Sustaining Healthy Habits: The Enduring Impact of Combined School–Family Interventions on Consuming Sugar-Sweetened Beverages among Pilot Chinese Schoolchildren

 ,
, 
Abstract
1. Introduction
2. Subjects and Methods
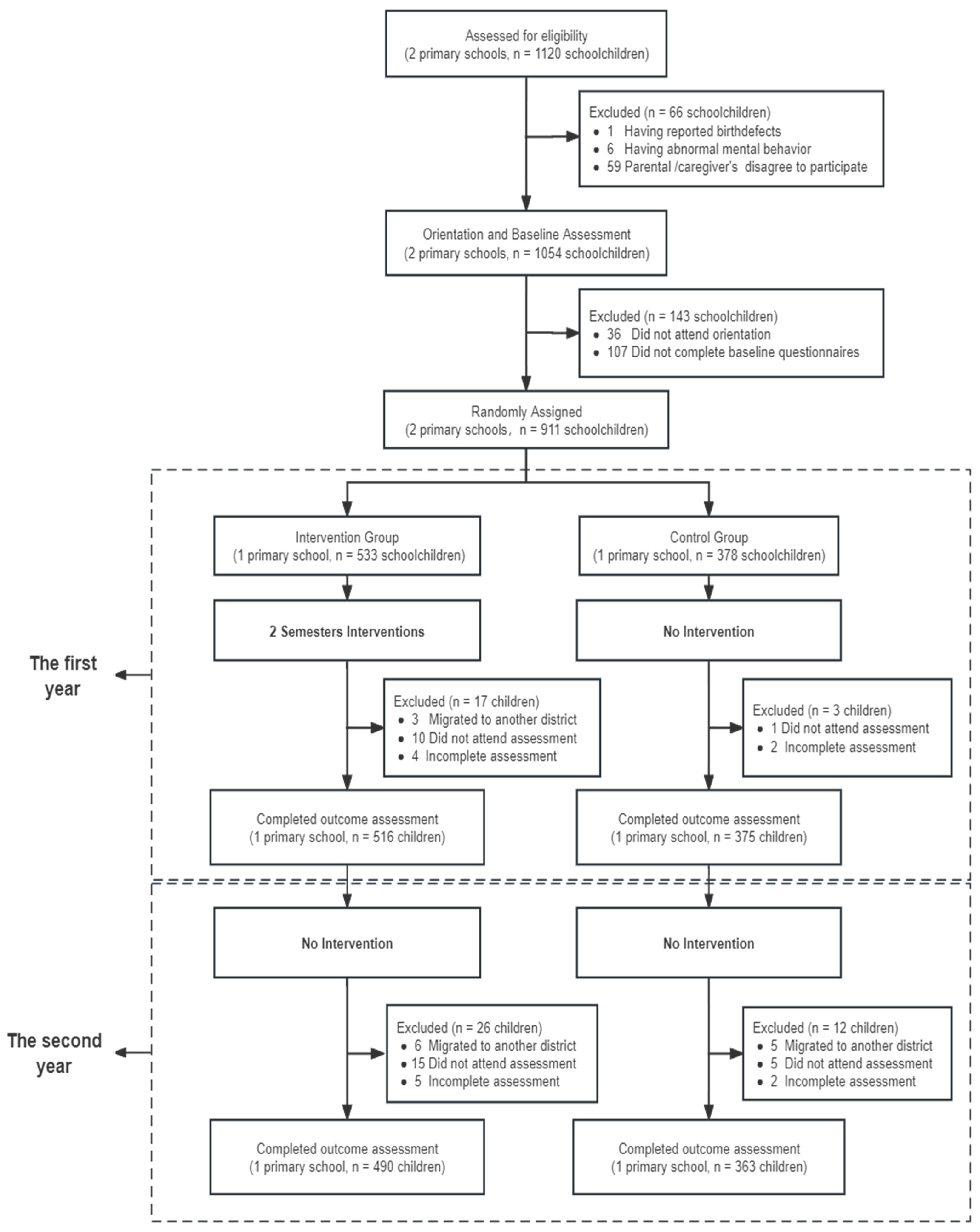
2.1. Participants
2.2. Study Design
2.3. Intervention Methods
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Knowledge about SSBs
3.3. Differences in Family Environment with Parents Concerning SSBs
3.4. Frequency and Quantity of SSB Consumption
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC. Get the Facts: Sugar-Sweetened Beverages and Consumption. 2017. Available online: https://www.cdc.gov/nutrition/data-statistics/sugar-sweetened-beverages-intake.html (accessed on 25 November 2023).
