

Vitamin D Status in the Adult Population of Romania—Results of the European Health Examination Survey
 and
and
Abstract
1. Introduction
2. Methodology
Study Design and Setting
3. Study Population
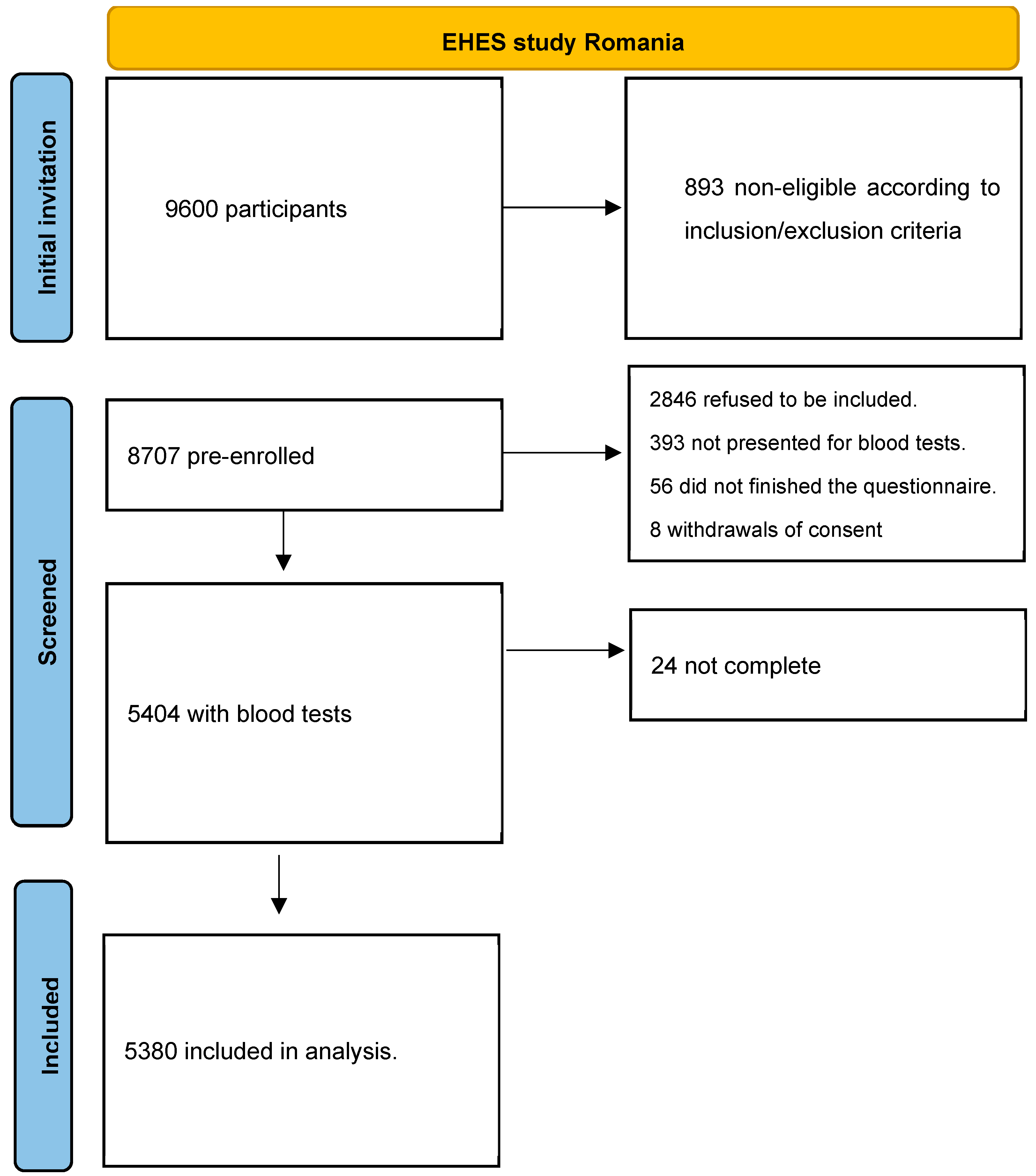
3.1. Selection of Participants
3.2. Data Collection Method
3.3. Data Analysis
3.4. Ethical Approval
4. Results
5. Discussion
6. Conclusions
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080s–1086s. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.A.; Cooper, C.; Ebeling, P.R.; Eggersdorfer, M.; Hilger, J.; Hoffmann, K.; Josse, R.; Kanis, J.A.; Mithal, A.; Pierroz, D.D.; et al. A global representation of vitamin D status in healthy populations. Arch. Osteoporos. 2012, 7, 155–172. [Google Scholar] [CrossRef]
- Díaz-Rizzolo, D.A.; Kostov, B.; Gomis, R.; Sisó-Almirall, A. Paradoxical suboptimal vitamin D levels in a Mediterranean area: A population-based study. Sci. Rep. 2022, 12, 19645. [Google Scholar] [CrossRef]
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689s–1696s. [Google Scholar] [CrossRef]
- Edwards, M.H.; Cole, Z.A.; Harvey, N.C.; Cooper, C. The global epidemiology of vitamin D status. J. Aging Res. Clin. Pract. 2014, 3, 148–158. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A.; Sundus, S.; Bachuwa, G.; Alkotob, M.L.; et al. Vitamin D Supplementation and Cardiovascular Disease Risks in More Than 83,000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [CrossRef]
- Pilz, S.; Trummer, C.; Theiler-Schwetz, V.; Grübler, M.R.; Verheyen, N.D.; Odler, B.; Karras, S.N.; Zittermann, A.; März, W. Critical Appraisal of Large Vitamin D Randomized Controlled Trials. Nutrients 2022, 14, 303. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Yang, M. Trends of serum 25(OH) vitamin D and association with cardiovascular disease and all-cause mortality: From NHANES survey cycles 2001–2018. Front. Nutr. 2024, 11, 1328136. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Staten, M.A.; Knowler, W.C.; Nelson, J.; Vickery, E.M.; LeBlanc, E.S.; Neff, L.M.; Park, J.; Pittas, A.G.; D2d Research Group. Intratrial Exposure to Vitamin D and New-Onset Diabetes among Adults with Prediabetes: A Secondary Analysis from the Vitamin D and Type 2 Diabetes (D2d) Study. Diabetes Care 2020, 43, 2916–2922. [Google Scholar] [CrossRef]
- Valer-Martinez, A.; Martinez, J.A.; Sayon-Orea, C.; Galvano, F.; Grosso, G.; Bes-Rastrollo, M. Vitamin D and Cardio-Metabolic Risk Factors in Overweight Adults: An Overview of the Evidence. Curr. Pharm. Des. 2019, 25, 2407–2420. [Google Scholar] [CrossRef]
- Win, S.S.; Camargo, C.A., Jr.; Khaw, K.T.; Lawes, C.M.M.; Sluyter, J.; Waayer, D.; Toop, L.; Scragg, R. Cross-sectional associations of vitamin D status with asthma prevalence, exacerbations, and control in New Zealand adults. J. Steroid Biochem. Mol. Biol. 2019, 188, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chandler, P.D.; Chen, W.Y.; Ajala, O.N.; Hazra, A.; Cook, N.; Bubes, V.; Lee, I.-M.; Giovannucci, E.L.; Willett, W.; Buring, J.E.; et al. Effect of Vitamin D3 Supplements on Development of Advanced Cancer: A Secondary Analysis of the VITAL Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2025850. [Google Scholar] [CrossRef]
