
Dietary Adequacy in Older Adult Nursing Home Residents of the Northern Iberian Peninsula

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Data Collection
2.3. Nutritional Intake
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Nutritional Intake
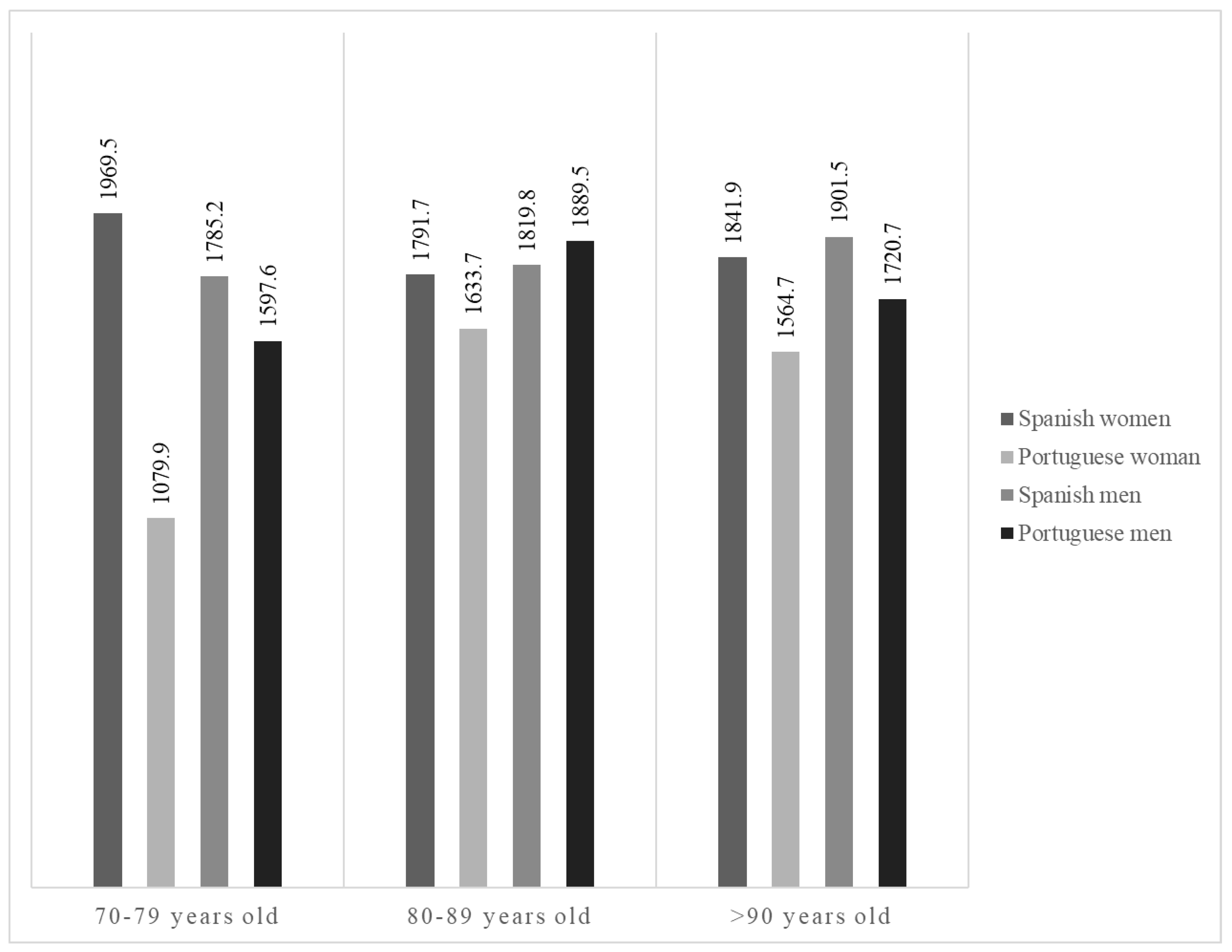
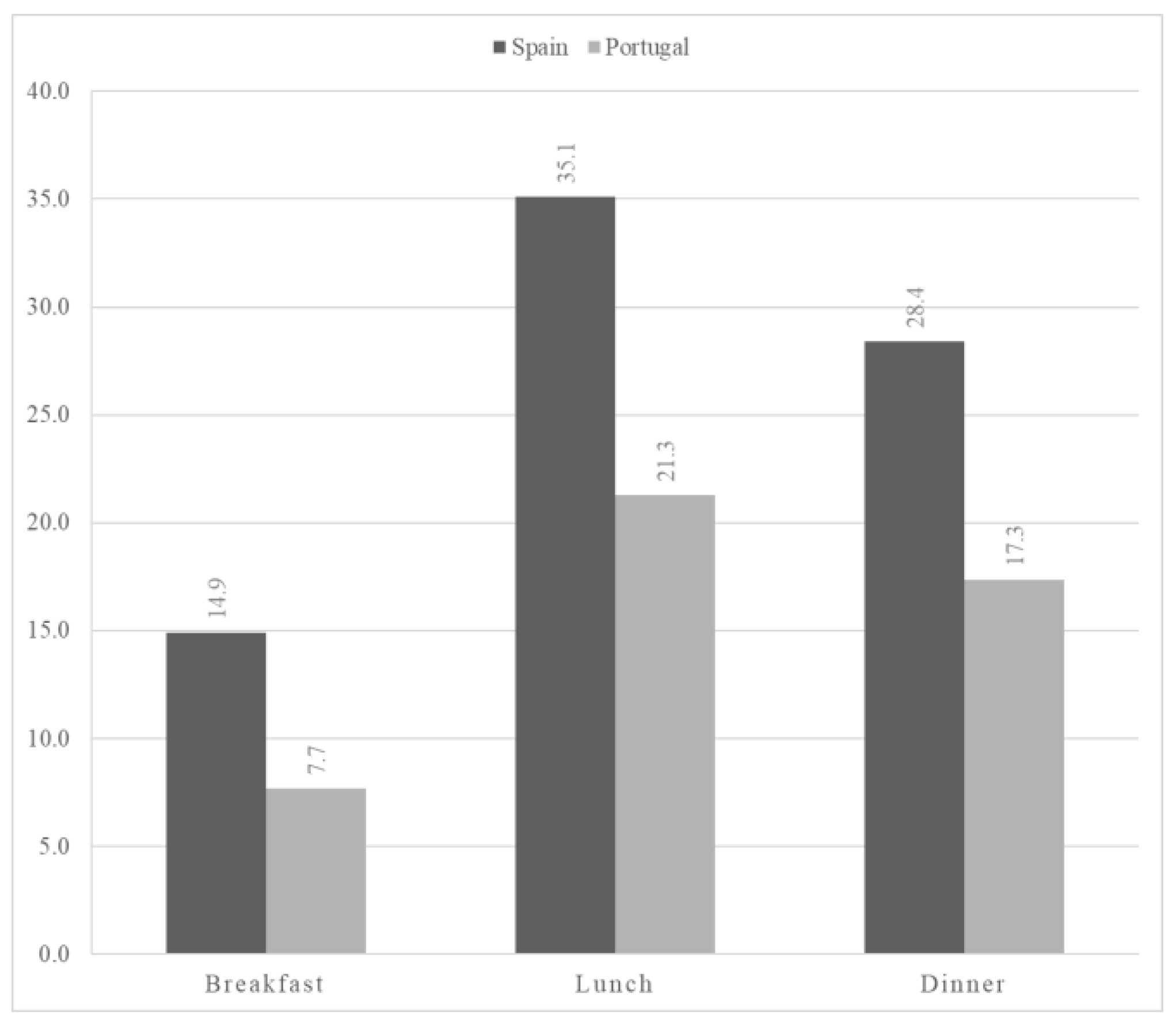
3.2.1. Energy Consumption
3.2.2. Macronutrient Distribution
