
Nutritional Considerations of Irish Performance Dietitians and Nutritionists in Concussion Injury Management




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics and Procedure
2.3. Participants Characteristics
2.4. Sampling and Eligibility Criteria
2.5. Data Collection
2.6. Researcher Description
2.7. Data Analysis
2.8. Transcription
2.9. Coding
3. Results
3.1. Participant Characteristics
3.2. Thematic Results
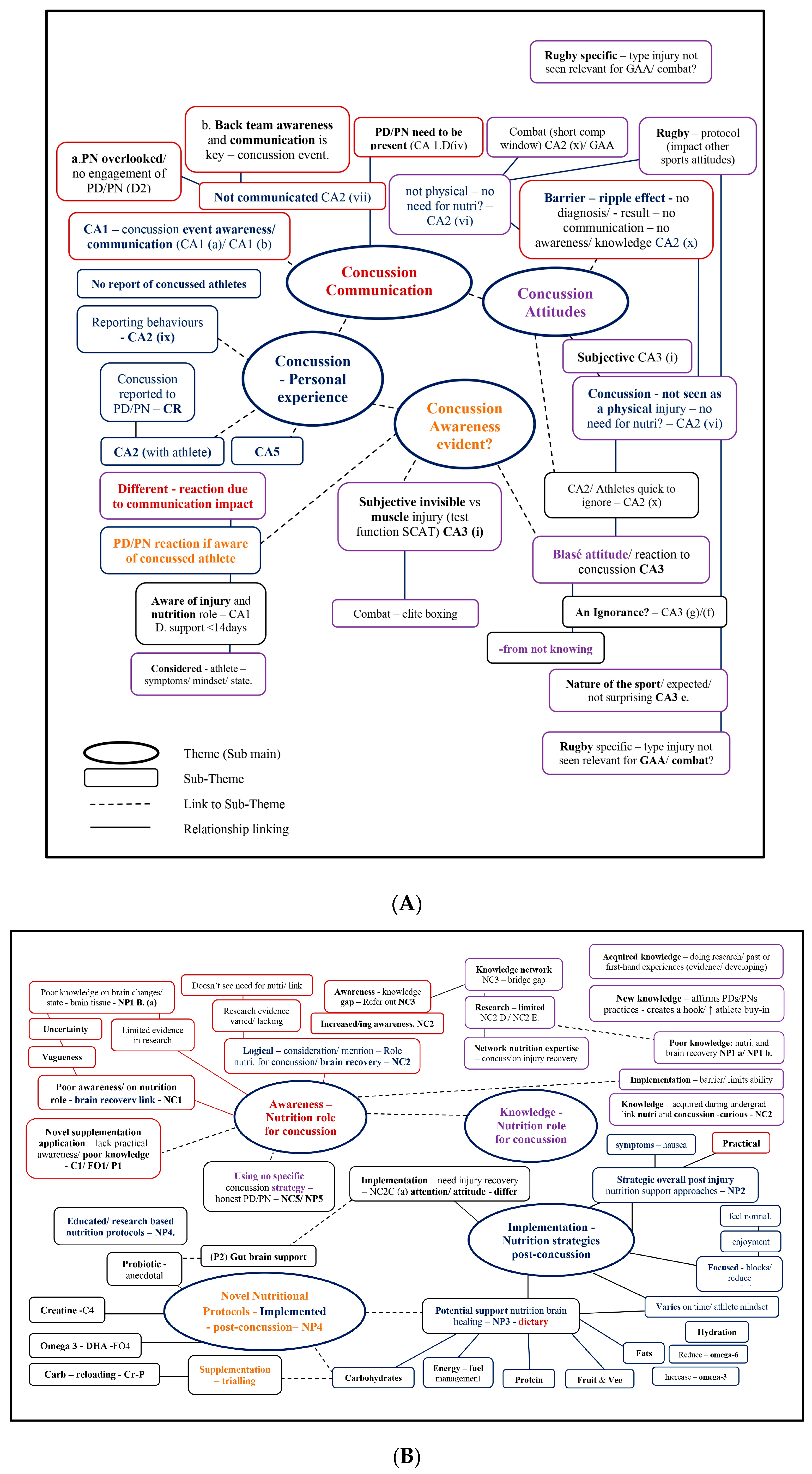
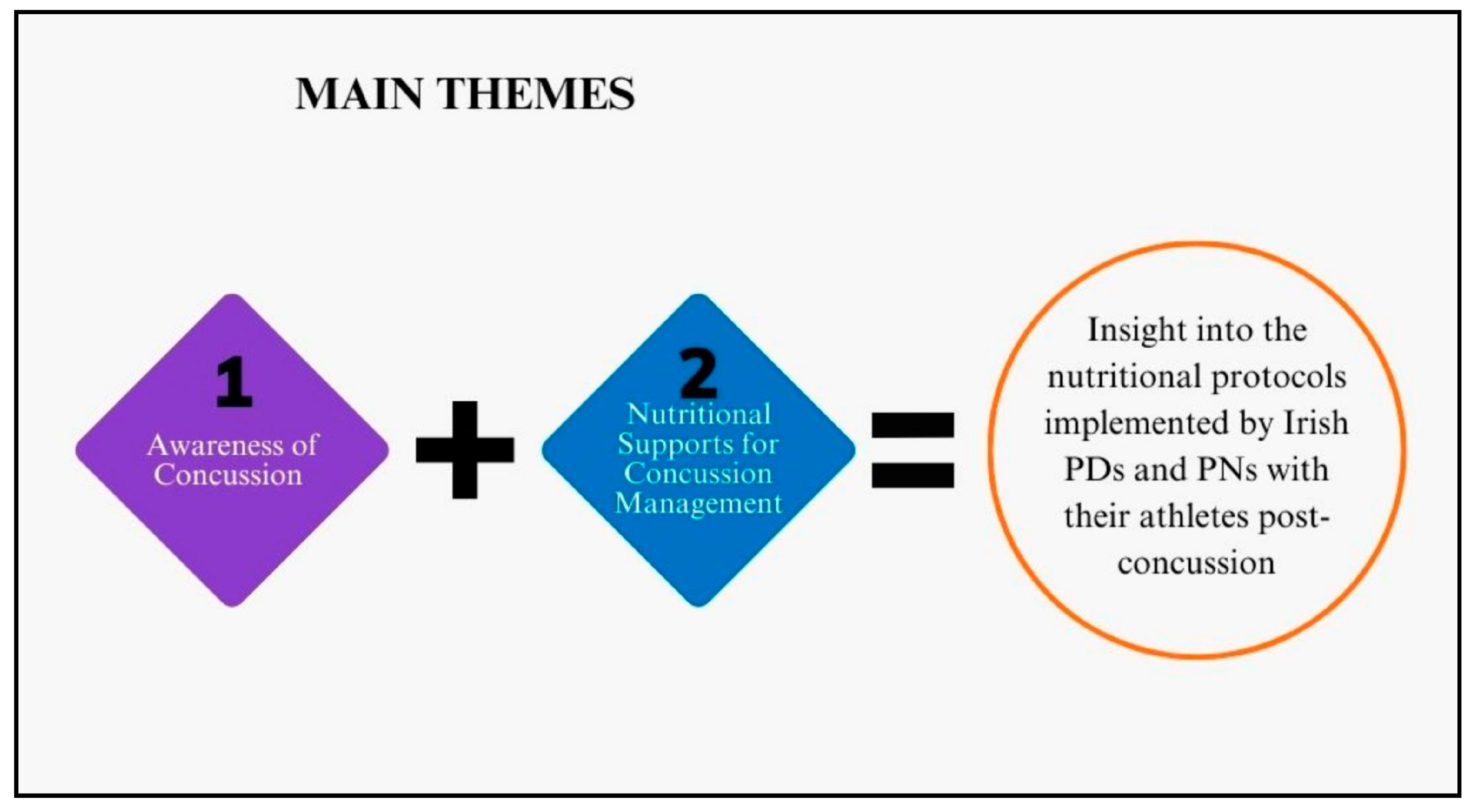
3.2.1. Irish Performance Dietitians and Nutritionists’ Awareness of Concussion
Concussion: Personal Experience
“I suppose obviously within… within rugby; we have like a lot of the collision-based injuries. So, for example, you know, the likes of concussion come up a lot and kind of ligament… ligament and tendons would be the ones that I see a lot of…”[PN 17]
“…I’m so lucky that, in just having the conversation with you there now… I’m just thinking back like five years, five years working in performance nutrition directly, and I have never had anyone with real…real acute injuries like.”[PN 10]
Concussion Communication
“Luckily, we don’t really get too many of them now like that I can; I can miss some as well just by not being on site too often…”[PN 4]
“I know when there is a decent backroom team that are all together, and I know when…they don’t really believe in all the different pillars as much as their own pillar… If you’ve got a backroom team that is set up in a very efficient way, it’s just them firing off a message to one person who does their part…”[PN 4]
“…the amateur, intercounty level…nutritionists are nearly shoved to the side ‘ahhh we don’t need the nutritionist on match day’, you know, but like physios they’re stade on foot…it’s happening at all corners, and that’s at the top level”[PN 13]
“…if you know the doc is on to them if you know the coach, the manager is on to them… if you know the physios are on to them, it sometimes best to void your time… I’ve gotten a little bit better at identifying when you are helpful and when you are just annoying them, you know?”[PN 5]
“I think in that scenario (pause)… I would wait to hear from…some other medical professional before doing anything…Rugby is one of those sports…I think that it’s further ahead than a lot of sports certainly in Ireland, where they do have that support on hand.”[PN 16]
Concussion Attitudes
“Overall, there’s nearly always have some kind of knock or a niggle or a strain… When we’re coming out off the back of matches…They’re just constantly in a state of basically recovery because they come out so beat and bruised from games.”[PN 8]
“…with guys that are there concussed, which are probably be quite regularly… which is unfortunately the case, your kind of on to them to stay away…”[PN 2]
“They don’t really care… I think it’s cause it’s such a common injury, like while concussion in GAA might be less common. When it’s so common in rugby…concussion is just like another…another injury”[PN 8]
Concussion Awareness Evidence
“But like, even if you look at concussions, like concussions, like a shortage of energy in the brain at the time of impact” [PN 9] (referring to increasing energy/caloric intake).
