
Empowering Young Women: A Qualitative Co-Design Study of a Social Media Health Promotion Programme




Abstract
1. Introduction
2. Materials and Methods
- Which social media components might work best?
- How should the program be delivered?
- What nutrition behaviours should the program aim to change?
- Who should deliver the program?
2.1. Participant Recruitment
2.2. Participatory Design
2.3. Knowledge Translation
Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Phase 1: Expert Focus Groups and Interviews
“The company spends a lot of time trying to create a community—so having a lot of back and forth, which means we often put question boxes up saying “What do you want to see next? What colours? What styles?”—a digital marketer.
“You need to know what features of the social media applications they use most frequently.”—a NZ-registered dietitian;
“Understanding what they’re using social media for. You know, whether they are using social media for health information.”—a NZ-registered dietitian
“Seeing what sort of health content they are engaging with. And asking them, is there something else that would motivate you to engage with it? And what are any barriers to using social media? I would investigate what are the barriers to using social media for health-related information. Because it might be more of an access issue.”—a NZ-registered dietitian;
“What are the problems? What do they want to know more about? What are the pain points around their well-being? What do they feel they need to work on to achieve better health, and how important is that to them?”—a NZ-registered dietitian.
3.3. Phase 2: End-User Workshops
3.3.1. Session One
“Doing things that make you feel good, not focusing on what makes others feel good, or what you think others would like.”—young adult 4;
“Connecting with yourself to connect with others. I think that’s really important.”—young adult 5;
“The words that I would use to describe health would be variety and unlimited.”—young adult 2.
“I think an issue at the moment is that there’s too much emphasis on perfection when it comes to health.”—young woman 3;
“I just find understanding nutrition like really difficult, like I just don’t get it”—young woman 8;
“Health is not all one size fits all, and it’s really, really difficult to navigate life constantly comparing yourself and your own health to what other people eat in a day or how much other people exercise, or how other people view themselves in their bodies.”—young woman 12.
3.3.2. Session Two
“It is quite refreshing to see videos with quite normal ingredients. Quite often, when I get these videos on my social media, it looks amazing but it’s really expensive ingredients and takes a lot of time.”—young woman 11;
“I feel like with health… I find that there is a lot of different information, even if it’s with a credible source?”—young woman 13.
3.3.3. Session Three
3.3.4. Social Media Features and Strategy
“We weren’t too sure about the contacting participants… not going to lie… but we thought maybe, I don’t know, we thought don’t DM people because they will think it’s a scam, so you might not get answers”—young woman 1.
3.3.5. Information Delivery
3.3.6. Other Insights
“That is a real barrier—understanding what the standards are that are being pushed on us on social media vs. who am I?”—young adult 8;
“I feel like at some point it’s kind of like trying to confirm if I was correct? Because, you know, I might have some values, I might have some knowledge about this particular topic, but it’s just me and, you know, it will be really nice if I can look out to a platform that is so easily accessible, and there are people up there like, regardless of them being right or wrong or not, but you know we’re all on the same topic.”—young woman 2;
“I found that a massive barrier is that I don’t invest as much ‘in person’ time with my friends as much as with social media.”—young woman 8.
