
Lower Multiple Sclerosis Severity Score Is Associated with Higher Adherence to Mediterranean Diet in Subjects with Multiple Sclerosis from Northwestern Italy

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
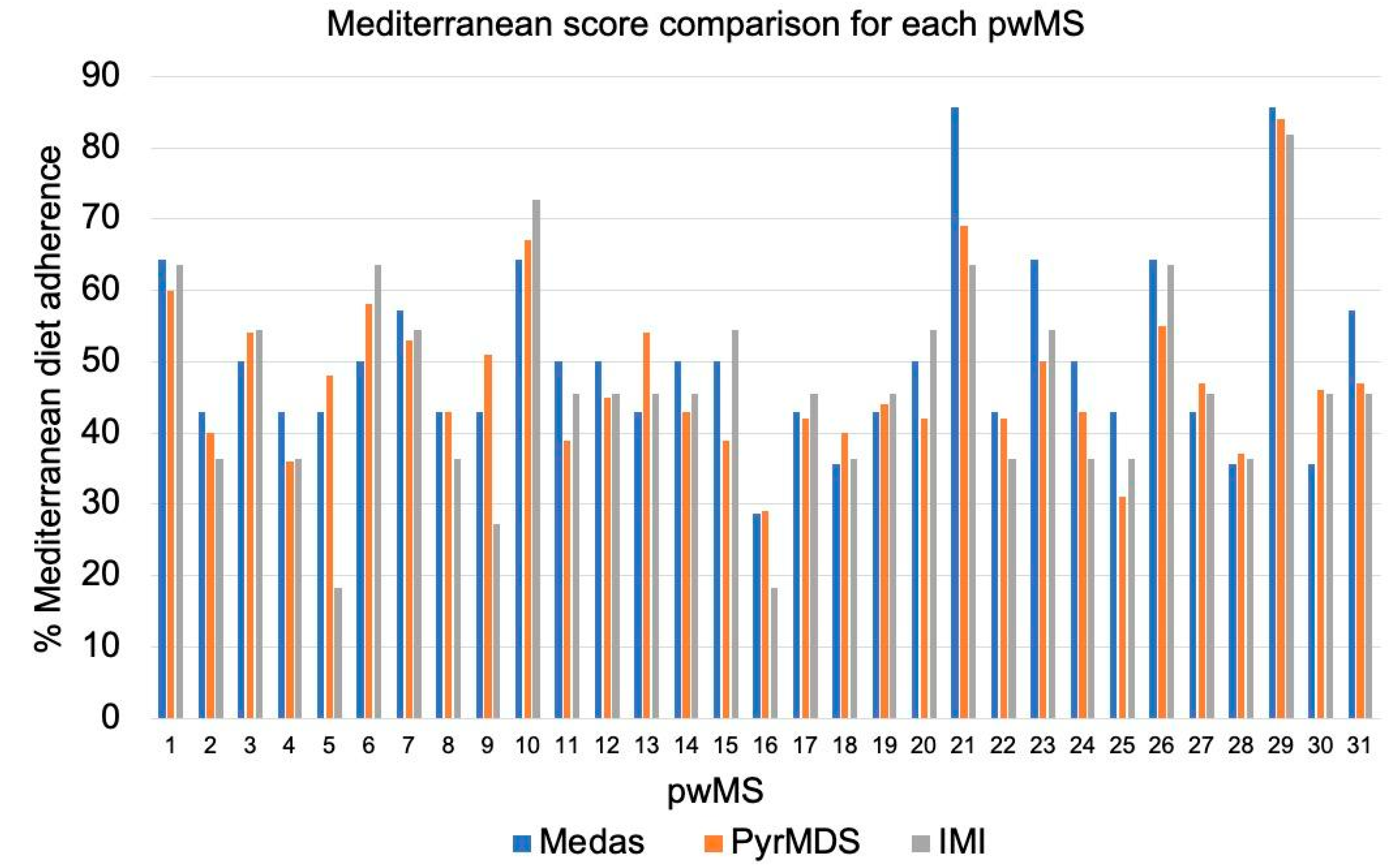
2.2. Mediterranean Diet Questionnaires
- -
- Fifteen item Pyramid-based Mediterranean Diet Score (PyrMDS) [17], which consists of 15 items and adopts the strategy of introducing different and continuous weights for both under- and over-consumption, but in a different way for each food item in order to quantify how they fit the 2011 version of the MD pyramid [14,18]. To estimate the adherence to the MD based on the PyrMDS, we used an open web-based tool [19].
