
Vitamin D Status and Reference Intervals Measured by Liquid Chromatography–Tandem Mass Spectrometry for the Early Adulthood to Geriatric Ages in a South Korean Population during 2017–2022

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
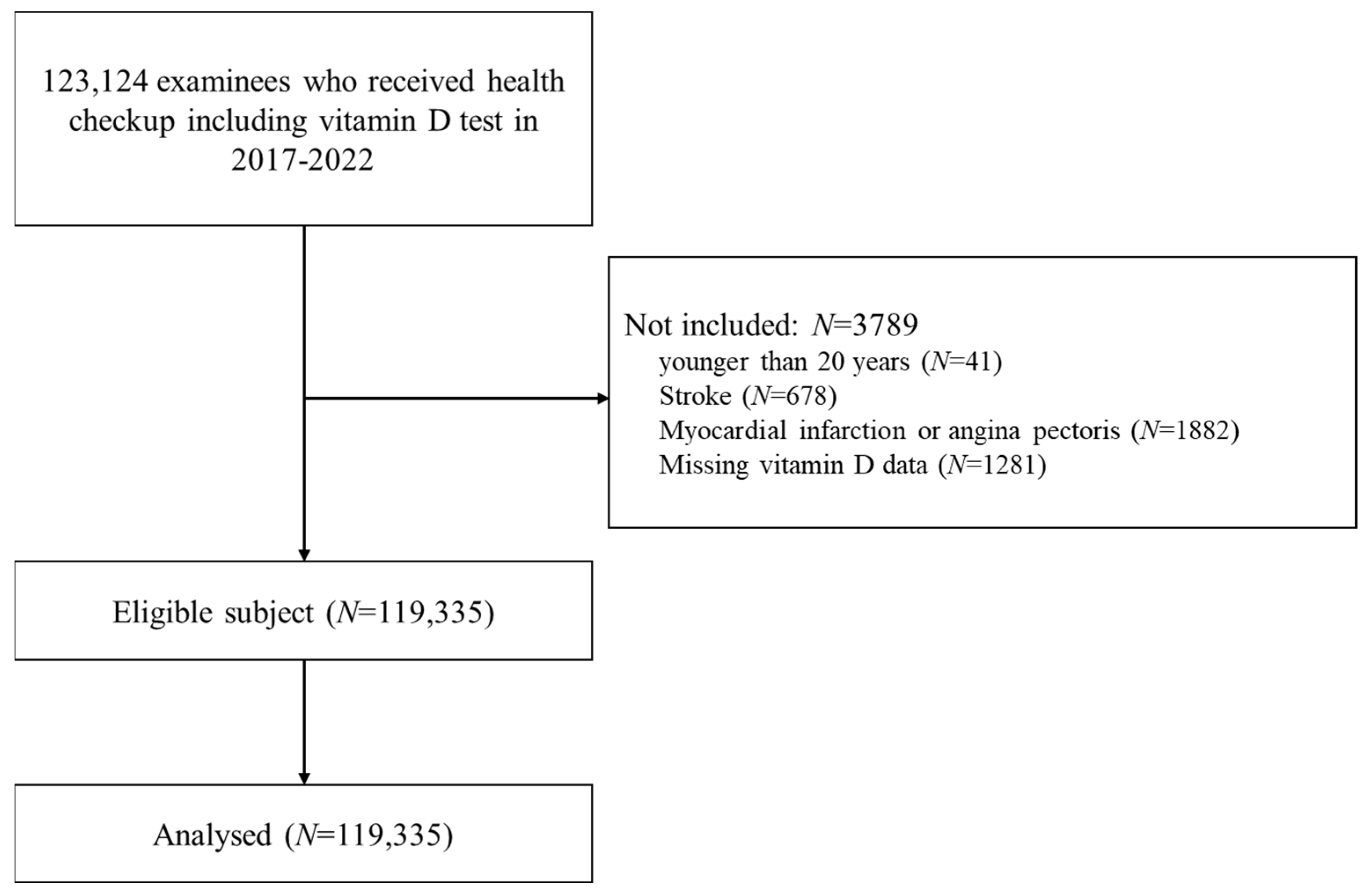
2.1. Study Population
2.2. Laboratory Measurements of Serum 25(OH)D
2.3. Statistical Analysis and Calculation of Reference Intervals for Serum 25(OH)D2, 25(OH)D3, and Total 25(OH)D
3. Results
3.1. Characteristics of Study Subjects
3.2. Distributions of Total 25(OH)D, 25(OH)D2, and 25(OH)D3 Concentrations by Sex, Age, Season, and Demographic Characteristics
3.3. RIs for Serum 25(OH) D2, 25(OH)D3, and Total 25(OH)D
3.4. Prevalence of 25(OH)D Deficiency for Different Cutoff Values
3.5. Factors Associated with Total Serum 25(OH)D Concentration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Aspray, T.J.; Bowring, C.; Fraser, W.; Gittoes, N.; Javaid, M.K.; Macdonald, H.; Patel, S.; Selby, P.; Tanna, N.; Francis, R.M.; et al. National Osteoporosis Society Vitamin D Guideline Summary. Age Ageing 2014, 43, 592–595. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Jang, G.; Park, J.W.; Lee, Y.-K.; Koo, K.-H. Vitamin D Deficiency and Sarcopenia in Hip Fracture Patients. J. Bone Metab. 2021, 28, 79–83. [Google Scholar] [CrossRef]
- Giovannucci, E.; Liu, Y.; Rimm, E.B.; Hollis, B.W.; Fuchs, C.S.; Stampfer, M.J.; Willett, W.C. Prospective Study of Predictors of Vitamin D Status and Cancer Incidence and Mortality in Men. J. Natl. Cancer Inst. 2006, 98, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, L.H.M.; Butler, A.E.; Dargham, S.R.; Latif, A.; Robay, A.; Chidiac, O.M.; Jayyousi, A.; Al Suwaidi, J.; Crystal, R.G.; Atkin, S.L.; et al. Association of Vitamin D2 and D3 with Type 2 Diabetes Complications. BMC Endocr. Disord. 2020, 20, 65. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, M.; Sullivan, D.R.; Veillard, A.-S.; McCorquodale, T.; Straub, I.R.; Scott, R.; Laakso, M.; Topliss, D.; Jenkins, A.J.; Blankenberg, S.; et al. Serum 25-Hydroxyvitamin D: A Predictor of Macrovascular and Microvascular Complications in Patients with Type 2 Diabetes. Diabetes Care 2015, 38, 521–528. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Theodor, E.; Segal, R.M.; Shoenfeld, Y. Vitamin D in Systemic and Organ-Specific Autoimmune Diseases. Clin. Rev. Allergy. Immunol. 2013, 45, 256–266. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Sternberg, M.R.; Looker, A.C.; Yetley, E.A.; Lacher, D.A.; Sempos, C.T.; Taylor, C.L.; Durazo-Arvizu, R.A.; Maw, K.L.; Chaudhary-Webb, M.; et al. National Estimates of Serum Total 25-Hydroxyvitamin D and Metabolite Concentrations Measured by Liquid Chromatography-Tandem Mass Spectrometry in the US Population during 2007–2010. J. Nutr. 2016, 146, 1051–1061. [Google Scholar] [CrossRef]