- Muñoz, A.; Grant, W.B. Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms. Nutrients 2022, 14, 1448. [Google Scholar] [CrossRef]
- Holick, M.F. The Death D-Fying Vitamin D3 for Digestive Tract Cancers—The p53 Antibody Connection. JAMA Netw. Open 2023, 6, e2328883. [Google Scholar] [CrossRef]
- Kanno, K.; Akutsu, T.; Ohdaira, H.; Suzuki, Y.; Urashima, M. Effect of Vitamin D Supplements on Relapse or Death in a p53-Immunoreactive Subgroup with Digestive Tract Cancer: Post Hoc Analysis of the AMATERASU Randomized Clinical Trial. JAMA Netw. Open 2023, 6, e2328886. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Wang, R.; Mao, D.; Chen, J.; Li, M.; Li, W.; Yang, X.; Yang, L. Vitamin D Status and Associated Factors of Older Adults in the Cross-Sectional 2015–2017 Survey. Nutrients 2023, 15, 4476. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Lazaretti-Castro, M.; Lips, P.; Marcocci, C.; Bilezikian, J.P. Vitamin D in the older population: A consensus statement. Endocrine 2023, 79, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Harse, J.D.; Zhu, K.; Bucks, R.S.; Hunter, M.; Lim, E.M.; Cooke, B.R.; Walsh, J.P.; Murray, K. Investigating Potential Dose-Response Relationships between Vitamin D Status and Cognitive Performance: A Cross-Sectional Analysis in Middle- to Older-Aged Adults in the Busselton Healthy Ageing Study. Int. J. Environ. Res. Public Health 2021, 19, 450. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.W.; Niles, J.K.; Kroll, M.H.; Bi, C.; Holick, M.F. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS ONE 2020, 15, e0239252. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.-Y.; Mulick, A.; Mathur, R.; Smeeth, L.; Warren-Gash, C.; Langan, S. The association between vitamin D status and COVID-19 in England: A cohort study using UK Biobank. PLoS ONE 2022, 17, e0269064. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Rosen, C.J. Vitamin D: 100 years of discoveries, yet controversy continues. Lancet Diabetes Endocrinol. 2023, 11, 362–374. [Google Scholar] [CrossRef]
- Cashman, K.D.; Kiely, M. Towards prevention of vitamin D deficiency and beyond: Knowledge gaps and research needs in vitamin D nutrition and public health. Br. J. Nutr. 2011, 106, 1617–1627. [Google Scholar] [CrossRef]
- Kimball, S.M.; Holick, M.F. Official recommendations for vitamin D through the life stages in developed countries. Eur. J. Clin. Nutr. 2020, 74, 1514–1518. [Google Scholar] [CrossRef]
- Lips, P.; de Jongh, R.T.; van Schoor, N.M. Trends in Vitamin D Status Around the World. JBMR Plus 2021, 5, e10585. [Google Scholar] [CrossRef]
- Mendoza-Garcés, L.; Velázquez-Alva, M.C.; Cabrer-Rosales, M.F.; Arrieta-Cruz, I.; Gutiérrez-Juárez, R.; Irigoyen-Camacho, M.E. Vitamin D Deficiency is Associated with Handgrip Strength, Nutritional Status and T2DM in Community-Dwelling Older Mexican Women: A Cross-Sectional Study. Nutrients 2021, 13, 736. [Google Scholar] [CrossRef]