- -
- Fourteen item Mediterranean Diet Adherence Screener (MEDAS) [20], which assesses typical consumption of healthful foods (e.g., olive oil, vegetables) and avoidance of unhealthy foods (e.g., red meat, butter). Patients receive a score of 1 or 0 for each item which is summed to derive a MEDAS score.
- -
2.3. Food Diaries
2.4. MS Clinical Scores
2.5. Statistical Analysis
3. Results
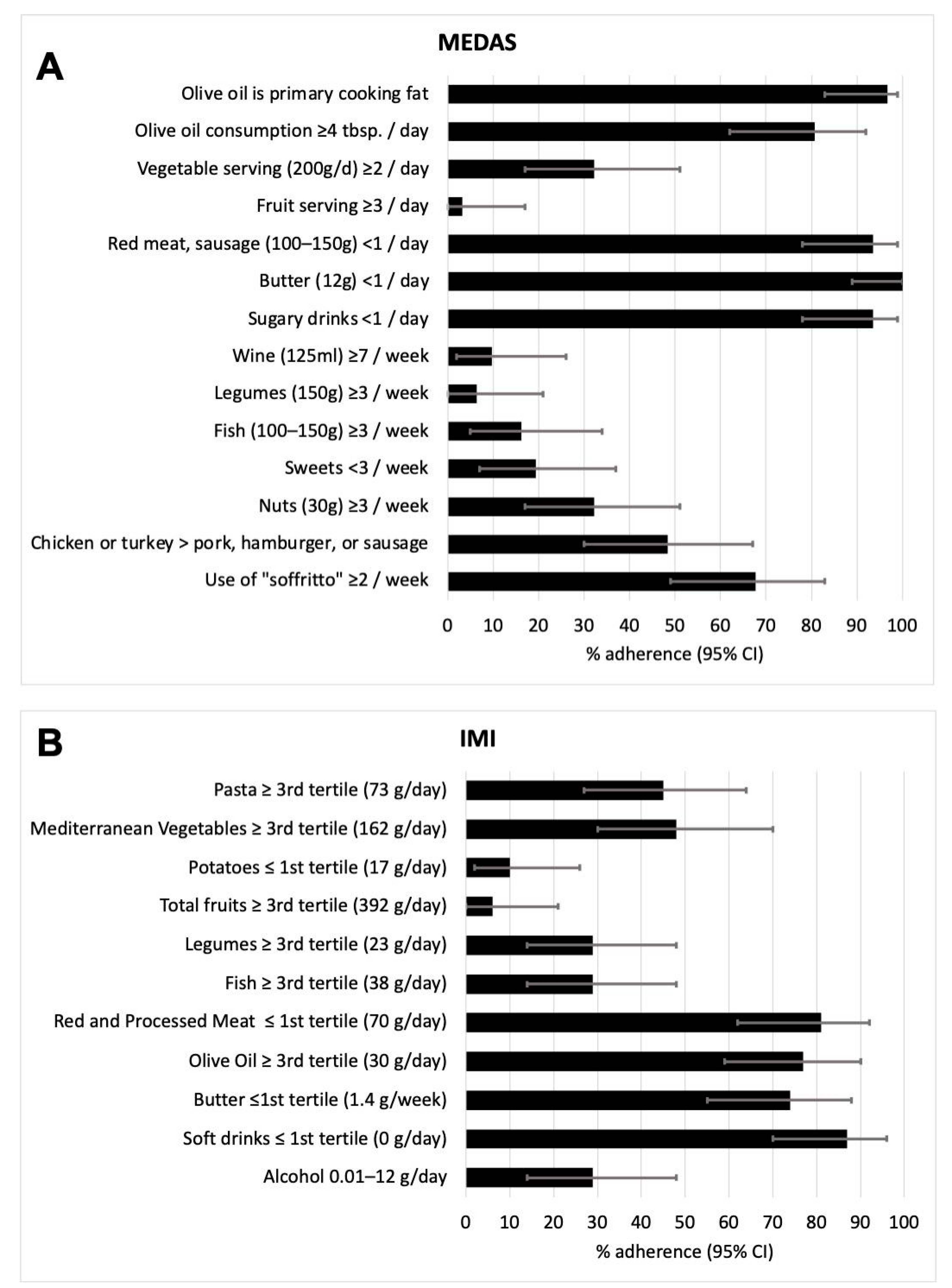
3.1. Dietary Pattern of the Population
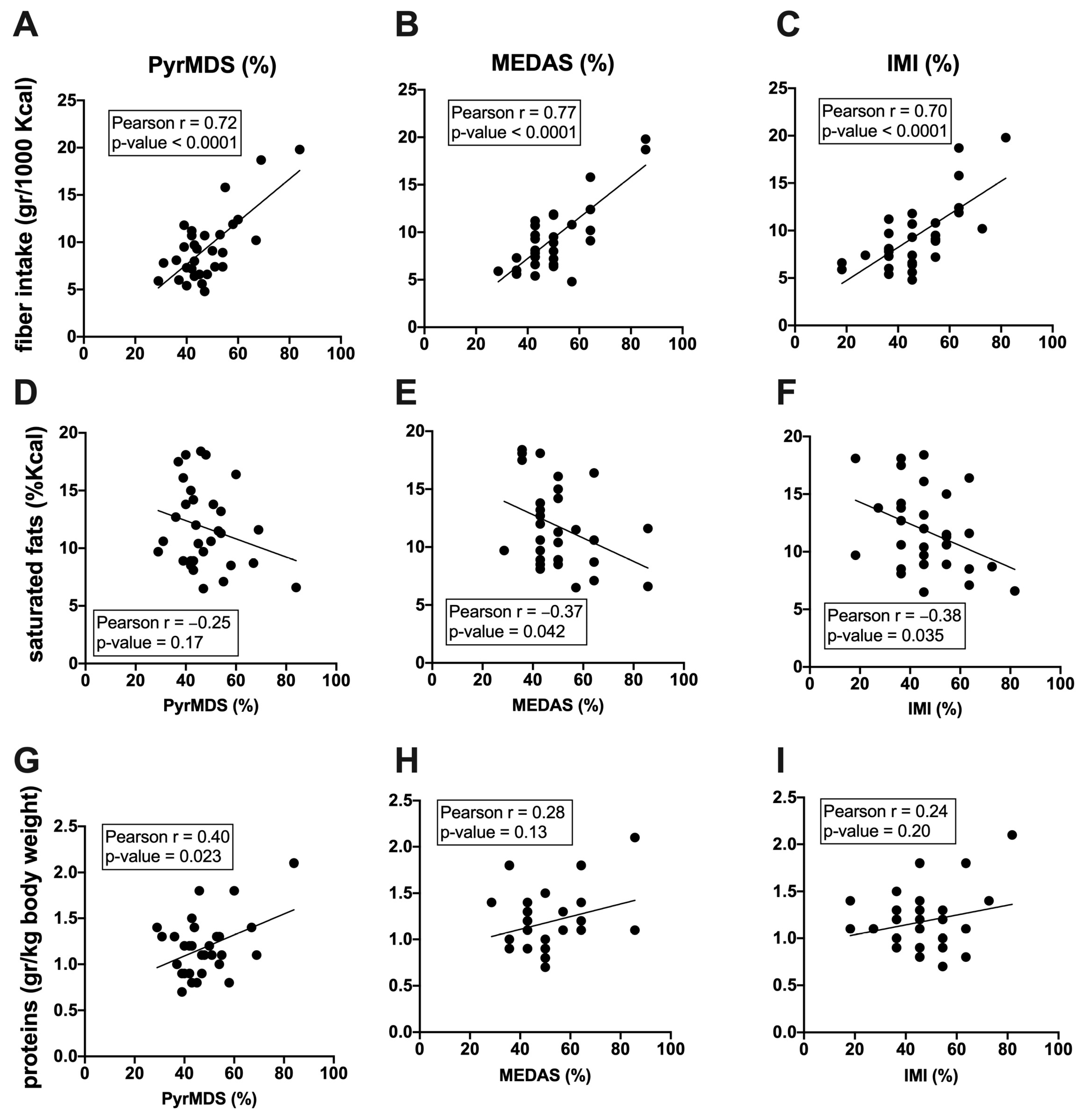
3.2. Adherence to MD Positively Correlates with Fiber and Protein Intake and Is Negatively Correlated with Saturated Fats Intake
3.3. Adherence to MD Is Associated to a Milder Disease Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olek, M.J. Multiple Sclerosis. Ann. Intern. Med. 2021, 174, ITC81–ITC96. [Google Scholar] [CrossRef]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of Multiple Sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Stoiloudis, P.; Kesidou, E.; Bakirtzis, C.; Sintila, S.-A.; Konstantinidou, N.; Boziki, M.; Grigoriadis, N. The Role of Diet and Interventions on Multiple Sclerosis: A Review. Nutrients 2022, 14, 1150. [Google Scholar] [CrossRef] [PubMed]
- Bronzini, M.; Maglione, A.; Rosso, R.; Matta, M.; Masuzzo, F.; Rolla, S.; Clerico, M. Feeding the Gut Microbiome: Impact on Multiple Sclerosis. Front. Immunol. 2023, 14, 1176016. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100.e11. [Google Scholar] [CrossRef]