- Sarafin, K.; Durazo-Arvizu, R.; Tian, L.; Phinney, K.W.; Tai, S.; Camara, J.E.; Merkel, J.; Green, E.; Sempos, C.T.; Brooks, S.P.J. Standardizing 25-Hydroxyvitamin D Values from the Canadian Health Measures Survey. Am. J. Clin. Nutr. 2015, 102, 1044–1050. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D Deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Seamans, K.M.; Cashman, K.D. Existing and Potentially Novel Functional Markers of Vitamin D Status: A Systematic Review. Am. J. Clin. Nutr. 2009, 89, 1997S–2008S. [Google Scholar] [CrossRef] [PubMed]
- Roth, H.J.; Schmidt-Gayk, H.; Weber, H.; Niederau, C. Accuracy and Clinical Implications of Seven 25-Hydroxyvitamin D Methods Compared with Liquid Chromatography-Tandem Mass Spectrometry as a Reference. Ann. Clin. Biochem. 2008, 45, 153–159. [Google Scholar] [CrossRef] [PubMed]
- US Preventive Services Task Force; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Epling, J.W.; et al. Screening for Vitamin D Deficiency in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1436–1442. [Google Scholar] [CrossRef]
- Vogeser, M.; Seger, C. A Decade of HPLC-MS/MS in the Routine Clinical Laboratory--Goals for Further Developments. Clin. Biochem. 2008, 41, 649–662. [Google Scholar] [CrossRef]
- Phinney, K.W.; Bedner, M.; Tai, S.S.-C.; Vamathevan, V.V.; Sander, L.C.; Sharpless, K.E.; Wise, S.A.; Yen, J.H.; Schleicher, R.L.; Chaudhary-Webb, M.; et al. Development and Certification of a Standard Reference Material for Vitamin D Metabolites in Human Serum. Anal. Chem. 2012, 84, 956–962. [Google Scholar] [CrossRef]
- Wise, S.A.; Camara, J.E.; Burdette, C.Q.; Hahm, G.; Nalin, F.; Kuszak, A.J.; Merkel, J.; Durazo-Arvizu, R.A.; Williams, E.L.; Popp, C.; et al. Interlaboratory Comparison of 25-Hydroxyvitamin D Assays: Vitamin D Standardization Program (VDSP) Intercomparison Study 2—Part 2 Ligand Binding Assays—Impact of 25-Hydroxyvitamin D2 and 24R,25-Dihydroxyvitamin D3 on Assay Performance. Anal. Bioanal. Chem. 2022, 414, 351–366. [Google Scholar] [CrossRef]
- You, H.; Shin, H.R.; Song, S.; Ly, S.Y. Vitamin D Intake and Bone Mineral Density in Korean Adults: Analysis of the 2009-2011 Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2022, 16, 775–788. [Google Scholar] [CrossRef]
