
Elevated Inflammation and Poor Diet Quality Associated with Lower eGFR in United States Adults: An NHANES 2015–2018 Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Dietary Assessment
2.4. Data Analysis Plan
3. Results
3.1. Descriptive Statistics of Population
3.2. Multiple Linear Regression Analysis: Interaction Effect of DQ and hs-CRP on eGFR
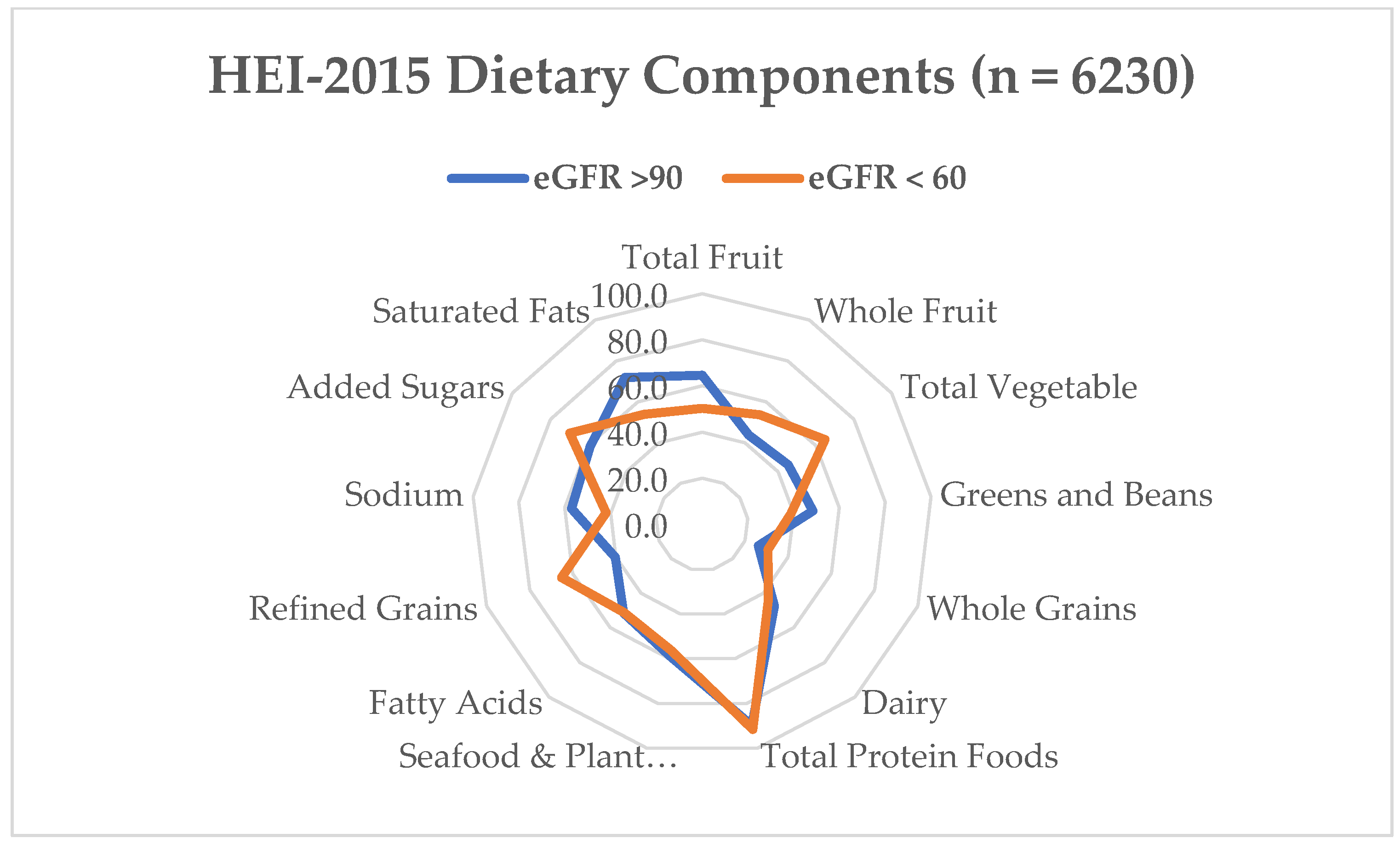
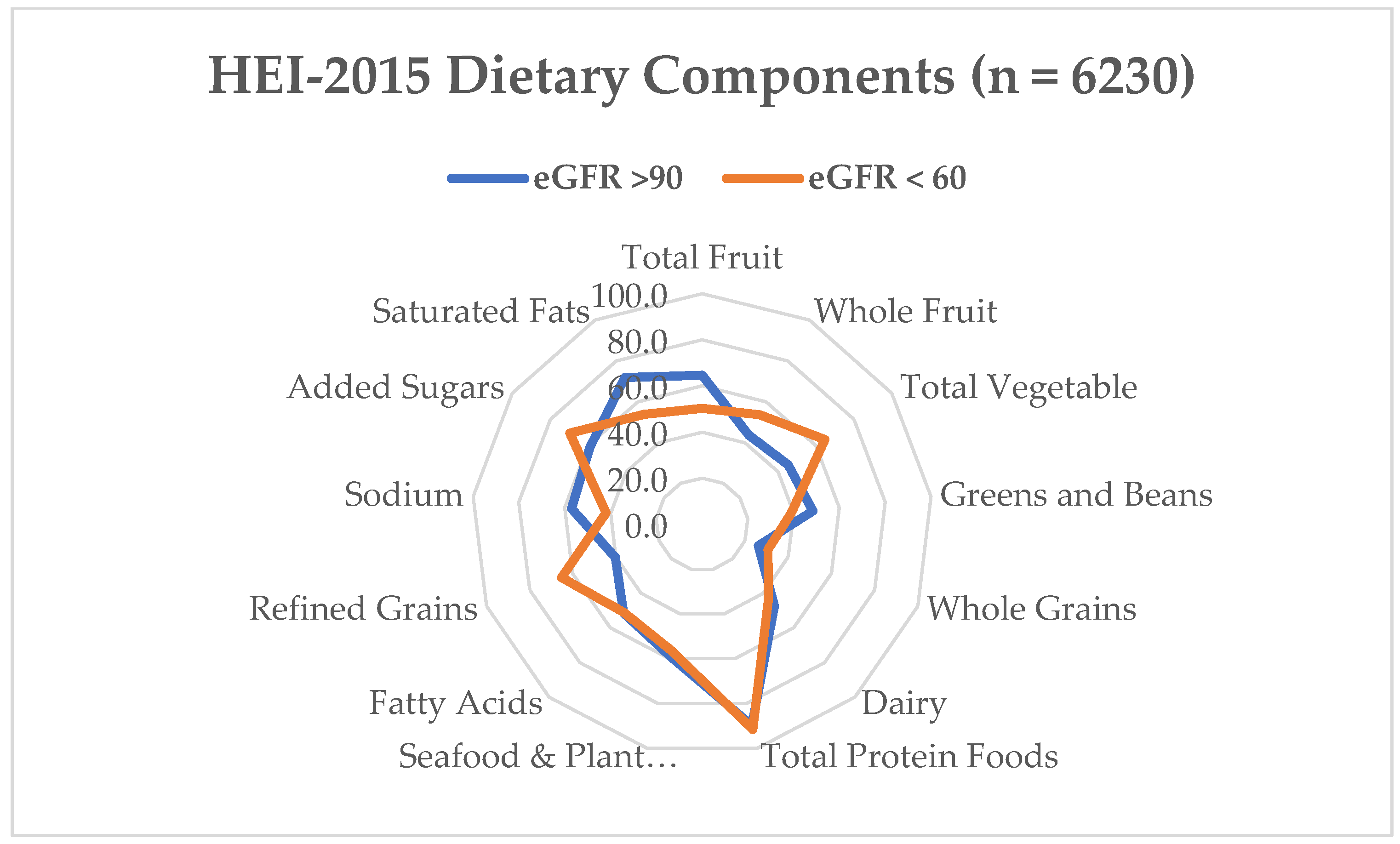
3.3. Multiple Linear Regression Analysis: Relationship between Dietary Components and eGFR
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control. Chronic Kidney Disease in the United States, 2023; Centers for Disease Control and Prevention: Washington, DC, USA, 2023. [Google Scholar]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Mihai, S.; Codrici, E.; Popescu, I.D.; Enciu, A.M.; Albulescu, L.; Necula, L.G.; Mambet, C.; Anton, G.; Tanase, C. Inflammation-Related Mechanisms in Chronic Kidney Disease Prediction, Progression, and Outcome. J. Immunol. Res. 2018, 2018, 2180373. [Google Scholar] [CrossRef]
- Del Guidice, M.; Gangestad, S.W. Rethinking IL-6 and CRP: Why They Are More than Inflammatory Biomarkers, and Why It Matters. Brain. Behav. Immun. 2018, 70, 61–75. [Google Scholar] [CrossRef]
- ZoCCali, C.; Vanholder, R.; Massy, Z.A.; Ortiz, A.; Sarafidis, P.; Dekker, F.W.; Fliser, D.; Fouque, D.; Heine, G.; Jager, K.; et al. The Systemic Nature of CKD. Nat. Rev. Nephrol. 2017, 13, 344–358. [Google Scholar] [CrossRef]
- Rose-John, S. Interleukin-6 Family Cytokines. Cold Spring Harb. Perspect. Biol. 2018, 10, a028415. [Google Scholar] [CrossRef]
- Eckschlager, C.; Schwenoha, K.; Roth, C.; Bogner, B.; Oostingh, G.J. Comparative Analysis of High CRP-Levels in Human Blood Using Point-of-Care and Laboratory-Based Methods. Pract. Lab. Med. 2019, 17, e00137. [Google Scholar] [CrossRef] [PubMed]
- Ajjarapu, A.S.; Hinkle, S.N.; Li, M.; Francis, E.C.; Zhang, C. Dietary Patterns and Renal Health Outcomes in Thegeneral Population: A Review Focusing on Prospective Studies. Nutrients 2019, 11, 1877. [Google Scholar] [CrossRef] [PubMed]
