokudome, S.; Goto, C.; Imaeda, N.; Tokudome, Y.; Ikeda, M.; Maki, S. Development of a data-based short food frequency questionnaire for assessing nutrient intake by middle-aged Japanese. Asian Pac. J. Cancer Prev. 2004, 5, 40–43. [Google Scholar]
- Zhao, W.; Hasegawa, K.; Chen, J. The use of food-frequency questionnaires for various purposes in China. Public Health Nutr. 2002, 5, 829–833. [Google Scholar] [CrossRef]
- Mina, K.; Fritschi, L.; Knuiman, M. A valid semiquantitative food frequency questionnaire to measure fish consumption. Eur. J. Clin. Nutr. 2007, 61, 1023–1031. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Willet, W.C. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Guidelines Review Committee. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Surveillance and Epidemiology Branch. Report of Population Health Survey 2014/2015; Centre for Health Protection, Department of Health, Hong Kong Special Administrative Region Government: Hong Kong, China, 2017. [Google Scholar]
- Salt Iodisation: A Practical Guide for Salt Importers, Wholesalers and Retailers. Available online: https://www.cfs.gov.hk/english/programme/programme_fii/files/Food_Iodisation_e.pdf (accessed on 2 April 2024).
- Universal Salt Iodization and Sodium Intake Reduction: Compatible, Cost-Effective Strategies of Great Public Health Benefit. Available online: https://www.who.int/publications/i/item/9789240053717 (accessed on 2 April 2024).
- Population Health Survey 2020–2022: Thematic Report on Lodine Status. Available online: https://www.chp.gov.hk/files/pdf/dh_phs_2020-22_iodine_report_eng.pdf (accessed on 2 April 2024).
- Dietary Macro- and Micro-Nutrient Recommended Intake of Chinese People. Available online: http://www.nhc.gov.cn/wjw/yingyang/wsbz.shtml (accessed on 12 February 2024).
- Zhang, H.R.; Yang, Y.; Tian, W.; Sun, Y.J. Dietary Fiber and All-Cause and Cardiovascular Mortality in Older Adults with Hypertension: A Cohort Study Of NHANES. J. Nutr. Health Aging 2022, 26, 407–414. [Google Scholar] [CrossRef]
- The First Hong. Kong Total Diet. Study: Minerals. Available online: https://www.cfs.gov.hk/english/programme/programme_firm/files/Report_on_the_1st_HK_Total_Diet_Study_Minerals_e.pdf (accessed on 3 March 2024).
- Ye, K.X.; Sun, L.; Lim, S.L.; Li, J.; Kennedy, B.K.; Maier, A.B.; Feng, L. Adequacy of Nutrient Intake and Malnutrition Risk in Older Adults: Findings from the Diet and Healthy Aging Cohort Study. Nutrients 2023, 15, 3446. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zhang, Y.; Liu, Y.; Zhang, J.; Lu, J.; Wang, X.; Zhang, N.; Ma, G. Analysis on fluid intake and urination behaviors among the elderly in five cities in China: A cross-sectional study. Front. Nutr. 2023, 10, 1280098. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Standing Committee on the Scientific Evaluation of Dietary Reference, Intakes. The National Academies Collection: Reports funded by National Institutes of Health. In Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academies Press: Washington, DC, USA, 1997. [Google Scholar]