3.2.3. Specific Nutrients
3.3. Nutritional Adequacy
4. Discussion
4.1. Energy Intake
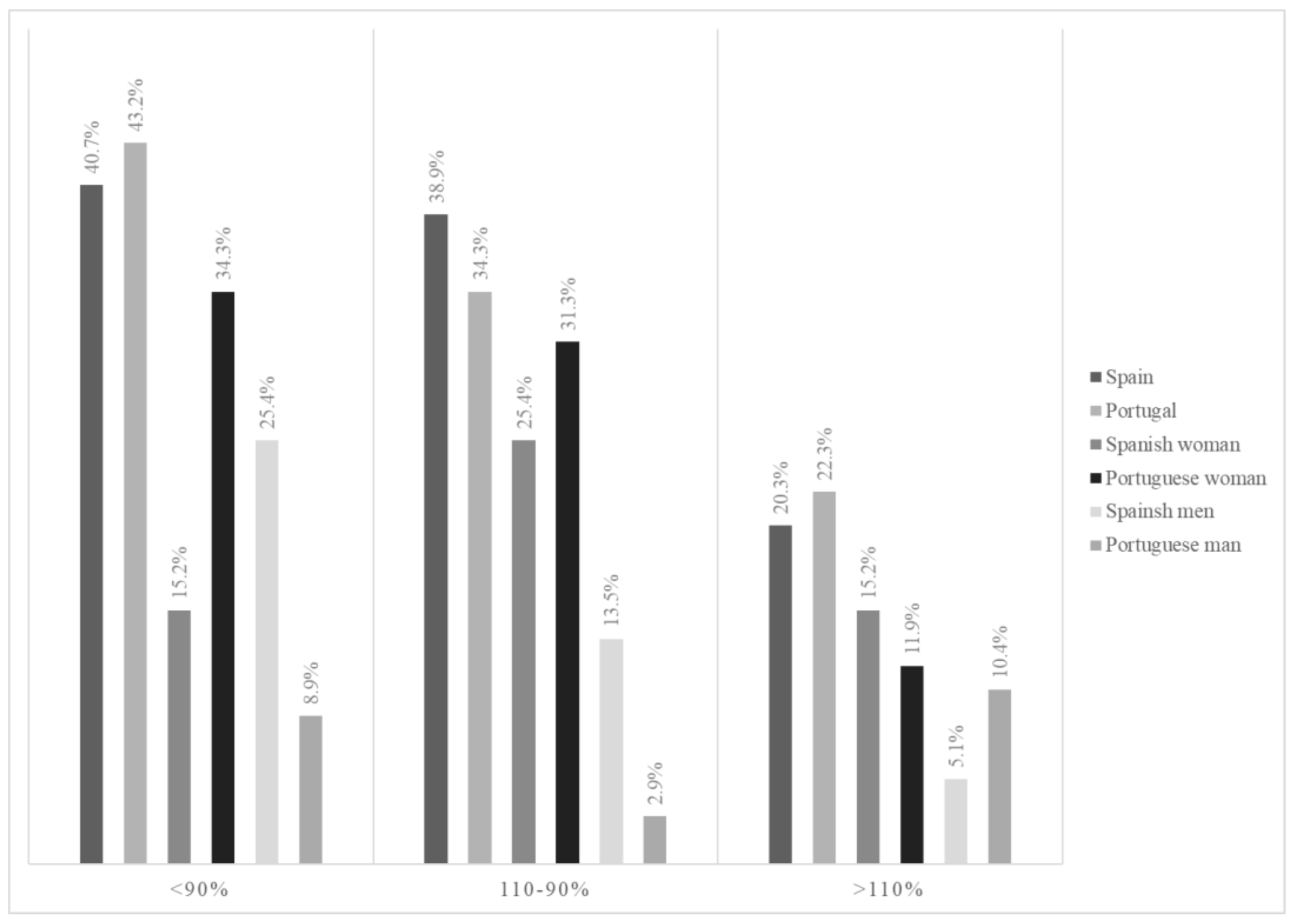
4.2. Individual Energy Requirements
4.3. Macronutrient Distribution
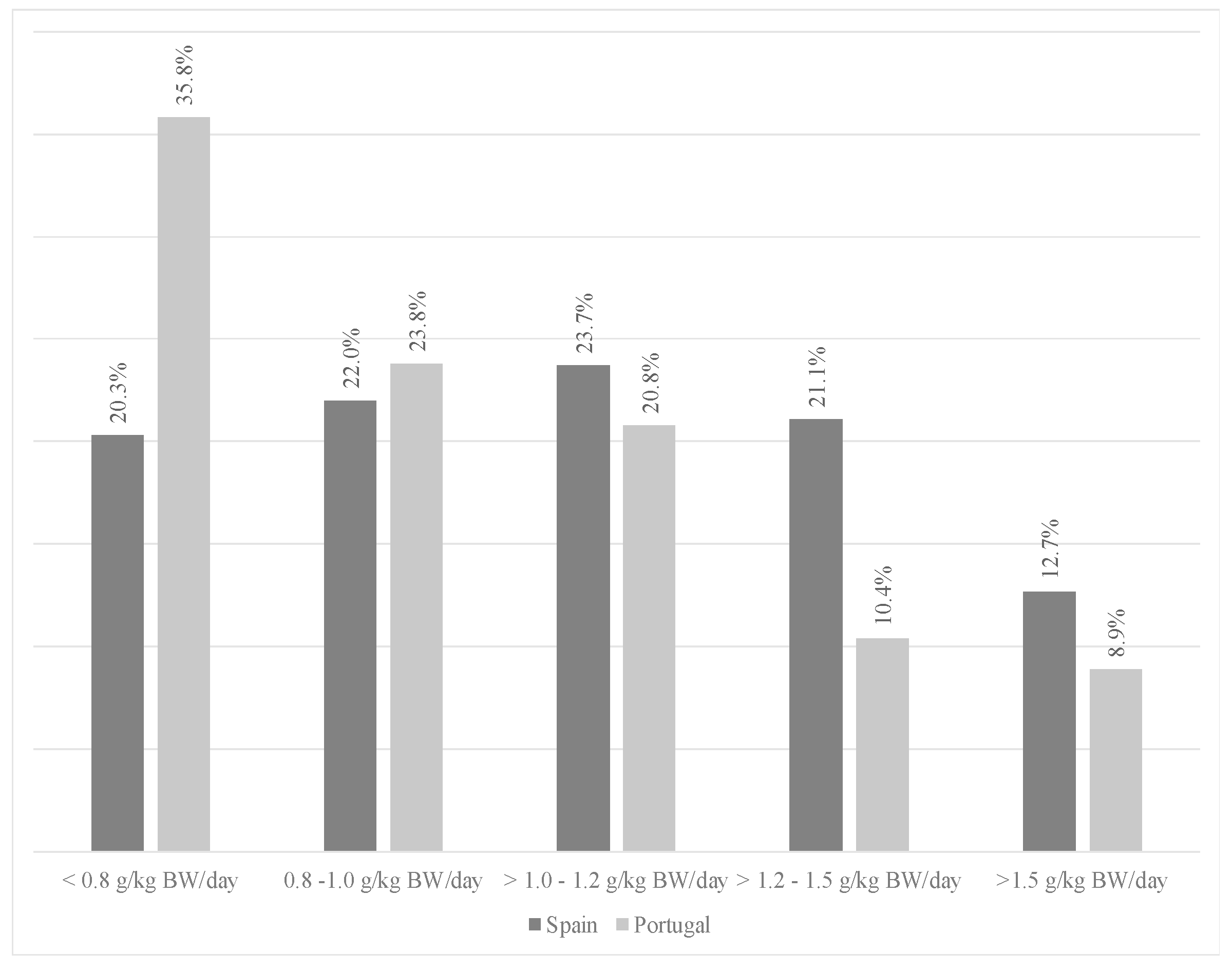
4.3.1. Protein Intake
4.3.2. Total Fat Intake
4.3.3. Carbohydrate Intake
4.3.4. Specific Nutrients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morais, C.; Oliveira, B.; Afonso, C.; Lumbers, M.; Raats, M.; de Almeida, M.D.V. Nutritional risk of European elderly. Eur. J. Clin. Nutr. 2013, 67, 1215–1219. [Google Scholar] [CrossRef]
- Pérez-Díaz, J.; Ramiro-Farinas, D.; Aceituno-Nieto, P.; Díaz, C.M.; Clara; López, B.; Ruiz-Santacruz, J.S.; Morales, I.F.; Belmonte, A.B.C.; de las Obras-Loscertales Sampériz, J.; et al. Un Perfil de las Personas Mayores en España, 2022. Indicadores Estadísticos Básicos. Consejo Superior de Investigaciones Científicas (CSIC). Centro de Ciencias Humanas y Sociales (CCHS). Envejecimiento en Red. 2022. Informes Envejecimiento en Red No. 29, 40p. Available online: http://envejecimiento.csic.es/documentos/documentos/enred-indicadoresbasicos2022.pdf (accessed on 12 October 2022).