“to help with that energy availability side of things… Ehmm, if the brain can’t fully use their glucose efficiently” [PN 8] (referring to implementing creatine supplementation).
3.2.2. Theme 2: Nutritional Support for Concussion Management
Awareness of Using Nutrition in Concussion Management
“Not too sure, really, just keep up the good habits. But I haven’t looked at it… Is there much? Is there much research on concussion and nutrition immediate or…?”[PN 1]
“I think it’s a really good way of putting it in terms of like an invisible injury. You don’t, you don’t necessarily think that there’s a, there’s a change required. I guess they’re not wrong in saying that there probably isn’t from a nutrient point of view.”[PN 15]
“I know there is a little bit on creatine and omega-3 fish oils as well. Ehmm, so again, not a whole lot we can do.”[PN 7]
“Yeah, it’s, it’s an area I’m doing a bit of reading around at moment. But definitely, concussions are not that well-researched. But I think from what I have read there’s a couple things you can do and creatine, I believe is important in the… not even the acute phase of, of, of having a concussion, but I think consistently for optimal cognition.”[PN 2]
“So, what would I implement with somebody else? I think to be honest…the rest and the regular eating are, are crucial and then…the extra probiotics or, ehmm you know, whether they make that much of a difference, I don’t really know. But the anti-inflammatory, the protein, the carb, I think they would be crucial. Obviously, you know…your healthy fats as well. But the diet…the diet itself is probably the most important thing.”[PN 11]
“With regards to concussion, then we have two dietitians. One that actually has worked in rugby and who would I suppose work and are more familiar with the concussion side of things…”[PN 13]
“But like, even if you look at concussions, like concussions, like shortage of energy in the brain at the time of impact…you could, like, I’d broadly say it to people, you know…’just to make sure you eat enough during this time, and kind of, you know’, were kind of very basic interventions. But nothing, I don’t think we ever…got to a stage where we were comfortable giving nutrition advice to someone who was concussed because there was stuff out there on creatine and stuff on the high dose DHA, but…we never formalised that to a policy.”[PN 9]
Implementation—Nutrition Post-Concussion
“…if the player isn’t overly motivated, they’ll get blanket ehmm…they get blanket attention. The motivated player will get more attention. The educated player will snap back into their habits…”[PN 1]
“So tried to ensure energy levels were kept up just through kind of liquid-based meals, small little snacks, nothing that was going to cause…stomach aggravation… So, it was more kind of in that, you know, couple days after…after the knock as opposed to long term”[PN 7]
“So, the initial being, their protection phase, for example… I try row in with that being with ‘this is your initial focus’ instead of trying to bombard them with loads. Saying, ‘this is what I really want to get out of this block’, and then we tried to do it in focus.”[PN 8]
Potential Barriers
“…the guys who have been concussed recently… I definitely know one of them 100% was because he was looking for more creatine and everything, you know, because he was loading up on it”[PN 12]