- Choi, I.Y.; Piccio, L.; Childress, P.; Bollman, B.; Ghosh, A.; Brandhorst, S.; Suarez, J.; Michalsen, A.; Cross, A.H.; Morgan, T.E.; et al. Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms. Cell Rep. 2016, 15, 2136–2146. [Google Scholar] [CrossRef]
- Farez, M.F.; Fiol, M.P.; Gaitán, M.I.; Quintana, F.J.; Correale, J. Sodium Intake Is Associated with Increased Disease Activity in Multiple Sclerosis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.C.; Munger, K.L.; Hartung, H.P.; Freedman, M.S.; Montalbán, X.; Edan, G.; Wicklein, E.-M.; Radue, E.-W.; Kappos, L.; Pohl, C.; et al. Sodium Intake and Multiple Sclerosis Activity and Progression in BENEFIT. Ann. Neurol. 2017, 82, 20–29. [Google Scholar] [CrossRef]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean Diet and Multiple Health Outcomes: An Umbrella Review of Meta-Analyses of Observational Studies and Randomised Trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Katz Sand, I. The Role of Diet in Multiple Sclerosis: Mechanistic Connections and Current Evidence. Curr. Nutr. Rep. 2018, 7, 150–160. [Google Scholar] [CrossRef]
- Abbasi, H.; Shakouri, F.; Mosaddeghi-Heris, R.; Gholipour-Khalili, E.; Jahanshahlou, F.; Sanaie, S.; Naseri, A.; Talebi, M. Mediterranean-like Diets in Multiple Sclerosis: A Systematic Review. Rev. Neurol. 2023. [Google Scholar] [CrossRef]
