
Close Adherence to a Mediterranean Diet during Pregnancy Decreases Childhood Overweight/Obesity: A Prospective Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Dietary Assessment
2.3. Outcome
2.4. Other Maternal and Child Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef]
- Aranceta-Bartrina, J.; Gianzo-Citores, M.; Pérez-Rodrigo, C. Prevalencia de sobrepeso, obesidad y obesidad abdominal en población española entre 3 y 24 años. Estudio ENPE. Rev. Española Cardiol. 2020, 73, 290–299. [Google Scholar] [CrossRef]
- Sommer, A.; Twig, G. The Impact of Childhood and Adolescent Obesity on Cardiovascular Risk in Adulthood: A Systematic Review. Curr. Diab. Rep. 2018, 18, 91. [Google Scholar] [CrossRef]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef]
- Raab, R.; Michel, S.; Günther, J.; Hoffmann, J.; Stecher, L.; Hauner, H. Associations between lifestyle interventions during pregnancy and childhood weight and growth: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 8. [Google Scholar] [CrossRef]
- Nishtar, S.; Gluckman, P.; Armstrong, T. Ending childhood obesity: A time for action. Lancet 2016, 387, 825–827. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Guasch-Ferré, M.; Lee, C.H.; Estruch, R.; Clish, C.B.; Ros, E. Protective Effects of the Mediterranean Diet on Type 2 Diabetes and Metabolic Syndrome. J. Nutr. 2015, 146, 920S–927S. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Veronese, N.; Di Bella, G.; Cusumano, C.; Parisi, A.; Tagliaferri, F.; Ciriminna, S.; Barbagallo, M. Mediterranean diet in the management and prevention of obesity. Exp. Gerontol. 2023, 174, 112121. [Google Scholar] [CrossRef] [PubMed]
- Notario-Barandiaran, L.; Valera-Gran, D.; Gonzalez-Palacios, S.; Garcia-de-la-Hera, M.; Fernández-Barrés, S.; Pereda-Pereda, E.; Fernández-Somoano, A.; Guxens, M.; Iñiguez, C.; Romaguera, D.; et al. High adherence to a mediterranean diet at age 4 reduces overweight, obesity and abdominal obesity incidence in children at the age of 8. Int. J. Obes. 2020, 44, 1906–1917. [Google Scholar] [CrossRef]
- Kanellopoulou, A.; Giannakopoulou, S.P.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Kornilaki, E.N.; Konstantinou, E.; Lagiou, A.; Panagiotakos, D.B. The association between adherence to the Mediterranean diet and childhood obesity; the role of family structure: Results from an epidemiological study in 1728 Greek students. Nutr. Health 2021, 27, 39–47. [Google Scholar] [CrossRef]
- Zheng, X.; Wang, H.; Wu, H. Association between diet quality scores and risk of overweight and obesity in children and adolescents. BMC Pediatr. 2023, 23, 169. [Google Scholar] [CrossRef]
- Saunders, L.; Guldner, L.; Costet, N.; Kadhel, P.; Rouget, F.; Monfort, C.; Thomé, J.-P.; Multigner, L.; Cordier, S. Effect of a Mediterranean Diet during Pregnancy on Fetal Growth and Preterm Delivery: Results from a French Caribbean Mother–Child Cohort Study (TIMOUN). Paediatr. Perinat. Epidemiol. 2014, 28, 235–244. [Google Scholar] [CrossRef]
- Chatzi, L.; Mendez, M.; Garcia, R.; Roumeliotaki, T.; Ibarluzea, J.; Tardón, A.; Amiano, P.; Lertxundi, A.; Iñiguez, C.; Vioque, J.; et al. Mediterranean diet adherence during pregnancy and fetal growth: INMA (Spain) and RHEA (Greece) mother–child cohort studies. Br. J. Nutr. 2012, 107, 135–145. [Google Scholar] [CrossRef]
- Díaz-López, A.; Díaz-Torres, S.; Martín-Luján, F.; Basora, J.; Arija, V. Prenatal adherence to the Mediterranean diet decreases the risk of having a small-for-gestational-age baby, ECLIPSES study. Sci. Rep. 2022, 12, 13794. [Google Scholar] [CrossRef]
- Gesteiro, E.; Rodríguez Bernal, B.; Bastida, S.; Sánchez-Muniz, F.J. Maternal diets with low healthy eating index or Mediterranean diet adherence scores are associated with high cord-blood insulin levels and insulin resistance markers at birth. Eur. J. Clin. Nutr. 2012, 66, 1008–1015. [Google Scholar] [CrossRef]