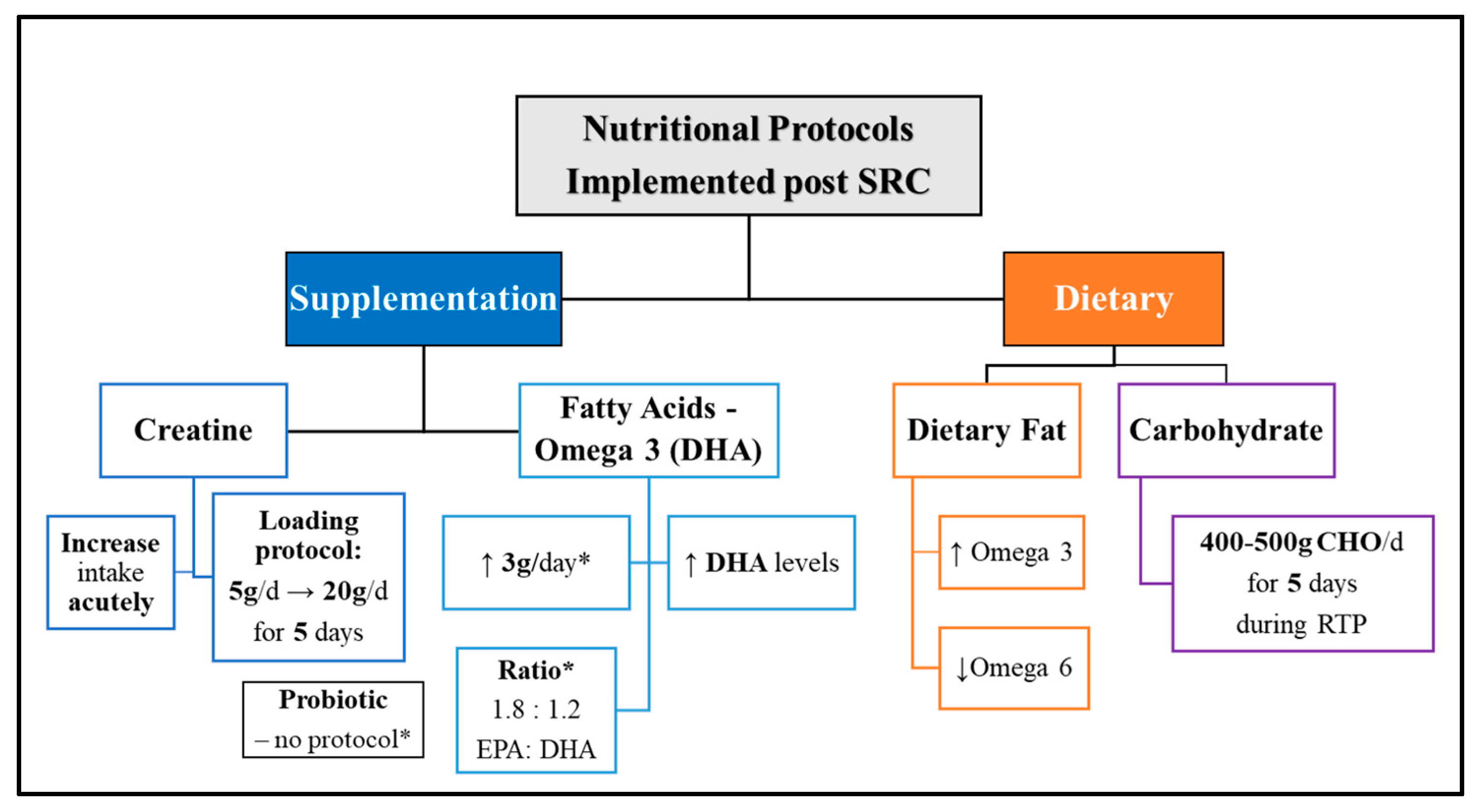
Novel Nutritional Protocol Implementation Post-Concussion
“…a lot of our athletes would take creatine. But if they haven’t or around a concussion, potentially increasing that creatine intake”[PN 8]
“I’ll even tell them to load creatine and during that period…the week after a concussion, instead of just taking 5 g a day, I’ll get them to load like 20 g a day of creatine just for that little period…then the rest is kind of lead…by the physio”[PN 12]
“Ehmm, 3 about 3 g of…so that’s about 1.8 g. I think it’s like 1.8 to…the ratio was like 1.8 to 1.2, EPA:DHA…with the concussion. I’m trying to get the DHA levels up a little bit more.”[PN 12]
“…like 4 or 500 g of carbs in the 5 days, after concussion versus the guys that had a low carbohydrate diet and the symptoms for the guys that had more carbohydrates were got back to baseline that bit quicker.So, that is kind of something I have been doing; it’s like, well, if a guy is in a gradual return to play protocol, then can you eat enough food? Specifically, carbohydrates…in that 5-day period. So that’s one new area…”[PN 2]
“…I would recommend a probiotic as well for a little while anyway… I know it’s not maybe an area that’s not that well researched yet, but the link between the gut and the head (holding head).”[PN 11]
4. Discussion
4.1. Nutrition Protocols Being Implemented Irish PDs/PNs
4.1.1. Omega-3–Docosahexaenoic Acid (DHA)
“Ehmm, 3 about 3 g of, so that’s about 1.8 g. I think it’s like 1.8 to…the ratio was like 1.8 to 1.2, EPA:DHA…with the concussion. I’m trying to get the DHA levels up a little bit more…”[PN 12]
4.1.2. Carbohydrates
4.1.3. Probiotics
4.2. Impact of Back-Team Collaboration and Communication
4.2.1. Communication, Collaboration, and SRC Reporting
4.2.2. Roles and Perceived Responsibility
4.3. Limitations
4.4. Future Recommendations
- 1.
- Further research that is robust and can be safely implemented to support and manage concussion recovery in a sporting context is needed. Irish PDs/PNs have cited using creatine, omega-3 fatty acids, probiotics, and carbohydrate reloading strategies. The availability of human-based evidence is limited, highlighting the necessity for additional investigation and research in this area.
- 2.
- Concussion and head injury education and training should be mandatory for all healthcare practitioners supporting athletes, including nutrition experts (PDs and PNs), psychologists, and physical therapists (physio, rehabilitation, and athletic) working with or as part of the back team. According to the latest concussion management protocols, a diagnosis should ideally be conducted by medical healthcare professionals such as a doctor or physiotherapist [1], which is not feasible for many sports settings (i.e., amateur, underage, and female). To address this limitation, we recommended that all healthcare practitioners in the multidisciplinary care team receive comprehensive training on brain injuries and concussions.
- 3.
- Open and transparent communication among all back-team members, actively involving PDs/PNs in player analysis, performance, and injury discussions, is needed. This collaborative approach will help mitigate the risk of missing acute injury management and the subsequent risk of poor recovery outcomes for athletes.
- 4.