- Lovell, A.L.; Davies, P.S.W.; Hill, R.J.; Milne, T.; Matsuyama, M.; Jiang, Y.; Chen, R.X.; Heath, A.M.; Grant, C.C.; Wall, C.R. Validation and calibration of the Eating Assessment in Toddlers FFQ (EAT FFQ) for children, used in the Growing Up Milk—Lite (GUMLi) randomised controlled trial. Br. J. Nutr. 2021, 125, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Food Forum. The National Academies Collection: Reports funded by National Institutes of Health. In Providing Healthy and Safe Foods As We Age: Workshop Summary; National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Goodwill, A.M.; Szoeke, C. A Systematic Review and Meta-Analysis of The Effect of Low Vitamin D on Cognition. J. Am. Geriatr. Soc. 2017, 65, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Gioia, G.; Rossi Fanelli, F.; Muscaritoli, M. The role for dietary omega-3 fatty acids supplementation in older adults. Nutrients 2014, 6, 4058–4072. [Google Scholar] [CrossRef]
- Kjeldby, I.K.; Fosnes, G.S.; Ligaarden, S.C.; Farup, P.G. Vitamin B6 deficiency and diseases in elderly people—A study in nursing homes. BMC Geriatr. 2013, 13, 13. [Google Scholar] [CrossRef]
- Butts, M.; Sundaram, V.L.; Murughiyan, U.; Borthakur, A.; Singh, S. The Influence of Alcohol Consumption on Intestinal Nutrient Absorption: A Comprehensive Review. Nutrients 2023, 15, 1571. [Google Scholar] [CrossRef]
- Godos, J.; Giampieri, F.; Chisari, E.; Micek, A.; Paladino, N.; Forbes-Hernández, T.Y.; Quiles, J.L.; Battino, M.; La Vignera, S.; Musumeci, G.; et al. Alcohol Consumption, Bone Mineral Density, and Risk of Osteoporotic Fractures: A Dose-Response Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1515. [Google Scholar] [CrossRef] [PubMed]
- Ramel, A.; Stenholm, S. Obesity and Health in Older Adults. In Interdisciplinary Nutritional Management and Care for Older Adults: An Evidence-Based Practical Guide for Nurses; Geirsdóttir, Ó.G., Bell, J.J., Eds.; Springer International Publishing: Cham, Switerland, 2021; pp. 207–214. [Google Scholar]
- Laclaustra, M.; Rodriguez-Artalejo, F.; Guallar-Castillon, P.; Banegas, J.R.; Graciani, A.; Garcia-Esquinas, E.; Ordovas, J.; Lopez-Garcia, E. Prospective association between added sugars and frailty in older adults. Am. J. Clin. Nutr. 2018, 107, 772–779. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean (±SD)/N (%) | ||
|---|---|---|---|
| Total (n = 198) | Male (n = 66) | Female (n = 132) | |
| Age (years) | 64.0 ± 6.0 | 66.0 ± 5.3 | 63.5 ± 5.7 |
| BMI at enrolment (kg/m2) | 22.8 ± 3.4 | 24.0 ± 3.1 | 22.0 ± 3.5 |
| Education | |||
| Junior Secondary or below | 29 (14.6%) | 5 (7.5%) | 24 (18.2%) |
| Senior Secondary | 62 (31.3%) | 17 (25.8%) | 45 (34.1%) |
| Post-Secondary | 36 (18.2%) | 13 (19.7%) | 23 (17.4%) |
| Tertiary or above | 71 (35.9%) | 31 (47.0%) | 40 (30.3%) |
| Marital status | |||
| Not married a | 72 (36.4%) | 13 (19.7%) | 59 (44.7%) |
| Married | 126 (63.6%) | 53 (80.3%) | 73 (55.3%) |
| Total family income (HKD) | |||
| <10,000 | 72 (36.4%) | 20 (30.3%) | 52 (39.4%) |
| 10,000–19,999 | 26 (13.1%) | 9 (13.6%) | 17 (12.9%) |
| 20,000–29,999 | 23 (11.6%) | 6 (9.1%) | 17 (12.9%) |
| 30,000–39,999 | 24 (12.1%) | 9 (13.6%) | 15 (11.4%) |
| >40,000 | 53 (26.8%) | 22 (33.3%) | 31 (23.5%) |
| Smoking status | |||