- Park, J.-H.; Hong, I.Y.; Chung, J.W.; Choi, H.S. Vitamin D Status in South Korean Population: Seven-Year Trend from the KNHANES. Medicine 2018, 97, e11032. [Google Scholar] [CrossRef]
- Choi, R.; Cho, S.-E.; Lee, S.G.; Lee, E.H. Recent Information on Vitamin D Deficiency in an Adult Korean Population Visiting Local Clinics and Hospitals. Nutrients 2022, 14, 1978. [Google Scholar] [CrossRef]
- Royal Osteoporosis Society. Vitamin D and Bone Health: A Practical Clinical Guideline for Patient Management. Available online: https://strwebprdmedia.blob.core.windows.net/media/ef2ideu2/ros-vitamin-d-and-bone-health-in-adults-february-2020.pdf (accessed on 25 December 2023).
- C28-A3; Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory: Approved Guideline. 3rd ed, Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2010; ISBN 978-1-56238-682-5.
- Scragg, R.; Sluyter, J.D. Is There Proof of Extraskeletal Benefits From Vitamin D Supplementation From Recent Mega Trials of Vitamin D? JBMR Plus 2021, 5, e10459. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The Health Effects of Vitamin D Supplementation: Evidence from Human Studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.F. Clinical Review: The 2011 Report on Dietary Reference Intake for Vitamin D: Where Do We Go from Here? J. Clin. Endocrinol. Metab. 2011, 96, 2987–2996. [Google Scholar] [CrossRef] [PubMed]
- Rabenberg, M.; Scheidt-Nave, C.; Busch, M.A.; Rieckmann, N.; Hintzpeter, B.; Mensink, G.B.M. Vitamin D Status among Adults in Germany—Results from the German Health Interview and Examination Survey for Adults (DEGS1). BMC Public Health 2015, 15, 641. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products. Nutrition and Allergies (NDA) Dietary Reference Values for Vitamin D. EFSA 2016, 14. [Google Scholar] [CrossRef]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the Healthy European Paediatric Population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global Prevalence and Disease Burden of Vitamin D Deficiency: A Roadmap for Action in Low- and Middle-Income Countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef]
- Cashman, K.D.; Ritz, C.; Adebayo, F.A.; Dowling, K.G.; Itkonen, S.T.; Öhman, T.; Skaffari, E.; Saarnio, E.M.; Kiely, M.; Lamberg-Allardt, C. Differences in the Dietary Requirement for Vitamin D among Caucasian and East African Women at Northern Latitude. Eur. J. Nutr. 2019, 58, 2281–2291. [Google Scholar] [CrossRef]