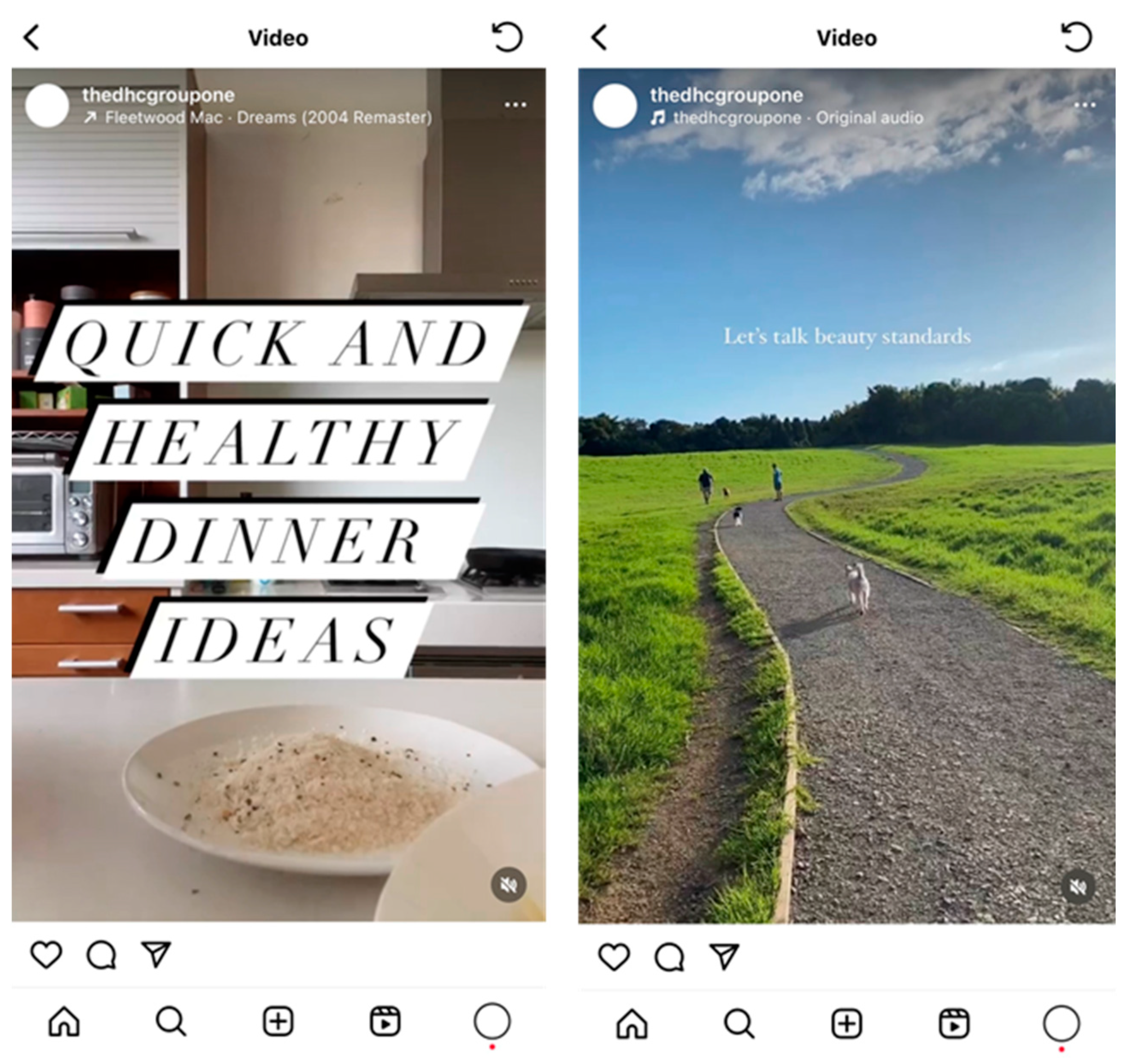
3.4. Phase 3: Content Co-Creation
The Daily Health Coach Website
3.5. End-User Feedback
“Thanks for including me in your study, I really enjoyed being a part of it”.
“It was a really great experience to share my ideas around health and food with a small group. I definitely learnt a lot about other’s perceptions and how I could incorporate little habits to make my mealtimes healthier”.
“Thanks for the opportunity! I really enjoyed getting involved”.
4. Discussion
4.1. Principal Findings
4.2. Comparison to Similar Research
4.3. Relevance and Contribution of Research
4.4. Strengths and Limitations
5. Conclusions
Future Applications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Web Index (GWI). Social Media behind the Scenes. 2023. Available online: https://www.gwi.com/webinars/social-media-behind-the-screens (accessed on 1 November 2023).
