
Low Adherence to Mediterranean Diet Characterizes Metabolic Patients with Gastrointestinal Cancer
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Clinical Assessment and Biochemical Measurements
2.3. Chrono MedDiet Score
2.4. Med Diet Score
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Increased WC and Low HDL Cholesterol, Not BMI and LDL Cholesterol, Identify Cancer Patients
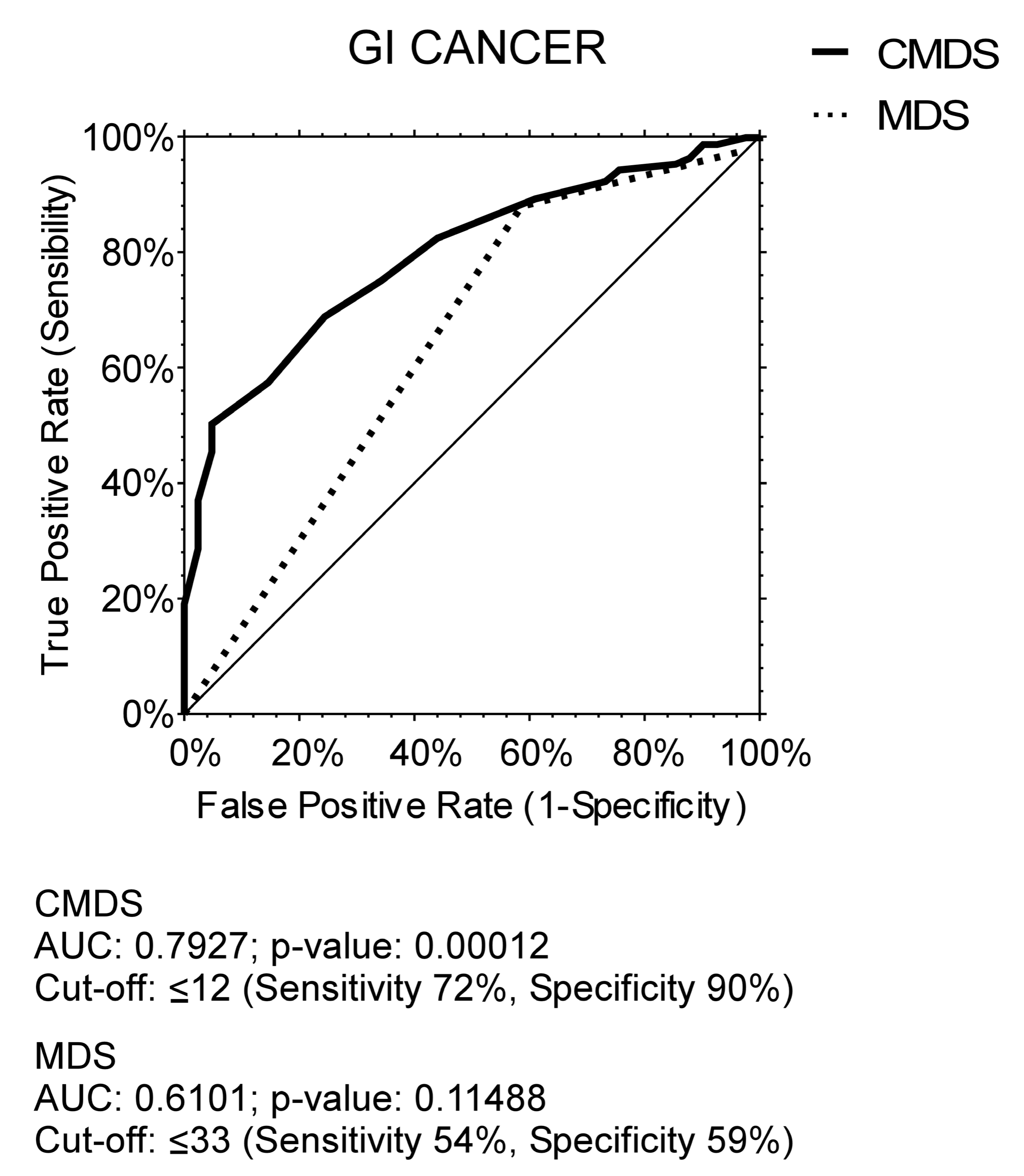
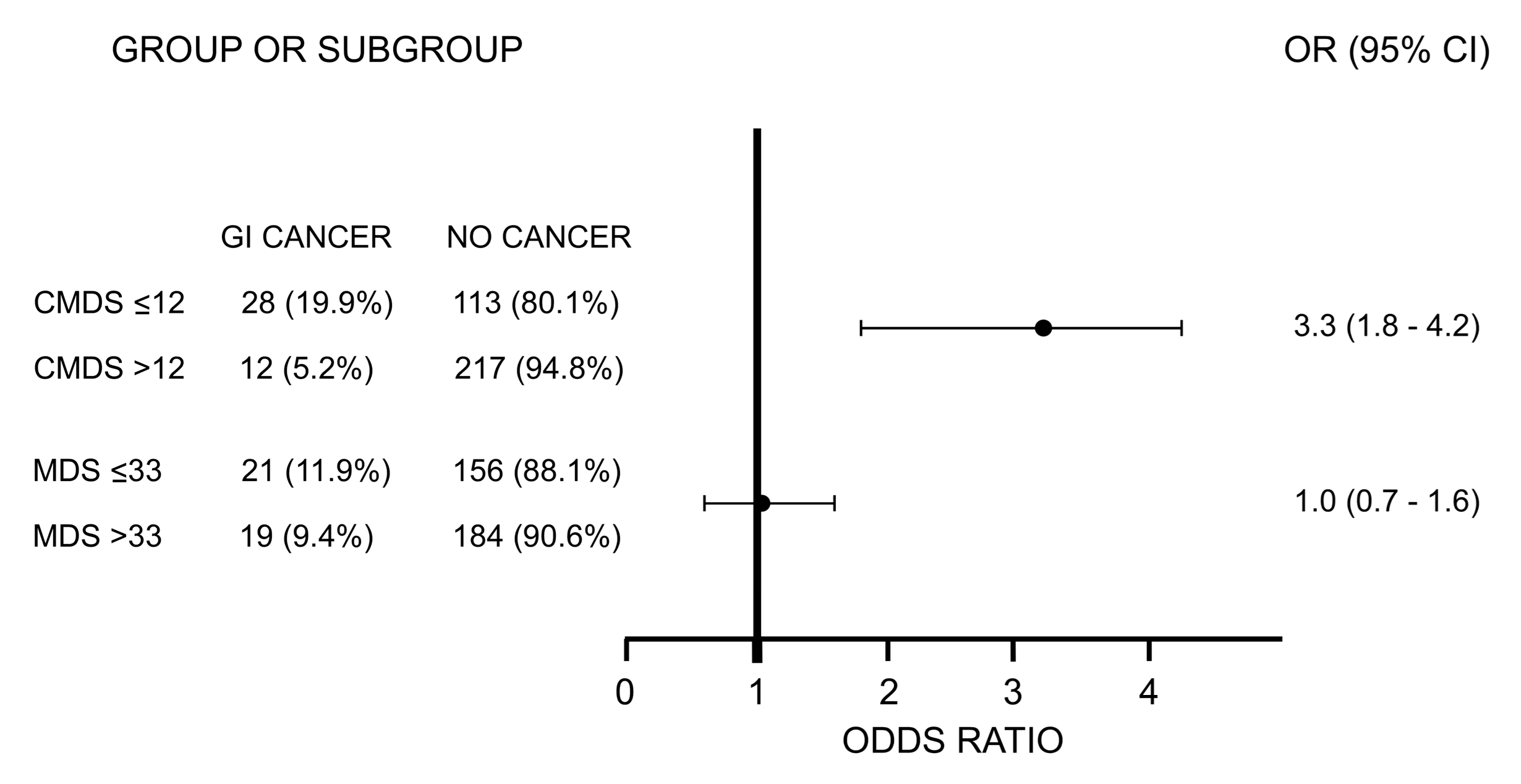
3.3. CMDS Is Associated with GI Cancer
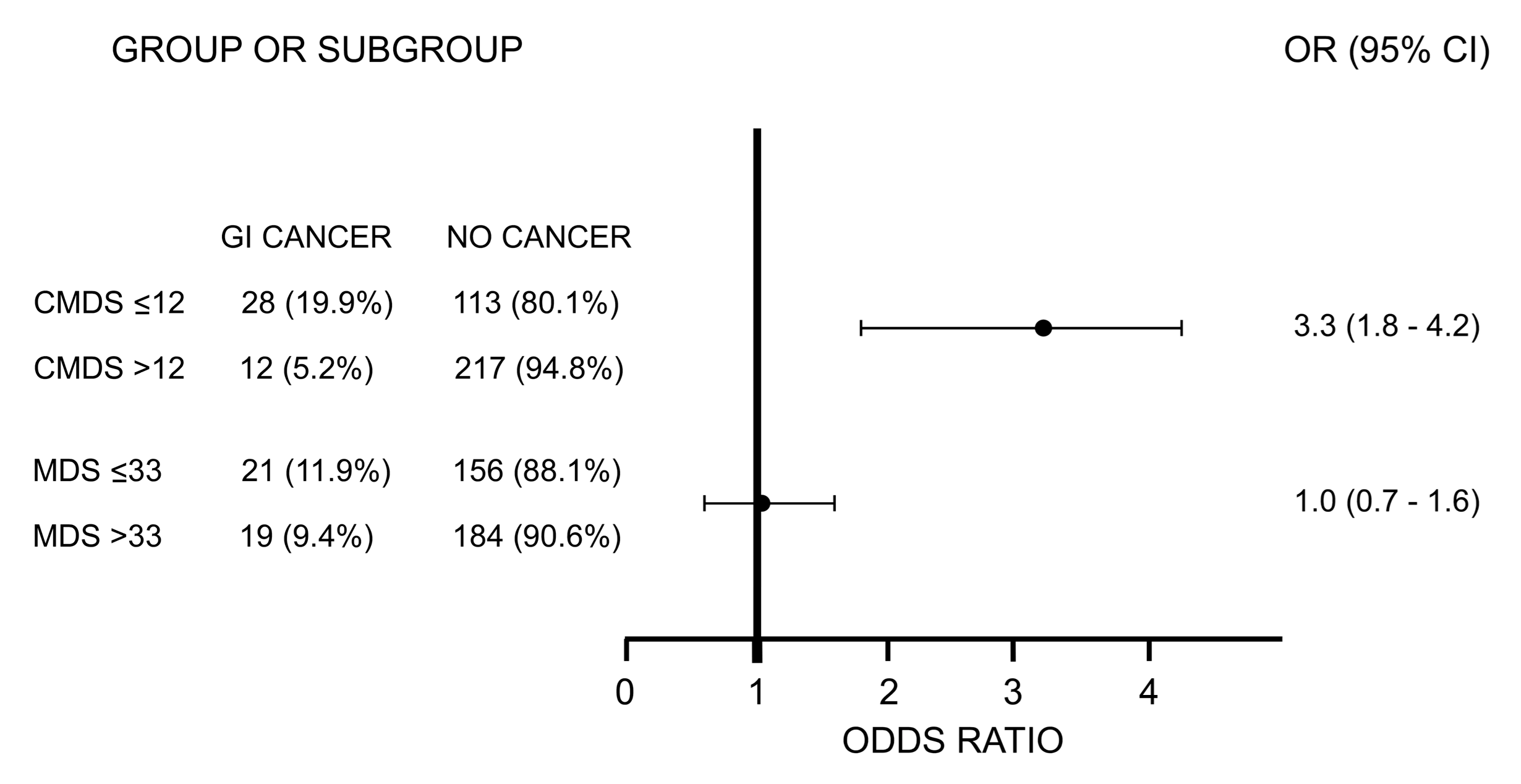
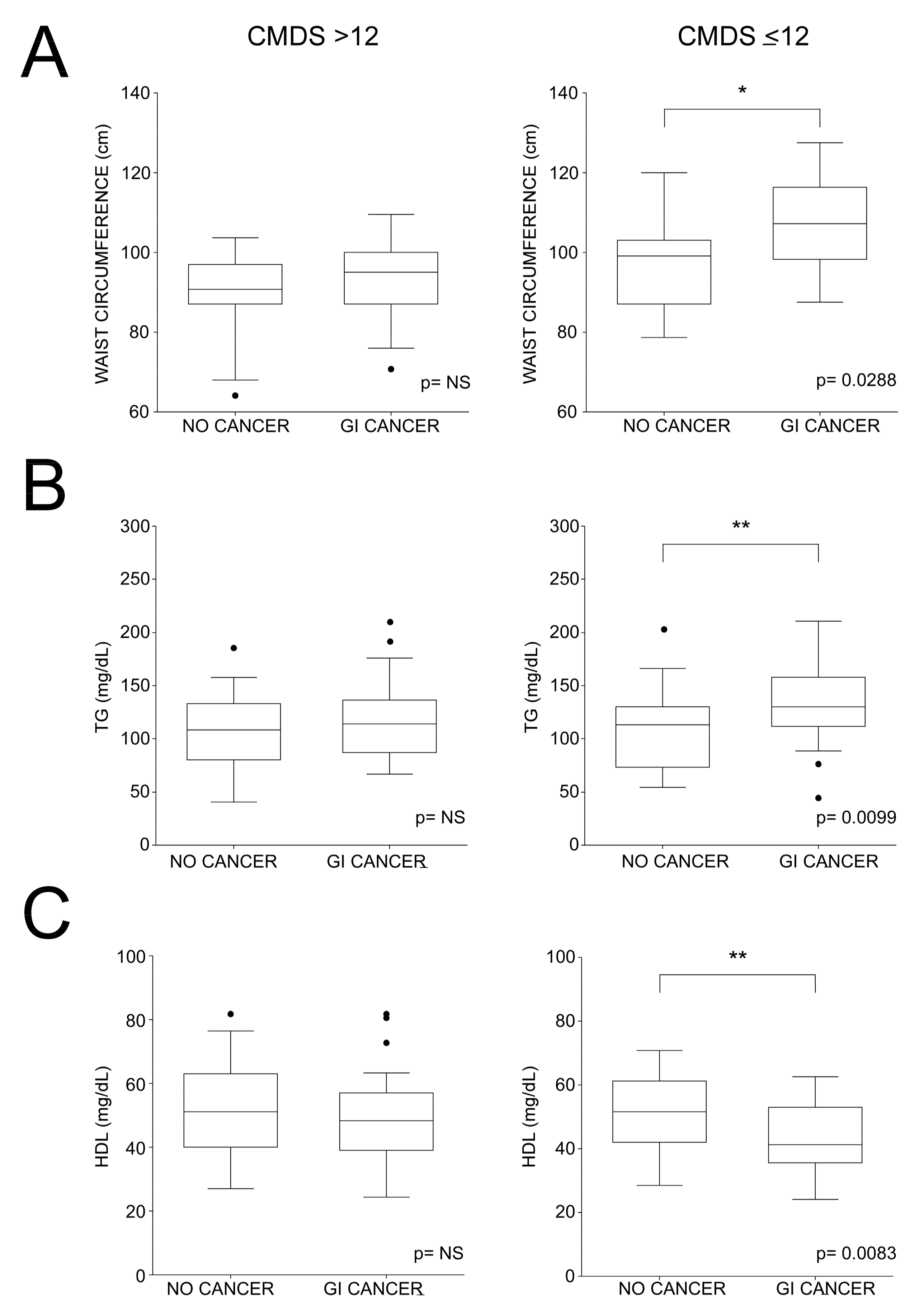
3.4. Characterization of GI Cancer Subjects According to CMDS Values
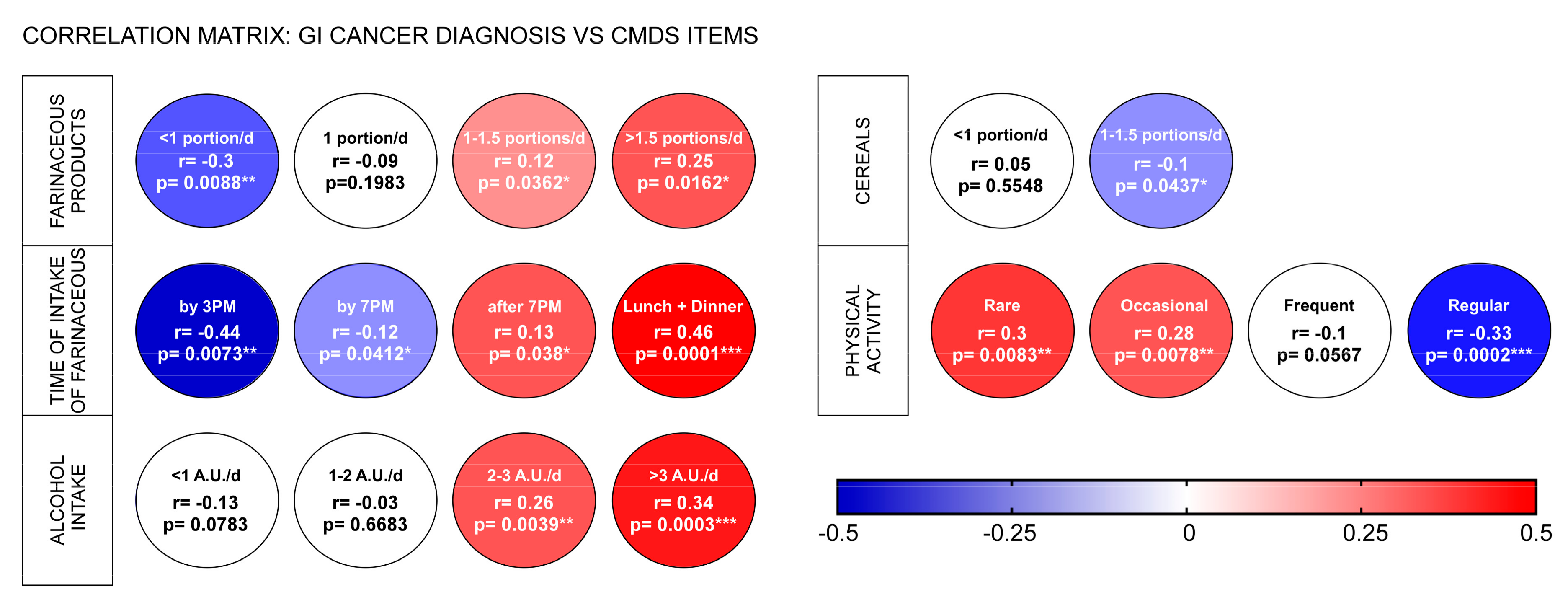
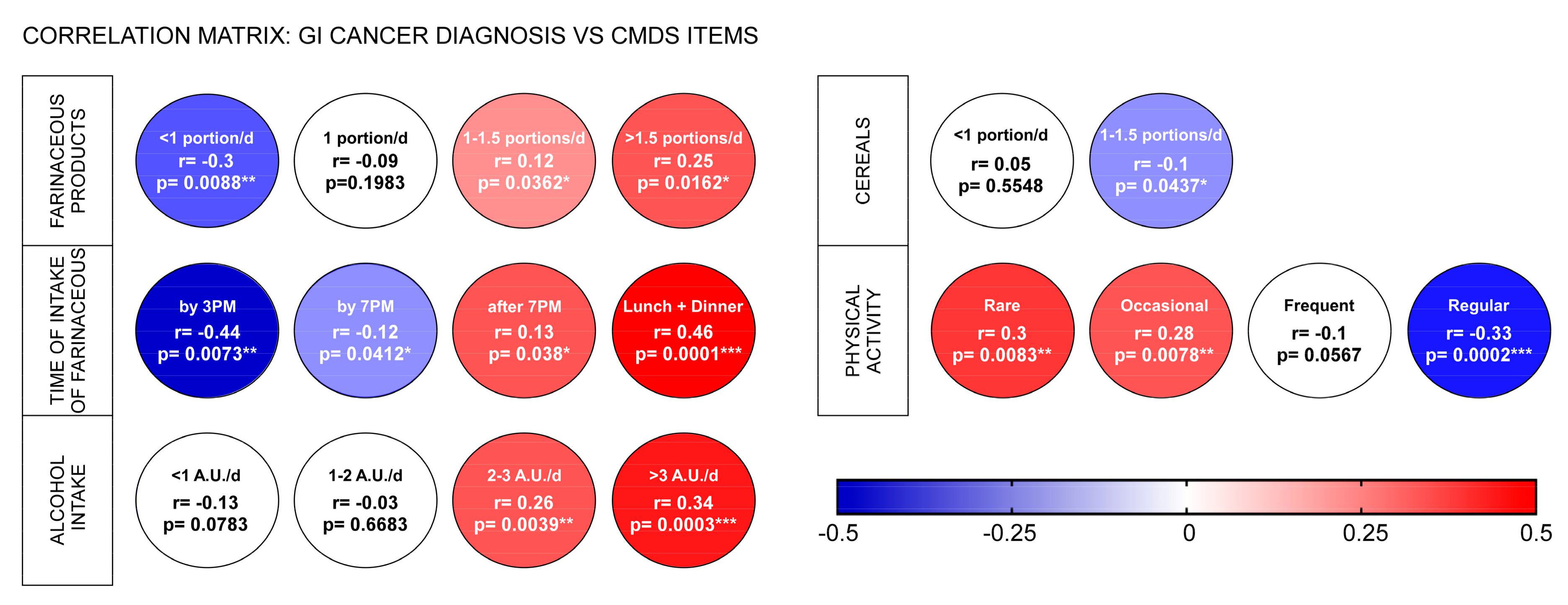
3.5. Correlations between GI Cancer Diagnosis and Specific CMDS Items
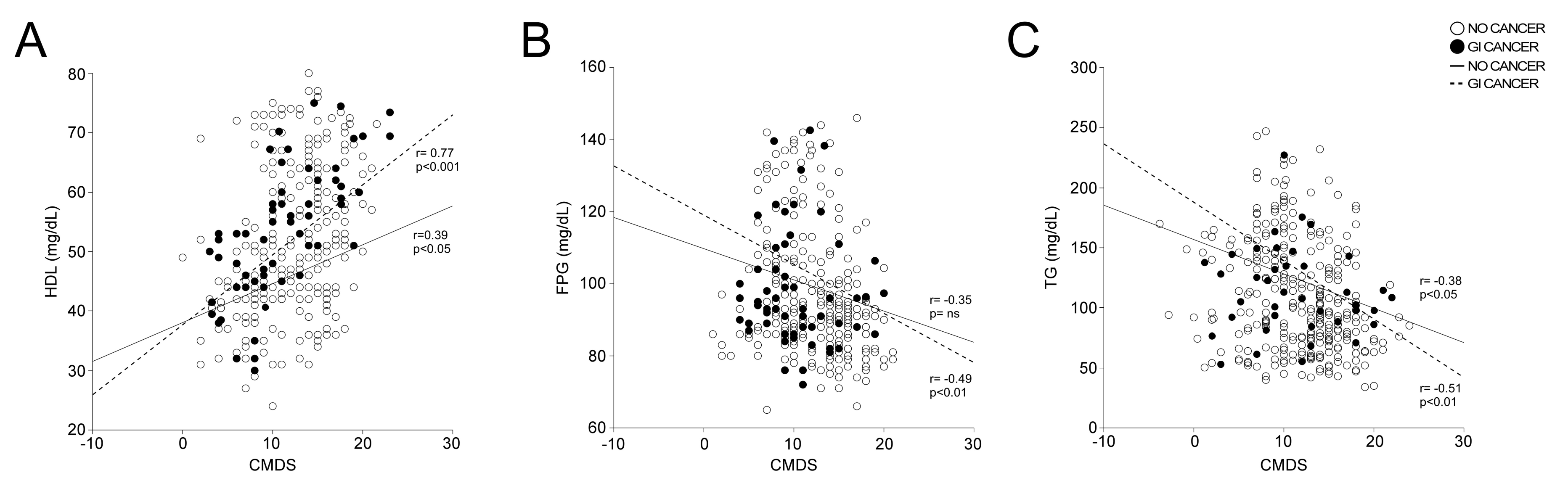
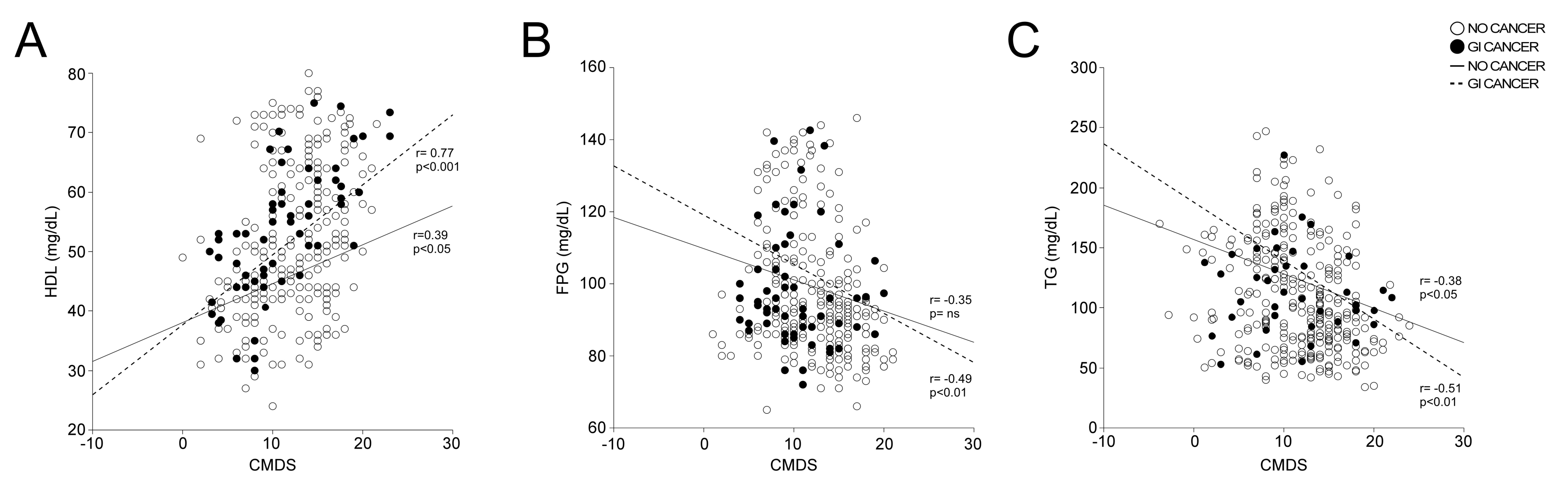