- Giuliani, S.; Barbieri, V.; Di Pierro, A.M.; Rossi, F.; Widmann, T.; Lucchiari, M.; Pusceddu, I.; Pilz, S.; Obermayer-Pietsch, B.; Herrmann, M. LC-MS/MS Based 25(OH)D Status in a Large Southern European Outpatient Cohort: Gender- and Age-Specific Differences. Eur. J. Nutr. 2019, 58, 2511–2520. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Kinsella, M.; Walton, J.; Flynn, A.; Hayes, A.; Lucey, A.J.; Seamans, K.M.; Kiely, M. The 3 Epimer of 25-Hydroxycholecalciferol Is Present in the Circulation of the Majority of Adults in a Nationally Representative Sample and Has Endogenous Origins. J. Nutr. 2014, 144, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Sowah, D.; Fan, X.; Dennett, L.; Hagtvedt, R.; Straube, S. Vitamin D Levels and Deficiency with Different Occupations: A Systematic Review. BMC Public Health 2017, 17, 519. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Papa, F.; Magrini, A. Are Shiftwork and Indoor Work Related to D3 Vitamin Deficiency? A Systematic Review of Current Evidences. J. Environ. Public Health 2018, 2018, 8468742. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | 25(OH)D2 | p-Value | Multiple Comparison | 25(OH)D3 | p-Value | Multiple Comparison | Total 25(OH)D | p-Value | Multiple Comparison | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD (nmol/L) | Mean ± SD (nmol/L) | Mean ± SD (nmol/L) | |||||||||
| All | 119,335 | 0.5 ± 2.53 | - | 54.0 ± 24.0 | - | 54.5 ± 24.0 | - | ||||
| Sex | |||||||||||
| Male | 58,151 | 0.43 ± 2.2 | <0.001 | 52.3 ± 21.0 | <0.001 | 52.5 ± 21.0 | <0.001 | ||||
| Female | 61,184 | 0.6 ± 2.8 | 55.5 ± 26.5 | 56.3 ± 26.5 | |||||||
| Age, year | |||||||||||
| 20–29 a | 1981 | 0.33 ± 2.25 | <0.001 | a,b,c < d < e < f | 39.8 ± 19.0 | <0.001 | a < b < c < d < e < f | 40.0 ± 19.0 | <0.001 | a < b < c < d < e < f | |
| 30–39 b | 9286 | 0.38 ± 2.18 | 46.0 ± 20.8 | 46.3 ± 20.8 | |||||||
| 40–49 c | 22,175 | 0.38 ± 2.08 | 48.5 ± 21.0 | 48.8 ± 21.0 | |||||||
| 50–59 d | 38,049 | 0.45 ± 2.15 | 54.3 ± 23.3 | 54.8 ± 23.3 | |||||||
| 60–69 e | 37,557 | 0.63 ± 2.85 | 58.0 ± 25.0 | 58.5 ± 25.0 | |||||||
| ≥70 f | 10,287 | 0.75 ± 3.63 | 60.0 ± 27.0 | 60.5 ± 27.0 | |||||||
| Month | |||||||||||
| December–February a | 30,839 | 0.5 ± 2.25 | <0.001 | a,c,d < b | 49.5 ± 24.3 | <0.001 | a < b < d < c | 50.0 ± 24.3 | <0.001 | a < b < d < c | |
| March–May b | 26,608 | 0.75 ± 2.75 | 52.5 ± 25.3 | 53.3 ± 25.3 | |||||||
| June–August c | 31,239 | 0.5 ± 2.5 | 57.0 ± 22.8 | 57.5 ± 22.8 | |||||||
| September–November d | 30,649 | 0.5 ± 2.5 | 56.3 ± 23.3 | 56.8 ± 23.5 | |||||||
| BMI, kg/m2 | |||||||||||
| <25 | 71,253 | 0.53 ± 2.65 | <0.001 | 55.5 ± 25.5 | <0.001 | 56.0 ± 25.5 | <0.001 | ||||
| ≥25 | 45,353 | 0.45 ± 2.33 | 51.3 ± 21.3 | 51.8 ± 21.3 | |||||||
| hs-CRP, mg/L | |||||||||||