- Oliveira, A.; Araújo, J.; Severo, M.; Correia, D.; Ramos, E.; Torres, D.; Lopes, C.; the IAN-AF Consortium. Prevalence of general and abdominal obesity in Portugal: Comprehensive results from the National Food, nutrition and physical activity survey 2015–2016. BMC Public Health 2018, 18, 614. [Google Scholar] [CrossRef]
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef]
- Rodríguez-Sánchez, B.; Sulo, S.; Carnicero, J.A.; Rueda, R.; Rodríguez-Mañas, L. Malnutrition Prevalence and Burden on Healthcare Resource Use Among Spanish Community-Living Older Adults: Results of a Longitudinal Analysis. Clin. Outcomes Res. 2020, 12, 355–367. [Google Scholar] [CrossRef]
- Vaca Bermejo, R.; Ancizu García, I.; Moya Galera, D.; de las Heras Rodríguez, M.; Pascual Torramadé, J. Prevalencia de desnutrición en personas mayores institucionalizadas en España: Un análisis multicéntrico nacional. Nutr. Hosp. 2015, 31, 1205–1216. [Google Scholar] [CrossRef]
- Dent, E.; Wright, O.L.R.; Woo, J.; Hoogendijk, E.O. Malnutrition in older adults. Lancet 2023, 401, 951–966. [Google Scholar] [CrossRef]
- Keller, H.H.; Carrier, N.; Duizer, L.; Lengyel, C.; Slaughter, S.E.; Steele, C.M. Making the Most of Mealtimes (M3): Grounding mealtime interventions with a conceptual model. J. Am. Med. Dir. Assoc. 2014, 20, 344–349. [Google Scholar] [CrossRef]
- Simmons, S.; Hollingsworth, E.; Long, E.; Liu, X.; Shotwell, M.; Keeler, E. Training nonnursing staff to assist with nutritional care delivery in nursing homes: A cost-effectiveness analysis. J. Am. Geriatr. Soc. 2016, 65, 313–322. [Google Scholar] [CrossRef]
- Beck, A.M.; Christensen, A.G.; Hansen, B.S.; Damsbo-Svendsen, S.; Møller, T.K. Multidisciplinary nutritional support for undernutrition in nursing home and home-care: A cluster randomized controlled trial. Nutrition 2016, 32, 199–205. [Google Scholar] [CrossRef]
- Chisholm, A.; Jensen, J.; Field, P. Eating environment in the aged-care residential setting in New Zealand: Promoters and barriers to achieving optimum nutrition. Observations of the foodservice, menu, and meals. Nutr. Diet. 2011, 68, 161–166. [Google Scholar] [CrossRef]
- Ocké, M.C. Evaluation of methodologies for assessing the overall diet: Dietary quality scores and dietary pattern analysis. Proc. Nutr. Soc. 2013, 72, 191–199. [Google Scholar] [CrossRef]
- Dietary Reference Values for Nutrients Summary Report. European Food Safety Authority. Available online: https://www.efsa.europa.eu/es/supporting/pub/e15121 (accessed on 11 May 2021).
- WHO. Human energy requirements: Report of a joint FAO/ WHO/UNU Expert Consultation. Food Nutr Bull. 2005, 26, 166. [Google Scholar]
- Pangman, V.C.; Sloan, J.; Guse, L. An Examination of Psychometric Properties of the Mini-Mental Status Examination and the Standardized Mini-Mental Status Examination: Implications for Clinical Practice. Appl. Nurs. Res. 2000, 13, 209–213. [Google Scholar] [CrossRef]
- Guzmán-Hernández, C.; Reinoza-Calderón, G.; Hernández-Hernández, R.A. Estimation of height from leg length measured with tape measure. Nutr. Hosp. 2005, 20, 358–363. [Google Scholar]
- Lipschitz, D.A. Screening for nutritional status in the elderly. Prim. Care 1994, 21, 55–67. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 19th ed.; Pirámide: Madrid, Spain, 2018. [Google Scholar]
- Tabela da Composiçao de Alimentos. Plataforma Portuguesa de Informação Alimentar. 2021. Available online: http://portfir.insa.pt/# (accessed on 10 October 2022).