- Yan, X.; Zhang, N.; Cheng, S.; Wang, Z.; Qin, Y. Gender Differences in Vitamin D Status in China. Med. Sci. Monit. 2019, 25, 7094–7099. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Sai, A.J. Vitamin D insufficiency, deficiency, and bone health. J. Clin. Endocrinol. Metab. 2010, 95, 2630–2633. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. Med. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Sempos, C.T.; Vesper, H.W.; Phinney, K.W.; Thienpont, L.M.; Coates, P.M. Vitamin D status as an international issue: National surveys and the problem of standardization. Scand. J. Clin. Lab. Investig. Suppl. 2012, 243, 32–40. [Google Scholar]
- Acherjya, G.K.; Ali, M.; Tarafder, K.; Akhter, N.; Chowdhury, M.K.; Islam, D.U.; Rahman, M.H.; Miah, M.T. Study of Vitamin D Deficiency among the Apparently Healthy Population in Jashore, Bangladesh. Mymensingh Med. J. 2019, 28, 214–221. [Google Scholar]
- Akinlawon, O.J.; Lai, C.Q.; Noel, S.E.; Flanagan, K.D.; Tucker, K.L. Risk Factors Associated with Vitamin D Status among Older Puerto Rican Adults. J. Nutr. 2021, 151, 999–1007. [Google Scholar] [CrossRef]
- Farhat, K.H.; Arafa, M.A.; Rabah, D.M.; Amin, H.S.; Ibrahim, N.K. Vitamin D status and its correlates in Saudi male population. BMC Public Health 2019, 19, 211. [Google Scholar] [CrossRef]
- Gill, T.K.; Hill, C.L.; Shanahan, E.M.; Taylor, A.W.; Appleton, S.L.; Grant, J.F.; Shi, Z.; Dal Grande, E.; Price, K.; Adams, R.J. Vitamin D levels in an Australian population. BMC Public Health 2014, 14, 1001. [Google Scholar] [CrossRef]
- Hutchings, N.; Babalyan, V.; Heijboer, A.C.; Baghdasaryan, S.; Qefoyan, M.; Ivanyan, A.; Ackermans, M.T.; Formenti, A.M.; Lesnyak, O.; Giustina, A.; et al. Vitamin D status in Armenian women: A stratified cross-sectional cluster analysis. Eur. J. Clin. Nutr. 2022, 76, 220–226. [Google Scholar] [CrossRef]
- Jiang, W.; Wu, D.B.; Xiao, G.B.; Ding, B.; Chen, E.Q. An epidemiology survey of vitamin D deficiency and its influencing factors. Med. Clin. 2020, 154, 7–12. [Google Scholar] [CrossRef]
- Kamińska, S.; Pikala, M.; Dziankowska-Zaborszczyk, E.; Bielecki, W.; Rębowska, E.; Kozakiewicz, K.; Nadrowski, P.; Drygas, W.; Kwaśniewska, M. Vitamin D—Dietary intake, supplementation and metabolic status of Polish adults. Int. J. Occup. Med. Environ. Health 2020, 33, 107–118. [Google Scholar] [CrossRef]
- Leão, L.; Rodrigues, B.C.; Dias, P.T.P.; Gehrke, B.; Souza, T.; Hirose, C.K.; Freire, M.D.C. Vitamin D status and prevalence of hypovitaminosis D in different genders throughout life stages: A Brazilian cross-sectional study. Clinics 2021, 76, e2571. [Google Scholar] [CrossRef]
- Lee, M.J.; Hsu, H.J.; Wu, I.W.; Sun, C.Y.; Ting, M.K.; Lee, C.C. Vitamin D deficiency in northern Taiwan: A community-based cohort study. BMC Public Health 2019, 19, 337. [Google Scholar] [CrossRef]
- Lin, L.Y.; Smeeth, L.; Langan, S.; Warren-Gash, C. Distribution of vitamin D status in the UK: A cross-sectional analysis of UK Biobank. BMJ Open 2021, 11, e038503. [Google Scholar] [CrossRef]