| Smoker | 5 (2.5%) | 3 (4.5%) | 2 (1.5%) |
| Former smoker | 13 (6.6%) | 11 (16.7%) | 2 (1.5%) |
| Never-smoker | 180 (90.9%) | 52 (78.8%) | 128 (97.0%) |
| Exercise habits | |||
| <1 time per week | 23 (11.6%) | 10 (15.2%) | 13 (9.8%) |
| 1–2 times per week | 37 (18.7%) | 12 (18.2%) | 25 (18.9%) |
| 3–4 times per week | 56 (28.3%) | 18 (27.3%) | 38 (28.8%) |
| >5 times per week | 82 (41.4%) | 26 (39.4%) | 56 (42.4%) |
| Supplement consumption frequency | |||
| <1 time per week | 76 (38.4%) | 32 (48.5%) | 44 (33.3%) |
| 1–2 times per week | 6 (3.0%) | 3 (4.5%) | 3 (2.3%) |
| 3–4 times per week | 13 (6.6%) | 2 (3.0%) | 11 (8.3%) |
| >5 times per week | 103 (52.0%) | 29 (43.9%) | 74 (56.1%) |
| Medical history b | |||
| None | 91 (46.0%) | 24 (36.4%) | 67 (50.8%) |
| Diabetes | 19 (9.6%) | 13 (19.7%) | 6 (4.5%) |
| Hypertension | 45 (22.7%) | 19 (28.8%) | 26 (19.7%) |
| Hyperlipidemia | 36 (18.2% | 14 (21.2%) | 22 (16.7%) |
| Arteriosclerosis | 2 (1.0%) | 2 (3.0%) | 0 (0%) |
| Stroke | 2 (1.0%) | 1 (1.5%) | 1 (0.8%) |
| Cancers | 8 (4.0%) | 2 (3.0%) | 6 (4.5%) |
| Others | 13 (6.6%) | 1 (1.5%) | 12 (9.1%) |
| FFQ completion time (minutes) | |||
| 1st FFQ | 33.9 ± 7.5 | 34.6 ± 7.7 | 33.6 ± 7.4 |
| 2nd FFQ | 27.3 ± 7.2 | 28.2 ± 8.1 | 26.9 ± 6.7 |
| Intervals between the two FFQs (days) | 25.1 ± 3.6 | 25.3 ± 3.8 | 25.0 ± 3.5 |
| Parameters | Prevalence (%) |
|---|---|
| Above DRIs | |
| Energy from Total Fat 2 | 74.8 |
| Energy from Saturated Fat 2 | 29.1 |
| Energy from Trans Fat 4 | 2.91 |
| Total Sugar 2 | 58.3 |
| Cholesterol 4 | 68.9 |
| Sodium 4 | 93.2 |
| Below DRIs | |
| Total Energy 1 | 68.9 |
| Protein 5 | 6.8 |
| Carbohydrates 5 | 3.9 |
| Total Dietary Fiber 3 | 84.5 |
| Water 3 | 64.1 |
| Vitamin C 5 | 32.0 |
| Calcium 5 | 74.8 |
| Copper 5 | 0.0 |
| Iron 5 | 35.0 |
| Magnesium 5 | 52.4 |
| Manganese 3 | 76.7 |
| Phosphorus 5 | 1.0 |
| Potassium 3 | 23.3 |
| Zinc 5 | 33.0 |
| Parameters | FFQ1 | FFQ2 | ICCs | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | Crude | Energy-Adjusted | |
| Energy (kcal) | 1541.2 | 334.0 | 1524.4 | 1321.6 | 1753.7 | 1536.5 | 331.8 | 1503.9 | 1315.3 | 1745.4 | 0.96 ** | -- |
| Energy from Total Fat (kcal) | 509.6 | 147.9 | 488.0 | 397.0 | 589.9 | 507.4 | 151.4 | 482.7 | 388.8 | 601.7 | 0.95 ** | -- |
| Energy from Saturated Fat (kcal) | 130.4 | 40.7 | 127.1 | 100.6 | 148.9 | 128.1 | 39.5 | 121.4 | 99.5 | 149.7 | 0.96 ** | -- |
| Energy from Trans Fat (kcal) | 3.5 | 2.1 | 3.0 | 2.1 | 4.3 | 3.5 | 2.1 | 2.9 | 2.1 | 4.2 | 0.90 ** | -- |
| Protein (g) | 73.8 | 17.9 | 72.2 | 61.0 | 83.7 | 72.7 | 17.7 | 70.5 | 60.8 | 83.1 | 0.94 ** | 0.93 ** |
| Carbohydrates (g) | 186.6 | 46.6 | 183.0 | 152.7 | 220.7 | 187.0 | 44.8 | 185.8 | 152.6 | 214.5 | 0.95 ** | 0.93 ** |
| Total Dietary Fiber (g) | 15.9 | 5.2 | 15.4 | 12.6 | 19.1 | 15.9 | 5.2 | 15.2 | 12.3 | 18.8 | 0.96 ** | 0.97 ** |
| Total Sugar (g) | 51.9 | 18.2 | 50.1 | 37.6 | 62.7 | 52.0 | 17.9 | 50.3 | 39.3 | 62.1 | 0.94 ** | 0.94 ** |
| Total Fat (g) | 56.9 | 16.6 | 54.3 | 44.3 | 65.8 | 56.7 | 17.0 | 53.8 | 43.5 | 67.3 | 0.95 ** | 0.93 ** |
| Saturated Fat (g) | 14.5 | 4.5 | 14.1 | 11.1 | 16.5 | 14.2 | 4.4 | 13.5 | 11.1 | 16.6 | 0.96 ** | 0.95 ** |