3.6. Correlations between CMDS and Serum Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349.e315. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Boden, S.; Myte, R.; Wennberg, M.; Harlid, S.; Johansson, I.; Shivappa, N.; Hebert, J.R.; Van Guelpen, B.; Nilsson, L.M. The inflammatory potential of diet in determining cancer risk; A prospective investigation of two dietary pattern scores. PLoS ONE 2019, 14, e0214551. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef]
- Crudele, L.; Piccinin, E.; Moschetta, A. Visceral Adiposity and Cancer: Role in Pathogenesis and Prognosis. Nutrients 2021, 13, 2101. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. International Agency for Research on Cancer Handbook Working G Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed]
- Murphy, N.; Jenab, M.; Gunter, M.J. Adiposity and gastrointestinal cancers: Epidemiology, mechanisms and future directions. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Piccinin, E.; Cariello, M.; De Santis, S.; Ducheix, S.; Sabba, C.; Ntambi, J.M.; Moschetta, A. Role of Oleic Acid in the Gut-Liver Axis: From Diet to the Regulation of Its Synthesis via Stearoyl-CoA Desaturase 1 (SCD1). Nutrients 2019, 11, 2283. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R., Jr.; Gross, M.D.; Tapsell, L.C. Food synergy: An operational concept for understanding nutrition. Am. J. Clin. Nutr. 2009, 89, 1543S–1548S. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Gonzalez, C.A.; Agudo, A.; Vilardell, M.; Berenguer, A.; Amiano, P.; Ardanaz, E.; Arriola, L.; Barricarte, A.; Basterretxea, M.; et al. Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study. Am. J. Epidemiol. 2009, 170, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Critselis, E. Mediterranean diet and longevity. Eur. J. Cancer Prev. 2004, 13, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Praud, D.; Bertuccio, P.; Bosetti, C.; Turati, F.; Ferraroni, M.; La Vecchia, C. Adherence to the Mediterranean diet and gastric cancer risk in Italy. Int. J. Cancer 2014, 134, 2935–2941. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Does a Mediterranean-Type Diet Reduce Cancer Risk? Curr. Nutr. Rep. 2016, 5, 9–17. [Google Scholar] [CrossRef]