- Della Corte, K.; Fife, J.; Gardner, A.; Murphy, B.L.; Kleis, L.; Della Corte, D.; Schwingshackl, L.; LeCheminant, J.D.; Buyken, A.E. World trends in sugar-sweetened beverage and dietary sugar intakes in children and adolescents: A systematic review. Nutr. Rev. 2021, 79, 274–288. [Google Scholar] [CrossRef]
- Wang, Y.C.; Bleich, S.N.; Gortmaker, S.L. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988–2004. Pediatrics 2008, 121, 1604–1614. [Google Scholar] [CrossRef]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef]
- Sim, E.; Sohn, W.; Choi, E.S.; Noh, H. Sugar-sweetened beverage consumption frequency in Korean adolescents: Based on the 2015 Youth Risk Behavior Web-Based Survey. Int. Dent. J. 2019, 69, 376–382. [Google Scholar] [CrossRef]
- Ma, G. Report on the Consumption of Sugar-Sweetened Beverages of Children in China; China Population Publishing House: Bejing, China, 2018; pp. 34–35. [Google Scholar]
- China National Health and Family Planning Commission. Report on Nutrition and Chronic Diseases of Chinese Residents; People’s Medical Publishing House: Beijing, China, 2020; pp. 18–20.
- Qin, Z.; Xu, F.; Ye, Q.; Zhou, H.; Li, C.; He, J.; Wang, Z.; Hong, X.; Hou, X. Sugar-sweetened beverages and school students’ hypertension in urban areas of Nanjing. China J. Hum. Hypertens. 2018, 32, 392–396. [Google Scholar] [CrossRef]
- Malik, V.S.; Hu, F.B. The role of sugar-sweetened beverages in the global epidemics of obesity and chronic diseases. Nat. Rev. Endocrinol. 2022, 18, 205–218. [Google Scholar] [CrossRef]
- Bleich, S.N.; Vercammen, K.A. The negative impact of sugar-sweetened beverages on children’s health: An update of the literature. BMC Obes. 2018, 5, 6. [Google Scholar] [CrossRef]
- Rousham, E.K.; Goudet, S.; Markey, O.; Griffiths, P.; Boxer, B.; Carroll, C.; Petherick, E.S.; Pradeilles, R. Unhealthy Food and Beverage Consumption in Children and Risk of Overweight and Obesity: A Systematic Review and Meta-Analysis. Adv. Nutr. 2022, 13, 1669–1696. [Google Scholar] [CrossRef]
- Efthymiou, V.; Charmandari, E.; Vlachakis, D.; Tsitsika, A.; Pałasz, A.; Chrousos, G.; Bacopoulou, F. Adolescent Self-Efficacy for Diet and Exercise Following a School-Based Multicomponent Lifestyle Intervention. Nutrients 2021, 14, 97. [Google Scholar] [CrossRef]
- Xu, Y.; Bi, X.; Gao, T.; Yang, T.; Xu, P.; Gan, Q.; Xu, J.; Cao, W.; Wang, H.; Pan, H.; et al. Effect of School-Based Nutrition and Health Education for Rural Chinese Children. Nutrients 2022, 14, 3997. [Google Scholar] [CrossRef]
- Honkala, S. World Health Organization approaches for surveys of health behaviour among schoolchildren and for health-promoting schools. Med. Princ. Pract. 2014, 23 (Suppl. 1), 24–31. [Google Scholar] [CrossRef]
- Ooi, J.Y.; Wolfenden, L.; Yoong, S.L.; Janssen, L.M.; Reilly, K.; Nathan, N.; Sutherland, R. A trial of a six-month sugar-sweetened beverage intervention in secondary schools from a socio-economically disadvantaged region in Australia. Aust. N. Z. J. Public Health 2021, 45, 599–607. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Feldman, H.A.; Chomitz, V.R.; Antonelli, T.A.; Gortmaker, S.L.; Osganian, S.K.; Ludwig, D.S. A randomized trial of sugar-sweetened beverages and adolescent body weight. N. Engl. J. Med. 2012, 367, 1407–1416. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Friend, S.; Horning, M.; Flattum, C.; Draxten, M.; Neumark-Sztainer, D.; Gurvich, O.; Garwick, A.; Story, M.; Kubik, M.Y. Family Home Food Environment and Nutrition-Related Parent and Child Personal and Behavioral Outcomes of the Healthy Home Offerings via the Mealtime Environment (HOME) Plus Program: A Randomized Controlled Trial. J. Acad. Nutr. Die 2018, 118, 240–251. [Google Scholar] [CrossRef]