- Chatzi, L.; Rifas-Shiman, S.L.; Georgiou, V.; Joung, K.E.; Koinaki, S.; Chalkiadaki, G.; Margioris, A.; Sarri, K.; Vassilaki, M.; Vafeiadi, M.; et al. Adherence to the Mediterranean diet during pregnancy and offspring adiposity and cardiometabolic traits in childhood. Pediatr. Obes. 2017, 12 (Suppl. S1), 47–56. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Barrés, S.; Romaguera, D.; Valvi, D.; Martínez, D.; Vioque, J.; Navarrete-Muñoz, E.M.; Amiano, P.; Gonzalez-Palacios, S.; Guxens, M.; Pereda, E.; et al. Mediterranean dietary pattern in pregnant women and offspring risk of overweight and abdominal obesity in early childhood: The INMA birth cohort study. Pediatr. Obes. 2016, 11, 491–499. [Google Scholar] [CrossRef]
- Fernández-Barrés, S.; Vrijheid, M.; Manzano-Salgado, C.B.; Valvi, D.; Martínez, D.; Iñiguez, C.; Jimenez-Zabala, A.; Riaño-Galán, I.; Navarrete-Muñoz, E.M.; Santa-Marina, L.; et al. The Association of Mediterranean Diet during Pregnancy with Longitudinal Body Mass Index Trajectories and Cardiometabolic Risk in Early Childhood. J. Pediatr. 2019, 206, 119–127.e6. [Google Scholar] [CrossRef]
- Monthé-Drèze, C.; Rifas-Shiman, S.L.; Aris, I.M.; Shivappa, N.; Hebert, J.R.; Sen, S.; Oken, E. Maternal diet in pregnancy is associated with differences in child body mass index trajectories from birth to adolescence. Am. J. Clin. Nutr. 2021, 113, 895. [Google Scholar] [CrossRef]
- Gonzalez-Nahm, S.; Marchesoni, J.; Maity, A.; Maguire, R.L.; House, J.S.; Tucker, R.; Atkinson, T.; Murphy, S.K.; Hoyo, C. Maternal Mediterranean Diet Adherence and Its Associations with Maternal Prenatal Stressors and Child Growth. Curr. Dev. Nutr. 2022, 6, nzac146. [Google Scholar] [CrossRef]
- Strohmaier, S.; Bogl, L.H.; Eliassen, A.H.; Massa, J.; Field, A.E.; Chavarro, J.E.; Ding, M.; Tamimi, R.M.; Schernhammer, E. Maternal healthful dietary patterns during peripregnancy and long-term overweight risk in their offspring. Eur. J. Epidemiol. 2020, 35, 283. [Google Scholar] [CrossRef]
- Arija, V.; Fargas, F.; March, G.; Abajo, S.; Basora, J.; Canals, J.; Ribot, B.; Aparicio, E.; Serrat, N.; Hernández-Martínez, C.; et al. Adapting iron dose supplementation in pregnancy for greater effectiveness on mother and child health: Protocol of the ECLIPSES randomized clinical trial. BMC Pregnancy Childbirth 2014, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Trinidad Rodríguez, I.; Fernández Ballart, J.; Cucó Pastor, G.; Biarnés Jordà, E.; Arija Val, V. Validation of a short questionnaire on frequency of dietary intake: Reproducibility and validity. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar]
- Favier, J.C.; Ireland-Ripert, J.; Toque, C.; Feinberg, M. Répertoire Général des Aliments: Tables de Composition; Technique & Documentation; INRA: Paris, France, 1995; p. 897. [Google Scholar]
- Jardí, C.; Aparicio, E.; Bedmar, C.; Aranda, N.; Abajo, S.; March, G.; Basora, J.; Arija, V.; the ECLIPSES Study Group. Food Consumption during Pregnancy and Post-Partum. ECLIPSES Study. Nutrients 2019, 11, 2447. [Google Scholar] [CrossRef]
- Who Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. S4), S164–S192. [Google Scholar] [CrossRef]
- Institut d’Estadística de Catalunya. Classificació Catalana D’Ocupacions 2011 (CCO-2011); Institut d’Estadística de Catalunya: Catalunya, Spain, 2011; Available online: http://idescat.cat/p/cco2011 (accessed on 2 August 2023).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Dabatase on Body Mass Index; World Health Organization: Geneva, Switzerland, 2006; Available online: https://scholar.google.com/scholar_lookup?title=Global+Dabatase+on+Body+Mass+Index&publication_year=2006& (accessed on 10 August 2023).