- Verberne, L.; Bach-Faig, A.; Buckland, G.; Serra-Majem, L. Association between the Mediterranean diet and cancer risk: A review of observational studies. Nutr. Cancer 2010, 62, 860–870. [Google Scholar] [CrossRef]
- De Santis, S.; Cariello, M.; Piccinin, E.; Sabba, C.; Moschetta, A. Extra Virgin Olive Oil: Lesson from Nutrigenomics. Nutrients 2019, 11, 2085. [Google Scholar] [CrossRef]
- Li, Y.; Peng, Y.; Shen, Y.; Zhang, Y.; Liu, L.; Yang, X. Dietary polyphenols: Regulate the advanced glycation end products-RAGE axis and the microbiota-gut-brain axis to prevent neurodegenerative diseases. Crit. Rev. Food Sci. Nutr. 2023, 63, 9816–9842. [Google Scholar] [CrossRef]
- Merra, G.; Noce, A.; Marrone, G.; Cintoni, M.; Tarsitano, M.G.; Capacci, A.; De Lorenzo, A. Influence of Mediterranean Diet on Human Gut Microbiota. Nutrients 2020, 13, 7. [Google Scholar] [CrossRef]
- UNESCO. The Mediterranean Diet, Inscribed in 2013 on the Representative List of the Intangible Cultural Heritage of Humanity. Available online: https://ich.unesco.org/en/RL/mediterranean-diet-00884 (accessed on 28 January 2024).
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef]
- Buckland, G.; Agudo, A.; Travier, N.; Huerta, J.M.; Cirera, L.; Tormo, M.J.; Navarro, C.; Chirlaque, M.D.; Moreno-Iribas, C.; Ardanaz, E.; et al. Adherence to the Mediterranean diet reduces mortality in the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (EPIC-Spain). Br. J. Nutr. 2011, 106, 1581–1591. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, C.; Crudele, L.; Battaglia, S.; Loconte, T.; Rotondo, A.; Ferrulli, R.; Gadaleta, R.M.; Piazzolla, G.; Suppressa, P.; Sabba, C.; et al. Identification of a Novel Score for Adherence to the Mediterranean Diet That Is Inversely Associated with Visceral Adiposity and Cardiovascular Risk: The Chrono Med Diet Score (CMDS). Nutrients 2023, 15, 1910. [Google Scholar] [CrossRef]
- Cubiella, J.; Marzo-Castillejo, M.; Mascort-Roca, J.J.; Amador-Romero, F.J.; Bellas-Beceiro, B.; Clofent-Vilaplana, J.; Carballal, S.; Ferrandiz-Santos, J.; Gimeno-Garcia, A.Z.; Jover, R.; et al. Clinical practice guideline. Diagnosis and prevention of colorectal cancer. 2018 Update. Gastroenterol. Hepatol. 2018, 41, 585–596. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Associazione Italiana Oncologia Medica. Guidelines on Colorectal Tumours; Associazione Italiana Oncologia Medica: Milan, Italy, 2021. [Google Scholar]
- Saftoiu, A.; Hassan, C.; Areia, M.; Bhutani, M.S.; Bisschops, R.; Bories, E.; Cazacu, I.M.; Dekker, E.; Deprez, P.H.; Pereira, S.P.; et al. Role of gastrointestinal endoscopy in the screening of digestive tract cancers in Europe: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement. Endoscopy 2020, 52, 293–304. [Google Scholar] [CrossRef]
- World Medical Association. WMA Declaration of Helsinki-Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 12 February 2024).