- Kaufman-Shriqui, V.; Fraser, D.; Friger, M.; Geva, D.; Bilenko, N.; Vardi, H.; Elhadad, N.; Mor, K.; Feine, Z.; Shahar, D.R. Effect of a School-Based Intervention on Nutritional Knowledge and Habits of Low-Socioeconomic School Children in Israel: A Cluster-Randomized Controlled Trial. Nutrients 2016, 8, 234. [Google Scholar] [CrossRef]
- Teo, C.H.; Chin, Y.S.; Lim, P.Y.; Masrom, S.A.H.; Shariff, Z.M. Impacts of a School-Based Intervention That Incorporates Nutrition Education and a Supportive Healthy School Canteen Environment among Primary School Children in Malaysia. Nutrients 2021, 13, 1712. [Google Scholar] [CrossRef]
- Battram, D.S.; Piché, L.; Beynon, C.; Kurtz, J.; He, M. Sugar-Sweetened Beverages: Children’s Perceptions, Factors of Influence, and Suggestions for Reducing Intake. J. Nutr. Educ. Behav. 2016, 48, 27–34. [Google Scholar] [CrossRef]
- Haq, I.U.; Liu, Y.; Liu, M.; Xu, H.; Wang, H.; Liu, C.; Zeb, F.; Jiang, P.; Wu, X.; Tian, Y.; et al. Association of Smoking-Related Knowledge, Attitude, and Practices (KAP) with Nutritional Status and Diet Quality: A Cross-Sectional Study in China. BioMed Res. Int. 2019, 2019, 5897478. [Google Scholar] [CrossRef]
- Assefa, E.M. Knowledge, attitude and practice (KAP) of health providers towards safe abortion provision in Addis Ababa health centers. BMC Women’s Health 2019, 19, 138. [Google Scholar] [CrossRef]
- Qian, M.B.; Gan, X.Q.; Zhao, J.G.; Zheng, W.J.; Li, W.; Jiang, Z.H.; Zhu, T.J.; Zhou, X.N. Effectiveness of health education in improving knowledge, practice and belief related to clonorchiasis in children. Acta Trop. 2020, 207, 105436. [Google Scholar] [CrossRef]
- Sagbo, H.; Kpodji, P. Dietary diversity and associated factors among school-aged children and adolescents in Lokossa district of southern Benin: A cross-sectional study. BMJ Open 2023, 13, e066309. [Google Scholar] [CrossRef]
- Ochola, S.; Masibo, P.K. Dietary intake of schoolchildren and adolescents in developing countries. Ann. Nutr. Metab. 2014, 64 (Suppl. 2), 24–40. [Google Scholar] [CrossRef]
- Mohieldein, A.; Elhabiby, M.; Abu Mustafa, A.; Shehade, M.; Alsuhaibani, S. A Cross-Sectional Analysis of Health Behavior in School-Aged Children: The Qassim Study. Cureus 2023, 15, e48420. [Google Scholar] [CrossRef]
- GB10789-2008; General Standard for Beverage. Standardization Administration of the People’s Republic of China: Beijing, China, 2008.
- Sirasa, F.; Mitchell, L.; Azhar, A.; Chandrasekara, A.; Harris, N. A six-week healthy eating intervention with family engagement improves food knowledge and preferences but not dietary diversity among urban preschool children in srilanka. Public Health Nutr. 2021, 24, 4328–4338. [Google Scholar] [CrossRef]