- Marks, K.J.; Hartman, T.J.; Judd, S.E.; Ilori, T.O.; Cheung, K.L.; Warnock, D.G.; Gutiérrez, O.M.; Goodman, M.; Cushman, M.; McClellan, W.M. Dietary Oxidative Balance Scores and Biomarkers of Inflammation among Individuals with and without Chronic Kidney Disease. Nephron Extra 2018, 8, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; D’Alessandro, C.; Gesualdo, L.; Cosola, C.; Gallieni, M.; Egidi, M.F.; Fusaro, M. Non-Traditional Aspects of Renal Diets: Focus on Fiber, Alkali and Vitamin K1 Intake. Nutrients 2017, 9, 444. [Google Scholar] [CrossRef] [PubMed]
- Cigarrán Guldris, S.; Latorre Catalá, J.A.; Sanjurjo Amado, A.; Menéndez Granados, N.; Piñeiro Varela, E. Fibre Intake in Chronic Kidney Disease: What Fibre Should We Recommend? Nutrients 2022, 14, 4419. [Google Scholar] [CrossRef] [PubMed]
- Müller, R.-U.; Greenwood, S.A.; Castle, E.M.; Simopoulos, A.P. Dietary Changes and Their Influence in the Development of Kidney Disease. Kidney Dial. 2022, 2, 131–137. [Google Scholar] [CrossRef]
- Hariharan, D.; Vellanki, K.; Kramer, H. The Western Diet and Chronic Kidney Disease. Curr. Hypertens. Rep. 2015, 17, 16. [Google Scholar] [CrossRef] [PubMed]
- Kramer, H. Diet and Chronic Kidney Disease. Adv. Nutr. 2019, 10, S367–S379. [Google Scholar] [CrossRef] [PubMed]
- Bin Zarah, A.; Feraudo, M.C.; Andrade, J.M. Development and Relative Validity of the Chronic Kidney Disease Short Food Frequency Questionnaire (Ckd Sffq) to Determine Diet Quality and Dietary Habits among Adults with Chronic Kidney Disease. Nutrients 2021, 13, 3610. [Google Scholar] [CrossRef]
- Alkerwi, A. Diet Quality Concept. Nutrition 2014, 30, 613–618. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.R.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Endre, Z.H.; Walker, R.J. Biomarkers of Cardiovascular Risk in Chronic Kidney Disease. Biomark. Kidney Dis. 2017, 485–511. [Google Scholar] [CrossRef]
- Zhubi-Bakija, F.; Bajraktari, G.; Bytyçi, I.; Mikhailidis, D.P.; Henein, M.Y.; Latkovskis, G.; Rexhaj, Z.; Zhubi, E.; Banach, M.; Alnouri, F.; et al. The Impact of Type of Dietary Protein, Animal versus Vegetable, in Modifying Cardiometabolic Risk Factors: A Position Paper from the International Lipid Expert Panel (ILEP). Clin. Nutr. 2021, 40, 255–276. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- National Cancer Institute. Developing the Healthy Eating Index. Available online: https://epi.grants.cancer.gov/hei/developing.html (accessed on 17 October 2019).