| Trans Fat (g) | 0.4 | 0.2 | 0.3 | 0.2 | 0.4 | 0.4 | 0.2 | 0.3 | 0.2 | 0.5 | 0.90 ** | 0.87 ** |
| Cholesterol (mg) | 290.2 | 93.1 | 286.1 | 218.6 | 353.1 | 287.4 | 92.9 | 278.7 | 219.5 | 349.3 | 0.94 ** | 0.94 ** |
| Water (g) | 2537.7 | 593.6 | 2488.9 | 2094.7 | 2894.9 | 2538.8 | 598.3 | 2462.8 | 2145.2 | 2878.6 | 0.93 ** | 0.92 ** |
| Vitamin C (mg) | 119.1 | 43.9 | 114.5 | 89.0 | 144.7 | 120.2 | 43.6 | 115.1 | 90.8 | 141.8 | 0.95 ** | 0.95 ** |
| Calcium (mg) | 685.9 | 224.9 | 631.5 | 547.0 | 803.5 | 653.7 | 221.4 | 653.7 | 537.5 | 774.6 | 0.94 ** | 0.95 ** |
| Copper (mg) | 1.0 | 0.3 | 0.9 | 0.7 | 1.1 | 0.9 | 0.3 | 0.9 | 0.7 | 1.1 | 0.93 ** | 0.94 ** |
| Iron (mg) | 11.5 | 4.5 | 10.4 | 8.7 | 13.3 | 11.1 | 4.0 | 10.4 | 8.2 | 13.4 | 0.93 ** | 0.92 ** |
| Magnesium (mg) | 281.2 | 79.1 | 266.9 | 233.4 | 326.2 | 279.1 | 78.1 | 267.5 | 222.8 | 318.2 | 0.96 ** | 0.97 ** |
| Manganese (mg) | 3.8 | 1.2 | 3.6 | 3.0 | 4.3 | 3.7 | 1.2 | 3.6 | 2.9 | 4.3 | 0.93 ** | 0.92 ** |
| Phosphorus (mg) | 1070.0 | 272.5 | 1032.8 | 891.3 | 1251.2 | 1058.6 | 270.0 | 1021.1 | 864.6 | 1206.1 | 0.94 ** | 0.95 ** |
| Potassium (mg) | 2183.3 | 589.9 | 2183.3 | 1837.9 | 2603.0 | 2249.6 | 598.6 | 2166.7 | 1859.12 | 2572.0 | 0.95 ** | 0.95 ** |
| Sodium (mg) | 2393.3 | 582.3 | 2441.3 | 1842.6 | 2813.1 | 2381.0 | 545.3 | 2484.1 | 1829.9 | 2779.5 | 0.85 ** | 0.82 ** |
| Zinc (mg) | 8.6 | 2.2 | 8.2 | 7.0 | 9.9 | 8.5 | 2.2 | 8.1 | 6.9 | 9.6 | 0.95 ** | 0.93 ** |
| Parameters | FFQ1 | FFQ2 | ICCs | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | Crude | Energy-Adjusted | |
| Condiments (g) | 16.4 | 5.9 | 21.3 | 10.7 | 21.3 | 18.6 | 5.5 | 21.3 | 10.7 | 21.3 | 0.81 ** | 0.81 ** |
| Grains (g) | 349.1 | 139.5 | 344.7 | 257.0 | 436.1 | 346.5 | 134.2 | 354.3 | 255.1 | 429.0 | 0.96 ** | 0.90 ** |
| Fruits (g) | 187.2 | 101.8 | 152.7 | 120.0 | 230.4 | 197.3 | 104.1 | 152.3 | 120.0 | 236.6 | 0.96 ** | 0.95 ** |
| Vegetables (g) | 245.7 | 122.3 | 240.0 | 170.0 | 310.3 | 266.2 | 120.9 | 236.4 | 165.5 | 315.0 | 0.94 ** | 0.93 ** |
| Meat, Poultry, Processed Meat, and Organ Meat (g) | 86.3 | 45.4 | 80.0 | 53.9 | 111.8 | 98.2 | 42.7 | 76.6 | 51.4 | 109.3 | 0.96 ** | 0.90 ** |
| Fish and Seafoods (g) | 45.9 | 31.6 | 43.7 | 23.1 | 58.0 | 50.6 | 33.4 | 41.6 | 19.8 | 57.9 | 0.89 ** | 0.88 ** |
| Eggs (g) | 37.7 | 21.3 | 38.8 | 25.0 | 50.0 | 35.4 | 22.2 | 40.0 | 25.0 | 50.0 | 0.94 ** | 0.94 ** |
| Dairy and Dairy Products (g) | 85.8 | 112.7 | 36.6 | 5.0 | 137.9 | 51.7 | 113.1 | 35.9 | 8.7 | 128.5 | 0.89 ** | 0.96 ** |
| Beverages (mL) | 57.6 | 144.5 | 19.4 | 0.0 | 61.9 | 89.8 | 142.9 | 27.0 | 0.0 | 85.6 | 0.95 ** | 0.95 ** |
| Tea or Coffee (mL) | 315.9 | 291.5 | 249.3 | 88.2 | 441.7 | 342.8 | 294.5 | 230.2 | 76.2 | 460.4 | 0.86 ** | 0.85 ** |
| Soy and Soy Products (g) | 78.4 | 85.6 | 50.9 | 21.0 | 92.4 | 52.9 | 83.5 | 44.8 | 23.2 | 96.6 | 0.93 ** | 0.93 ** |
| Legumes (g) | 15.5 | 19.1 | 7.2 | 3.6 | 21.6 | 10.1 | 15.1 | 8.2 | 3.6 | 18.9 | 0.76 ** | 0.75 ** |
| Nuts and Seeds (g) | 7.2 | 9.2 | 4.5 | 1.4 | 9.3 | 8.8 | 9.3 | 4.5 | 1.4 | 9.7 | 0.96 ** | 0.82 ** |
| Sugary Snacks (g) | 19.0 | 23.9 | 10.4 | 3.5 | 28.0 | 28.7 | 22.9 | 9.2 | 4.3 | 21.1 | 0.83 ** | 0.92 ** |