- Regular monitoring of athletes’ hydration and mental capacity status should be implemented during pre-match hydration test protocols to identify and prevent cognitive decline and, as a result, help reduce the risk of an impact occurring during gameplay. PDs/PNs can use the CRT6 and SCAT6 tools to educate athletes about the effects of their hydration and its impact on brain function. They can use it as evidence to address suboptimal nutrition, assess performance, and measure the recovery of athletes with SRC. By conducting regular evaluations and the monitoring of athletes, PDs/PNs can enhance nutrition protocols for concussion recovery and support athletes, ultimately helping them prevent injury and achieve optimal recovery and RTP outcomes.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patricios, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus statement on concussion in sport: The 6th international conference on concussion in sport–Amsterdam, October 2022. Br. J. Sports Med. 2023, 57, 695–711. [Google Scholar] [CrossRef]
- Hallock, H.; Mantwill, M.; Vajkoczy, P.; Wolfarth, B.; Reinsberger, C.; Lampit, A.; Finke, C. Sport-related concussion: A cognitive perspective. Neurol. Clin. Pract. 2023, 13, e200123. [Google Scholar] [CrossRef]
- Finnegan, E.; Daly, E.; Pearce, A.J.; Ryan, L. Nutritional interventions to support acute mTBI recovery. Front. Nutr. 2022, 9, 977728. [Google Scholar] [CrossRef]
- Van Pelt, K.L.; Puetz, T.; Swallow, J.; Lapointe, A.P.; Broglio, S.P. Data-driven risk classification of concussion rates: A systematic review and meta-analysis. Sports Med. 2021, 51, 1227–1244. [Google Scholar] [CrossRef]
- Harmon, K.G.; Drezner, J.A.; Gammons, M.; Guskiewicz, K.M.; Halstead, M.; Herring, S.A.; Kutcher, J.S.; Pana, A.; Putukian, M.; Roberts, W.O. American medical society for sports medicine position statement: Concussion in sport. Br. J. Sports Med. 2013, 47, 15–26. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Nowinski, C.J.; McKee, A.C.; Cantu, R.C. The epidemiology of sport-related concussion. Clin. Sports Med. 2011, 30, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Langlois, J.A.; Rutland-Brown, W.; Wald, M.M. The epidemiology and impact of traumatic brain injury: A brief overview. J. Head Trauma Rehabil. 2006, 21, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.J.; Patricios, J.; Echemendia, R.J.; Makdissi, M.; Davis, G.A.; Ahmed, O.H.; Blauwet, C.; Dvorak, J.; Engebretsen, L. Concussion in sport: The consensus process continues. Br. J. Sports Med. 2022, 56, 1059–1060. [Google Scholar] [CrossRef] [PubMed]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef]
- Daly, E.; Pearce, A.J.; Finnegan, E.; Cooney, C.; McDonagh, M.; Scully, G.; McCann, M.; Doherty, R.; White, A.; Phelan, S.; et al. An assessment of current concussion identification and diagnosis methods in sports settings: A systematic review. BMC Sports Sci. Med. Rehabil. 2022, 14, 125. [Google Scholar] [CrossRef] [PubMed]
- Walrand, S.; Gaulmin, R.; Aubin, R.; Sapin, V.; Coste, A.; Abbot, M. Nutritional factors in sport-related concussion. Neurochirurgie 2021, 67, 255–258. [Google Scholar] [CrossRef]
- Lust, C.A.C.; Mountjoy, M.; Robinson, L.E.; Oliver, J.M.; Ma, D.W. Sports-related concussions and subconcussive impacts in athletes: Incidence, diagnosis, and the emerging role of EPA and DHA. Appl. Physiol. Nutr. Metab. 2020, 45, 886–892. [Google Scholar] [CrossRef]
- Beidler, E.; Wallace, J.; Alghwiri, A.A.; O’Connor, S. Collegiate athletes’ concussion awareness, understanding, and -reporting behaviors in different countries with varying concussion publicity. J. Athl. Train. 2021, 56, 77–84. [Google Scholar] [CrossRef]
- O’Connor, S.; Geaney, D.; Beidler, E. Non-disclosure in Irish collegiate student-athletes: Do concussion history, knowledge, pressure to play and gender impact concussion reporting? Phys. Sportsmed. 2020, 48, 186–193. [Google Scholar] [CrossRef]
- Leahy, R.; Farrington, S.; Whyte, E.; O’Connor, S. Concussion reporting, knowledge and attitudes in Irish amateur Gaelic games athletes. Phys. Ther. Sport 2019, 43, 236–243. [Google Scholar] [CrossRef]
- Nolan, K.E.; Caccese, J.B.; Kontos, A.P.; Buckley, T.A.; Garcia, G.P.; Port, N.; Broglio, S.P.; McAllister, T.W.; McCrea, M.; Pasquina, P.F.; et al. Primary and Secondary risk factors associated with concussion symptom clusters in collegiate athletes: Results from the NCAA-DoD grand alliance CARE consortium. Orthop. J. Sports Med. 2023, 11, 23259671231163581. [Google Scholar] [CrossRef]
- Ryan, L.; Daly, E.; Blackett, A.D. Sport-related concussion disclosure in women’s rugby—A social identity approach. Front. Sports Act. Living 2023, 5, 1058305. [Google Scholar] [CrossRef]
- Piedade, S.R.; Hutchinson, M.R.; Ferreira, D.M.; Cristante, A.F.; Maffulli, N. The management of concussion in sport is not standardized. A systematic review. J. Saf. Res. 2021, 76, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Rotundo, M.; Sokol-Randell, D.; Bleakley, C.M.; Donnelly, P.; Tierney, G. Characteristics of potential concussive events in elite hurling: A video-analysis study. Ir. J. Med. Sci. 2023, 17, 3175–3185. [Google Scholar] [CrossRef] [PubMed]
- Walshe, A.; Daly, E.; Ryan, L. Epidemiology of sport-related concussion rates in female contact/collision sport: A systematic review. BMJ Open Sport Exerc. Med. 2022, 8, e001346. [Google Scholar] [CrossRef] [PubMed]
- Meehan, W.P.; Taylor, A.M.; Berkner, P.; Sandstrom, N.J.; Peluso, M.W.; Kurtz, M.M.; Pascual-Leone, A.; Mannix, R. Division III collision sports are not associated with neurobehavioral quality of life. J. Neurotrauma 2016, 33, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Turnagöl, H.H.; Koşar, N.; Güzel, Y.; Aktitiz, S.; Atakan, M.M. Nutritional considerations for injury prevention and recovery in combat sports. Nutrients 2021, 14, 53. [Google Scholar] [CrossRef] [PubMed]
- Lemme, N.J.; Johnston, B.; DeFroda, S.F.; Owens, B.D.; Kriz, P.K. Incidence of combat sport-related mild traumatic brain injuries presenting to the emergency department from 2012 to 2016. Clin. J. Sport Med. 2020, 30, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Neidecker, J.; Sethi, N.K.; Taylor, R.; Monsell, R.; Muzzi, D.; Spizler, B.; Lovelace, L.; Ayoub, E.; Weinstein, R.; Estwanik, J.; et al. Concussion management in combat sports: Consensus statement from the association of ringside physicians. Br. J. Sports Med. 2019, 53, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Heron, N.; Jones, N.; Cardwell, C.; Gomes, C. ‘If in doubt, sit them out’: How long to return to elite cycling competition following a sports-related concussion (SRC)? Int. J. Environ. Res. Public Health 2023, 20, 5449. [Google Scholar] [CrossRef]
- Lumba-Brown, A.; Yeates, K.O.; Sarmiento, K.; Breiding, M.J.; Haegerich, T.M.; Gioia, G.A.; Turner, M.; Benzel, E.C.; Suskauer, S.J.; Giza, C.C.; et al. Diagnosis and management of mild traumatic brain injury in children: A systematic review. JAMA Pediatr. 2018, 172, e182847. [Google Scholar] [CrossRef]