- Petrenya, N.; Lamberg-Allardt, C.; Melhus, M.; Broderstad, A.R.; Brustad, M. Vitamin D status in a multi-ethnic population of northern Norway: The SAMINOR 2 Clinical Survey. Public Health Nutr. 2020, 23, 1186–1200. [Google Scholar] [CrossRef]
- Siddiqee, M.H.; Bhattacharjee, B.; Siddiqi, U.R.; MeshbahurRahman, M. High prevalence of vitamin D deficiency among the South Asian adults: A systematic review and meta-analysis. BMC Public Health 2021, 21, 1823. [Google Scholar] [CrossRef]
- Smirnova, D.V.; Rehm, C.D.; Fritz, R.D.; Kutepova, I.S.; Soshina, M.S.; Berezhnaya, Y.A. Vitamin D status of the Russian adult population from 2013 to 2018. Sci. Rep. 2022, 12, 16604. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Wu, Y.; Rao, J.; Hu, H.; Wang, C.; Wu, J.; Shi, Y.; Fu, Y.; Cheng, X.; Li, P. Associations among vitamin D, tobacco smoke, and hypertension: A cross-sectional study of the NHANES 2001–2016. Hypertens. Res. 2022, 45, 1986–1996. [Google Scholar] [CrossRef] [PubMed]
- Herrick, K.A.; Storandt, R.; Afful, J.; Pfeiffer, C.M.; Schleicher, R.L.; Gahche, J.J.; Potischman, N. Vitamin D status in the United States, 2011–2014. Am. J. Clin. Nutr. 2019, 110, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Rooney, M.R.; Harnack, L.; Michos, E.D.; Ogilvie, R.P.; Sempos, C.T.; Lutsey, P.L. Trends in Use of High-Dose Vitamin D Supplements Exceeding 1000 or 4000 International Units Daily, 1999–2014. JAMA J. Am. Med. Assoc. 2017, 317, 2448–2450. [Google Scholar] [CrossRef] [PubMed]
- OECD; European Observatory on Health Systems and Policies. Romania: Country Health Profile 2023; OECD: Paris, France, 2023. [Google Scholar]
- Ministry of Health. Ghid Privind Evaluarea Statusului Vitaminei D la Adulti. Available online: https://oldsite.ms.ro/wp-content/uploads/2019/07/Anexa2-Ghid-pentru-evaluarea-statusului-vitaminei-D-la-adulti-1-1.pdf (accessed on 15 January 2024).
- Ministry of Health. Activity Report of the Ministry of Health for 2022, p. 561. Available online: https://ms.ro/ro/informatii-de-interes-public/rapoarte/rapoarte-de-activitate/ (accessed on 15 January 2024).
- Kuulasmaa, K.; Tolonen, H. What Is EHES and Why It Is Needed? National Institute for Health and Welfare: Helsinki, Finland, 2013. [Google Scholar]
- Tolonen, H.; Koponen, P.; Al-kerwi, A.a.; Capkova, N.; Giampaoli, S.; Mindell, J.; Paalanen, L.; Ruiz-Castell, M.; Trichopoulou, A.; Kuulasmaa, K.; et al. European health examination surveys—A tool for collecting objective information about the health of the population. Arch. Public Health 2018, 76, 38. [Google Scholar] [CrossRef]
- Guga, Ș.; Mihăilescu, A.; Spatari, M. Coșul Minim de Consum Lunar Pentru un Trai Decent Pentru Populația României; Friedrich-Ebert Stiftung: Berlin, Germany, 2018; Volume 24, p. 2021. [Google Scholar]
- Institutul National de Sanatate Publica, Home Page-Proiecte in Derulare. The Methodology of Implementation of the European Health Survey (EHES) in Romania. Available online: https://proiect-pdp1.insp.gov.ro/ancheta-europeana-de-examinare-a-starii-de-sanatate-ehes/ (accessed on 15 January 2024).