| Water (mL) | 1286.8 | 529.2 | 1295.4 | 967.8 | 1572.6 | 1282.9 | 526.4 | 1330.7 | 967.8 | 1572.6 | 0.92 ** | 0.92 ** |
| Savory Snacks (g) | 1.6 | 3.2 | 0.0 | 0.0 | 1.5 | 2.1 | 2.8 | 0.0 | 0.0 | 1.5 | 0.76 ** | 0.76 ** |
| Dim Sum (g) | 26.8 | 28.0 | 18.8 | 8.0 | 33.8 | 46.9 | 27.2 | 20.0 | 10.8 | 36.6 | 0.89 ** | 0.89 ** |
| Oil (mL) | 18.6 | 11.0 | 17.0 | 10.2 | 25.0 | 11.1 | 11.4 | 17.9 | 10.6 | 25.1 | 0.94 ** | 0.89 ** |
| Sugars (g) | 1.1 | 2.2 | 0.0 | 0.0 | 1.0 | 2.3 | 2.1 | 0.0 | 0.0 | 0.7 | 0.89 ** | 0.88 ** |
| Wine (mL) | 9.6 | 57.1 | 0.0 | 0.0 | 0.0 | 12.7 | 58.6 | 0.0 | 0.0 | 0.0 | 0.98 ** | 0.98 ** |
| Parameters | FFQ1 | Three-Day DRs | Pearson Correlation Coefficients | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | Crude | Energy-Adjusted | |
| Energy (kcal) | 1541.2 | 334.0 | 1524.4 | 1321.6 | 1753.7 | 1669.0 | 375.7 | 1614.7 | 1410.3 | 1935.2 | 0.81 ** | -- |
| Energy from Total Fat (kcal) | 509.6 | 147.9 | 488.0 | 397.0 | 589.9 | 572.4 | 173.1 | 554.5 | 443.3 | 682.6 | 0.75 ** | -- |
| Energy from Saturated Fat (kcal) | 130.4 | 40.7 | 127.1 | 100.6 | 148.9 | 150.7 | 56.4 | 141.3 | 111.8 | 184.6 | 0.72 ** | -- |
| Energy from Trans Fat (kcal) | 3.5 | 2.1 | 3.0 | 2.1 | 4.3 | 1.9 | 1.5 | 1.5 | 0.8 | 2.6 | 0.43 ** | -- |
| Protein (g) | 73.8 | 17.9 | 72.2 | 61.0 | 83.7 | 79.1 | 20.6 | 77.4 | 63.9 | 91.7 | 0.76 ** | 0.69 ** |
| Carbohydrates (g) | 186.6 | 46.6 | 183.0 | 152.7 | 220.7 | 197.8 | 50.0 | 195.6 | 165.3 | 229.4 | 0.79 ** | 0.70 ** |
| Total Dietary Fiber (g) | 15.9 | 5.2 | 15.4 | 12.6 | 19.1 | 17.1 | 5.7 | 16.0 | 13.0 | 20.8 | 0.78 ** | 0.79 ** |
| Total Sugar (g) | 51.9 | 18.2 | 50.1 | 37.6 | 62.7 | 51.5 | 19.3 | 51.0 | 36.2 | 62.4 | 0.68 ** | 0.67 ** |
| Total Fat (g) | 56.9 | 16.6 | 54.3 | 44.3 | 65.8 | 63.8 | 19.3 | 61.7 | 49.5 | 76.1 | 0.75 ** | 0.71 ** |
| Saturated Fat (g) | 14.5 | 4.5 | 14.1 | 11.1 | 16.5 | 16.7 | 6.3 | 15.7 | 12.4 | 20.5 | 0.72 ** | 0.67 ** |
| Trans Fat (g) | 0.4 | 0.2 | 0.3 | 0.2 | 0.4 | 0.2 | 0.2 | 0.2 | 0.1 | 0.3 | 0.43 ** | 0.36 ** |
| Cholesterol (mg) | 290.2 | 93.1 | 286.1 | 218.6 | 353.1 | 347.9 | 126.0 | 337.8 | 254.0 | 418.3 | 0.66 ** | 0.67 ** |
| Water (g) | 2537.7 | 593.6 | 2488.9 | 2094.7 | 2894.9 | 2543.7 | 629.6 | 2500.2 | 2095.1 | 2869.8 | 0.73 ** | 0.73 ** |
| Vitamin C (mg) | 119.1 | 43.9 | 114.5 | 89.0 | 144.7 | 126.2 | 64.9 | 119.2 | 74.4 | 162.6 | 0.61 ** | 0.57 ** |
| Calcium (mg) | 685.9 | 224.9 | 631.5 | 547.0 | 803.5 | 636.1 | 265.8 | 580.9 | 437.6 | 767.2 | 0.69 ** | 0.67 ** |
| Copper (mg) | 1.0 | 0.3 | 0.9 | 0.7 | 1.1 | 1.2 | 0.4 | 1.1 | 0.9 | 1.4 | 0.64 ** | 0.62 ** |
| Iron (mg) | 11.5 | 4.5 | 10.4 | 8.7 | 13.3 | 10.5 | 4.1 | 9.5 | 7.7 | 12.3 | 0.65 ** | 0.62 ** |
| Magnesium (mg) | 281.2 | 79.1 | 266.9 | 233.4 | 326.2 | 276.2 | 87.5 | 254.7 | 215.8 | 327.7 | 0.76 ** | 0.77 ** |
| Manganese (mg) | 3.8 | 1.2 | 3.6 | 3.0 | 4.3 | 3.2 | 1.4 | 3.0 | 2.3 | 4.0 | 0.68 ** | 0.65 ** |
| Phosphorus (mg) | 1070.0 | 272.5 | 1032.8 | 891.3 | 1251.2 | 1058.1 | 281.1 | 1042.0 | 844.3 | 1232.0 | 0.72 ** | 0.65 ** |
| Potassium (mg) | 2183.3 | 589.9 | 2183.3 | 1837.9 | 2603.0 | 2429.0 | 704.2 | 2337.6 | 1981.4 | 2900.2 | 0.73 ** | 0.72 ** |