- Marchand, N.E.; Jensen, M.K. The role of dietary and lifestyle factors in maintaining cognitive health. Am. J. Lifestyle Med. 2018, 12, 268–285. [Google Scholar] [CrossRef] [PubMed]
- Verboon, L.N.; Patel, H.C.; Greenhalgh, A.D. The immune system’s role in the consequences of mild traumatic brain injury (concussion). Front. Immunol. 2021, 12, 620698. [Google Scholar] [CrossRef]
- Shukla, D.; Devi, B.I. Mild traumatic brain injuries in adults. J. Neurosci. Rural. Pract. 2010, 1, 82–88. [Google Scholar] [CrossRef]
- Scullion, E.; Heron, N. A scoping review of concussion guidelines in amateur sports in the United Kingdom. Int. J. Environ. Res. Public Health 2022, 19, 1072. [Google Scholar] [CrossRef]
- Conaghan, C.; Daly, E.; Ryan, L. An accessible concussion education tool that improves athlete, coach and parent knowledge and attitudes. Austin. Sports Med. 2022, 7, 1049. [Google Scholar]
- Halstead, M.E.; Walter, K.D.; Moffatt, K.; Council on Sports Medicine and Fitness. Sport-Related Concussion in Children and Adolescents. Pediatrics 2018, 142, e20183074. [Google Scholar] [CrossRef]
- Iverson, G.L.; Gardner, A.J.; Terry, D.P.; Ponsford, J.L.; Sills, A.K.; Broshek, D.K.; Solomon, G.S. Predictors of clinical recovery from concussion: A systematic review. Br. J. Sports Med. 2017, 51, 941–948. [Google Scholar] [CrossRef]
- Kim, S.; Han, S.C.; Gallan, A.J.; Hayes, J.P.; Fakhran, S.; Delic, J.; Alhilali, L.; Jagannathan, J.; McDevitt, J.; Krynetskiy, E.; et al. Neurometabolic indicators of mitochondrial dysfunction in repetitive mild traumatic brain injury. Concussion 2017, 2, CNC45. [Google Scholar] [CrossRef] [PubMed]
- Flueck, J.L.; Parnell, J.A. Protein considerations for athletes with a spinal cord injury. Front. Nutr. 2021, 8, 142441. [Google Scholar] [CrossRef] [PubMed]
- Smith-Ryan, A.E.; Hirsch, K.R.; Saylor, H.E.; Gould, L.M.; Blue, M.N.M. Nutritional considerations and strategies to facilitate injury recovery and rehabilitation. J. Athl. Train. 2020, 55, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.I.; Ahmad, A.; Wafa, S.W.W.S.S.T.; Latif, A.Z.A.; Yusoff, N.A.M.; Jasmiad, M.K.; Udin, N.; Karim, K.A. Determination of calorie and protein intake among acute and sub-acute traumatic brain injury patients. Chin. J. Traumatol. 2020, 23, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Dighriri, I.M.; Alsubaie, A.M.; Hakami, F.M.; Hamithi, D.M.; Alshekh, M.M.; Khobrani, F.A.; Dalak, F.E.; Hakami, A.A.; Alsueaadi, E.H.; Alsaawi, L.S.; et al. Effects of omega-3 polyunsaturated fatty acids on brain functions: A systematic review. Cureus 2022, 14, e30091. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.M.; Zynda, A.J.; Sabatino, M.J.; Jo, C.; Ellis, H.B.; Dimeff, R.J. A pilot randomized controlled trial of docosahexaenoic acid for the treatment of sport-related concussion in adolescents. Clin. Pediatr. 2022, 61, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Heileson, J.L.; Anzalone, A.J.; Carbuhn, A.F.; Askow, A.T.; Stone, J.D.; Turner, S.M.; Hillyer, L.M.; Ma, D.W.L.; Luedke, J.A.; Jagim, A.R.; et al. The effect of omega-3 fatty acids on a biomarker of head trauma in NCAA football athletes: A multi-site, non-randomized study. J. Int. Soc. Sports Nutr. 2021, 18, 65. [Google Scholar] [CrossRef]
- Thielecke, F.; Blannin, A. Omega-3 fatty acids for sport performance—Are they equally beneficial for athletes and amateurs? A narrative review. Nutrients 2020, 12, 3712. [Google Scholar] [CrossRef]
- Armstrong, A.; Anzalone, A.J.; Pethick, W.; Murray, H.; Dahlquist, D.T.; Askow, A.T.; Heileson, J.L.; Hillyer, L.M.; Ma, D.W.L.; Oliver, J.M. An evaluation of omega-3 status and intake in Canadian elite rugby 7s players. Nutrients 2021, 13, 3777. [Google Scholar] [CrossRef] [PubMed]
- Ritz, P.P.; Rogers, M.B.; Zabinsky, J.S.; Hedrick, V.E.; Rockwell, J.A.; Rimer, E.G.; Kostelnik, S.B.; Hulver, M.W.; Rockwell, M.S. Dietary and biological assessment of the omega-3 status of collegiate athletes: A cross-sectional analysis. PLoS ONE 2020, 15, e0228834. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the Tolerable Upper Intake Level of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and docosapentaenoic acid (DPA). EFSA J. 2012, 10, 2815. [Google Scholar]
- Lawrence, D.W.; Sharma, B. A review of the neuroprotective role of vitamin D in traumatic brain injury with implications for supplementation post-concussion. Brain Inj. 2016, 30, 960–968. [Google Scholar] [CrossRef]
- Standiford, L.; O’Daniel, M.; Hysell, M.; Trigger, C. A randomized cohort study of the efficacy of PO magnesium in the treatment of acute concussions in adolescents. Am. J. Emerg. Med. 2020, 44, 419–422. [Google Scholar] [CrossRef]
- Prokopidis, K.; Giannos, P.; Triantafyllidis, K.K.; Kechagias, K.S.; Forbes, S.C.; Candow, D.G. Effects of creatine supplementation on memory in healthy individuals: A systematic review and meta-analysis of randomized controlled trials. Nutr. Rev. 2023, 81, 416–427. [Google Scholar] [CrossRef]
- Forbes, S.C.; Cordingley, D.M.; Cornish, S.M.; Gualano, B.; Roschel, H.; Ostojic, S.M.; Rawson, E.S.; Roy, B.D.; Prokopidis, K.; Giannos, P.; et al. Effects of creatine supplementation on brain function and health. Nutrients 2022, 14, 921. [Google Scholar] [CrossRef]
- Beck, K.L.; Thomson, J.S.; Swift, R.J.; von Hurst, P.R. Role of nutrition in performance enhancement and postexercise recovery. Open Access J. Sports Med. 2015, 6, 259–267. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Draper, A.; Swift, J.A. Qualitative research in nutrition and dietetics: Data collection issues. J. Hum. Nutr. Diet. 2011, 24, 3–12. [Google Scholar] [CrossRef]
- Valerio, M.A.; Rodriguez, N.; Winkler, P.; Lopez, J.; Dennison, M.; Liang, Y.; Turner, B.J. Comparing two sampling methods to engage hard-to-reach communities in research priority setting. BMC Med. Res. Methodol. 2016, 16, 146. [Google Scholar] [CrossRef]
- Tufford, L.; Newman, P. Bracketing in qualitative research. Qual. Soc. Work. 2010, 11, 80–96. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Fuller, G.W.; Kemp, S.; Decq, P. The International Rugby Board (IRB) pitch side concussion assessment trial: A pilot test accuracy study. Br. J. Sports Med. 2015, 49, 529–535. [Google Scholar] [CrossRef]
- Sport concussion assessment tool—5th edition. Br. J. Sports Med. 2017, 51, 851–858. [CrossRef]
- Echemendia, R.J.; Meeuwisse, W.; McCrory, P.; Davis, G.A.; Putukian, M.; Leddy, J.; Makdissi, M.; Sullivan, S.J.; Broglio, S.P.; Raftery, M.; et al. The Sport Concussion Assessment Tool 5th Edition (SCAT5). Br. J. Sports Med. 2017, 51, 848–850. [Google Scholar] [CrossRef] [PubMed]
- Frakes, M.R. The Impact of Dietary Intake on Concussion Recovery in Division I NCAA Athletes. Ph.D. Thesis, University of Mississippi, Mississippi, MS, USA, 2020. Available online: https://egrove.olemiss.edu/etd/1870 (accessed on 22 June 2023).