| <1 | 107,790 | 0.5 ± 2.55 | 0.625 | 54.0 ± 23.8 | <0.001 | 54.5 ± 23.8 | <0.001 | ||||
| ≥1 | 2183 | 0.48 ± 2.5 | 51.8 ± 22.3 | 52.3 ± 22.3 | |||||||
| 25(OH)D2, nmol/L | 25(OH)D3, nmol/L | 25(OH)D, nmol/L | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2.5th | CI | 97.5th | CI | 2.5th | CI | 97.5th | CI | 2.5th | CI | 97.5th | CI | ||
| Total | <LOD NA | 5.0 | (4.8, 5.0) | 19.0 | (18.8, 19.0) | 109.8 | (109.3, 110.5) | 19.3 | (19.0, 19.3) | 110.3 | (109.5, 111.0) | ||
| Sex | |||||||||||||
| Male | <LOD NA | 4.3 | (4.0, 4.3) | 20.3 | (20.0, 20.5) | 99.5 | (98.8, 100.5) | 20.5 | (20.3, 20.8) | 100.0 | (99.0, 100.8) | ||
| Female | <LOD NA | 5.8 | (5.5, 6.0) | 17.8 | (17.8, 18) | 116.8 | (115.8, 118.0) | 18.0 | (18.0, 18.3) | 117.3 | (116.3, 118.5) | ||
| Age, years | |||||||||||||
| 20–29 | <LOD NA | 3.5 | (3.3, 4.5) | 14.3 | (13.5, 14.8) | 86.3 | (83.0, 92.3) | 14.5 | (13.8, 15.3) | 88.0 | (83.0, 91.3) | ||
| 30–39 | <LOD NA | 4.0 | (3.8, 4.3) | 16.3 | (16.0, 16.8) | 94.5 | (92.8, 97.3) | 16.5 | (16.3, 16.8) | 94.8 | (93.3, 97.5) | ||
| 40–49 | <LOD NA | 4.0 | (3.8, 4.3) | 18.0 | (17.8, 18.3) | 95.3 | (94.0, 96.5) | 18.0 | (17.8, 18.5) | 95.5 | (94.5, 96.8) | ||
| 50–59 | <LOD NA | 4.8 | (4.5, 4.8) | 19.8 | (19.5, 20.0) | 107.8 | (106.8, 109.3) | 20.0 | (19.8, 20.3) | 108.3 | (107.0, 109.8) | ||
| 60–69 | <LOD NA | 5.8 | (5.5, 6.0) | 20.5 | (20.3, 20.8) | 116.0 | (114.8, 117.3) | 20.8 | (20.5, 21.3) | 116.8 | (115.3, 117.8) | ||
| Over 70 | <LOD NA | 6.8 | (6.0, 7.8) | 19.0 | (18.3, 19.5) | 122.3 | (120.0, 125.3) | 19.5 | (19.0, 20.0) | 123.0 | (120.5, 126.0) | ||
| <25 nmol/L | 25–49.9 nmol/L | 50–74.9 nmol/L | ≥75 nmol/L | * p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | N | (%) | |||
| All subjects | 9014 | (7.6) | 47,598 | (39.9) | 42,255 | (35.4) | 20,468 | (17.2) | - | |
| Males (age, years) | ||||||||||
| 20–29 | 173 | (20.1) | 454 | (52.7) | 187 | (21.7) | 47 | (5.5) | <0.001 | |
| 30–39 | 569 | (11.1) | 2630 | (51.4) | 1526 | (29.8) | 396 | (7.7) | ||
| 40–49 | 917 | (7.4) | 6035 | (48.4) | 4349 | (34.9) | 1157 | (9.3) | ||
| 50–59 | 910 | (5.1) | 7685 | (43.4) | 6895 | (38.9) | 2233 | (12.6) | ||
| 60–69 | 749 | (4.3) | 6720 | (38.7) | 7127 | (41.1) | 2761 | (15.9) | ||
| Over 70 | 232 | (5.0) | 1688 | (36.5) | 1808 | (39.0) | 903 | (19.5) | ||
| Total | 3550 | (6.1) | 25,212 | (43.4) | 21,892 | (37.7) | 7497 | (12.9) | ||
| Females (age, years) | ||||||||||
| 20–29 | 258 | (23.0) | 602 | (53.8) | 201 | (18.0) | 59 | (5.3) | <0.001 | |
| 30–39 | 662 | (15.9) | 1929 | (46.3) | 1183 | (28.4) | 391 | (9.4) | ||