| Sodium (mg) | 2393.3 | 582.3 | 2441.3 | 1842.6 | 2813.1 | 3032.4 | 840.5 | 2922.3 | 2461.3 | 3573.3 | 0.44 ** | 0.37 ** |
| Zinc (mg) | 8.6 | 2.2 | 8.2 | 7.0 | 9.9 | 8.9 | 3.6 | 8.3 | 6.7 | 10.3 | 0.49 ** | 0.21 ** |
| Parameters | FFQ1 | Three-Day DRs | Pearson Correlation Coefficients | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | 25th | 75th | Mean | SD | Median | 25th | 75th | Crude | Energy-Adjusted | |
| Condiments (g) | 16.4 | 5.9 | 21.3 | 10.7 | 21.3 | 18.6 | 9.9 | 16.1 | 12.4 | 21.3 | 0.19 ** | 0.18 * |
| Grains (g) | 349.1 | 139.5 | 344.7 | 257.0 | 436.1 | 346.5 | 139.1 | 337.5 | 240.6 | 436.0 | 0.80 ** | 0.73 ** |
| Fruits (g) | 187.2 | 101.8 | 152.7 | 120.0 | 230.4 | 197.3 | 115.1 | 195.3 | 121.5 | 256.9 | 0.80 ** | 0.79 ** |
| Vegetables (g) | 245.7 | 122.3 | 240.0 | 170.0 | 310.3 | 266.2 | 149.1 | 242.8 | 161.6 | 347.7 | 0.75 ** | 0.75 ** |
| Meat, Poultry, Processed Meat, and Organ Meat (g) | 86.3 | 45.4 | 80.0 | 53.9 | 111.8 | 98.2 | 55.6 | 87.9 | 55.3 | 135.4 | 0.66 ** | 0.60 ** |
| Fish and Seafoods (g) | 45.9 | 31.6 | 43.7 | 23.1 | 58.0 | 50.6 | 43.6 | 42.4 | 15.6 | 76.7 | 0.53 ** | 0.52 ** |
| Eggs (g) | 37.7 | 21.3 | 38.8 | 25.0 | 50.0 | 35.4 | 26.0 | 33.3 | 16.7 | 50.0 | 0.74 ** | 0.74 ** |
| Dairy and Dairy Products (g) | 85.8 | 112.7 | 36.6 | 5.0 | 137.9 | 51.7 | 98.2 | 10.7 | 0.0 | 61.3 | 0.69 ** | 0.69 ** |
| Beverages (mL) | 57.6 | 144.5 | 19.4 | 0.0 | 61.9 | 89.8 | 136.5 | 8.1 | 0.0 | 161.7 | 0.52 ** | 0.51 ** |
| Tea or Coffee (mL) | 315.9 | 291.5 | 249.3 | 88.2 | 441.7 | 342.8 | 362.7 | 251.7 | 80.1 | 510.4 | 0.68 ** | 0.68 ** |
| Soy and Soy Products (g) | 78.4 | 85.6 | 50.9 | 21.0 | 92.4 | 52.9 | 84.7 | 12.4 | 0.0 | 80.0 | 0.66 ** | 0.66 ** |
| Legumes (g) | 15.5 | 19.1 | 7.2 | 3.6 | 21.6 | 10.1 | 21.8 | 0.0 | 0.0 | 10.0 | 0.27 ** | 0.24 ** |
| Nuts and Seeds (g) | 7.2 | 9.2 | 4.5 | 1.4 | 9.3 | 8.8 | 13.9 | 3.2 | 0.0 | 12.0 | 0.71 ** | 0.70 ** |
| Sugary Snacks (g) | 19.0 | 23.9 | 10.4 | 3.5 | 28.0 | 28.7 | 38.8 | 14.1 | 0.0 | 40.0 | 0.36 ** | 0.34 ** |
| Water (mL) | 1286.8 | 529.2 | 1295.4 | 967.8 | 1572.6 | 1282.9 | 508.8 | 1282.2 | 961.6 | 1602.7 | 0.84 ** | 0.84 ** |
| Savory Snacks (g) | 1.6 | 3.2 | 0.0 | 0.0 | 1.5 | 2.1 | 7.6 | 0.0 | 0.0 | 0.0 | 0.16 * | 0.18 * |
| Dim Sum (g) | 26.8 | 28.0 | 18.8 | 8.0 | 33.8 | 46.9 | 59.7 | 33.3 | 0.0 | 75.4 | 0.46 ** | 0.44 ** |
| Oil (mL) | 18.6 | 11.0 | 17.0 | 10.2 | 25.0 | 11.1 | 7.9 | 9.2 | 5.9 | 14.8 | 0.61 ** | 0.54 ** |
| Sugars (g) | 1.1 | 2.2 | 0.0 | 0.0 | 1.0 | 2.3 | 4.2 | 0.2 | 0.0 | 2.4 | 0.50 ** | 0.49 ** |
| Wine (mL) | 9.6 | 57.1 | 0.0 | 0.0 | 0.0 | 12.7 | 70.8 | 0.0 | 0.0 | 0.0 | 0.87 ** | 0.87 ** |
| Parameters | Crude a | Adjusted for Energy a | ||||
|---|---|---|---|---|---|---|
| Same Quartile | Adjacent Quartile b | Extreme Quartile c | Same Quartile | Adjacent Quartile b | Extreme Quartile c | |
| Energy (kcal) | 61.6 | 33.3 | 5.1 | -- | -- | -- |
| Energy from Total Fat (kcal) | 52.5 | 35.9 | 11.6 | -- | -- | -- |
| Energy from Saturated Fat (kcal) | 46.0 | 40.9 | 13.1 | -- | -- | -- |
| Energy from Trans Fat (kcal) | 44.4 | 35.4 | 20.2 | -- | -- | -- |
| Protein (g) | 52.0 | 37.9 | 10.1 | 44.9 | 41.9 | 13.1 |