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.R.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S. The Automated Self-Administered 24-Hour Dietary Recall (ASA24): A Resource for Researchers, Clinicians and Educators from the National Cancer Institute. J. Dev. Behav. Pediatr. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control. NHANES Tutorials. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx (accessed on 15 October 2023).
- SAS: Analytics, Artificial Intelligence and Data Management. 2013. Available online: https://www.sas.com/en_us/software/viya.html?utm_source=other&utm_medium=cpm&utm_campaign=non-cbo-us&dclid=&gclid=Cj0KCQiAw6yuBhDrARIsACf94RUPO0NKQ9EGpHVCPPSTu_V3hk3BCseHhuGRPuMW-MfuYYhcSlte0zgaAuSJEALw_wcB (accessed on 15 October 2023).
- National Cancer Institute. Visualizing and Interpreting Healthy Eating Index Scores. Available online: https://epi.grants.cancer.gov/hei/interpret-visualize-hei-scores.html (accessed on 12 May 2023).
- Yan, L.J.; Zhang, F.R.; Ma, C.S.; Zheng, Y. Higher Dietary Inflammatory Index Is Associated with Increased All-Cause Mortality in Adults with Chronic Kidney Disease. Front. Nutr. 2022, 9, 883838. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, V.M.R.; Wei, G.; Baird, B.C.; Murtaugh, M.; Chonchol, M.B.; Raphael, K.L.; Greene, T.; Beddhu, S. High Dietary Fiber Intake Is Associated with Decreased Inflammation and All-Cause Mortality in Patients with Chronic Kidney Disease. Kidney Int. 2012, 81, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Calle, M.C.; Andersen, C.J. Assessment of Dietary Patterns Represents a Potential, yet Variable, Measure of Inflammatory Status: A Review and Update. Dis. Markers 2019, 2019, 3102870. [Google Scholar] [PubMed]
- Gill, P.A.; Inniss, S.; Kumagai, T.; Rahman, F.Z.; Smith, A.M. The Role of Diet and Gut Microbiota in Regulating Gastrointestinal and Inflammatory Disease. Front. Immunol. 2022, 13, 866059. [Google Scholar] [CrossRef] [PubMed]