- Odeyemi, O.A.; Sani, N.A.; Obadina, A.O.; Saba, C.K.S.; Bamidele, F.A.; Abughoush, M.; Asghar, A.; Dongmo, F.F.D.; Macer, D.; Aberoumand, A. Food safety knowledge, attitudes and practices among consumers in developing countries: An international survey. Food Res. Int. 2019, 116, 1386–1390. [Google Scholar] [CrossRef]
- Wang, M.; Fang, H. The effect of health education on knowledge and behavior toward respiratory infectious diseases among students in Gansu, China: A quasi-natural experiment. BMC Public Health 2020, 20, 681. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2017, 97, 667–675. [Google Scholar] [CrossRef]
- Mensink, F.; Schwinghammer, S.A.; Smeets, A. The Healthy School Canteen programme: A promising intervention to make the school food environment healthier. J. Environ. Public Health 2012, 2012, 415746. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Aranceta, J. School-based nutrition education: Lessons learned and new perspectives. Public Health Nutr. 2001, 4, 131–139. [Google Scholar] [CrossRef]
- Vázquez-Paz, A.M.; Michel-Nava, R.M.; Delgado-Pérez, E.E.; Lares-Michel, M.; Espinosa-Curiel, I.E. Parents’ mHealth App for Promoting Healthy Eating Behaviors in Children: Feasibility, Acceptability, and Pilot Study. J. Med. Syst. 2022, 46, 70. [Google Scholar] [CrossRef]
- Vinke, P.C.; Blijleven, K.A.; Luitjens, M.H.H.S.; Corpeleijn, E. Young Children’s Sugar-Sweetened Beverage Consumption and 5-Year Change in BMI: Lessons Learned from the Timing of Consumption. Nutrients 2020, 12, 2486. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Ober, A.J.; Klein, D.J.; Hawes-Dawson, J.; Cowgill, B.O.; Uyeda, K.; Schuster, M.A. Home Sweet Home: Parent and Home Environmental Factors in Adolescent Consumption of Sugar-Sweetened Beverages. Acad. Pediatr. 2017, 17, 529–536. [Google Scholar] [CrossRef]
- Pearson, N.; Finch, M.; Sutherland, R.; Kingsland, M.; Wolfenden, L.; Wedesweiler, T.; Herrmann, V.; Yoong, S.L. AnmHealth Intervention to Reduce the Packing of Discretionary Foods in Children’s Lunch Boxes in Early Childhood Education and Care Services: Cluster Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e27760. [Google Scholar] [CrossRef]
- Guagliano, J.M.; Morton, K.L.; Hughes, C.; van Sluijs, E.M.F. Effective and resource-efficient strategies for recruiting families in physical activity, sedentary behavior, nutrition, and obesity prevention research: A systematic review with expert opinion. Obes. Rev. 2021, 22, e13161. [Google Scholar] [CrossRef]
- Østbye, T.; Malhotra, R.; Stroo, M.; Lovelady, C.; Brouwer, R.; Zucker, N.; Fuemmeler, B. The effect of the home environment on physical activity and dietary intake in preschool children. Int. J. Obes. 2013, 37, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Luo, C.; Qu, S.; Wei, X.; Feng, J.; Zhang, S.; Wang, Y.; Su, J. Effects of School-Based Interventions on Reducing Sugar-Sweetened Beverage Consumption among Chinese Children and Adolescents. Nutrients 2021, 13, 1862. [Google Scholar] [CrossRef]
- Sligo, F.X.; Jameson, A.M. The knowledge—Behavior gap in use of health information. J. Am. Soc. Inf. Sci. 2000, 51, 858–869. [Google Scholar] [CrossRef]