- Rasmussen, K.M.; Yaktine, A.L.; Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines (Eds.) Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Garrido-Migue, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of Overweight and Obesity among European Preschool Children: A Systematic Review and Meta-Regression by Food Group Consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef]
- Martíncrespo-Blanco, M.C.; Varillas-Delgado, D.; Blanco-Abril, S.; Cid-Exposito, M.G.; Robledo-Martín, J. Effectiveness of an Intervention Programme on Adherence to the Mediterranean Diet in a Preschool Child: A Randomised Controlled Trial. Nutrients 2022, 14, 1536. [Google Scholar] [CrossRef]
- Cadenas-Sanchez, C.; Intemann, T.; Labayen, I.; Artero, E.G.; Alvarez-Bueno, C.; Sanchis-Moysi, J.; Benito, P.J.; Beltran-Valls, M.R.; Pérez-Bey, A.; Sanchez-Delgado, G.; et al. Prevalence of severe/morbid obesity and other weight status and anthropometric reference standards in Spanish preschool children: The PREFIT project. Pediatr. Res. 2020, 87, 501–510. [Google Scholar] [CrossRef]
- Parlee, S.D.; MacDougald, O.A. Maternal nutrition and risk of obesity in offspring: The Trojan horse of developmental plasticity. Biochim. Biophys. Acta 2014, 1842, 495–506. [Google Scholar] [CrossRef]
- Amati, F.; Hassounah, S.; Swaka, A. The Impact of Mediterranean Dietary Patterns during Pregnancy on Maternal and Offspring Health. Nutrients 2019, 11, 1098. [Google Scholar] [CrossRef]
- Biagi, C.; Di Nunzio, M.; Bordoni, A.; Gori, D.; Lanari, M. Effect of Adherence to Mediterranean Diet during Pregnancy on Children’s Health: A Systematic Review. Nutrients 2019, 11, 997. [Google Scholar] [CrossRef]
- Zhang, Y.; Xia, M.; Weng, S.; Wang, C.; Yuan, P.; Tang, S. Effect of Mediterranean diet for pregnant women: A meta-analysis of randomized controlled trials. J. Matern. Fetal Neonatal Med. 2022, 35, 4824–4829. [Google Scholar] [CrossRef]