- Frakes, M.; Valliant, M.W.; Crowther, M.; Michel, J.; Callaway, K.; Morgan, B.; Franks, C.; Beyke, A. Collegiate athletes that consumed adequate energy post-concussion reported fewer days of concussion-related symptoms. Med. Sci. Sports Exerc. 2019, 51, 864–865. [Google Scholar] [CrossRef]
- Vagnozzi, R.; Signoretti, S.; Floris, R.; Marziali, S.; Manara, M.; Amorini, A.M.; Belli, A.; Di Pietro, V.; D’Urso, S.; Pastore, F.S.; et al. Decrease in n-acetylaspartate following concussion may be coupled to decrease in creatine. J. Head Trauma Rehabil. 2013, 28, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Ashbaugh, A.; McGrew, C. The role of nutritional supplements in sports concussion treatment. Curr. Sports Med. Rep. 2016, 15, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Solis, M.Y.; Artioli, G.G.; Otaduy, M.C.G.; Leite, C.D.C.; Arruda, W.; Veiga, R.R.; Gualano, B. Effect of age, diet, and tissue type on PCr response to creatine supplementation. J. Appl. Physiol. 2017, 123, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Kaviani, M.; Shaw, K.; Chilibeck, P.D. Benefits of creatine supplementation for vegetarians compared to omnivorous athletes: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 3041. [Google Scholar] [CrossRef] [PubMed]
- Giza, C.C.; Hovda, D.A. The new neurometabolic cascade of concussion. Neurosurgery 2014, 75 (Suppl. S4), S24–S33. [Google Scholar] [CrossRef] [PubMed]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef]
- Januszko, P.; Lange, E. Nutrition, supplementation and weight reduction in combat sports: A review. AIMS Public Health 2021, 8, 485–498. [Google Scholar] [CrossRef]
- Rici, T.; Forbes, S.C.; Candow, D.G. Creatine supplementation: Practical strategies and considerations for mixed martial arts. J. Exerc. Nutr. 2020, 3, s2. Available online: https://www.journalofexerciseandnutrition.com/index.php/JEN/article/view/58 (accessed on 28 June 2023).
- Turner, C.E.; Byblow, W.D.; Gant, N. Creatine Supplementation enhances corticomotor excitability and cognitive performance during oxygen deprivation. J. Neurosci. 2015, 35, 1773–1780. [Google Scholar] [CrossRef]
- The Omega-3 Protocol for Brain Health—Brain Health Education and Research Institute [Internet]. Available online: http://www.brainhealtheducation.org/resources/brain-injury-protocol/ (accessed on 21 June 2023).
- Falk, H.; Korley, F. A pilot study of omega-3 polyunsaturated fatty acid treatment in mild acute TBI (Optima-TBI pilot). J. Neurotrauma. 2018, 35, A144. [Google Scholar] [CrossRef]
- Baracaldo-Santamaría, D.; Ariza-Salamanca, D.F.; Corrales-Hernández, M.G.; Pachón-Londoño, M.J.; Hernandez-Duarte, I.; Calderon-Ospina, C.A. Revisiting excitotoxicity in traumatic brain injury: From bench to bedside. Pharmaceutics 2022, 14, 152. [Google Scholar] [CrossRef]
- Brenner, L.A.; Forster, J.E.; Stearns-Yoder, K.A.; Stamper, C.E.; Hoisington, A.J.; Brostow, D.P.; Mealer, M.; Wortzel, H.S.; Postolache, T.T.; Lowry, C.A. Evaluation of an Immunomodulatory Probiotic Intervention for Veterans with Co-occurring Mild Traumatic Brain injury and posttraumatic stress disorder: A pilot study. Front. Neurol. 2020, 11, 1015. [Google Scholar] [CrossRef]
- Soriano, S.; Curry, K.; Sadrameli, S.S.; Wang, Q.; Nute, M.; Reeves, E.; Kabir, R.; Wiese, J.; Criswell, A.; Schodrof, S.; et al. Alterations to the gut microbiome after sport-related concussion in a collegiate football players cohort: A pilot study. Brain, Behav. Immun. Health 2022, 21, 100438. [Google Scholar] [CrossRef]
- Ekstrand, J.; Lundqvist, D.; Davison, M.; D’Hooghe, M.; Pensgaard, A.M. Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs. Br. J. Sports Med. 2019, 53, 304–308. [Google Scholar] [CrossRef]
- Ghrairi, M.; Loney, T.; Pruna, R.; Malliaropoulos, N.; Valle, X. Effect of poor cooperation between coaching and medical staff on muscle re-injury in professional football over 15 seasons. Open Access J. Sports Med. 2019, 10, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Corman, S.R.; Adame, B.J.; Tsai, J.-Y.; Ruston, S.W.; Beaumont, J.S.; Kamrath, J.K.; Liu, Y.; Posteher, K.A.; Tremblay, R.; van Raalte, L.J. Socioecological influences on concussion reporting by NCAA Division 1 athletes in high-risk sports. PLoS ONE 2019, 14, e0215424. [Google Scholar] [CrossRef] [PubMed]
- Knollman-Porter, K.; Thaxton, S.; Hughes, M.R.; Constantinidou, F. Management and recovery patterns following sport-related mild traumatic brain injury in male and female college athletes. Top. Lang. Disord. 2019, 39, 257–275. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Participants Profile | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample (n) | n = 17 | ||||||||||
| Gender | Male | Female | |||||||||
| % (n) | 59% (10) | 51% (7) | |||||||||
| Undergraduate degree | BSc Dietetics and nutrition sciences | BSc Human nutrition sciences | BSc Nutrition and sports sciences | BSc Health, sport, and exercise sciences | BA Education with science | Other (BA, BCom, BBS non-science degrees) | |||||
| % (n) | 11.8% (2) | 17.6% (3) | 5.9% (1) | 35.3% (6) | 11.8% (2) | 17.6% (3) | |||||
| Post Graduate degree (MSc/PhD) | MSc in Sports Nutrition | Dip Sports Nutrition | MSc Sports and Exercise Nutrition | MSc in Human or/and Nutrition, | MRes in Sport and Exercise Nutrition | Doctor of Philosophy (PhD) | |||||
| (n) | (4) | (3) | (9) | (2) | (1) | (5) Specialisms included: Energy, Sports, and Exercise Nutrition Bone Health, Exercise Biochemistry, Bioactives in Health and Exercise. | |||||
| SENr Registered % (n) | Yes 100% (17) | ||||||||||
| Previously concussed (history) % (n) | Yes 23.5% (4) | No 76.5% (13) | |||||||||
| PN-ID | Type Athlete/Client | Teams/Organisations | Part/Full-time | ||||||||
| PN 1 | Elite teams: male senior and U20s Gaelic footballers—county-level. | GAA | Part-time/contract roles | ||||||||
| PN 2 | Elite teams: male athletes in rugby union—academy and senior squads; male Gaelic footballers—county-level. | IRFU, GAA | Full-time | ||||||||
| PN 3 | Elite individual athletes (mixed); elite teams: rugby union (senior, academy males/7s, XVs female) and senior (male) Gaelic football and hurling athletes—county and intercounty levels. | Sport Ireland, University scholarships, Athletics Ireland, IRFU, LGFA, GAA | Part-time/contract roles | ||||||||