- Hart, M.J.; Torres, S.J.; McNaughton, S.A.; Milte, C.M. Dietary Patterns and Associations with Biomarkers of Inflammation in Adults: A Systematic Review of Observational Studies. Nutr. J. 2021, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Siener, R. Dietary Treatment of Metabolic Acidosis in Chronic Kidney Disease. Nutrients 2018, 10, 512. [Google Scholar] [CrossRef]
- Storz, M.A.; Ronco, A.L.; Hannibal, L. Observational and Clinical Evidence That Plant-Based Nutrition Reduces Dietary Acid Load. J. Nutr. Sci. 2022, 11, e93. [Google Scholar] [CrossRef]
- Mendivil, C.O. Dietary Fish, Fish Nutrients, and Immune Function: A Review. Front. Nutr. 2021, 7, 617652. [Google Scholar] [CrossRef]
- Dispensa, A.; Andrade, J.M. The Relationship Between Protein Types and Hs-CRP on EGFR. UF J. Undergrad. Res. 2023, 25. [Google Scholar] [CrossRef]
- Millar, S.R.; Navarro, P.; Harrington, J.M.; Perry, I.J.; Phillips, C.M. Dietary Quality Determined by the Healthy Eating Index-2015 and Biomarkers of Chronic Low-Grade Inflammation: A Cross-Sectional Analysis in Middle-to-Older Aged Adults. Nutrients 2021, 13, 222. [Google Scholar] [CrossRef]
- Xu, H.; Sjögren, P.; Ärnlöv, J.; Banerjee, T.; Cederholm, T.; Risérus, U.; Lindholm, B.; Lind, L.; Carrero, J.J. A Proinflammatory Diet Is Associated with Systemic Inflammation and Reduced Kidney Function in Elderly Adults. J. Nutr. 2015, 145, 729–735. [Google Scholar] [CrossRef]
- Banerjee, T.; Crews, D.C.; Wesson, D.E.; Tilea, A.M.; Saran, R.; Ríos-Burrows, N.; Williams, D.E.; Powe, N.R.; Hsu, C.Y.; Bibbins-Domingo, K.; et al. High Dietary Acid Load Predicts ESRD among Adults with CKD. J. Am. Soc. Nephrol. 2015, 26, 1693–1700. [Google Scholar] [CrossRef]
- Adeva-Andany, M.M.; Fernández-Fernández, C.; Carneiro-Freire, N.; Vila-Altesor, M.; Ameneiros-Rodríguez, E. The Differential Effect of Animal versus Vegetable Dietary Protein on the Clinical Manifestations of Diabetic Kidney Disease in Humans. Clin. Nutr. ESPEN 2022, 48, 21–35. [Google Scholar] [CrossRef]