- Perkins, J.; Re, T.; Ong, S.; Niu, Z.; Wen, X. Meta-Analysis on Associations of Timing of Maternal Smoking Cessation before and during Pregnancy with Childhood Overweight and Obesity. Nicotine Tob. Res. 2023, 25, 605–615. [Google Scholar] [CrossRef]
- Ruiz, M.; Goldblatt, P.; Morrison, J.; Porta, D.; Forastiere, F.; Hryhorczuk, D.; Antipkin, Y.; Saurel-Cubizolles, M.J.; Lioret, S.; Vrijheid, M.; et al. Impact of Low Maternal Education on Early Childhood Overweight and Obesity in Europe. Paediatr. Perinat. Epidemiol. 2016, 30, 274–284. [Google Scholar] [CrossRef]
- Giles, L.C.; Whitrow, M.J.; Davies, M.J.; Davies, C.E.; Rumbold, A.R.; Moore, V.M. Growth trajectories in early childhood, their relationship with antenatal and postnatal factors, and development of obesity by age 9 years: Results from an Australian birth cohort study. Int. J. Obes. 2015, 39, 1049–1056. [Google Scholar] [CrossRef]
- Sharp, G.C.; Lawlor, D.A.; Richmond, R.C.; Fraser, A.; Simpkin, A.; Suderman, M.; Shihab, H.A.; Lyttleton, O.; McArdle, W.; Ring, S.M.; et al. Maternal pre-pregnancy BMI and gestational weight gain, offspring DNA methylation and later offspring adiposity: Findings from the Avon Longitudinal Study of Parents and Children. Int. J. Epidemiol. 2015, 44, 1288–1304. [Google Scholar] [CrossRef]
- Wang, T.; Heianza, Y.; Sun, D.; Huang, T.; Ma, W.; Rimm, E.B.; Manson, J.E.; Hu, F.B.; Willett, W.C.; Qi, L. Improving adherence to healthy dietary patterns, genetic risk, and long term weight gain: Gene-diet interaction analysis in two prospective cohort studies. Br. Med. J. 2018, 360, j5644. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Aubert, A.M.; Shivappa, N.; Bernard, J.Y.; Mensink-Bout, S.M.; Geraghty, A.A.; Mehegan, J.; Suderman, M.; Polanska, K.; Hanke, W.; et al. Maternal dietary quality, inflammatory potential and childhood adiposity: An individual participant data pooled analysis of seven European cohorts in the ALPHABET consortium. BMC Med. 2021, 19, 33. [Google Scholar] [CrossRef] [PubMed]