- Souberbielle, J.C.; Massart, C.; Brailly-Tabard, S.; Cavalier, E.; Chanson, P. Prevalence and determinants of vitamin D deficiency in healthy French adults: The VARIETE study. Endocrine 2016, 53, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Rabenberg, M.; Scheidt-Nave, C.; Busch, M.A.; Rieckmann, N.; Hintzpeter, B.; Mensink, G.B. Vitamin D status among adults in Germany--Results from the German Health Interview and Examination Survey for Adults (DEGS1). BMC Public Health 2015, 15, 641. [Google Scholar] [CrossRef]
- Bouloukaki, I.; Markakis, M.; Pateli, R.; Lyronis, I.; Schiza, S.; Tsiligianni, I. Vitamin D levels in primary care patients: Correlations with clinical, seasonal, and quality-of-life parameters. Fam. Pract. 2022, 39, 678–684. [Google Scholar] [CrossRef] [PubMed]
- României, C. Administrația Natională de Meteorologie; Editura Academiei Române Bucureşti: București, Romania, 2008. [Google Scholar]
- Engelsen, O. The Relationship between ultraviolet radiation exposure and vitamin D status. Nutrients 2010, 2, 482–495. [Google Scholar] [CrossRef] [PubMed]
- Zugravu, C.A.; Soptica, F.; Tarcea, M.; Cucu, A. Pertinence of vitamin D supplementation in the adult Romanian population. Farmacia 2016, 64, 467–472. [Google Scholar]
- Haq, A.; Svobodová, J.; Imran, S.; Stanford, C.; Razzaque, M.S. Vitamin D deficiency: A single centre analysis of patients from 136 countries. J. Steroid Biochem. Mol. Biol. 2016, 164, 209–213. [Google Scholar] [CrossRef]
- da Silveira, E.A.; Moura, L.; Castro, M.C.R.; Kac, G.; Hadler, M.; Noll, P.; Noll, M.; Rezende, A.T.O.; Delpino, F.M.; Oliveira, C. Prevalence of Vitamin D and Calcium Deficiency and Insufficiency in Women of Childbearing Age and Associated Risk Factors: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 4351. [Google Scholar] [CrossRef]
- Rostami, M.; Tehrani, F.R.; Simbar, M.; Bidhendi Yarandi, R.; Minooee, S.; Hollis, B.W.; Hosseinpanah, F. Effectiveness of Prenatal Vitamin D Deficiency Screening and Treatment Program: A Stratified Randomized Field Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2936–2948. [Google Scholar] [CrossRef]
- Hollis, B.W.; Johnson, D.; Hulsey, T.C.; Ebeling, M.; Wagner, C.L. Vitamin D supplementation during pregnancy: Double-blind, randomized clinical trial of safety and effectiveness. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2011, 26, 2341–2357. [Google Scholar] [CrossRef]
- Anagnostis, P.; Livadas, S.; Goulis, D.G.; Bretz, S.; Ceausu, I.; Durmusoglu, F.; Erkkola, R.; Fistonic, I.; Gambacciani, M.; Geukes, M.; et al. EMAS position statement: Vitamin D and menopausal health. Maturitas 2023, 169, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Danese, V.C.; Pepe, J.; Ferrone, F.; Colangelo, L.; De Martino, V.; Nieddu, L.; Ferrazza, G.; Panzini, E.; Pascone, R.; Blocki, F.; et al. The Mutual Interplay between Bone, Glucose and Lipid Metabolism: The Role of Vitamin D and PTH. Nutrients 2023, 15, 2998. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Overall (n = 5380) | Male (n = 2315) | Female (n = 3065) | p-Value |
|---|---|---|---|---|
| 25(OH)D (ng/mL) (mean ± SD) | 26.6 ± 9.5 | 28.0 ± 9.8 | 25.2 ± 8.9 | <0.001 |
| Age (mean ± SD) | 45.1 ± 10.9 | 44.8 ± 10.8 | 45.4 ± 11.0 | 0.063 |
| Age group (%) | 0.221 | |||