- Ranganathan, N.; Anteyi, E. The Role of Dietary Fiber and Gut Microbiome Modulation in Progression of Chronic Kidney Disease. Toxins 2022, 14, 183. [Google Scholar] [CrossRef] [PubMed]
- Hertzler, S.R.; Lieblein-Boff, J.C.; Weiler, M.; Allgeier, C. Plant Proteins: Assessing Their Nutritional Quality and Effects on Health and Physical Function. Nutrients 2020, 12, 3704. [Google Scholar] [CrossRef]
- Gopinath, B.; Harris, D.; Flood, V.; Burkutsky, G.; Mitchell, P. A Better Diet Quality Is Associated with a Reduced Likelihood of CKD in Older Adults. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 937–943. [Google Scholar] [CrossRef]
- Mazidi, M.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Kengne, A.P. Greater Dietary Inflammatory Index Score Is Associated with Higher Likelihood of Chronic Kidney Disease. Br. J. Nutr. 2018, 120, 204–209. [Google Scholar] [CrossRef]
- Karalius, V.P.; Shoham, D.A. Dietary Sugar and Artificial Sweetener Intake and Chronic Kidney Disease: A Review. Adv. Chronic Kidney Dis. 2013, 20, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Kretowicz, M.; Johnson, R.J.; Ishimoto, T.; Nakagawa, T.; Manitius, J. The Impact of Fructose on Renal Function and Blood Pressure. Int. J. Nephrol. 2011, 2011, 315879. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ge, X.; Li, X.; He, J.; Wei, X.; Du, J.; Sun, J.; Li, X.; Xun, Z.; Liu, W.; et al. High-Fat Diet Promotes Renal Injury by Inducing Oxidative Stress and Mitochondrial Dysfunction. Cell Death Dis. 2020, 11, 914. [Google Scholar] [CrossRef] [PubMed]
- Imig, J.D.; Ryan, M.J. Immune and Inflammatory Role in Renal Disease. Compr. Physiol. 2013, 3, 957–976. [Google Scholar] [CrossRef] [PubMed]
- Stehouwer, C.D.A.; Gall, M.-A.; Twisk, J.W.; Knudsen, E.; Emeis, J.J.; Parving, H.-H. Increased Urinary Albumin Excretion, Endothelial Dysfunction, and Chronic Low-Grade Inflammation in Type 2 Diabetes Progressive, Interrelated, and Independently Associated With Risk of Death. Diabetes 2002, 51, 1157–1165. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.K.; Shaheen, M.; Rajavashisth, T.B.; Pan, D.; Norris, K.C.; Nicholas, S.B. Association of Race/Ethnicity, Inflammation, and Albuminuria in Patients with Diabetes and Early Chronic Kidney Disease. Diabetes Care 2014, 37, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Nerpin, E.; Helmersson-Karlqvist, J.; Risérus, U.; Sundström, J.; Larsson, A.; Jobs, E.; Basu, S.; Ingelsson, E.; Ärnlöv, J. Inflammation, Oxidative Stress, Glomerular Filtration Rate, and Albuminuria in Elderly Men: A Cross-Sectional Study. BMC Res. Notes 2012, 5, 537. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.; Mitra, N.; Kanetsky, P.A.; Devaney, J.; Wing, M.R.; Reilly, M.; Shah, V.O.; Balakrishnan, V.S.; Guzman, N.J.; Girndt, M.; et al. Association between Albuminuria, Kidney Function, and Inflammatory Biomarker Profile in CKD in CRIC. Clin. J. Am. Soc. Nephrol. 2012, 7, 1938–1946. [Google Scholar] [CrossRef] [PubMed]
- Ku, E.; Lee, B.J.; Wei, J.; Weir, M.R. Hypertension in CKD: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 74, 120–131. [Google Scholar] [CrossRef]
- Eriksen, B.O.; Stefansson, V.T.N.; Jenssen, T.G.; Mathisen, U.D.; Schei, J.; Solbu, M.D.; Wilsgaard, T.; Melsom, T. Blood Pressure and Age-Related GFR Decline in the General Population. BMC Nephrol. 2017, 18, 77. [Google Scholar] [CrossRef]
- Yu, Z.; Rebholz, C.M.; Wong, E.; Chen, Y.; Matsushita, K.; Coresh, J.; Grams, M.E. Association Between Hypertension and Kidney Function Decline: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Kidney Dis. 2019, 74, 310–319. [Google Scholar] [CrossRef]
- Pugh, D.; Gallacher, P.J.; Dhaun, N. Management of Hypertension in Chronic Kidney Disease. Drugs 2019, 79, 365–379. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.D.; McCulloch, C.E.; Banerjee, T.; Pavkov, M.E.; Burrows, N.R.; Gillespie, B.W.; Saran, R.; Shlipak, M.G.; Rowe, N.R.; Tuot, D.S. CKD Awareness among US Adults by Future Risk of Kidney Failure. Am. J. Kidney Dis. 2020, 76, 174–183. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | eGFR ≥ 90 | eGFR < 60 | p-Value * |
|---|---|---|---|
| N = 5543 | N = 687 | ||
| Age, mean ± S.E., y | 43.5 ± 15.1 | 70.2 ± 11.1 | <0.001 * |
| Sex (female), % | 2936 (53.0%) | 352 (51.2%) | 0.2 |
| Race/ethnicity, % | <0.001 * | ||