- Sharps, M.A.; Hetherington, M.M.; Blundell-Birtill, P.; Rolls, B.J.; Evans, C.E. The effectiveness of a social media intervention for reducing portion sizes in young adults and adolescents. Digit. Health 2019, 5, 878076. [Google Scholar] [CrossRef] [PubMed]
- Malloy, J.; Partridge, S.R.; Kemper, J.A.; Braakhuis, A.; Roy, R. Co-design of digital health interventions with young people: A scoping review. Digit. Health 2023, 9, 219117. [Google Scholar] [CrossRef] [PubMed]
- Pressgrove, G.; McKeever, B.; Jang, M. What is Contagious? Exploring why content goes viral on Twitter: A case study of the ALS Ice Bucket Challenge. Int. J. Nonprofit Volunt. Sect. Mark. 2017, 23, e1586. [Google Scholar] [CrossRef]
- Pedrana, A.; Hellard, M.; Gold, J.; Ata, N.; Chang, S.; Howard, S.; Asselin, J.; Ilic, O.; Batrouney, C.; Stoove, M. Queer as F**k: Reaching and engaging gay men in sexual health promotion through social networking sites. J. Med. Internet Res. 2013, 15, e25. [Google Scholar] [CrossRef] [PubMed]
- Ministy of Health New Zealand. Annual Data Explorer 2021/2022: New Zealand Health Survey [Data File]. 2022. Available online: https://www.health.govt.nz/publication/annual-update-key-results-2021-22-new-zealand-health-survey (accessed on 1 December 2023).
- Ministry of Health New Zealand. Eating and Activity Guidelines for New Zealand Adults: Updated 2020; Ministry of Health: Wellington, New Zealand, 2020. Available online: https://www.health.govt.nz/publication/eating-and-activity-guidelines-new-zealand-adults (accessed on 1 December 2023).
- Lawrence, E.; Mollborn, S.; Goode, J.; Pampel, F. Health Lifestyles and the Transition to Adulthood. Socius Sociol. Res. Dyn. World 2020, 6, 942070. [Google Scholar] [CrossRef]
- Denniss, E.; Lindberg, R.; McNaughton, S.A. Quality and accuracy of online nutrition-related information: A systematic review of content analysis studies. Public Health Nutr. 2023, 26, 1345–1357. [Google Scholar] [CrossRef] [PubMed]
- Aparicio-Martinez, P.; Perea-Moreno, A.-J.; Martinez-Jimenez, M.P.; Redel-Macías, M.D.; Pagliari, C.; Vaquero-Abellan, M. Social Media, Thin-Ideal, Body Dissatisfaction and Disordered Eating Attitudes: An Exploratory Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4177. [Google Scholar] [CrossRef]
- Ridout, B.; Campbell, A. The Use of Social Networking Sites in Mental Health Interventions for Young People: Systematic Review. J. Med. Internet Res. 2018, 20, e12244. [Google Scholar] [CrossRef]
- Kruzan, K.P.; Williams, K.D.; Meyerhoff, J.; Yoo, D.W.; O’Dwyer, L.C.; De Choudhury, M.; Mohr, D.C. Social media-based interventions for adolescent and young adult mental health: A scoping review. Internet Interv. 2022, 30, 100578. [Google Scholar] [CrossRef]
- Chau, M.M.; Burgermaster, M.; Mamykina, L. The use of social media in nutrition interventions for adolescents and young adults—A systematic review. Int. J. Med. Inform. 2018, 120, 77–91. [Google Scholar] [CrossRef]
- Rice, S.M.; Goodall, J.; Hetrick, S.E.; Parker, A.G.; Gilbertson, T.; Amminger, G.P.; Davey, C.G.; McGorry, P.D.; Gleeson, J.; Alvarez-Jimenez, M. Online and Social Networking Interventions for the Treatment of Depression in Young People: A Systematic Review. J. Med. Internet Res. 2014, 16, e206. [Google Scholar] [CrossRef] [PubMed]
- Goodyear, V.A.; Wood, G.; Skinner, B.; Thompson, J.L. The effect of social media interventions on physical activity and dietary behaviours in young people and adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 72. [Google Scholar] [PubMed]
- Malloy, J.A.; Partridge, S.R.; Kemper, J.A.; Braakhuis, A.; Roy, R. Co-Design of Digital Health Interventions for Young Adults: Protocol for a Scoping Review. JMIR Res. Protoc. 2022, 11, e38635. [Google Scholar] [CrossRef] [PubMed]
- Vargas, C.; Whelan, J.; Brimblecombe, J.; Allender, S. Co-creation, co-design, co-production for public health—A perspective on definitions and distinctions. Pub. Health Res. Pract. 2022, 32, 2. [Google Scholar] [CrossRef] [PubMed]