| PN 4 | Elite teams: men’s hurling and ladies’ and men’s Gaelic football (male/female) athletes. Individuals: amateur/non-elite-MMA, soccer athletes. | LGFA, GAA | Part-time/contract roles | ||||||||
| PN 5 | Elite amateur teams: Gaelic football athletes; individual: amateur/non-elite endurance and rugby athletes | GAA | Full-time | ||||||||
| PN 6 | Individual: retired professional/high-level amateur-endurance (runners, cyclists), kickboxing, high-intensity functional training, powerlifting athletes | N/A | Full-time-self-employed | ||||||||
| PN 7 | High-level amateur teams: U20 hurlers (county) and senior men’s Gaelic footballers (intercounty). Individual: soccer athletes. | GAA | Part-time roles | ||||||||
| PN 8 | Elite/Professional teams: academy, youth, and senior men’s rugby union (current). Women’s soccer, senior ladies’, and U20s men’s Gaelic football and hurling at county and intercounty levels (past). Individual: Triathletes (paralympic squad, past). | IRFU, LGFA, GAA, Women’s FC | Full-time | ||||||||
| PN 9 | Elite: Women’s XV and 7s and men’s 7s academy and sub-academy rugby union teams. Amateur: junior Gaelic intercounty team athletes. | IRFU, GAA | Full-time | ||||||||
| PN 10 | Teams: U21s and mixed 1–1 Gaelic footballs. Individual: professional and amateur combat male/female athletes—boxers, MMA, and kickboxing. | GAA | Full-time-self-employed | ||||||||
| PN 11 | Teams: Elite/high-level women’s soccer, hockey, and rugby union squads. Individual: mixed 1–1 athletes. | WFC, women’s hockey, IRFU, SN private practice | Part-time/contract roles | ||||||||
| PN 12 | Elite/high-level amateur teams: U20s and senior Gaelic footballers and hurlers. | GAA | Part-time/contract roles | ||||||||
| PN 13 | Elite teams: women’s hockey, individual junior gymnastic athletes, and endurance athletes (cyclists). | Sport Ireland | Full-time | ||||||||
| PN 14 | Teams: professional rugby union and high-level amateur Gaelic football athletes. Individual: elite/professional Olympic boxers, rowers, athletics, judo, and cricket athletes. | Sport Ireland | Full-time | ||||||||
| PN 15 | Teams: senior and U21 Gaelic footballers and hurlers, academy male rugby union athletes. Individual: Gaelic footballers, hurlers, and jockeys. | GAA, IRFU | Part-time roles | ||||||||
| PN 16 | Team: rugby/soccer/hockey/Gaelic hurling, camogie, football, club, intercounty, ladies, men’s athletes. Individual: competitive/high level/weight class athletes/HIFT/multi-sport athletes (boxers, Olympic, power weightlifting/MMA)/endurance athletes. | N/A | Full-time | ||||||||
| PN 17 | Teams: professional rugby union—male academy/NTS squads (16 years up), high-level amateur intercounty Gaelic football and Camogie athletes. Individual: endurance athletes. | IRFU | Part-time roles | ||||||||
| Theme | Subtheme | Example Quote |
|---|---|---|
| 1. PD/PN Personal experiences with concussion injuries | Concussion diagnosis reported to PD/PN | …your first most common will be, ehmm, connective tissue injuries. So, like your shoulders…shoulders, ACLs, ankles syndesmosis, then followed by concussion, and then you have your hamstrings and calves like soft tissues, and then you have your broken bones, and then your kind of back injuries would be. [PN 9] |
| Concussions not reported by athletes to PD/PN | …you never…never even hear of like concussions reported back to you, but God knows, even though it’s probably likely you’ll never hear back! [PN 12] | |
| Personal concussion experience | First impact: …the first one happened during a hockey match… I just stepped back, and the player behind me…stepped back, and it was just like totally innocuous. No big deal; we didn’t even hit heads that that hard! I played on…totally, sort of out of it! I went off, and then I tried to insist on going back on, but then eventually the penny dropped that I wasn’t ok and like I couldn’t keep my eyes open… I felt fine again a few hours later… If I’m honest, I didn’t change anything about the way I was eating, then. I just…sort of slept a bit more. [PN 11] Second impact: …next one, then only about four months later, I got a ball right into the face; a hockey ball. I kind of knew then I’m obviously slower… I did make the change (nutritionally) at that stage…I would be, you know, eating more regularly…making sure my protein intake would better across the day…the probiotics… I was a bit worried. [PN 11] Third impact: …the third one. I was playing with my kids in the swimming pool…managed to smack my head off the bottom of it…then…I didn’t play hockey for quite a while because I wanted…to get a brain scan… Three in 18 months is a lot! [PN 11] | |
| 2. Concussion injury communication | Back-team communication key-acute injury | …I know when there is a decent backroom team that are all together, and I know when… they don’t really believe in all the different pillars as much as their own pillar… If you’ve got a backroom team that is set up in a very efficient way, it’s just then firing off a message to one person who does their part… I would work very closely with one set of backroom teams, the doctor and the physio, and the S&C coach… Even though they’ve changed… the doctor never has… there has always been a kind of a multi-faceted approach… Whereas in other situations, it hasn’t been as strong, you know, and I think that makes a big difference in terms of catching the acute phase. [PN 4] |
| Open Communication | So, making contact… as soon as possible, but again… if you know the doc is on to them if you know the coach, the manager is on to them… if you know the physios are on to them, it is sometimes best to void your time… I’ve gotten a little bit better at identifying when are you helpful and when are you just annoying them you know? [PN 5] | |
| 3. Poor Concussion Reporting-Risk | Lucky or poor communication and reporting? | I’m…I’m so I’m so lucky that in just having the conversation with you there now… I’m just thinking back like five years, five years working in performance nutrition directly, and I have never had anyone with real…real acute injuries like. [PN 10] |
| Concussion underdiagnosed or a reality of poor communication? | So, ehhh…luckily, we don’t really get too many of them; now, like that, I can; I can miss some as well just by not being on site too often. Ehmm…again, like I’ll go back to my old role of just turning up when, ehhh…when the, the rugby season is a little bit over. [PN 4] | |