- Tahir, M.J.; Haapala, J.L.; Foster, L.P.; Duncan, K.M.; Teague, A.M.; Kharbanda, E.O.; McGovern, P.M.; Whitaker, K.M.; Rasmussen, K.M.; Fields, D.A.; et al. Higher Maternal Diet Quality during Pregnancy and Lactation Is Associated with Lower Infant Weight-for-Length, Body Fat Percent, and Fat Mass in Early Postnatal Life. Nutrients 2019, 11, 632. [Google Scholar] [CrossRef]
- Mathias, P.C.F.; Elmhiri, G.; De Oliveira, J.C.; Delayre-Orthez, C.; Barella, L.F.; Tófolo, L.P.; Fabricio, G.S.; Chango, A.; Abdennebi-Najar, L. Maternal diet, bioactive molecules, and exercising as reprogramming tools of metabolic programming. Eur. J. Nutr. 2014, 53, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Tounian, P. Programming towards childhood obesity. Ann. Nutr. Metab. 2011, 58 (Suppl. S2), 30–41. [Google Scholar] [CrossRef]
- Li, Y. Epigenetic mechanisms link maternal diets and gut microbiome to obesity in the offspring. Front. Genet. 2018, 9, 342. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zeng, Y.; Zhang, Q.; Xiao, X. The Role of Maternal Vitamin D Deficiency in Offspring Obesity: A Narrative Review. Nutrients 2023, 15, 533. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Yoon, B.-E.; Park, J.; Kwon, E.H.; Kim, K.; Lee, S.; Kim, J.; Yoon, B.-E.; Park, J.; Kwon, E.H.; et al. The Association between Maternal Folate Status and Childhood Obesity-Systematic Review and Meta-Analysis. Exerc. Sci. 2022, 31, 159–167. [Google Scholar] [CrossRef]
- Harmancıoğlu, B.; Kabaran, S. Maternal high fat diets: Impacts on offspring obesity and epigenetic hypothalamic programming. Front. Genet. 2023, 14, 1158089. [Google Scholar] [CrossRef]


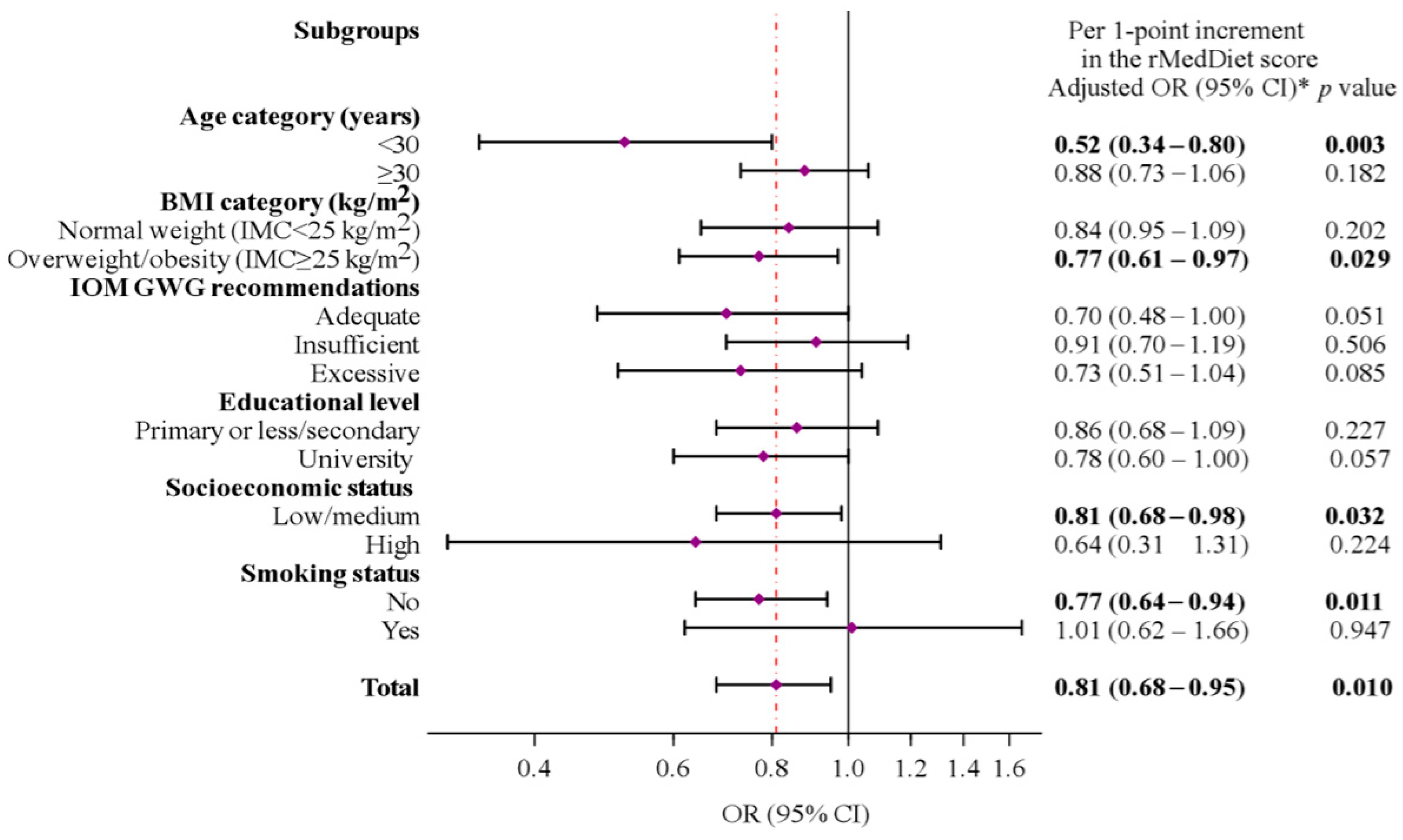

{kind=link}
{kind=link}
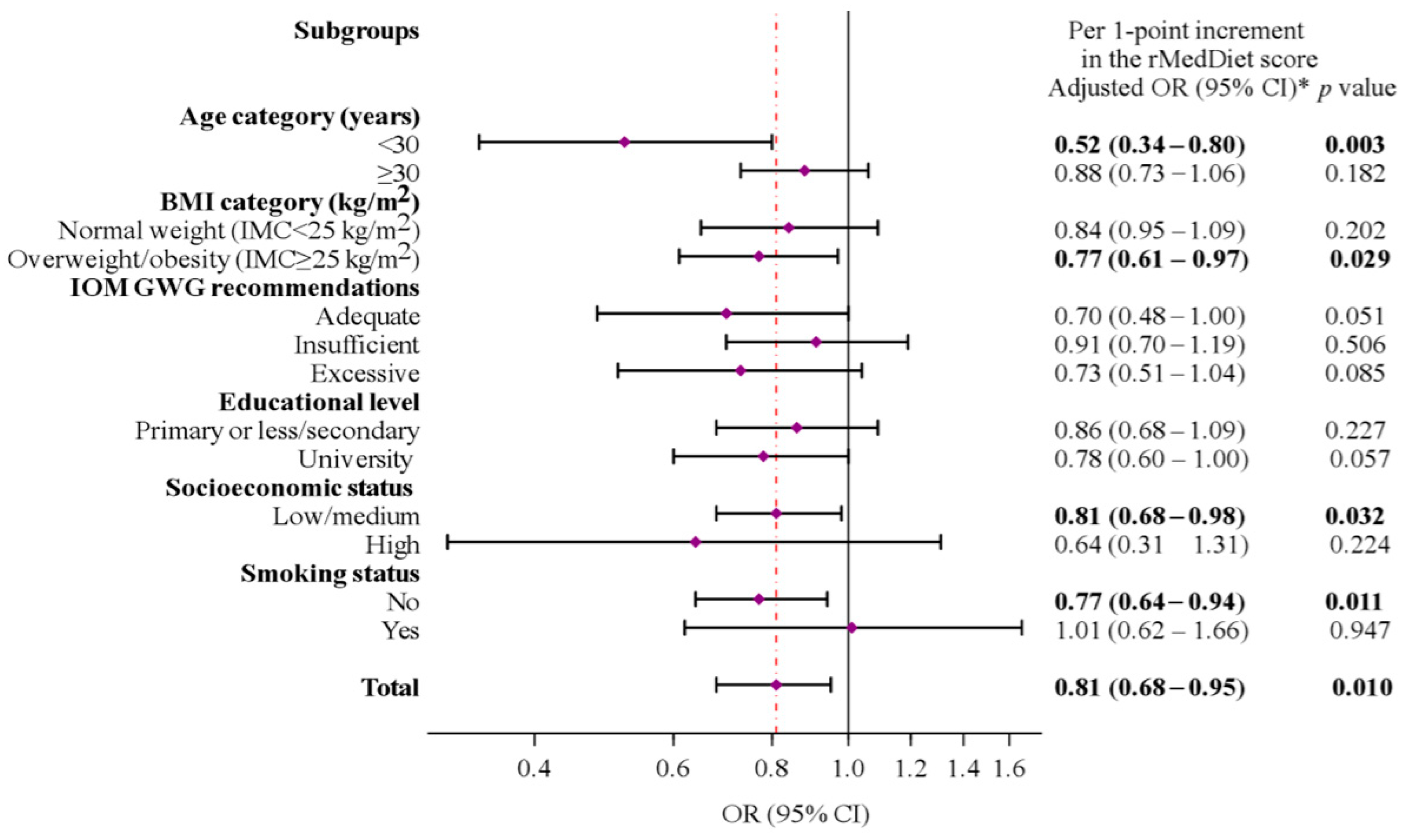{kind=link}
| Characteristics | Total | Normal Weight | Overweight/Obese | p-Value | |
|---|---|---|---|---|---|
| (n = 272) | (n = 202; 74.3%) | (n = 70; 25.7%) | |||
| Maternal characteristics | |||||
| Age (years), mean ± SD | 31.6 ± 4.6 | 31.9 ± 4.3 | 30.9 ± 5.3 | 0.129 | |
| Age category (years), n (%) | |||||