| Carbohydrates (g) | 62.6 | 32.3 | 5.1 | 37.4 | 32.3 | 30.3 |
| Total Dietary Fiber (g) | 49.5 | 41.4 | 9.1 | 53.0 | 39.4 | 7.6 |
| Total Sugar (g) | 43.4 | 43.9 | 12.6 | 42.9 | 41.9 | 15.2 |
| Total Fat (g) | 52.5 | 35.9 | 11.6 | 44.4 | 42.9 | 12.6 |
| Saturated Fat (g) | 46.0 | 40.9 | 13.1 | 51.5 | 35.9 | 12.6 |
| Trans Fat (g) | 44.4 | 35.4 | 20.2 | 34.8 | 46.0 | 19.2 |
| Cholesterol (mg) | 46.5 | 41.4 | 12.1 | 45.5 | 38.9 | 15.7 |
| Water (g) | 49.0 | 39.9 | 11.1 | 50.0 | 40.4 | 9.6 |
| Vitamin C (mg) | 39.4 | 40.4 | 20.2 | 33.3 | 48.5 | 18.2 |
| Calcium (mg) | 43.9 | 44.9 | 11.1 | 44.9 | 42.9 | 12.1 |
| Copper (mg) | 42.4 | 39.9 | 17.7 | 42.4 | 40.9 | 16.7 |
| Iron (mg) | 46.0 | 39.4 | 14.6 | 48.0 | 37.4 | 14.6 |
| Magnesium (mg) | 52.0 | 37.9 | 10.1 | 58.1 | 34.3 | 7.6 |
| Manganese (mg) | 51.5 | 37.4 | 11.1 | 50.0 | 38.4 | 11.6 |
| Phosphorus (mg) | 54.5 | 34.8 | 10.6 | 49.0 | 38.4 | 12.6 |
| Potassium (mg) | 51.0 | 36.4 | 12.6 | 54.0 | 32.8 | 13.1 |
| Sodium (mg) | 40.4 | 33.3 | 26.3 | 35.4 | 39.4 | 25.3 |
| Zinc (mg) | 47.5 | 36.4 | 16.2 | 41.4 | 32.8 | 25.8 |
| Parameters | Crude a | Adjusted for Energy a | ||||
|---|---|---|---|---|---|---|
| Same Quartile | Adjacent Quartile b | Extreme Quartile c | Same Quartile | Adjacent Quartile b | Extreme Quartile c | |
| Condiments (g) | 36.4 | 37.4 | 26.3 | 27.8 | 39.4 | 32.8 |
| Grains (g) | 63.1 | 32.3 | 4.5 | 55.1 | 32.8 | 12.1 |
| Fruits (g) | 56.1 | 34.3 | 9.6 | 54.0 | 36.4 | 9.6 |
| Vegetables (g) | 53.5 | 36.4 | 10.1 | 53.0 | 35.4 | 11.6 |
| Meat, Poultry, Processed Meat, and Organ Meat (g) | 48.0 | 38.4 | 13.6 | 44.4 | 36.4 | 19.2 |
| Fish and Seafoods (g) | 38.9 | 37.4 | 23.8 | 41.4 | 38.4 | 20.3 |
| Eggs (g) | 59.6 | 20.7 | 19.7 | 40.9 | 46.5 | 12.6 |
| Dairy and Dairy Products (g) | 41.4 | 38.9 | 19.7 | 42.4 | 42.9 | 14.6 |
| Beverages (mL) | 36.9 | 25.8 | 37.3 | 42.4 | 30.8 | 26.8 |
| Tea or Coffee (mL) | 50.5 | 38.9 | 10.6 | 54.0 | 32.8 | 13.1 |
| Soy and Soy Products (g) | 38.9 | 31.8 | 29.3 | 34.8 | 40.9 | 24.2 |
| Legumes (g) | 29.8 | 29.8 | 40.4 | 35.9 | 36.4 | 27.8 |
| Nuts and Seeds (g) | 56.6 | 27.3 | 12.6 | 50.0 | 35.9 | 14.1 |
| Sugary Snacks (g) | 31.8 | 37.4 | 30.8 | 39.9 | 35.4 | 16.7 |
| Water (mL) | 65.5 | 27.0 | 7.4 | 68.2 | 24.2 | 7.6 |
| Savory Snacks (g) | 61.1 | 4.0 | 34.8 | 27.8 | 21.7 | 50.5 |
| Dim Sum (g) | 35.9 | 35.9 | 28.3 | 37.9 | 41.4 | 20.8 |
| Oil (mL) | 43.9 | 38.4 | 17.6 | 39.4 | 42.4 | 18.2 |
| Sugars (g) | 60.6 | 10.6 | 28.8 | 56.6 | 26.3 | 17.1 |
| Wine (mL) | 79.3 | 0 | 20.7 | 74.7 | 19.7 | 5.5 |
| Parameters | Mean Difference | p-Value | Beta-Coefficient | p-Value |
|---|---|---|---|---|
| Nutrients | ||||
| Energy (kcal) | 127.841 | <0.001 * | 0.195 | 0.006 * |
| Energy from Total Fat (kcal) | 62.729 | <0.001 * | 0.231 | 0.001 * |
| Energy from Saturated Fat (kcal) | 20.334 | <0.001 * | 0.429 | <0.001 * |
| Energy from Trans Fat (kcal) | −1.690 | <0.001 * | −0.370 | <0.001 * |
| Protein (g) | 5.204 | <0.001 * | 0.210 | 0.003 |
| Carbohydrates (g) | 11.153 | <0.001 * | 0.117 | 0.100 |
| Total Dietary Fiber (g) | 1.175 | <0.001 * | 0.143 | 0.045 * |
| Total Sugar (g) | −0.481 | 0.651 | 0.076 | 0.285 |
| Total Fat (g) | 6.842 | <0.001 * | 0.224 | 0.001 * |