- Katz Sand, I.; Levy, S.; Fitzgerald, K.; Sorets, T.; Sumowski, J.F. Mediterranean Diet Is Linked to Less Objective Disability in Multiple Sclerosis. Mult. Scler. 2023, 29, 248–260. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean Diet and Health: A Comprehensive Overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Chiriacò, M.; Tubili, C.; Bo, S.; Parillo, M.; Vetrani, C.; Mazzotti, A.; Pistis, D.; Marelli, G.; Grandone, I.; Natali, A. Critical Evaluation of the Questionnaires Assessing Adherence to the Mediterranean Diet That Are Based on Servings. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 724–736. [Google Scholar] [CrossRef] [PubMed]
- Agnoli, C.; Krogh, V.; Grioni, S.; Sieri, S.; Palli, D.; Masala, G.; Sacerdote, C.; Vineis, P.; Tumino, R.; Frasca, G.; et al. A Priori–Defined Dietary Patterns Are Associated with Reduced Risk of Stroke in a Large Italian Cohort1. J. Nutr. 2011, 141, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of Multiple Sclerosis: 2017 Revisions of the McDonald Criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Tong, T.Y.N.; Wareham, N.J.; Khaw, K.-T.; Imamura, F.; Forouhi, N.G. Prospective Association of the Mediterranean Diet with Cardiovascular Disease Incidence and Mortality and Its Population Impact in a Non-Mediterranean Population: The EPIC-Norfolk Study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean Diet Pyramid Today. Science and Cultural Updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef]
- Alimentazione e diabete. Available online: https://www.siditalia.it/divulgazione/alimentazione-e-diabete (accessed on 2 February 2024).