- Raeside, R.; Todd, A.; Wardak, S.; Gardner, L.; Champion, K.E.; Kang, M.; Mihrshahi, S.; Steinbeck, K.; Redfern, J.; Partridge, S.R.; et al. Striking the right balance: Co-designing the Health4Me healthy lifestyle digital health intervention with adolescents. Res. Involv. Engagem. 2023, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mandoh, M.; Redfern, J.; Mihrshahi, S.; Cheng, H.L.; Phongsavan, P.; Partridge, S.R. Shifting from Tokenism to Meaningful Adolescent Participation in Research for Obesity Prevention: A Systematic Scoping Review. Front. Public Health 2021, 9, 789535. [Google Scholar] [CrossRef]
- Roy, R.; Jessica, M. Evolving Role of Social Media in Health Promotion. In Health Promotion; Bishan Swarup, G., Ed.; Chapter 6; IntechOpen: Rijeka, Croatia, 2023. [Google Scholar]
- Korpershoek, Y.J.; Hermsen, S.; Schoonhoven, L.; Schuurmans, M.J.; Trappenburg, J.C. User-centered design of a mobile health intervention to enhance exacerbation-related self-management in patients with chronic obstructive pulmonary disease (Copilot): Mixed methods study. J. Med. Internet Res. 2020, 22, e15449. [Google Scholar] [CrossRef]
- Abroms, L.C.; Westmaas, J.L.; Bontemps-Jones, J.; Ramani, R.; Mellerson, J. A content analysis of popular smartphone apps for smoking cessation. Am. J. Prev. Med. 2013, 45, 732–736. [Google Scholar] [CrossRef]
- Cheng, V.W.S.; Davenport, T.A.; Johnson, D.; Vella, K.; Mitchell, J.; Hickie, I.B. An app that incorporates gamification, mini-games, and social connection to improve men’s mental health and well-being (MindMax): Participatory design process. JMIR Ment. Health 2018, 5, e11068. [Google Scholar] [CrossRef]
- Man, M.; Abrams, T.; McLeod, R. Implementing and Evaluating Co-Design: A Step-by-Step Toolkit. 2019. Available online: https://www.thinknpc.org/wp-content/uploads/2019/07/Co-design-guidance-July-2019.pdf (accessed on 1 October 2021).
- Health Cascade Network. Training and Tools. 2024. Available online: https://healthcascade.eu/ (accessed on 1 November 2023).
- Hagen, P.; Collin, P.; Metcalf, A.; Nicholas, M.; Rahilly, K.; Swainston, N. Participatory Design of Evidence-Based Online Youth Mental Health Promotion, Intervention and Treatment; Young and Well Cooperative Research Centre: Melbourne, Australia, 2012; Available online: https://www.westernsydney.edu.au/__data/assets/pdf_file/0005/476330/Young_and_Well_CRC_IM_PD_Guide.pdf (accessed on 1 October 2021).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for inter-views and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Malloy, J.A.; Roy, R.; Kemper, J.A.; Partridge, S.R. Co-designing a social media health promotion program for young women: A study protocol. Int. J. Qual. Method 2024, 23, 1–10. [Google Scholar] [CrossRef]
- Zoom Video Communications, Inc. Version: 514610 (25689). Software Program. Available online: https://zoom.us/ (accessed on 25 June 2023).
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Krueger, R.; Casey, M. Focus Groups: A Practical Guide for Applied Research; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2014; Volume 5. [Google Scholar]
- Lumivero. NVivo Qualitative Data Analysis Software, version 12; Lumivero Ltd.: Denver, CO, USA, 2018. [Google Scholar]
- Gray, S.H. Social Aspects of Body Image: Perception of normalcy of weight and affect of college undergraduates. Percept. Mot. Ski. 1977, 45, 1035–1040. [Google Scholar] [CrossRef]
- Anglé, S.; Engblom, J.; Eriksson, T.; Kautiainen, S.; Saha, M.-T.; Lindfors, P.; Lehtinen, M.; Rimpelä, A. Three factor eating questionnaire-R18 as a measure of cognitive restraint, uncontrolled eating and emotional eating in a sample of young Finnish females. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 41. [Google Scholar] [CrossRef]
- West, R.; Michie, S. A Brief Introduction to the COM-B Model of Behaviour and the PRIME Theory of Motivation. Qeios. 2020. Available online: https://www.qeios.com/read/WW04E6 (accessed on 1 December 2023).