- Mila, R.; Abellana, R.; Padro, L.; Farran, A. Assessment of food consumption, energy and protein intake in the meals offered in four Spanish nursing homes. Nutr. Hosp. 2012, 27, 914–921. [Google Scholar]
- Buckinx, F.; Allepaerts, S.; Paquot, N.; Reginster, J.Y.; de Cock, C.; Petermans, J.; Bruyère, O. Energy and Nutrient Content of Food Served and Consumed by Nursing Home Residents. J. Nutr. Health Aging 2017, 21, 727–732. [Google Scholar] [CrossRef]
- López-Contreras, M.J.; Torralba, C.; Zamora, S.; Pérez-Llamas, F. Nutrition and prevalence of undernutrition assessed by different diagnostic criteria in nursing homes for elderly people. J. Hum. Nutr. Diet. 2012, 25, 239–246. [Google Scholar] [CrossRef]
- Suominem, M.; Laine, A.; Routasalo, P.; Pitkala, K.H.; Rasanen, L. Nutrient content of served food, nutrient intake, and nutritional status of residents with dementia in a Finnish nursing home. J. Nutr. Health Aging 2004, 8, 234–238. [Google Scholar]
- Calvo, M. Valoración nutricional de la oferta y de la ingesta dietética en una residencia geriátrica. Rev. Española Nutr. Comunitaria 2013, 19, 20–28. Available online: https://www.renc.es/imagenes/auxiliar/files/RENC%202013_1-art3%281%29.pdf (accessed on 15 October 2022).
- Rodríguez-Rejón, A.I.; Ruiz-López, M.D.; Malafarina, V.; Zuñiga, A.; Artacho, R. Menus offered in long-term care homes: Quality of meal service and nutritional analysis. Nutr. Hosp. 2017, 34, 584–592. [Google Scholar] [CrossRef]
- Mila, R.; Abellana, R.; Padro, L.; Basulto, J.; Farran, A. High consumption foods and their influence on energy and protein intake in institutionalized older adults. J. Nutr. Health Aging 2011, 16, 115–122. [Google Scholar] [CrossRef]
- Bogacka, A.; Heberlej, A.; Usarek, A.; Okoniewska, J. Diet and nutritional status of elderly people depending on their place of residence. Rocz. Panstw. Zakl. Hig. 2019, 70, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Lam, I.T.; Keller, H.H.; Duizer, L.; Stark, K. Micronutrients on the Menu: Enhancing the Quality of Food in Long-term Care for Regular, Nontherapeutic Menus. Can. J. Diet. Pract. Res. 2015, 76, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Ongan, D.; Rakıcıoğlu, N. Nutritional status and dietary intake of institutionalized elderly in Turkey: A cross-sectional, multi-center, country representative study. Arch. Gerontol. Geriatr. 2015, 61, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Aghdassi, E.; McArthur, M.; Liu, B.; McGeer, A.; Simor, A.; Allard, J.P. Dietary intake of elderly living in Toronto long-term care facilities: Comparison to the dietary reference intake. Rejuvenation Res. 2007, 10, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Paquot, N.; Fadeur, M. Assessment of the energy expenditure of Belgian nursing home residents using indirect calorimetry. Nutrition 2019, 57, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Kalinowski, S.; Wulff, I.; Kölzsch, M.; Kopke, K.; Kreutz, R.; Dräger, D. Physical activity in nursing homes—Barriers and facilitators: A cross-sectional study. J. Aging Phys. Act. 2012, 20, 421–441. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Den Ouden, M.; Bleijlevens, M.H.C.; Meijers, J.M.M.; Zwakhalen, S.M.G.; Braun, S.M.; Tan, F.E.S.; Hamers, J.P.H. Daily (In)Activities of Nursing Home Residents in Their Wards: An Observation Study. J. Am. Med. Dir. Assoc. 2015, 16, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards, and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar]