| 40–49 | 1312 | (13.5) | 4392 | (45.2) | 2876 | (29.6) | 1137 | (11.7) | ||
| 50–59 | 1581 | (7.8) | 7553 | (37.2) | 7017 | (34.5) | 4175 | (20.5) | ||
| 60–69 | 1250 | (6.2) | 6348 | (31.4) | 7141 | (35.4) | 5461 | (27.0) | ||
| Over 70 | 401 | (7.1) | 1562 | (27.6) | 1945 | (34.4) | 1748 | (30.9) | ||
| Total | 5464 | (8.9) | 22,386 | (36.6) | 20,363 | (33.3) | 12,971 | (21.2) | ||
| Unadjusted Model | Adjusted Model | ||||||
|---|---|---|---|---|---|---|---|
| Coeff. | (95% CI) | p-Value | Coeff. | (95% CI) | p-Value | ||
| Sex, ref: female | |||||||
| Male | −1.45 | (−1.6, −1.3) | <0.001 | −0.88 | (−1, −0.8) | <0.001 | |
| Age, year | 0.17 | (0.1, 0.2) | <0.001 | 0.17 | (0.1, 0.2) | <0.001 | |
| Month, ref: December–February | |||||||
| March–May | 1.22 | (1.1, 1.4) | <0.001 | 0.94 | (0.8, 1.1) | <0.001 | |
| June–August | 2.91 | (2.8, 3.1) | <0.001 | 2.96 | (2.8, 3.1) | <0.001 | |
| September–November | 2.66 | (2.5, 2.8) | <0.001 | 2.89 | (2.7, 3) | <0.001 | |
| BMI, ref: <25 kg/m2 | |||||||
| ≥25 kg/m2 | −1.68 | (−1.8, −1.6) | <0.001 | −1.42 | (−1.5, −1.3) | <0.001 | |
| hs-CRP, ref: <1 mg/L | |||||||
| ≥1 mg/L | −0.87 | (−1.3, −0.5) | <0.001 | −0.74 | (−1.1, −0.3) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Choi, Y.; Cho, S.; Park, H.; Kim, S.; Cho, H.-I.; Nah, E.-H. Vitamin D Status and Reference Intervals Measured by Liquid Chromatography–Tandem Mass Spectrometry for the Early Adulthood to Geriatric Ages in a South Korean Population during 2017–2022. Nutrients 2024, 16, 604. https://doi.org/10.3390/nu16050604
Park J, Choi Y, Cho S, Park H, Kim S, Cho H-I, Nah E-H. Vitamin D Status and Reference Intervals Measured by Liquid Chromatography–Tandem Mass Spectrometry for the Early Adulthood to Geriatric Ages in a South Korean Population during 2017–2022. Nutrients. 2024; 16(5):604. https://doi.org/10.3390/nu16050604
Chicago/Turabian StylePark, Jooheon, Yongjun Choi, Seon Cho, Hyeran Park, Suyoung Kim, Han-Ik Cho, and Eun-Hee Nah. 2024. "Vitamin D Status and Reference Intervals Measured by Liquid Chromatography–Tandem Mass Spectrometry for the Early Adulthood to Geriatric Ages in a South Korean Population during 2017–2022" Nutrients 16, no. 5: 604. https://doi.org/10.3390/nu16050604
APA StylePark, J., Choi, Y., Cho, S., Park, H., Kim, S., Cho, H.-I., & Nah, E.-H. (2024). Vitamin D Status and Reference Intervals Measured by Liquid Chromatography–Tandem Mass Spectrometry for the Early Adulthood to Geriatric Ages in a South Korean Population during 2017–2022. Nutrients, 16(5), 604. https://doi.org/10.3390/nu16050604