- Ministry of Health New Zealand. Māori Health Models. 2024. Available online: https://www.health.govt.nz/our-work/populations/maori-health/maori-health-models (accessed on 1 December 2023).
- Denniss, E.; Lindberg, R.; McNaughton, S.A. Development of Principles for Health-Related Information on Social Media: Delphi Study. J. Med. Internet Res. 2022, 24, e37337. [Google Scholar] [CrossRef] [PubMed]
- Wix. Wix Website Editor. 2024. Available online: https://www.wix.com/ (accessed on 1 August 2022).
- Tanner, A.E.; Song, E.Y.; Mann-Jackson, L.; Alonzo, J.; Schafer, K.; Ware, S.; Garcia, J.M.; Hall, E.A.; Bell, J.C.; Van Dam, C.N.; et al. Preliminary Impact of the weCare Social Media Intervention to Support Health for Young Men Who Have Sex with Men and Transgender Women with HIV. AIDS Patient Care STDs 2018, 32, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Gan, D.Z.Q.; McGillivray, L.; Larsen, M.E.; Bloomfield, T.; Torok, M. Promoting Engagement with Smartphone Apps for Suicidal Ideation in Young People: Development of an Adjunctive Strategy Using a Lived Experience Participatory Design Approach. JMIR Form. Res. 2023, 7, e45234. [Google Scholar] [CrossRef] [PubMed]
- Greer, S.; Ramo, D.; Chang, Y.-J.; Fu, M.; Moskowitz, J.; Haritatos, J. Use of the chatbot “vivibot” to deliver positive psychology skills and promote well-being among young people after cancer treatment: Randomized controlled feasibility trial. JMIR mHealth uHealth 2019, 7, e15018. [Google Scholar] [CrossRef] [PubMed]
- Pachankis, J.E.; Lelutiu-Weinberger, C.; Golub, S.A.; Parsons, J.T. Developing an online health intervention for young gay and bisexual men. AIDS Behav. 2013, 17, 2986–2998. [Google Scholar] [CrossRef] [PubMed]
- Ito-Jaeger, S.; Perez Vallejos, E.; Curran, T.; Crawford, P. What’s up with Everyone? A qualitative study on young people’s perceptions of cocreated online animations to promote mental health literacy. Health Expect. 2022, 25, 1633–1642. [Google Scholar] [CrossRef] [PubMed]
- Duara, R.; Chowdhury, D.; Dey, R.; Goswami, S.; Madill, A. Using cocreated visually informed community mental health education in low- and middle-income countries: A case study of youth substance misuse in Assam, India. Health Expect. 2022, 25, 1930–1944. [Google Scholar] [CrossRef]
- Lederman, R.; Wadley, G.; Gleeson, J.; Bendall, S.; Álvarez-Jiménez, M. Moderated online social therapy: Designing and evaluating technology for mental health. ACM Trans. Comput.-Hum. Interact. 2014, 21, 1–26. [Google Scholar] [CrossRef]
- Singh, D.R.; Sah, R.K.; Simkhada, B.; Darwin, Z. Potentials and challenges of using co-design in health services research in low- and middle-income countries. Glob. Health Res. Policy 2023, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mandoh, M.; Raeside, R.; Todd, A.; Redfern, J.; Mihrshahi, S.; Cheng, H.L.; Phongsavan, P.; Partridge, S.R. Evaluating the effect of a 12-month youth advisory group on adolescent’s leadership skills and perceptions related to chronic disease prevention research: A mixed-methods study. BMC Public Health 2023, 23, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Slattery, P.; Saeri, A.K.; Bragge, P. Research co-design in health: A rapid overview of reviews. Health Res. Policy Syst. 2020, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Silvola, S.; Restelli, U.; Bonfanti, M.; Croce, D. Co-Design as Enabling Factor for Patient-Centred Healthcare: A Bibliometric Literature Review. Clin. Outcomes Res. 2023, 15, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Gurney, J.; Stanley, J.; Sarfati, D. The inequity of morbidity: Disparities in the prevalence of morbidity between ethnic groups in New Zealand. J. Comorbidity 2020, 10, 971168. [Google Scholar] [CrossRef]
- Wispelwey, B.; Tanous, O.; Asi, Y.; Hammoudeh, W.; Mills, D. Because its power remains naturalized: Introducing the settler colonial determinants of health. Front. Public Health 2023, 11, 1137428. [Google Scholar] [CrossRef]
- Berghan, G.; Came, H.; Coupe, N.; Doole, C.; Fay, J.; McCreaner, T.; Simpson, T. Te Tiriti o Waitangi-Based Practice in Health Promotion; STIR, Stop Institutional Racism: Auckland, New Zealand, 2017; ISBN 978-0-473-41439-9. Available online: https://trc.org.nz/treaty-waitangi-based-practice-health-promotion (accessed on 1 February 2022).