| Mexican American | 1106 (20.0%) | 67 (9.8%) | |
| Other Hispanic | 724 (13.1%) | 45 (6.6%) | |
| Non-Hispanic White | 1707 (30.8%) | 307 (44.7%) | |
| Non-Hispanic Black | 935 (16.9%) | 228 (33.2%) | |
| Non-Hispanic Asian | 1071 (19.3%) | 40 (5.8%) | |
| Other | |||
| Health conditions | |||
| Diabetes (yes), % | 759 (13.7%) | 262 (38.1%) | <0.01 * |
| Hypertension (yes), % | 1513 (27.3%) | 522 (76.0%) | <0.01 * |
| Cardiovascular disease (yes), % | 325 (5.9%) | 259 (37.7%) | <0.01 * |
| Kidney disease awareness (yes), % | 77 (1.4%) | 186 (27.1%) | <0.01 * |
| hs-CRP mg/L, mean ± S.E. | 3.9 ± 7.2 | 5.7 ± 10.2 | <0.01 * |
| DQ, median (25th, 75th percentile) | 52.8 (12.7, 62.0) | 53.3 (43.8, 63.1) | 0.2 |
| eGFR mL/min/1.73 m2, mean ± S.E. | 108.4 ± 11.5 | 46.4 ± 11.8 | <0.01 * |
| Model | Parameter | eGFR ≥ 90 | eGFR < 60 |
|---|---|---|---|
| β (95% CI) * | β (95% CI) * | ||
| 1 | Interaction: DQ×hs-CRP | −0.0 (−0.0–0.0) * | −0.004 (46.5–48.5) * |
| 2 | hs-CRP | −0.1 (−0.1–−0.0) * | −0.2 (−0.3–−0.1) * |
| DQ | −0.1 (−0.1–−0.1) * | 0.1 (0.0–0.1) * | |
| 3 | hs-CRP | 0.0 (−0.0–0.0) | −0.1 (−0.2–−0.0) * |
| DQ | 0.0 (−0.0–0.0) | 0.1 (0.0–0.1)* | |
| Gender | 2.1 (1.7–2.6) * | −0.5 (−2.2–1.3) | |
| Age | −0.5 (−0.5–−0.5) * | −0.1 (−0.7–−0.00) * | |
| Mexican American | 4.6 (3.9–5.2) * | 0.01 (−4.4–4.5) | |
| Other Hispanic | 2.5 (1.7–3.2) * | 0.8 (−4.0–5.7) | |
| Non-Hispanic White | −2.2 (−2.7–−1.7) * | 2.7 (−1.1–6.5) | |
| Non-Hispanic Black | −2.3 (−3.0–−1.7) * | 1.3 (−2.6–5.1) | |
| Other | Ref. | ||
| Hypertension | −0.1 (−0.7–0.5) | −3.9 (−2.5–1.1) * | |
| Diabetes | 1.7 (1.0–2.4) * | −0.8 (−2.6–1.0) | |
| Cardiovascular Disease | 0.0 (−0.9–1.0) | −0.7 (−2.5–1.1) | |
| Kidney awareness | 0.0 (−1.9–1.9) | −8.9 (−10.9–−7.0) * | |
| 4 | hs-CRP | 0.0 (−0.0–0.1) | −0.1 (−0.2–−0.5) * |
| DQ | 0.03 (0.0–0.1) * | 0.1 (0.0–0.1) * | |
| Age | −0.5 (−0.5–−0.5) * | −0.1 (−0.2–−0.0) * | |
| Hypertension | −0.5 (−1.0–0.1) | −4.3 (−6.1–−2.4) * | |
| Kidney awareness | 0.7 (−1.3–2.6) | −9.2 (−11.1–−7.4) * | |
| Dietary Components | eGFR ≥ 90 | eGFR < 60 | ||
|---|---|---|---|---|
| Median of DQ Scores (25th, 75th) | β (95% CI) * | Median of DQ Scores (25th, 75th) | β (95% CI) | |