- Naeeni, M.M.; Jafari, S.; Fouladgar, M.; Heidari, K.; Farajzadegan, Z.; Fakhri, M.; Karami, P.; Omidi, R. Nutritional Knowledge, Practice, and Dietary Habits among school Children and Adolescents. Int. J. Prev. Med. 2014, 5 (Suppl. S2), S171–S178. [Google Scholar] [CrossRef]
- Avery, A.; Bostock, L.; McCullough, F. A systematic review investigating interventions that can help reduce consumption of sugar-sweetened beverages in children leading to changes in body fatness. J. Hum. Nutr. Diet. 2015, 28 (Suppl. S1), 52–64. [Google Scholar] [CrossRef]
- Abdel Rahman, A.; Jomaa, L.; Kahale, L.A.; Adair, P.; Pine, C. Effectiveness of behavioral interventions to reduce the intake of sugar-sweetened beverages in children and adolescents: A systematic review and meta-analysis. Nutr. Rev. 2018, 76, 88–107. [Google Scholar] [CrossRef]
- Hajishafiee, M.; Kapellas, K.; Listl, S.; Pattamatta, M.; Gkekas, A.; Moynihan, P. Effect of sugar-sweetened beverage taxation on sugars intake and dental caries: An umbrella review of a global perspective. BMC Public Health 2023, 23, 986. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Retained in Trial (853) | Dropped Out (58) | X2/t | p |
|---|---|---|---|---|
| Sex | ||||
| Male | 467/54.7 | 32/55.2 | 0.004 | 0.950 |
| Female | 386/45.3 | 26/44.8 | ||
| Age (years) | 9.1 ± 0.4 | 9.1 ± 0.3 | 0.685 | 0.494 |
| Group | ||||
| Intervention Group | 490/57.4 | 34/58.6 | 0.031 | 0.861 |
| Control Group | 363/42.6 | 24/41.4 | ||
| Parental education level | ||||
| ≤9 years | 336/39.4 | 22/37.9 | 0.048 | 0.826 |
| >9 years | 517/60.6 | 36/62.1 | ||
| Father’s BMI a (kg/m2) | ||||
| <24 | 370/43.6 | 25/43.1 | 0.005 | 0.943 |
| ≥24 | 479/56.4 | 33/56.9 | ||
| Mother’s BMI a (kg/m2) | ||||
| <24 | 664/78.7 | 45/77.6 | 0.038 | 0.845 |
| ≥24 | 180/21.3 | 13/22.4 | ||
| Physical activity time outside school (min/week) | ||||
| <120 | 511/59.9 | 30/51.7 | 1.507 | 0.220 |
| ≥120 | 342/40.1 | 28/48.3 | ||
| Homework time (min/day) | ||||
| <120 | 444/52.2 | 26/44.8 | 1.193 | 0.275 |
| ≥120 | 406/47.8 | 32/55.2 | ||
| Screen time (min/day) | ||||
| <60 | 624/73.2 | 48/82.8 | 2.589 | 0.108 |
| ≥60 | 229/26.8 | 10/17.2 | ||
| BMI a | 17.4 ± 2.9 | 17.6 ± 2.9 | −0.722 | 0.470 |
| Frequency of SSB b consumption | 3.5 ± 4.0 | 3.5 ± 3.2 | 0.049 | 0.961 |
| Characteristics | Total (853) | Intervention Group (n = 490) | Control Group (n = 363) | X2/t | p |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 470/55.1 | 274/55.9 | 196/54.0 | 0.312 | 0.577 |
| Female | 383/44.9 | 216/44.1 | 167/46.0 | ||
| Age (years) | 9.1 ± 0.4 | 9.1 ± 0.3 | 9.1 ± 0.4 | −1.565 | 0.118 |
| Parental education level | |||||
| ≤9 years | 336/39.4 | 169/34.5 | 167/46.0 | 11.583 | 0.001 |
| >9 years | 517/60.6 | 321/65.5 | 196/54.0 | ||
| Father’s BMI a (kg/m2) | |||||
| <24 | 370/43.6 | 208/42.5 | 162/45.0 | 0.512 | 0.474 |
| ≥24 | 479/56.4 | 281/57.5 | 198/55.0 | ||
| Mother’s BMI a (kg/m2) | |||||
| <24 | 664/78.7 | 375/77.0 | 289/81.0 | 1.916 | 0.166 |
| ≥24 | 180/21.3 | 112/23.0 | 68/19.0 | ||
| Physical activity time outside school (min/week) | |||||
| <120 | 511/59.9 | 305/62.2 | 206/56.7 | 2.622 | 0.120 |
| ≥120 | 342/40.1 | 185/37.8 | 157/43.3 | ||
| Homework time (min/day) | |||||
| <120 | 444/52.2 | 263/53.7 | 181/50.3 | 0.959 | 0.332 |
| ≥120 | 406/47.8 | 227/46.3 | 179/49.7 | ||
| Screen time (min/day) | |||||