- Ní Shé, É.; Harrison, R. Mitigating unintended consequences of co-design in health care. Health Expect. 2021, 24, 1551–1556. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase | Participatory Activity | Participatory Stakeholders | # of Sessions |
|---|---|---|---|
| 1 | Expert Focus Groups and Interviews | Six dietitians, one nutrition researcher, two marketing academics, and three digital marketers. | Two focus groups and five one-on-one interviews. |
| 2 | End-User Co-design Workshops | Nineteen young women aged 18–24 years. | Three workshops, offered in three slots over three weeks. |
| 3 | Content Co-Creation | Ten student dietitians from the University of Auckland and one nutrition graduate from the co-design workshops. | |
| 4 | Expert and End-User Evaluation | One Senior Lecturer in Marketing, one Senior Research Fellow and Dietitian, and one participant from the co-design workshops. | |
| 5 | Content Finalisation | One student dietitian. |
| Median Age (yrs) | Location | Ethnicity | Occupation |
|---|---|---|---|
| 21.4 a | Auckland, NZ (n = 17) | NZ European (n = 8) | University Student (n = 12) |
| Waikato, NZ (n = 1) | Indian (n = 3) | Financial Sector (n = 3) | |
| Chinese (n = 3) | Food Industry (n = 2) | ||
| Fijian Indian (n = 2) | Health Research (n = 1) | ||
| Hong Kong Chinese (n = 1) | Retail (n = 1) | ||
| Korean (n = 1) | |||
| European (Other) (n = 1) |
| Workshop Session | Objectives | Activities | RQ(s) a |
|---|---|---|---|
| Session 1 |
|
| 1, 3 |
| Session 2 |
|
| 2, 3 |
| Session 3 |
|
| 1, 2, 3, 4 |
| Monday | Myth-Busting | Debunking common nutrition myths such as is a calorie a calorie, the ketogenic diet, fat-burning foods, and supplementation. |
| Tuesday | Simple Swaps | Simple and realistic swaps for each meal, baking and cooking to boost micronutrient and fibre content of dishes and snacks. |
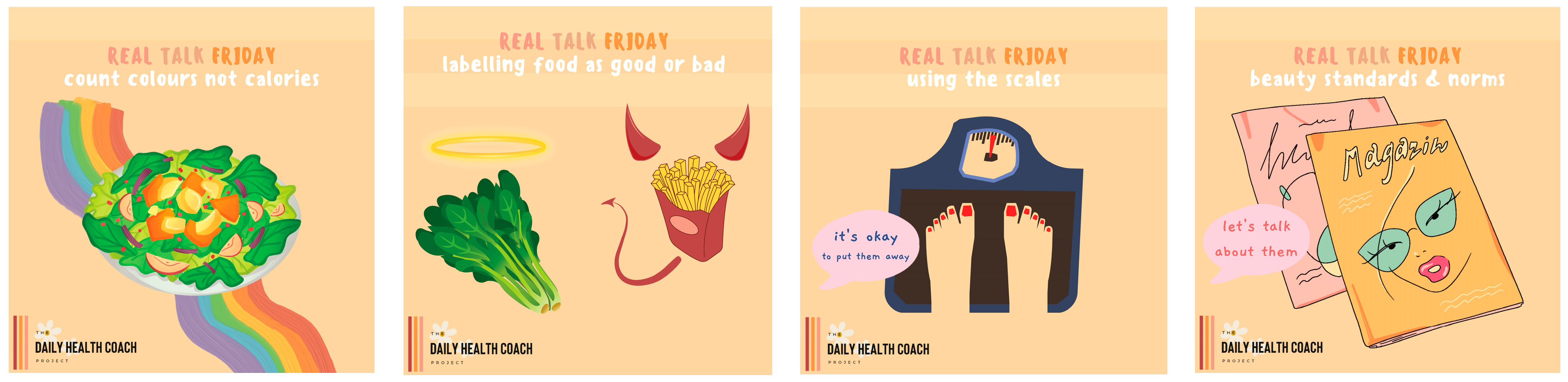