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women123. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Salvini, S.; Parpinel, M. Food Composition Database for Epidemiological Studies in Italy. Version 1.2022. Available online: http://www.bda-ieo.it/ (accessed on 2 February 2024).
- Società Italiana Di Nutrizione Umana (SINU) LARN: Livelli Di Assunzione Di Riferimento Di Nutrienti Ed Energia (2014) Milan. Available online: https://sinu.it/tabelle-larn-2014/ (accessed on 2 February 2024).
- Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS): Neurology: Vol 33, No 11. Available online: https://www.neurology.org/doi/10.1212/WNL.33.11.1444 (accessed on 2 February 2024).
- Roxburgh, R.H.S.R.; Seaman, S.R.; Masterman, T.; Hensiek, A.E.; Sawcer, S.J.; Vukusic, S.; Achiti, I.; Confavreux, C.; Coustans, M.; le Page, E.; et al. Multiple Sclerosis Severity Score. Neurology 2005, 64, 1144–1151. [Google Scholar] [CrossRef]
- Vitale, M.; Giosuè, A.; Vaccaro, O.; Riccardi, G. Recent Trends in Dietary Habits of the Italian Population: Potential Impact on Health and the Environment. Nutrients 2021, 13, 476. [Google Scholar] [CrossRef]
- Venasse, M.; Gauthier, A.; Giroux, I.; Pilutti, L.A. Dietary Intake and Characteristics in Persons with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 56, 103237. [Google Scholar] [CrossRef]
- SciELO—Brazil—Dietary Habits in a Group of Patients with Multiple Sclerosis Are Similar to Those of Healthy Control Subjects Dietary Habits in a Group of Patients with Multiple Sclerosis Are Similar to Those of Healthy Control Subjects. Available online: https://www.scielo.br/j/anp/a/qzGTBs9ZVQDzrV5z3GJrRZP/?lang=en (accessed on 2 February 2024).
- Felicetti, F.; Tommasin, S.; Petracca, M.; De Giglio, L.; Gurreri, F.; Ianniello, A.; Nistri, R.; Pozzilli, C.; Ruggieri, S. Eating Hubs in Multiple Sclerosis: Exploring the Relationship Between Mediterranean Diet and Disability Status in Italy. Front. Nutr. 2022, 9, 882426. [Google Scholar] [CrossRef]
- García-Conesa, M.-T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the Validity of the 14-Item Mediterranean Diet Adherence Screener (MEDAS): A Cross-National Study in Seven European Countries around the Mediterranean Region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Gorzynik-Debicka, M.; Przychodzen, P.; Cappello, F.; Kuban-Jankowska, A.; Marino Gammazza, A.; Knap, N.; Wozniak, M.; Gorska-Ponikowska, M. Potential Health Benefits of Olive Oil and Plant Polyphenols. Int. J. Mol. Sci. 2018, 19, 686. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.; Lonardo, M.S.; Cacciapuoti, N.; Muscariello, E.; Guida, B.; Faraonio, R.; Santillo, M.; Damiano, S. Dietary Polyphenols, Microbiome, and Multiple Sclerosis: From Molecular Anti-Inflammatory and Neuroprotective Mechanisms to Clinical Evidence. Int. J. Mol. Sci. 2023, 24, 7247. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi de Alvarenga, J.F.; Quifer-Rada, P.; Westrin, V.; Hurtado-Barroso, S.; Torrado-Prat, X.; Lamuela-Raventós, R.M. Mediterranean Sofrito Home-Cooking Technique Enhances Polyphenol Content in Tomato Sauce. J. Sci. Food Agric. 2019, 99, 6535–6545. [Google Scholar] [CrossRef] [PubMed]