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef]
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Crudele, L.; De Matteis, C.; Piccinin, E.; Gadaleta, R.M.; Cariello, M.; Di Buduo, E.; Piazzolla, G.; Suppressa, P.; Berardi, E.; Sabba, C.; et al. Low HDL-cholesterol levels predict hepatocellular carcinoma development in individuals with liver fibrosis. JHEP Rep. 2023, 5, 100627. [Google Scholar] [CrossRef]
- Crudele, L.; Novielli, F.; De Matteis, C.; Petruzzelli, S.; Suppressa, P.; Berardi, E.; Antonica, G.; Piazzolla, G.; Sabba, C.; Graziano, G.; et al. Thyroid nodule malignancy is associated with increased non-invasive hepatic fibrosis scores in metabolic subjects. Front. Oncol. 2023, 13, 1233083. [Google Scholar] [CrossRef]
- Crudele, L.; De Matteis, C.; Graziano, G.; Novielli, F.; Petruzzelli, S.; Piccinin, E.; Gadaleta, R.M.; Cariello, M.; Moschetta, A. AST/ALT-to-platelet ratio (AARPRI) predicts gynaecological cancers: A 8-years follow-up study in 653 women. Sci. Rep. 2023, 13, 17793. [Google Scholar] [CrossRef]
- Bovenga, F.; Sabba, C.; Moschetta, A. Uncoupling nuclear receptor LXR and cholesterol metabolism in cancer. Cell Metab. 2015, 21, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Moschetta, A. Nuclear receptor LXR as a novel therapeutic antitumoral target in glioblastoma. Cancer Discov. 2011, 1, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Estruch, R.; Corella, D.; Fito, M.; Ros, E.; Predimed, I. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Muralidharan, J.; Moreno-Indias, I.; Bullo, M.; Lopez, J.V.; Corella, D.; Castaner, O.; Vidal, J.; Atzeni, A.; Fernandez-Garcia, J.C.; Torres-Collado, L.; et al. Effect on gut microbiota of a 1-y lifestyle intervention with Mediterranean diet compared with energy-reduced Mediterranean diet and physical activity promotion: PREDIMED-Plus Study. Am. J. Clin. Nutr. 2021, 114, 1148–1158. [Google Scholar] [CrossRef]
- Dai, J.; Jones, D.P.; Goldberg, J.; Ziegler, T.R.; Bostick, R.M.; Wilson, P.W.; Manatunga, A.K.; Shallenberger, L.; Jones, L.; Vaccarino, V. Association between adherence to the Mediterranean diet and oxidative stress. Am. J. Clin. Nutr. 2008, 88, 1364–1370. [Google Scholar] [PubMed]
- Thompson, S.V.; Bailey, M.A.; Taylor, A.M.; Kaczmarek, J.L.; Mysonhimer, A.R.; Edwards, C.G.; Reeser, G.E.; Burd, N.A.; Khan, N.A.; Holscher, H.D. Avocado Consumption Alters Gastrointestinal Bacteria Abundance and Microbial Metabolite Concentrations among Adults with Overweight or Obesity: A Randomized Controlled Trial. J. Nutr. 2021, 151, 753–762. [Google Scholar] [CrossRef]
- Ocvirk, S.; Wilson, A.S.; Appolonia, C.N.; Thomas, T.K.; O’Keefe, S.J.D. Fiber, Fat, and Colorectal Cancer: New Insight into Modifiable Dietary Risk Factors. Curr. Gastroenterol. Rep. 2019, 21, 62. [Google Scholar] [CrossRef]
- Vareiro, D.; Bach-Faig, A.; Raido Quintana, B.; Bertomeu, I.; Buckland, G.; Vaz de Almeida, M.D.; Serra-Majem, L. Availability of Mediterranean and non-Mediterranean foods during the last four decades: Comparison of several geographical areas. Public Health Nutr. 2009, 12, 1667–1675. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72 (Suppl. S1), 83–91. [Google Scholar] [CrossRef]
- Zaragoza-Marti, A.; Cabanero-Martinez, M.J.; Hurtado-Sanchez, J.A.; Laguna-Perez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef]
- Aoun, C.; Papazian, T.; Helou, K.; El Osta, N.; Khabbaz, L.R. Comparison of five international indices of adherence to the Mediterranean diet among healthy adults: Similarities and differences. Nutr. Res. Pract. 2019, 13, 333–343. [Google Scholar] [CrossRef]
- Zhong, Y.; Zhu, Y.; Li, Q.; Wang, F.; Ge, X.; Zhou, G.; Miao, L. Association between Mediterranean diet adherence and colorectal cancer: A dose-response meta-analysis. Am. J. Clin. Nutr. 2020, 111, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Terzic, J.; Grivennikov, S.; Karin, E.; Karin, M. Inflammation and colon cancer. Gastroenterology 2010, 138, 2101–2114.e5. [Google Scholar] [CrossRef]
- Kay, J.; Thadhani, E.; Samson, L.; Engelward, B. Inflammation-induced DNA damage, mutations and cancer. DNA Repair. 2019, 83, 102673. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A.; Rock, E. Toward a new philosophy of preventive nutrition: From a reductionist to a holistic paradigm to improve nutritional recommendations. Adv. Nutr. 2014, 5, 430–446. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Gallus, S.; Trichopoulou, A.; Talamini, R.; Franceschi, S.; Negri, E.; La Vecchia, C. Influence of the Mediterranean diet on the risk of cancers of the upper aerodigestive tract. Cancer Epidemiol. Biomark. Prev. 2003, 12, 1091–1094. [Google Scholar]