| <25 | 21 (8) | 11 (5) | 10 (14) | ||
| 25–<30 | 61 (22) | 44 (22) | 17 (24) | 0.041 | |
| ≥30 | 190 (70) | 147 (73) | 43 (61) | ||
| BMI initial (kg/m2), mean ± SD | 25.1 ± 4.4 | 24.3 ± 3.9 | 27.3 ± 5.0 | <0.001 | |
| BMI category (kg/m2), n (%) | |||||
| Normal weight (18.5–<25) | 158 (58) | 132 (65) | 26 (37) | ||
| Overweight (25.0–<30) | 76 (28) | 50 (25) | 26 (37) | <0.001 | |
| Obesity (≥30) | 38 (14) | 20 (10) | 18 (26) | ||
| GWG (kg), mean ± SD | 10.3 ± 3.6 | 10.1 ± 3.4 | 10.5 ± 3.9 | 0.513 | |
| IOM GWG recommendations, n (%) † | |||||
| Adequate | 106 (39) | 81 (40) | 25 (36) | ||
| Insufficient | 112 (41) | 93 (46) | 19 (27) | <0.001 | |
| Excessive | 54 (20) | 28 (14) | 26 (37) | ||
| Educational level, n (%) | |||||
| Low (primary school or less)/ medium (secondary studies) | 153 (56) | 106 (52) | 47 (67) | 0.033 | |
| High (university or more) | 119 (44) | 96 (48) | 23 (32) | ||
| Familiar SES, n (%) | |||||
| Low/medium | 212 (79) | 151 (75) | 61 (87) | 0.030 | |
| High | 60 (22) | 51 (25) | 9 (13) | ||
| Smoking status, n (%) | 226 (83) | 174 (86) | 52 (74) | 0.023 | |
| Alcohol consumption in pregnancy, n (%) | 20 (8) | 12 (7) | 8 (13) | 0.111 | |
| Physical activity (METs/min/week) in pregnancy, mean ± SD | 447 ± 664 | 451 ± 683 | 436 ± 610 | 0.868 | |
| rMedDiet during pregnancy (points), mean ± SD * | 9.8 ± 2.3 | 10.0 ± 2.3 | 9.2 ± 2.1 | 0.028 | |
| Delivery mode, n (%) | |||||
| Vaginal delivery | 216 (79) | 163 (81) | 53 (76) | 0.375 | |
| Cesarean (any) | 56 (21) | 39 (19) | 17 (24) | ||
| Child characteristics | |||||
| Sex, female, n (%) | 134 (49) | 108 (53) | 26 (37) | 0.019 | |
| GA at delivery (weeks), mean ± SD | 39.7 ± 1.6 | 39.7 ± 1.5 | 39.6 ± 1.6 | 0.621 | |
| Age at 4-year visit (years), mean ± SD | 4.4 ± 0.4 | 4.4 ± 0.3 | 4.4 ± 0.4 | 0.711 | |
| Birth weight (g), mean ± SD | 3257 ± 466 | 3236 ± 440 | 3317 ± 535 | 0.217 | |
| Weight at 4-year visit (kg), mean ± SD | 18.1 ± 3.2 | 16.9 ± 1.9 | 21.4 ± 3.9 | <0.001 | |