| 25–34 years | 1012 (21.2) | 422 (21.6) | 590 (20.8) | |
| 35–44 years | 1465 (26.3) | 650 (26.9) | 815 (25.7) | |
| 45–54 years | 1637 (30.4) | 714 (30.6) | 923 (30.2) | |
| 55–64 years | 1266 (22.2) | 529 (20.9) | 737 (23.4) | |
| Residence (%) | 0.001 | |||
| Urban | 2927 (53.2) | 1283 (50.8) | 1644 (55.7) | |
| Rural | 2453 (46.8) | 1032 (49.2) | 1421 (44.3) | |
| Education (%) | <0.001 | |||
| ≤12 | 3118 (58.6) | 1382 (61.3) | 1736 (55.8) | |
| >12 | 2262 (41.4) | 933 (38.7) | 1329 (44.2) | |
| Income (%) | 0.001 | |||
| Low | 3462 (63.7) | 1406 (61.1) | 2056 (66.4) | |
| Over basic living expenses | 796 (14.9) | 391 (16.2) | 405 (13.4) | |
| Do not declare | 1122 (21.4) | 518 (22.7) | 604 (20.2) | |
| BMI (kg/m2) (mean ± SD) | 28.1 ± 5.9 | 28.6 ± 5.5 | 27.6 ± 6.2 | <0.001 |
| Underweight N (%) | 103 (1.7) | 14 (0.6) | 89 (2.9) | <0.001 |
| Normal N (%) | 1616 (29.6) | 557 (24.5) | 1059 (34.7) | |
| Overweight N (%) | 1904 (36.1) | 933 (40.3) | 971 (31.8) | |
| Obese N (%) | 1741 (32.6) | 805 (34.6) | 936 (30.6) | |
| Smoking status (%) | <0.001 | |||
| Non-smoker | 3305 (78.7) | 1170 (70.5) | 2135 (86.1) | |
| Smoker | 831 (21.3) | 492 (29.5) | 339 (13.9) | |
| Alcohol consumption (%) | <0.001 | |||
| Never drink | 2102 (36.5) | 444 (19.2) | 1658 (54.1) | |
| Drink occasionally | 1854 (34.9) | 800 (34.8) | 1054 (34.9) | |
| Drink frequently | 1392 (28.6) | 1058 (46.0) | 334 (11.0) | |
| Binge drinking | 1124 (37.3) | 943 (51.0) | 181 (13.0) | <0.001 |
| Comorbidities (%) | ||||
| HBP * | 1342 (24.2) | 614 (25.0) | 728 (23.3) | 0.170 |
| T2DM ** | 310 (5.6) | 177 (7.1) | 133 (4.2) | <0.001 |
| H-Chol *** | 1152 (21.0) | 540 (22.2) | 612 (19.8) | 0.042 |
| Month | 0.270 | |||
| August | 50 (1.0) | 16 (0.9) | 34 (1.0) | |
| September | 3563 (66.1) | 1508 (65.2) | 2055 (67.1) | |
| October | 1767 (32.9) | 791 (33.9) | 976 (31.9) |
| Variables | Vitamin D Deficiency (<20 ng/mL) | Vitamin D Insufficiency (20–30 ng/mL) | Vitamin D Sufficiency (>30 ng/mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Male | Female | Overall | Male | Female | Overall | Male | Female | |
| Overall | 24.8 | 20.2 | 29.4 | 44.3 | 42.5 | 46.1 | 30.9 | 37.3 | 24.5 |
| Age group | |||||||||
| 25–34 years | 25.5 | 22.5 | 28.6 | 44.8 | 43.6 | 46.2 | 29.7 | 34.0 | 25.2 |
| 35–44 years | 23.7 | 19.7 | 27.9 | 45.6 | 43.8 | 47.5 | 30.7 | 36.5 | 24.6 |
| 45–54 years | 24.7 | 19.3 | 30.3 | 43.8 | 41.4 | 46.3 | 31.5 | 39.3 | 23.4 |
| 55–64 years | 25.4 | 19.8 | 30.3 | 42.9 | 41.3 | 44.3 | 31.8 | 38.9 | 25.3 |
| Residence | |||||||||
| Urban | 26.5 | 23.0 | 29.8 | 43.5 | 42.7 | 44.3 | 30.0 | 34.3 | 25.9 |
| Rural | 22.7 | 17.3 | 28.8 | 45.2 | 42.4 | 48.4 | 32.1 | 40.3 | 22.8 |
| Education | |||||||||
| ≤12 | 25.9 | 19.8 | 32.6 | 44.1 | 42.2 | 46.4 | 30.0 | 38.0 | 21.0 |
| >12 | 23.2 | 20.9 | 25.3 | 44.5 | 43.1 | 45.8 | 32.2 | 36.0 | 28.9 |
| Income | |||||||||
| Low | 25.7 | 19.5 | 31.5 | 45.1 | 43.8 | 46.4 | 29.1 | 36.7 | 22.0 |
| Over basic living expenses | 21.2 | 19.9 | 22.7 | 44.9 | 43.1 | 47.0 | 33.9 | 37.0 | 30.2 |
| Do not declare | 24.4 | 22.3 | 26.8 | 41.4 | 38.7 | 44.5 | 34.2 | 39.1 | 28.7 |
| BMI * | |||||||||
| Underweight | 29.3 | 26.7 | 29.9 | 42.7 | 26.7 | 46.3 | 28.0 | 46.7 | 23.9 |
| Normal | 23.7 | 20.5 | 25.9 | 42.9 | 39.3 | 45.5 | 33.4 | 40.2 | 28.6 |