| Saturated Fat (g) | 2.259 | <0.001 * | 0.429 | <0.001 * |
| Trans Fat (g) | −0.188 | <0.001 * | −0.370 | <0.001 * |
| Cholesterol (mg) | 57.673 | <0.001 * | 0.380 | <0.001 * |
| Water (g) | 6.002 | 0.852 | 0.086 | 0.229 |
| Vitamin C (mg) | 7.078 | 0.056 | 0.449 | <0.001 * |
| Calcium (mg) | −49.747 | 0.001 * | 0.226 | 0.001 * |
| Copper (mg) | 0.253 | <0.001 * | 0.330 | <0.001 * |
| Iron (mg) | −0.992 | <0.001 * | −0.126 | 0.076 |
| Magnesium (mg) | −5.030 | 0.228 | 0.153 | 0.032 * |
| Manganese (mg) | −0.504 | <0.001 * | 0.139 | 0.051 |
| Phosphorus (mg) | −11.948 | 0.419 | 0.045 | 0.529 |
| Potassium (mg) | 171.353 | <0.001 * | 0.252 | <0.001 * |
| Sodium (mg) | 639.140 | <0.001 * | 0.385 | <0.001 * |
| Zinc (mg) | 0.368 | 0.105 | 0.490 | <0.001 * |
| Food Groups | ||||
| Condiments (g) | 2.123 | 0.005 * | 0.482 | <0.001 * |
| Grains (g) | −2.582 | 0.684 | −0.005 | 0.942 |
| Fruits (g) | 10.102 | 0.044 * | 0.201 | 0.005 * |
| Vegetables (g) | 20.539 | 0.004 * | 0.288 | <0.001 * |
| Meat, Poultry, Processed Meat, and Organ Meat (g) | 11.886 | <0.001 * | 0.263 | <0.001 * |
| Fish and Seafoods (g) | 4.692 | 0.083 | 0.359 | <0.001 * |
| Eggs (g) | −2.230 | 0.076 | 0.290 | <0.001 * |
| Dairy and Dairy Products (g) | −31.135 | <0.001 * | −0.188 | 0.008 * |
| Beverages (mL) | 32.132 | 0.001 * | −0.067 | 0.349 |
| Tea or Coffee (mL) | 26.845 | 0.165 | 0.287 | <0.001 * |
| Soy and Soy Products (g) | −25.521 | <0.001 * | −0.015 | 0.838 |
| Legumes (g) | −5.359 | 0.003 * | 0.137 | 0.055 |
| Nuts and Seeds (g) | 1.642 | 0.020 * | 0.517 | <0.001 * |
| Sugary Snacks (g) | 9.703 | <0.001 * | 0.476 | <0.001 * |
| Water (mL) | −3.921 | 0.850 | −0.073 | 0.304 |
| Savory Snacks (g) | 0.544 | 0.325 | 0.701 | <0.001 * |
| Dim Sum (g) | 20.077 | <0.001 * | 0.682 | <0.001 * |
| Oil (mL) | −7.473 | <0.001 * | −0.388 | <0.001 * |
| Sugars (g) | 1.259 | <0.001 * | 0.630 | <0.001 * |
| Wine (mL) | 3.083 | 0.220 | −0.055 | 0.438 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, V.W.-k.; Zhou, J.H.-s.; Li, L.; Tse, M.T.-h.; You, J.J.; Wong, M.-s.; Liu, J.Y.-w.; Lo, K.K.-h. Reproducibility and Relative Validity of a Short Food Frequency Questionnaire for Chinese Older Adults in Hong Kong. Nutrients 2024, 16, 1132. https://doi.org/10.3390/nu16081132
Chan VW-k, Zhou JH-s, Li L, Tse MT-h, You JJ, Wong M-s, Liu JY-w, Lo KK-h. Reproducibility and Relative Validity of a Short Food Frequency Questionnaire for Chinese Older Adults in Hong Kong. Nutrients. 2024; 16(8):1132. https://doi.org/10.3390/nu16081132
Chicago/Turabian StyleChan, Vicky Wai-ki, Joson Hao-shen Zhou, Liz Li, Michael Tsz-hin Tse, Jane Jia You, Man-sau Wong, Justina Yat-wa Liu, and Kenneth Ka-hei Lo. 2024. "Reproducibility and Relative Validity of a Short Food Frequency Questionnaire for Chinese Older Adults in Hong Kong" Nutrients 16, no. 8: 1132. https://doi.org/10.3390/nu16081132
APA StyleChan, V. W.-k., Zhou, J. H.-s., Li, L., Tse, M. T.-h., You, J. J., Wong, M.-s., Liu, J. Y.-w., & Lo, K. K.-h. (2024). Reproducibility and Relative Validity of a Short Food Frequency Questionnaire for Chinese Older Adults in Hong Kong. Nutrients, 16(8), 1132. https://doi.org/10.3390/nu16081132