- AlAmmar, W.A.; Albeesh, F.H.; Ibrahim, L.M.; Algindan, Y.Y.; Yamani, L.Z.; Khattab, R.Y. Effect of Omega-3 Fatty Acids and Fish Oil Supplementation on Multiple Sclerosis: A Systematic Review. Nutr. Neurosci. 2021, 24, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Tryfonos, C.; Pavlidou, E.; Vorvolakos, T.; Alexatou, O.; Vadikolias, K.; Mentzelou, M.; Tsourouflis, G.; Serdari, A.; Antasouras, G.; Papadopoulou, S.K.; et al. Association of Higher Mediterranean Diet Adherence With Lower Prevalence of Disability and Symptom Severity, Depression, Anxiety, Stress, Sleep Quality, Cognitive Impairment, and Physical Inactivity in Older Adults With Multiple Sclerosis. J. Geriatr. Psychiatry Neurol. 2023, 08919887231218754. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Sparaco, M.; Maniscalco, G.T.; Signoriello, E.; Lanzillo, R.; Russo, C.; Carmisciano, L.; Cepparulo, S.; Lavorgna, L.; Gallo, A.; et al. Lifestyle and Mediterranean Diet Adherence in a Cohort of Southern Italian Patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2021, 47, 102636. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, M.; Al-Qahtani, W.H.; Ferraris, C.; Grosso, G.; Fiorini, S.; Tavazzi, E.; Greco, G.; La Malfa, A.; Bergamaschi, R.; Tagliabue, A. Adherence to Mediterranean Diet Is Associated with Multiple Sclerosis Severity. Nutrients 2023, 15, 4009. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Kim, M.K.; Hwang, S.H.; Ahn, Y.; Shim, J.E.; Kim, D.H. Relative Validities of 3-Day Food Records and the Food Frequency Questionnaire. Nutr. Res. Pract. 2010, 4, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.J.; Davies, P.S.W. The Validity of Self-Reported Energy Intake as Determined Using the Doubly Labelled Water Technique. Br. J. Nutr. 2001, 85, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Capling, L.; Beck, K.L.; Gifford, J.A.; Slater, G.; Flood, V.M.; O’Connor, H. Validity of Dietary Assessment in Athletes: A Systematic Review. Nutrients 2017, 9, 1313. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | p-Value 3 | |
|---|---|---|---|
| n 1 | 20 (64.5) | 11 (35.5) | |
| Age 2 | 40.3 (12.6) | 36.2 (8.5) | 0.388 |
| Body Mass Index 2 | 23.2 (4.7) | 25.8 (3.4) | 0.112 |
| Smoking Status: current smokers 1 | 5 (20) | 6 (54.5) | 0.107 |
| Physical Activity | |||
| Sedentary 1 | 10 (50) | 4 (36.4) | 0.482 |
| Partially active 1 | 4 (20) | 5 (45.4) | 0.144 |
| Active 1 | 6 (30) | 2 (18) | 0.488 |
| Current MS therapy | |||
| Dimethyl fumarate 1 | 10 (32.2) | 7 (22.6) | |
| Cladribine 1 | 10 (32.2) | 4 (12.9) | |
| EDSS 2 | 1.6 (1.3) | 1.1 (0.9) | 0.335 |
| MSSS 2 | 3.5 (2.4) | 2.86 (2.34) | 0.460 |
| Disease duration 2 | 3.6 (5.2) | 1.5 (1.5) | 0.272 |
| Macronutrients | |||
| Energy Kcal 2 | 1804.3 (364) | 2120.7 (263.9) | 0.017 |
| Protein g/kg 2 | 1.3 (0.3) | 1 (0.2) | 0.027 |