| <60 | 624/73.2 | 352/71.8 | 272/74.9 | 1.017 | 0.348 |
| ≥60 | 229/26.8 | 138/28.2 | 91/25.1 | ||
| BMI a | 17.4 ± 2.9 | 17.3 ± 2.9 | 17.5 ± 3.0 | −1.163 | 0.245 |
| Frequency of SSB b consumption | 3.5 ± 4.0 | 3.5 ± 4.4 | 3.5 ± 3.2 | −0.144 | 0.885 |
| Knowledge | Baseline | First Year | Second Year | Change from Baseline | Compared to Baseline c | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First Year | Second Year | β1 d (95%CI) | Waldχ2 | p | β2 e (95%CI) | Waldχ2 | p | ||||
| Definition of SSBs b. | |||||||||||
| Intervention Group | 127/25.9 | 363/74.1 | 384/78.4 | 236/48.2 | 257/52.5 | 2.1 (1.8, 2.4) | 211.855 | <0.001 | 2.4 (2.1, 2.6) | 288.113 | <0.001 |
| Control Group | 129/35.5 | 175/48.2 | 196/54.0 | 46/12.7 | 67/18.5 | 0.5 (0.2, 0.8) | 12.913 | <0.001 | 0.8 (0.5, 1.0) | 26.653 | <0.001 |
| p | 0.003 | <0.001 | <0.001 | ||||||||
| SSBs are bad for health. | |||||||||||
| Intervention Group | 432/88.2 | 485/99.0 | 480/98.0 | 53/10.8 | 48/9.8 | 2.6 (1.7, 3.5) | 31.229 | <0.001 | 1.9 (1.2, 2.5) | 28.369 | <0.001 |
| Control Group | 342/94.2 | 348/95.9 | 356/98.1 | 6/1.7 | 14/3.9 | 0.4 (−0.3, 1.1) | 0.992 | 0.319 | 1.1 (0.3, 2.0) | 6.414 | 0.011 |
| p | 0.003 | 0.005 | 0.908 | ||||||||
| SSBs may cause tooth decay. | |||||||||||
| Intervention Group | 407/83.1 | 480/98.0 | 477/97.3 | 73/14.9 | 70/14.2 | 2.3 (1.6, 2.9) | 48.728 | <0.001 | 2.0 (1.4, 2.6) | 46.499 | <0.001 |
| Control Group | 321/88.4 | 337/92.8 | 336/92.6 | 16/4.4 | 15/4.2 | 0.5 (0.1, 1.0) | 5.522 | 0.019 | 0.5 (0.0, 0.9) | 4.756 | 0.029 |
| p | 0.031 | <0.001 | 0.002 | ||||||||
| SSBs may cause childhood overweight and obesity. | |||||||||||
| Intervention Group | 340/69.4 | 469/95.7 | 475/96.9 | 129/26.3 | 135/27.5 | 2.3 (1.8, 2.7) | 95.181 | <0.001 | 2.6 (2.1, 3.2) | 94.124 | <0.001 |
| Control Group | 266/73.3 | 320/88.2 | 319/87.9 | 54/14.9 | 53/14.6 | 1.0 (0.7, 1.3) | 39.511 | <0.001 | 1.0 (0.7, 1.3) | 37.507 | <0.001 |
| p | 0.223 | <0.001 | <0.001 | ||||||||
| SSBs can increase type 2 diabetes in children and in later life. | |||||||||||
| Intervention Group | 208/42.4 | 419/85.5 | 427/87.1 | 211/43.1 | 219/44.7 | 2.1 (1.8, 2.4) | 193.840 | <0.001 | 2.2 (1.9, 2.5) | 176.556 | <0.001 |
| Control Group | 181/49.9 | 216/59.5 | 207/57.0 | 35/9.6 | 26/7.1 | 0.4 (0.2, 0.6) | 15.994 | <0.001 | 0.3 (0.1, 0.5) | 7.979 | 0.005 |
| p | 0.037 | <0.001 | <0.001 | ||||||||
| Carbonated drinks may increase risks of bone in child. | |||||||||||
| Intervention Group | 197/40.2 | 411/83.9 | 431/88.0 | 214/43.7 | 234/47.8 | 2.1 (1.8, 2.3) | 217.081 | <0.001 | 2.4 (2.1, 2.7) | 201.966 | <0.001 |
| Control Group | 165/45.5 | 198/54.5 | 195/53.7 | 33/9.0 | 30/8.2 | 0.4 (0.2, 0.5) | 29.917 | <0.001 | 0.3 (0.2, 0.5) | 22.566 | <0.001 |
| p | 0.141 | <0.001 | <0.001 | ||||||||
| Fruit/vegetable drinks are not a substitute for fruits and vegetables. | |||||||||||
| Intervention Group | 276/56.3 | 426/86.9 | 447/91.2 | 150/30.6 | 171/34.9 | 1.6 (1.3, 1.9) | 118.776 | <0.001 | 2.1 (1.7, 2.4) | 137.909 | <0.001 |
| Control Group | 182/50.1 | 240/66.1 | 257/70.8 | 58/16.0 | 75/20.7 | 0.7 (0.5, 0.8) | 55.224 | <0.001 | 0.9 (0.7, 1.1) | 71.772 | <0.001 |
| p | 0.083 | <0.001 | <0.001 | ||||||||
| Milk drinks are not a substitute for milk. | |||||||||||