| Overweight | 21.0 | 17.8 | 25.3 | 45.1 | 43.4 | 47.2 | 33.9 | 38.8 | 27.5 |
| Obese | 29.5 | 22.5 | 37.4 | 44.9 | 43.9 | 45.9 | 25.7 | 33.6 | 16.6 |
| Smoking status | |||||||||
| Never smoker | 25.1 | 19.1 | 29.6 | 45.3 | 43.1 | 46.9 | 29.6 | 37.8 | 23.5 |
| Smoker > 1 year | 23.7 | 23.0 | 25.2 | 41.3 | 39.3 | 45.1 | 35.0 | 37.7 | 29.7 |
| Alcohol consumption | |||||||||
| Never | 30.0 | 24.1 | 32.1 | 45.4 | 41.9 | 46.7 | 24.6 | 34.1 | 21.2 |
| Occasionally | 23.0 | 19.6 | 26.3 | 45.7 | 46.0 | 45.4 | 31.3 | 34.4 | 28.3 |
| Frequently | 20.2 | 18.9 | 25.7 | 41.2 | 40.1 | 45.6 | 38.6 | 40.9 | 28.7 |
| Binge drinking | 21.2 | 20.0 | 29.9 | 40.4 | 39.9 | 43.8 | 32.3 | 35.9 | 28.7 |
| Comorbidities | |||||||||
| HBP ** | 25.3 | 21.0 | 30.0 | 43.0 | 40.8 | 45.3 | 31.7 | 38.2 | 24.6 |
| T2DM *** | 25.9 | 23.4 | 30.3 | 44.4 | 43.9 | 45.5 | 29.6 | 32.7 | 24.2 |
| H-Chol **** | 25.5 | 21.1 | 30.5 | 24.6 | 20.0 | 29.1 | 33.1 | 37.4 | 28.2 |
| Month | |||||||||
| August | 6.5 | 4.8 | 8.0 | 41.3 | 23.8 | 56.0 | 52.2 | 71.4 | 36.0 |
| September | 23.5 | 19.5 | 27.4 | 43.2 | 39.4 | 46.9 | 33.3 | 41.1 | 25.8 |
| October | 27.9 | 22.0 | 34.3 | 46.6 | 48.8 | 44.3 | 25.5 | 29.2 | 21.5 |
| Variables | OR of Vitamin D Deficiency | OR of Vitamin D Insufficiency | ||||
|---|---|---|---|---|---|---|
| Overall | Male | Female | Overall | Male | Female | |
| Age group | ||||||
| 25–34 years | 1 | 1 | 1 | 1 | 1 | 1 |
| 35–44 years | 0.89 (0.72–1.12) | 0.81 (0.59–1.11) | 0.99 (0.72–1.38) | 0.99 (0.81–1.20) | 0.94 (0.72–1.21) | 1.06 (0.79–1.42) |
| 45–54 years | 0.91 (0.74–1.13) | 0.74 (0.54–1.01) | 1.14 (0.83–1.56) | 0.92 (0.76–1.11) | 0.82 (0.63–1.05) | 1.09 (0.82–1.45) |
| 55–64 years | 0.93 (0.74–1.17) | 0.77 (0.55–1.08) | 1.06 (0.76–1.47) | 0.89 (0.73–1.10) | 0.83 (0.63–1.09) | 0.96 (0.71–1.30) |
| Residence | ||||||
| Urban | 1 | 1 | 1 | 1 | 1 | 1 |
| Rural | 0.80 (0.69–0.93) | 0.64 (0.51–0.80) | 1.10 (0.88–1.37) | 0.97 (0.85–1.11) | 0.85 (0.71–1.01) | 1.24 (1.02–1.52) |
| Education | ||||||
| ≤12 | 1 | 1 | 1 | 1 | 1 | 1 |
| >12 | 0.83 (0.71–0.97) | 1.11 (0.88–1.39) | 0.56 (0.45–0.71) | 0.94 (0.82–1.07) | 1.08 (0.89–1.30) | 0.72 (0.59–0.88) |
| Income | ||||||
| Low | 1 | 1 | 1 | 1 | 1 | 1 |
| Over basic living expenses | 0.70 (0.56–0.88) | 1.01 (0.74–1.37) | 0.52 (3.37–0.73) | 0.85 (0.71–1.03) | 0.98 (0.76–1.25) | 0.74 (0.56–0.98) |
| Do not declare | 0.81 (0.67–0.97) | 1.07 (0.82–1.39) | 0.66 (0.50–0.86) | 0.78 (0.66–0.92) | 0.83 (0.67–1.04) | 0.74 (0.57–0.95) |
| BMI (kg/m2) * | ||||||
| Underweight | 1.46 (0.81–2.64) | 1.21 (0.34–4.28) | 1.33 (0.67–2.62) | 1.19 (0.69–2.05) | 0.64 (0.18–2.23) | 1.19 (0.64–2.21) |
| Normal | 1 | 1 | 1 | 1 | 1 | 1 |
| Overweight | 0.88 (0.73–1.06) | 0.89 (0.67–1.19) | 1.02 (0.78–1.33) | 0.88 (0.72–1.06) | 1.15 (0.91–1.44) | 1.08 (0.85–1.37) |
| Obese | 1.63 (1.34–1.97) | 1.32 (0.99–1.75) | 2.49 (1.88–3.30) | 1.37 (1.15–1.62) | 1.34 (1.06–1.71) | 1.74 (1.34–2.27) |
| Smoking status (ref. ** non-smoker) | ||||||
| Smoker | 0.80 (0.65–0.99) | 1.21 (0.91–1.59) | 0.67 (0.48–0.96) | 0.77 (0.64–0.93) | 0.92 (0.73–1.16) | 0.75 (0.55–1.03) |
| Alcohol consumption | ||||||
| Never drink | 1 | 1 | 1 | 1 | 1 | 1 |
| Drink occasionally | 0.60 (0.50–0.72) | 0.81 (0.59–1.09) | 0.62 (0.49–0.78) | 0.79 (0.67–0.93) | 1.01 (0.84–1.41) | 0.73 (0.59–0.91) |