| Carbohydrate % En 2 | 47 (5.3) | 46.6 (6.9) | 0.856 |
| Simple Sugar % En 2 | 16.4 (4.2) | 14.7 (4.9) | 0.327 |
| Fat % En 2 | 35.3 (4.4) | 36.8 (6.8) | 0.477 |
| Saturated fat % En 2 | 11.5 (3.3) | 12.4 (4.2) | 0.519 |
| Fiber g 2 | 18.3 (6.1) | 15.6 (4.5) | 0.200 |
| Fiber g/1000 Kcal 2 | 10.5 (3.8) | 7.4 (2.1) | 0.011 |
| Adherence to Mediterranean diet | |||
| MEDAS/14 2 | 7.35 (2.1) | 6.4 (0.9) | 0.153 |
| PyrMDS/15 2 | 7.38 (2) | 6.74 (1) | 0.326 |
| IMI/11 2 | 5.35 (1.7) | 4.73 (1.3) | 0.304 |
| MEDAS | Q1 | Q2 | Q3 | Q4 |
| % of participants | 0 | 48.4 (15) | 45.2 (14) | 6.4 (2) |
| Average range value | 40.5 | 55.1 | 85.7 | |
| Median value range | 42.9 | 50.0 | 85.7 | |
| Interquartile Range | (35.7–42.9) | (50–64.3) | 85.7 | |
| PyrMDS | Q1 | Q2 | Q3 | Q4 |
| % of participants | 0 | 64.5 (20) | 32.2 (10) | 3.2 (1) |
| Average range value | 41.15 | 57.1 | 84 | |
| Median value range | 42 | 54.5 | 84 | |
| Interquartile Range | (29–47) | (50–67) | ||
| IMI | Q1 | Q2 | Q3 | Q4 |
| % of participants | 6.4 (2) | 58.1 (18) | 32.2 (10) | 3.2 (1) |
| Average range value | 18.2 | 40.4 | 60.0 | 81.8 |
| Median value range | 18.2 | 41.0 | 59.1 | 81.8 |
| Interquartile Range | 18.2 | (27.3–45.5) | (54.5–63.6) |
| Association between MSSS and Adherence to MD | |||
|---|---|---|---|
| Variable | Beta Coefficients | Standard Error | p-Value |
| Age (Years) | 0.07111 | 0.04149 | 0.1037 |
| Sex Female Male | Ref 0.09695 | 1.03061 | 0.9261 |
| BMI | −0.13093 | 0.11207 | 0.2579 |
| Physical activity Sedentary Partially active Active | Ref −1.46971 −1.26458 | 1.06682 1.13506 | 0.1852 0.2799 |
| MEDAS | −0.13303 | 0.05605 | 0.0290 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bronzini, M.; Maglione, A.; Rosso, R.; Masuzzo, F.; Matta, M.; Meroni, R.; Rolla, S.; Clerico, M. Lower Multiple Sclerosis Severity Score Is Associated with Higher Adherence to Mediterranean Diet in Subjects with Multiple Sclerosis from Northwestern Italy. Nutrients 2024, 16, 880. https://doi.org/10.3390/nu16060880
Bronzini M, Maglione A, Rosso R, Masuzzo F, Matta M, Meroni R, Rolla S, Clerico M. Lower Multiple Sclerosis Severity Score Is Associated with Higher Adherence to Mediterranean Diet in Subjects with Multiple Sclerosis from Northwestern Italy. Nutrients. 2024; 16(6):880. https://doi.org/10.3390/nu16060880
Chicago/Turabian StyleBronzini, Matteo, Alessandro Maglione, Rachele Rosso, Federica Masuzzo, Manuela Matta, Raffaella Meroni, Simona Rolla, and Marinella Clerico. 2024. "Lower Multiple Sclerosis Severity Score Is Associated with Higher Adherence to Mediterranean Diet in Subjects with Multiple Sclerosis from Northwestern Italy" Nutrients 16, no. 6: 880. https://doi.org/10.3390/nu16060880
APA StyleBronzini, M., Maglione, A., Rosso, R., Masuzzo, F., Matta, M., Meroni, R., Rolla, S., & Clerico, M. (2024). Lower Multiple Sclerosis Severity Score Is Associated with Higher Adherence to Mediterranean Diet in Subjects with Multiple Sclerosis from Northwestern Italy. Nutrients, 16(6), 880. https://doi.org/10.3390/nu16060880