| Intervention Group | 193/39.4 | 347/70.8 | 372/75.9 | 154/31.4 | 179/36.5 | 1.3 (1.1, 1.6) | 107.327 | <0.001 | 1.6 (1.3, 1.8) | 140.814 | <0.001 |
| Control Group | 126/34.7 | 191/52.6 | 207/57.0 | 65/17.9 | 81/22.3 | 0.7 (0.5, 1.0) | 43.263 | <0.001 | 0.9 (0.7, 1.2) | 56.205 | <0.001 |
| p | 0.174 | <0.001 | <0.001 | ||||||||
| SSBs are one of the high-sugar foods. | |||||||||||
| Intervention Group | 413/84.3 | 467/95.3 | 473/96.5 | 54/11.0 | 60/12.2 | 1.3 (1.0, 1.7) | 50.371 | <0.001 | 1.6 (1.2, 2.1) | 47.587 | <0.001 |
| Control Group | 305/84.0 | 314/86.5 | 322/88.7 | 9/2.5 | 17/4.7 | 0.2 (−0.0, 0.4) | 3.545 | 0.060 | 0.4 (0.1, 0.7) | 8.855 | 0.003 |
| p | 0.925 | <0.001 | <0.001 | ||||||||
| Definition of added sugar. | |||||||||||
| Intervention Group | 117/23.9 | 362/73.9 | 420/85.7 | 245/50.0 | 303/61.8 | 2.2 (2.0, 2.4) | 302.800 | <0.001 | 3.0 (2.7, 3.2) | 389.027 | <0.001 |
| Control Group | 88/24.2 | 204/56.2 | 212/58.4 | 116/32.0 | 124/7.8 | 1.4 (1.2, 1.6) | 138.515 | <0.001 | 1.5 (1.2, 1.7) | 117.253 | <0.001 |
| p | 0.935 | <0.001 | <0.001 | ||||||||
| Adequate knowledge about SSBs f | |||||||||||
| Intervention Group | 254/51.8 | 464/94.7 | 477/97.3 | 210/42.9 | 223/45.5 | 2.8 (2.4, 3.2) | 182.719 | <0.001 | 3.5 (3.0, 4.1) | 146.612 | <0.001 |
| Control Group | 212/58.4 | 296/81.5 | 302/83.2 | 84/23.1 | 90/24.8 | 1.1 (0.9, 1.4) | 64.239 | <0.001 | 1.3 (1.0, 1.6) | 71.304 | <0.001 |
| p | 0.061 | <0.001 | <0.001 | ||||||||
| Family Environment with Parents | Baseline | First Year | Second Year | Change from Baseline | Compared to Baseline c | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First Year | Second Year | β1 d (95%CI) | Waldχ2 | p | β2 e (95%CI) | Waldχ2 | p | ||||
| My home always has SSBs b | |||||||||||
| Intervention Group | 63/12.9 | 36/7.3 | 38/7.8 | −27/−5.6 | −25/−5.1 | −0.6 (−1.0, −0.2) | 8.256 | 0.004 | −0.6 (−1.0, −0.2) | 7.636 | 0.006 |
| Control Group | 54/14.9 | 49/13.5 | 45/12.4 | −5/−1.4 | −9/−2.5 | −0.1 (−0.5, 0.3) | 0.316 | 0.574 | −0.2 (−0.6, 0.2) | 1.051 | 0.305 |
| p | 0.421 | 0.004 | 0.026 | ||||||||
| Parents have been warned about harms of SSBs | |||||||||||
| Intervention Group | 290/59.2 | 408/83.3 | 454/92.7 | 118/24.1 | 164/33.5 | 1.2 (1.0, 1.5) | 99.418 | <0.001 | 2.2 (1.8, 2.5) | 136.718 | <0.001 |
| Control Group | 252/69.4 | 296/82.2 | 310/85.4 | 44/12.8 | 58/16.0 | 0.7 (0.3, 1.0) | 16.563 | <0.001 | 0.9 (0.6, 1.3) | 28.210 | <0.001 |
| p | 0.002 | 0.713 | 0.001 | ||||||||
| My parents restricted me from drinking SSBs | |||||||||||
| Intervention Group | 282/57.6 | 410/83.7 | 445/90.8 | 128/26.1 | 163/33.2 | 1.3 (1.1, 1.6) | 117.524 | <0.001 | 2.0 (1.7, 2.3) | 133.415 | <0.001 |
| Control Group | 205/56.5 | 289/79.6 | 312/86.0 | 84/23.1 | 107/29.5 | 1.1 (1.1, 1.6) | 54.764 | <0.001 | 1.6 (1.2, 1.9) | 76.188 | <0.001 |
| p | 0.780 | 0.150 | 0.029 | ||||||||
| My parents restricted me from eating sugary snacks | |||||||||||
| Intervention Group | 260/53.1 | 380/77.6 | 429/87.6 | 120/24.5 | 169/34.5 | 1.1 (0.9, 1.4) | 76.147 | <0.001 | 1.8 (1.5, 2.1) | 138.975 | <0.001 |
| Control Group | 199/54.8 | 297/81.8 | 306/84.3 | 98/27.0 | 107/29.5 | 1.3 (1.0, 1.6) | 62.450 | <0.001 | 1.5 (1.1, 1.8) | 71.582 | <0.001 |