- Gaillard, C.; Alix, E.; Sallé, A.; Berrut, G.; Ritz, P. Energy requirements in frail elderly people: A review of the literature. Clin. Nutr. 2007, 26, 16–24. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rejón, A.I.; Ruiz-López, M.D.; Artacho, R. Dietary Intake and Associated Factors in Long-Term Care Homes in Southeast Spain. Nutrients 2019, 11, 266. [Google Scholar] [CrossRef] [PubMed]
- Ocagli, H.; Lanera, C.; Azzolina, D.; Piras, G.; Soltanmohammadi, R.; Gallipoli, S.; Gafare, C.E.; Cavion, M.; Roccon, D.; Vedovelli, L.; et al. Resting Energy Expenditure in the Elderly: Systematic Review and Comparison of Equations in an Experimental Population. Nutrients 2021, 13, 458. [Google Scholar] [CrossRef] [PubMed]
- Zaragoza-Martí, A.; Ruiz-Robledillo, N.; Sánchez-SanSegundo, M.; Albaladejo-Blázquez, N.; Hurtado-Sánchez, J.A.; Ferrer-Cascales, R. Eating Habits in Older Adults: Compliance with the Recommended Daily Intakes and Its Relationship with Sociodemographic Characteristics, Clinical Conditions, and Lifestyles. Nutrients 2020, 12, 446. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Loprinzi, P.D.; Murphy, C.H.; Phillips, S.M. Per meal dose and frequency of protein consumption is associated with lean mass and muscle performance. Clin. Nutr. 2016, 35, 1506–1511. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.R.; Churchward-Venne, T.A.; Witard, O.; Breen, L.; Burd, N.A.; Tipton, K.D.; Phillips, S.M. Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 57–62. [Google Scholar] [CrossRef]
- Franzke, B.; Schober-Halper, B.; Hofmann, M.; Oesen, S.; Tosevska, A.; Strasser, E.M.; Marculescu, R.; Wessner, B.; Wagner, K.H. Fat Soluble Vitamins in Institutionalized Elderly and the Effect of Exercise, Nutrition and Cognitive Training on Their Status. The Vienna Active Aging Study (VAAS): A Randomized Controlled Trial. Nutrients 2019, 11, 1333. [Google Scholar] [CrossRef]
- EFSA. Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 2010, 8, 1461. [Google Scholar] [CrossRef]
- Babio, N.; Becerra-Tomás, N.; Martínez-González, M.A. Consumption of Yogurt, Low-Fat Milk, and Other Low-Fat Dairy Products Is Associated with Lower Risk of Metabolic Syndrome Incidence in an Elderly Mediterranean Population. J. Nutr. 2015, 145, 2308–2316. [Google Scholar] [CrossRef] [PubMed]
- Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [CrossRef]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef]
- Turck, D.; Bohn, T.; Castenmiller, J. Tolerable upper intake level for dietary sugars. EFSA J. 2022, 20, e07074. [Google Scholar] [CrossRef] [PubMed]
- Goletzke, J.; Buyken, A.E.; Gopinath, B.; Rochtchina, E.; Barclay, A.W.; Cheng, G.; Brand-Miller, J.C.; Mitchell, P. Carbohydrate quality is not associated with liver enzyme activity and plasma TAG and HDL concentrations over 5 years in an older population. Br. J. Nutr. 2013, 110, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Varela-Moreiras, G. Adequacy of the dietary intake of total and added sugars in the Spanish diet to the recommendations: ANIBES study. Nutr. Hosp. 2017, 34 (Suppl. 4), 45–52. [Google Scholar] [CrossRef]
- EFSA Panel on Nutrition; Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; et al. Dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar] [CrossRef]