| Wednesday | Things You Should Know | Nutrition education including ultra-processed foods, nutrient-rich fats and carbohydrates, the gut microbiome, and the importance of dietary variety. |
| Thursday | The Other Important Stuff | Conversations around exercise (finding what works for you), sleep, stress, mental wellbeing, self-care, intuitive eating, and holism. |
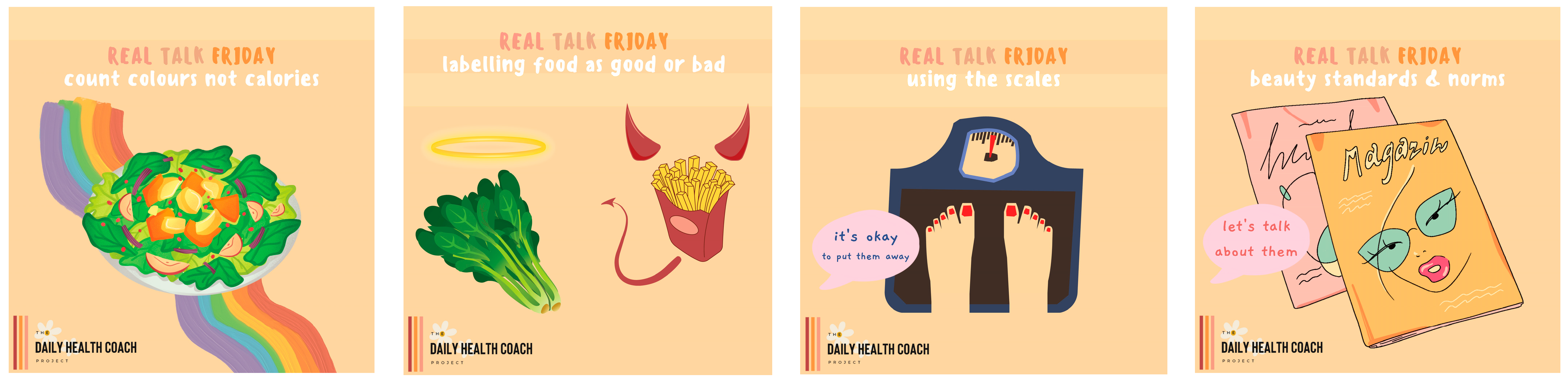
| Friday | Real Talk | Important topics of conversation suggested by co-designers including beauty standards and norms, restrictive or clean eating, food relationships (moralisation of food), and using the scales. |
| Saturday | Healthy Navigation | Suggestions to tailor social media use to increase digital health literacy, improve body image, and avoid damaging or triggering content. |
| Sunday | Recipe Sharing | Each content creator has shared a recipe that is special to them, including the price per recipe, per shop, and per meal. Recipes are affordable and balanced. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malloy, J.A.; Kemper, J.A.; Partridge, S.R.; Roy, R. Empowering Young Women: A Qualitative Co-Design Study of a Social Media Health Promotion Programme. Nutrients 2024, 16, 780. https://doi.org/10.3390/nu16060780
Malloy JA, Kemper JA, Partridge SR, Roy R. Empowering Young Women: A Qualitative Co-Design Study of a Social Media Health Promotion Programme. Nutrients. 2024; 16(6):780. https://doi.org/10.3390/nu16060780
Chicago/Turabian StyleMalloy, Jessica A., Joya A. Kemper, Stephanie R. Partridge, and Rajshri Roy. 2024. "Empowering Young Women: A Qualitative Co-Design Study of a Social Media Health Promotion Programme" Nutrients 16, no. 6: 780. https://doi.org/10.3390/nu16060780
APA StyleMalloy, J. A., Kemper, J. A., Partridge, S. R., & Roy, R. (2024). Empowering Young Women: A Qualitative Co-Design Study of a Social Media Health Promotion Programme. Nutrients, 16(6), 780. https://doi.org/10.3390/nu16060780