| p | 0.627 | 0.146 | 0.192 | ||||||||
| My parents often drink SSBs | |||||||||||
| Intervention Group | 51/10.4 | 20/4.1 | 18/3.7 | −31/−6.3 | −33/−6.7 | −1.0 (−1.5, −0.5) | 16.670 | <0.001 | −1.1 (−1.7, −0.6) | 16.175 | <0.001 |
| Control Group | 34/9.4 | 25/6.9 | 28/7.7 | −9/−2.5 | −6/−1.7 | −0.3 (−0.8, 0.2) | 1.645 | 0.200 | −0.2 (−0.7, 0.3) | 0.691 | 0.406 |
| p | 0.645 | 0.088 | 0.013 | ||||||||
| My parents often eat sugary snacks | |||||||||||
| Intervention Group | 33/6.7 | 40/8.2 | 23/4.7 | 7/1.5 | −10/−2.0 | 0.2 (−0.3, 0.7) | 0.709 | 0.400 | −0.4 (−0.9, 0.2) | 1.970 | 0.167 |
| Control Group | 27/7.4 | 27/7.4 | 35/9.6 | 0/0 | 8/2.2 | −0.1 (−0.6, 0.6) | <0.001 | 1.000 | 0.3 (−0.2, 0.8) | 1.139 | 0.286 |
| p | 0.687 | 0.797 | 0.006 | ||||||||
| SSB Consumption | Baseline | First Year | Second Year | Change from Baseline | Compared to Baseline b | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First Year | Second Year | β1 c (95%CI) | Waldχ2 | p | β2 d (95%CI) | Waldχ2 | p | ||||
| Frequency of SSB a consumption (times/week) | |||||||||||
| Intervention Group | 3.5 ± 3.4 | 2.4 ± 2.7 | 2.7 ± 3.1 | −1.0 ± 4.5 | −0.8 ± 4.9 | −1.4 (−1.4, −0.6) | 26.747 | <0.001 | −0.8 (−1.2, −0.4) | 12.723 | <0.001 |
| Control Group | 3.5 ± 3.2 | 3.4 ± 3.0 | 3.0 ± 3.2 | −0.1 ± 3.9 | −0.5 ± 4.0 | −0.1 (−0.5, 0.3) | 0.437 | 0.509 | −0.5 (−0.9, −0.0) | 4.784 | 0.029 |
| T/Z | −0.144 | −4.874 | −1.682 | −2.249 | −0.765 | ||||||
| p | 0.885 | <0.001 | 0.093 | 0.025 | 0.444 | ||||||
| Quantity of SSB a consumption (mL/week) | |||||||||||
| Intervention Group | 871 ± 1347 | 638 ± 822 | 748 ± 1125 | −233 ± 1392 | −122 ± 1630 | −232 (−356, −110) | 13.725 | <0.001 | −122 (−267, 22) | 2.769 | 0.096 |
| Control Group | 908 ± 956 | 1015 ± 1065 | 939 ± 1304 | 107 ± 1286 | 31 ± 1509 | 107 (−252, 239.0) | 2.518 | 0.113 | 31 (−124, 186) | 0.151 | 0.698 |
| T/Z | −0.450 | −5.835 | −2.283 | −2.719 | −0.092 | ||||||
| p | 0.653 | <0.001 | 0.023 | 0.005 | 0.927 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Chen, Y.; Xu, H.; Wang, W.; Zhou, H.; Sun, Q.; Hong, X.; Zhao, J. Sustaining Healthy Habits: The Enduring Impact of Combined School–Family Interventions on Consuming Sugar-Sweetened Beverages among Pilot Chinese Schoolchildren. Nutrients 2024, 16, 953. https://doi.org/10.3390/nu16070953
Wang C, Chen Y, Xu H, Wang W, Zhou H, Sun Q, Hong X, Zhao J. Sustaining Healthy Habits: The Enduring Impact of Combined School–Family Interventions on Consuming Sugar-Sweetened Beverages among Pilot Chinese Schoolchildren. Nutrients. 2024; 16(7):953. https://doi.org/10.3390/nu16070953
Chicago/Turabian StyleWang, Chenchen, Yijia Chen, Hao Xu, Weiwei Wang, Hairong Zhou, Qiannan Sun, Xin Hong, and Jinkou Zhao. 2024. "Sustaining Healthy Habits: The Enduring Impact of Combined School–Family Interventions on Consuming Sugar-Sweetened Beverages among Pilot Chinese Schoolchildren" Nutrients 16, no. 7: 953. https://doi.org/10.3390/nu16070953
APA StyleWang, C., Chen, Y., Xu, H., Wang, W., Zhou, H., Sun, Q., Hong, X., & Zhao, J. (2024). Sustaining Healthy Habits: The Enduring Impact of Combined School–Family Interventions on Consuming Sugar-Sweetened Beverages among Pilot Chinese Schoolchildren. Nutrients, 16(7), 953. https://doi.org/10.3390/nu16070953