| Total vegetables | 3.3 (2.0, 5.0) | −0.2 (−0.4–0.1) | 3.3 (1.9, 5.0) | 0.1 (−0.6–0.8) |
| Greens and Beans | 1.5 (0.0, 5.0) | 0.2 (−0.0–0.3) | 0.4 (0.0, 5.0) | 0.3 (−0.1–0.8) |
| Total Fruit | 1.9 (0.1, 4.8) | 0.2 (−0.1–0.5) | 2.3 (0.4, 5.0) | −0.1 (−0.9–0.8) |
| Whole Fruit | 2.2 (0.0, 5.0) | −0.5 (−0.7–−0.2) * | 3.0 (0.0, 5.0) | 0.4 (−0.3–1.1) |
| Whole Grain | 1.2 (0.0, 4.3) | −0.1 (−0.2–−0.2) * | 1.9 (0.0, 5.3) | −0.2 (−0.5–0.1) |
| Dairy | 4.4 (2.3, 7.0) | 0.2 (0.1–0.3) * | 3.9 (1.9, 6.5) | 0.2 (−0.1–0.6) |
| Total Protein | 5.0 (4.5, 5.0) | −0.1 (−0.5–0.2) | 5.0 (4.7, 5.0) | 0.2 (−1.0–1.4) |
| Seafood and Plant Proteins | 3.8 (0.2, 5.0) | −0.0 (−0.2–0.2) | 3.5 (0.0, 5.0) | 0.1 (−0.3–0.6) |
| Fatty Acids | 4.9 (2.2, 8.3) | −0.1 (−0.2–0.1) | 4.8 (2.4, 8.2) | 0.2 (−0.2–0.6) |
| Sodium | 3.8 (0.7, 6.5) | −0.1 (−0.2–0.0) | 4.1 (1.2, 6.7) | 0.2 (−0.1–0.6) |
| Refined Grains | 6.1 (2.7, 9.4) | −0.3 (−0.4–−0.2) * | 7.4 (4.2, 10.0) | 0.2 (−0.2–0.5) |
| Saturated Fats | 6.2 (3.4, 9.0) | 0.2 (0.1–0.3) * | 5.5 (2.6, 8.4) | −0.1 (−0.5–0.3) |
| Added Sugars | 8.3 (5.4, 10.0) | −0.1 (−0.2–0.0) | 7.9 (4.9, 10.0) | 0.0 (−0.3–0.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin Zarah, A.; Andrade, J.M. Elevated Inflammation and Poor Diet Quality Associated with Lower eGFR in United States Adults: An NHANES 2015–2018 Analysis. Nutrients 2024, 16, 528. https://doi.org/10.3390/nu16040528
Bin Zarah A, Andrade JM. Elevated Inflammation and Poor Diet Quality Associated with Lower eGFR in United States Adults: An NHANES 2015–2018 Analysis. Nutrients. 2024; 16(4):528. https://doi.org/10.3390/nu16040528
Chicago/Turabian StyleBin Zarah, Aljazi, and Jeanette Mary Andrade. 2024. "Elevated Inflammation and Poor Diet Quality Associated with Lower eGFR in United States Adults: An NHANES 2015–2018 Analysis" Nutrients 16, no. 4: 528. https://doi.org/10.3390/nu16040528
APA StyleBin Zarah, A., & Andrade, J. M. (2024). Elevated Inflammation and Poor Diet Quality Associated with Lower eGFR in United States Adults: An NHANES 2015–2018 Analysis. Nutrients, 16(4), 528. https://doi.org/10.3390/nu16040528