| Drink frequently | 0.43 (0.35–0.52) | 0.65 (0.48–0.87) | 0.59 (0.41–0.84) | 0.58 (0.49–0.68) | 0.79 (0.62–1.02) | 0.72 (0.52–0.99) |
| Binge drinking | 0.81 (0.66–0.98) | 0.96 (0.75–1.23) | 1.27 (0.79–2.03) | 0.74 (0.63–0.88) | 0.78 (0.64–0.95) | 1.05 (0.68–1.61) |
| Comorbidities | ||||||
| HBP *** | 0.99 (0.83–1.19) | 1.01 (0.79–1.31) | 1.01 (0.79–1.32) | 0.93 (0.80–1.09) | 0.92 (0.75–1.13) | 0.97 (0.77–1.23) |
| T2DM **** | 1.10 (0.79–1.52) | 1.32 (0.86–2.01) | 1.07 (0.62–1.85) | 1.05 (0.78–1.40) | 1.18 (0.83–1.70) | 0.99 (0.60–1.66) |
| H-Chol ***** | 0.95 (0.79–1.14) | 1.05 (0.81–1.37) | 0.87 (0.67–1.14) | 0.84 (0.72–0.99) | 0.97 (0.78–1.20) | 0.73 (0.57–0.93) |
| Month | ||||||
| August | 1 | 1 | 1 | 1 | 1 | 1 |
| September | 5.10 (1.60–16.29) | 7.93 (0.91–69.15) | 4.05 (0.97–16.93) | 1.60 (0.87–2.93) | 2.61 (0.96–7.08) | 1.20 (0.52–2.79) |
| October | 7.91 (2.47–25.34) | 12.53 (1.43–109.80) | 6.05 (1.44–25.46) | 2.26 (1.22–4.17) | 4.55 (1.66–12.41) | 1.36 (0.58–3.19) |
| Males | Females | |||||
|---|---|---|---|---|---|---|
| B | SE | p-Value | B | SE | p-Value | |
| Intercept | 32.47 | 2.26 | <0.001 | 29.54 | 1.88 | <0.001 |
| Age (* ref. 25–34 years) | ||||||
| 35–44 years | 0.92 | 0.58 | 0.11 | - | - | - |
| 45–54 years | 1.38 | 0.57 | 0.02 | - | - | - |
| 55–64 years | 1.17 | 0.63 | 0.06 | - | - | - |
| Residence (ref. urban) | ||||||
| Rural | 1.29 | 0.40 | 0.001 | - | - | - |
| Smoking (ref. non-smokers) | ||||||
| Smokers | - | - | - | 1.02 | 0.58 | 0.08 |
| Alcohol (ref. never) | ||||||
| Occasionally | 0.56 | 0.56 | 0.32 | 1.19 | 0.44 | 0.006 |
| Frequently | 1.32 | 0.54 | 0.01 | 0.75 | 0.69 | 0.28 |
| Education (ref. ≤ 12 years) | ||||||
| High (>12 years) | - | - | - | 1.40 | 0.44 | 0.002 |
| Income (ref. < low) | ||||||
| High | - | - | - | 0.27 | 0.62 | 0.67 |
| NA | - | - | - | 0.91 | 0.50 | 0.07 |
| Ponderal status (ref. normal) | ||||||
| Underweight | 4.43 | 2.59 | 0.08 | −1.72 | 1.32 | 0.19 |
| Overweight | 0.08 | 0.51 | 0.87 | −0.58 | 0.49 | 0.24 |
| Obese | −1.32 | 0.54 | 0.01 | −2.62 | 0.50 | <0.001 |
| Month (ref. August) | ||||||
| September | −5.83 | 2.16 | 0.007 | −4.37 | 1.85 | 0.02 |
| October | −7.54 | 2.17 | <0.001 | −5.67 | 1.87 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brîndușe, L.A.; Eclemea, I.; Neculau, A.E.; Cucu, M.A. Vitamin D Status in the Adult Population of Romania—Results of the European Health Examination Survey. Nutrients 2024, 16, 867. https://doi.org/10.3390/nu16060867
Brîndușe LA, Eclemea I, Neculau AE, Cucu MA. Vitamin D Status in the Adult Population of Romania—Results of the European Health Examination Survey. Nutrients. 2024; 16(6):867. https://doi.org/10.3390/nu16060867
Chicago/Turabian StyleBrîndușe, Lăcrămioara Aurelia, Irina Eclemea, Andrea Elena Neculau, and Maria Alexandra Cucu. 2024. "Vitamin D Status in the Adult Population of Romania—Results of the European Health Examination Survey" Nutrients 16, no. 6: 867. https://doi.org/10.3390/nu16060867
APA StyleBrîndușe, L. A., Eclemea, I., Neculau, A. E., & Cucu, M. A. (2024). Vitamin D Status in the Adult Population of Romania—Results of the European Health Examination Survey. Nutrients, 16(6), 867. https://doi.org/10.3390/nu16060867