| Height at 4-year visit (cm), mean ± SD | 105.8 ± 5.4 | 105.4 ± 5.6 | 107.0 ± 5.1 | 0.028 | |
| BMI at 4-year visit (kg/m2), mean ± SD | 16.0 ± 2.1 | 15.2 ± 1.0 | 18.6 ± 2.4 | <0.001 | |
| BMI z-score at 4-year visit, mean ± SD | 0.44 ± 1.36 | −0.11 ± 0.81 | 2.08 ± 1.29 | <0.001 | |
| rMedDiet Adherence Score (Point) | N Total/ Cases (%) | Univariable Model | p-Value | Multivariable Model | p-Value | |
|---|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | |||||
| Continuous (per 1-point increase) | 252/62 (24.6) | 0.86 (0.75–0.98) | 0.030 | 0.81 (0.68–0.95) | 0.010 | |
| Quartiles of adherence to the rMedDiet | ||||||
| Q1 (≤8 points) | 73/22 (30.1) | 1 (ref.) | 1 (ref.) | |||
| Q2 (9–10 points) | 91/23 (25.3) | 0.78 (0.39–1.56) | 0.488 | 0.76 (0.34–1.69) | 0.501 | |
| Q3 (11 points) | 31/7 (22.6) | 0.67 (0.25–1.80) | 0.433 | 0.53 (0.17–1.65) | 0.279 | |
| Q4 (≥12 points) | 57/10 (17.5) | 0.49 (0.21–1.15) | 0.102 | 0.34 (0.12–0.90) | 0.038 | |
| p for trend | 0.098 | 0.037 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díaz-López, A.; Rodríguez Espelt, L.; Abajo, S.; Arija, V. Close Adherence to a Mediterranean Diet during Pregnancy Decreases Childhood Overweight/Obesity: A Prospective Study. Nutrients 2024, 16, 532. https://doi.org/10.3390/nu16040532
Díaz-López A, Rodríguez Espelt L, Abajo S, Arija V. Close Adherence to a Mediterranean Diet during Pregnancy Decreases Childhood Overweight/Obesity: A Prospective Study. Nutrients. 2024; 16(4):532. https://doi.org/10.3390/nu16040532
Chicago/Turabian StyleDíaz-López, Andrés, Laura Rodríguez Espelt, Susana Abajo, and Victoria Arija. 2024. "Close Adherence to a Mediterranean Diet during Pregnancy Decreases Childhood Overweight/Obesity: A Prospective Study" Nutrients 16, no. 4: 532. https://doi.org/10.3390/nu16040532
APA StyleDíaz-López, A., Rodríguez Espelt, L., Abajo, S., & Arija, V. (2024). Close Adherence to a Mediterranean Diet during Pregnancy Decreases Childhood Overweight/Obesity: A Prospective Study. Nutrients, 16(4), 532. https://doi.org/10.3390/nu16040532