- Overwyk, K.J.; Quader, Z.S.; Maalouf, J.; Bates, M.; Webster, J.; George, M.G.; Merritt, R.K.; Cogswell, M.E. Dietary Sodium Intake and Health Indicators: A Systematic Review of Published Literature between January 2015 and December 2019. Adv. Nutr. 2020, 11, 1174–1200. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (n = 186) * | Spain | Portugal |
|---|---|---|
| Age (years), median | 85.0 | 85.0 |
| Percentile 25 | 82.0 | 80.0 |
| 75 | 88.0 | 91.0 |
| Male, n (%) | 52 (44.1) | 16 (23.5) |
| Female, n (%) | 66 (55.9) | 52 (76.5) |
| Weight (kg), median | 75.0 | 66.0 |
| Percentile 25 | 65.9 | 57.0 |
| 75 | 82.0 | 77.7 |
| Male median | 76.2 | 77.2 |
| Female median | 72.0 | 64.0 |
| BMI (kg/m2), median | 28.6 | 27.3 |
| Percentile 25 | 24.5 | 24.3 |
| 75 | 31.7 | 30.6 |
| Underweight (BMI < 22), n (%) | 8 (6.7) | 7 (10.2) |
| Normal (BMI 22–27), n (%) | 36 (30.5) | 25 (36.7) |
| Overweight (BMI > 27), n (%) | 74 (62.7) | 36 (52.9) |
| Spain | Portugal | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Percentage of Residents within Adequacy | Percentage of Residents within Adequacy | ||||||||||||
| Nutrient | RDI | Mean | SD | Median | IQR | % | 95% CI | Mean | SD | Median | IQR | % | 95% CI |
| Energy (kcal) | 1842 * | 1575–2056 | 1644 | 1367–1890 | |||||||||
| Carbohydrates (% of energy) | 45–60 a | 56.0 | 0.71 | 56.0 *** | 50.7–62.0 | 66.9 | 58.3–75.5 | 59.3 | 0.6 | 60.5 | 56.8–63.1 | 45.5 | 33.4–57.7 |
| Carbohydrates (g) | >100 | 258.1 | 6.1 | 250.7 | 209.5–300.2 | 243.1 | 7.2 | 239.6 | 199.6–274.6 | ||||
| Total sugar (g) | <90 | 66.0 | 2.1 | 59.6 | 50.6–75.6 | 88.1 | 82.2–94.0 | 72.3 | 2.4 | 71.1 | 56.4–85.3 | 86.7 | 78.5–95.0 |
| Total fat (% of energy) | 20–35 a | 24.1 | 0.7 | 24.0 * | 17.0–31.0 | 54.2 | 45.2–63.3 | 20.7 | 0.5 | 20.4 | 17.8–23.3 | 53.8 | 46.5–61.0 |
| Total fat (g) | 48.7 | 1.7 | 45.0 *** | 34.6–62.6 | 38.3 | 1.5 | 39.3 | 29.0–46.2 | |||||
| SFA (% of energy) | ALAP b | 6.9 | 0.2 | 7.2 | 4.8–8.6 | 7.49 | 0.2 | 7.3 | 6.3–8.2 | ||||
| Protein (% of energy) | 10–15 | 17.8 | 0.2 | 18.0 *** | 16.0–20.0 | 17.8 | 10.7–24.8 | 14.8 | 0.3 | 14.2 | 12.8–16.2 | 54.4 | 42.2–66.5 |
| Protein (g) | 82.2 | 2.3 | 77.3 *** | 67.2–92.9 | 61.0 | 2.1 | 62.5 | 48.3–73.8 | |||||
| Salt (g) | 5 c | 5.8 *** | 4.6–6.7 | 33.0 | 24.4–41.6 | 4.3 | 3.8–5.3 | 67.7 | 56.2–79.0 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pidrafita-Páez, N.; Silveira, J.; Pinto, E.; Franco, L.; Romero-Rodríguez, M.Á.; Vázquez-Odériz, M.L.; NUTRIAGE Study Group. Dietary Adequacy in Older Adult Nursing Home Residents of the Northern Iberian Peninsula. Nutrients 2024, 16, 798. https://doi.org/10.3390/nu16060798
Pidrafita-Páez N, Silveira J, Pinto E, Franco L, Romero-Rodríguez MÁ, Vázquez-Odériz ML, NUTRIAGE Study Group. Dietary Adequacy in Older Adult Nursing Home Residents of the Northern Iberian Peninsula. Nutrients. 2024; 16(6):798. https://doi.org/10.3390/nu16060798
Chicago/Turabian StylePidrafita-Páez, Nicolás, Joana Silveira, Elisabete Pinto, Luis Franco, Mª Ángeles Romero-Rodríguez, Mª Lourdes Vázquez-Odériz, and NUTRIAGE Study Group. 2024. "Dietary Adequacy in Older Adult Nursing Home Residents of the Northern Iberian Peninsula" Nutrients 16, no. 6: 798. https://doi.org/10.3390/nu16060798
APA StylePidrafita-Páez, N., Silveira, J., Pinto, E., Franco, L., Romero-Rodríguez, M. Á., Vázquez-Odériz, M. L., & NUTRIAGE Study Group. (2024). Dietary Adequacy in Older Adult Nursing Home Residents of the Northern Iberian Peninsula. Nutrients, 16(6), 798. https://doi.org/10.3390/nu16060798