- Morze, J.; Danielewicz, A.; Przybylowicz, K.; Zeng, H.; Hoffmann, G.; Schwingshackl, L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur. J. Nutr. 2021, 60, 1561–1586. [Google Scholar] [CrossRef]
- Larsson, S.C.; Hakansson, N.; Wolk, A. Healthy dietary patterns and incidence of biliary tract and gallbladder cancer in a prospective study of women and men. Eur. J. Cancer 2017, 70, 42–47. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Toledo, E.; Salas-Salvado, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fito, M.; Hu, F.B.; Aros, F.; et al. Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Dinu, M.; Pagliai, G.; Marcucci, R.; Casini, A. Validation of a literature-based adherence score to Mediterranean diet: The MEDI-LITE score. Int. J. Food Sci. Nutr. 2017, 68, 757–762. [Google Scholar] [CrossRef]
- Djuric, Z.; Rifkin, S. A New Score for Quantifying Adherence to a Cancer-Preventive Mediterranean Diet. Nutr. Cancer 2022, 74, 579–591. [Google Scholar] [CrossRef]
- Campbell, P.T.; Newton, C.C.; Kitahara, C.M.; Patel, A.V.; Hartge, P.; Koshiol, J.; McGlynn, K.A.; Adami, H.O.; Berrington de Gonzalez, A.; Beane Freeman, L.E.; et al. Body Size Indicators and Risk of Gallbladder Cancer: Pooled Analysis of Individual-Level Data from 19 Prospective Cohort Studies. Cancer Epidemiol. Biomark. Prev. 2017, 26, 597–606. [Google Scholar] [CrossRef]
- Lu, Y.; Cross, A.J.; Murphy, N.; Freisling, H.; Travis, R.C.; Ferrari, P.; Katzke, V.A.; Kaaks, R.; Olsson, A.; Johansson, I.; et al. Comparison of abdominal adiposity and overall obesity in relation to risk of small intestinal cancer in a European Prospective Cohort. Cancer Causes Control 2016, 27, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Pischon, T.; Lahmann, P.H.; Boeing, H.; Friedenreich, C.; Norat, T.; Tjonneland, A.; Halkjaer, J.; Overvad, K.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; et al. Body size and risk of colon and rectal cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst. 2006, 98, 920–931. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Variable | N = 401 (197M:204F) Mean ± SD |
|---|---|
| Age (Years) | 59.5 ± 5.9 |
| BMI (kg/m2) | 27.3 ± 4.3 |
| WC (cm) | 96.0 ± 7.4 |
| TC (mg/dL) | 177.4 ± 14.2 |
| HDL-c (mg/dL) | 52.5 ± 5.7 |
| LDL-c (mg/dL) | 105.2 ± 9.5 |
| TG (mg/dL) | 120.5 ± 13.5 |
| FPG (mg/dL) | 98.4 ± 11.4 |
| CMDS | 13.7 ± 1.9 |
| MDS | 33.0 ± 5.8 |
| Clinical Variable | No Cancer N = 330 (160M:170F) Mean ± SD | Cancer N = 71 (37M:34F) Mean ± SD | p-Value |
|---|---|---|---|
| Age (Years) | 61.7 ± 4.2 | 58.9 ± 5.8 | 0.3823 |
| BMI (kg/m2) | 26.8 ± 3.8 | 28.7 ± 4.4 | 0.2419 |
| WC (cm) | 94.1 ± 4.5 | 101.2 ± 6.8 | 0.0377 * |
| TC (mg/dL) | 168.4 ± 12.3 | 191.5 ± 13.2 | 0.1102 |
| HDL-c (mg/dL) | 52.8 ± 7.4 | 46.1 ± 6.3 | 0.0079 ** |
| LDL-c (mg/dL) | 106.1 ± 11.1 | 106.4 ± 15.4 | 0.8582 |
| TG (mg/dL) | 111.3 ± 9.3 | 143.7 ± 21.9 | 0.1155 |
| FPG (mg/dL) | 92.4 ± 8.4 | 116.8 ± 6.8 | 0.0175 * |
| No Cancer N = 330 (160M:170F) Mean ± SD | Cancer N = 71 (37M:34F) Mean ± SD | p-value | |
|---|---|---|---|
| CMDS | 14.9 ± 2.3 | 8.0 ± 2.1 | 0.0017 *** |
| MDS | 36.1 ± 2.8 | 33.9 ± 5.8 | 0.2768 |
| No Cancer N = 330 (160M:170F) Mean ± SD | GI Cancer N = 40 (27M:13F) Mean ± SD | p-value | |
| CMDS | 14.9 ± 2.3 | 6.3 ± 1.9 | 0.0029 *** |
| MDS | 36.1 ± 2.8 | 33.4 ± 7.5 | 0.1882 |
| GI Cancer N = 40 (27M:13F) Mean ± SD | Non-GI Cancer N = 31 (10M:21F) Mean ± SD | p-value | |
| CMDS | 6.3 ± 1.9 | 10.5 ± 3.1 | 0.0002 *** |
| MDS | 33.4 ± 7.5 | 34.1 ± 6.9 | 0.8993 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Matteis, C.; Crudele, L.; Gadaleta, R.M.; Di Buduo, E.; Novielli, F.; Petruzzelli, S.; Cariello, M.; Moschetta, A. Low Adherence to Mediterranean Diet Characterizes Metabolic Patients with Gastrointestinal Cancer. Nutrients 2024, 16, 630. https://doi.org/10.3390/nu16050630
De Matteis C, Crudele L, Gadaleta RM, Di Buduo E, Novielli F, Petruzzelli S, Cariello M, Moschetta A. Low Adherence to Mediterranean Diet Characterizes Metabolic Patients with Gastrointestinal Cancer. Nutrients. 2024; 16(5):630. https://doi.org/10.3390/nu16050630
Chicago/Turabian StyleDe Matteis, Carlo, Lucilla Crudele, Raffaella Maria Gadaleta, Ersilia Di Buduo, Fabio Novielli, Stefano Petruzzelli, Marica Cariello, and Antonio Moschetta. 2024. "Low Adherence to Mediterranean Diet Characterizes Metabolic Patients with Gastrointestinal Cancer" Nutrients 16, no. 5: 630. https://doi.org/10.3390/nu16050630
APA StyleDe Matteis, C., Crudele, L., Gadaleta, R. M., Di Buduo, E., Novielli, F., Petruzzelli, S., Cariello, M., & Moschetta, A. (2024). Low Adherence to Mediterranean Diet Characterizes Metabolic Patients with Gastrointestinal Cancer. Nutrients, 16(5), 630. https://doi.org/10.3390/nu16050630