| 4. Concussion Attitudes and Behaviours | Reaction to injury frequency of athletes-nature of sport? | Overall, there’s nearly always, have some kind of knock or a niggle or a strain… When we’re coming out off the back of matches ehmm to be honestly, injuries…they’re very varied… I’m always just always still, even in shock with these guys! Like, how can you cope with it like they’re just constantly in a state of basically recovery because they come out so beat and bruised from games. [PN 8] |
| Athletes blasé risky attitude–concussion | Oh yeah! I think they are very quick to dismiss…injuries, especially when, I suppose, there’s no, not that there’s no obvious symptoms of it. But you know, they’re not carrying their leg, for instance, or, you know? So, I definitely think they will try and mask it… I think your senior, more experienced players don’t do that as much, but I definitely think your younger players will do what they can to try and get back out… [PN 7] | |
| 5. Concussion Awareness Evident | Elite-level subjective injury ‘carrot’ proof protocol | …boxers when they’re dehydrated, looking at the SCAT test. So, we’ve actually used that as part of our showing them… Showing them that if they’re dehydrated, their response to the SCAT is actually a lot less. So, you know, we’ve…put that in place some years ago around, you know, trying to educate them, to show them… That if you cut back on your fluids or you dry out too quickly…the reason that they may be drying out too quickly is because they’re not following a better weight-making process. [PN 14] |
| Theme | Subtheme | Example Quote |
|---|---|---|
| 1. Awareness of Nutrition in Concussion Management | Poor awareness | Not too sure, really, just keep up the good habits. But I haven’t looked at it… Is there much? Is there much research on concussion and nutrition immediate or…? [PN 1] |
| Aware with limited knowledge | Yeah…yeah, I look; I’d be the first admit now I don’t… I know “X” and a few lads up in “x” are really interested in this area, and it’s it is really interesting! So, I’m kind of keeping an eye on creatine, fish oil supplementation, ehmm, and just to see the effects on recovery… If there’s anything there with creatine and fish oils. [PN 5] | |
| 2. Knowledge on the role of nutrition in concussion recovery | Acquired knowledge | Yeah, it’s; it’s an area I’m doing a bit of reading around at moment. But definitely, concussions are not that well-researched. But I think from what I have read, there’s a couple things you can do, and creatine, I believe, is important in the…not even the acute phase of, of, of having a concussion, but I think consistently for optimal cognition. [PN 2] |
| Personal led knowledge | …what would I implement with somebody else? I, I think, to be honest…the rest and the regular eating are…crucial and then… Whether, whether the extra probiotics or… Do you know whether they make that much of a difference? I don’t really know… But the anti-inflammatory, the protein, the carb, I think they would be crucial. Obviously, you know…you know your…your healthy fats as well. But the diet…the diet itself is probably the most important thing. [PN 11] | |
| Nutrition knowledge network | With regards to concussion, then we have two dietitians. One that actually has worked in rugby and who would I suppose work and are more familiar with the concussion side of things… [PN 13] | |
| Expertise in nutrition risk | …if you look at concussions, like concussion, is like shortage of energy in the brain at the time of impact, so…you could, like. I’d broadly say it to people, you know…’just to make sure you eat enough during this time, and kind of, you know’, were kind of very basic interventions, but nothing, I don’t think we ever…got to a stage where we were comfortable giving nutrition advice to someone who was concussed because there was stuff out there on creatine and stuff on there, high dose DHA, but we never…never formalised that to a policy. [PN 9] | |
| 3. Implementation—Nutrition post-concussion | Implementation with uncertainty | Ehmm, so I’m kind of keeping an eye on creatine, fish oil supplementation…and just to see the effects on recovery…if there’s anything there with creatine and fish oils. So, I would be kind of promoting or recommending to just keep those, the dosage on those… ehmm, keep including those if the lads have a concussion, and I would be in touch with the lads as well, like… …focus on the hydration. Keep on top of the omegas and the creatine. I’m not fully sure about the creatine yet, but they’re taking it anyway for other reasons and I think there could be? [PN 5] |
| Focused energy/symptom management | …one of the players who had been concussed had two in four weeks and was, you know, quite nauseous, wasn’t able to eat a lot. So, it was more around I suppose having smaller meals, more frequently liquid, a lot of liquid meals and stuff… I just didn’t really feel like it was settling him, but obviously, we are still, I suppose, were trying to get back to where he needs to be and be ready for when they get the go ahead to go back and train… So tried to ensure energy levels were kept up just through kind of liquid-based meals, small little snacks, nothing that was going to cause… stomach aggravation… So, it was more kind of in that, you know, couple days after… after the knock as opposed to long term [PN 7] | |
| Strategically blocked collaborative athlete support | I try to do it in smaller focuses instead of bombarding them all at once… So, let’s say they initially we try to break down even with the physios; we’d break down their rehab into, like, phases… So, the initial being, their protection phase, for example… I try row in with that being with ‘this is your initial focus’ instead of trying to bombard them with loads. Saying, ‘this is what I really want to get out of this block’, and then we tried to do it in focus. [PN 8] | |
| Supplementation–refocus | …if they do get a concussion, I kind of re-emphasise that. I’ll be like, you know… for some, not everyone will take fish oils ehmm, even though they have done… So, I’ll re-emphasise that you should be taking fish oils, and I’ll even tell them to load creatine and during that period… [PN 12] | |
| Dietary fat intake | your brain tissues are very, very reliant on kind of fat as its main fuel source… in terms of kind of recovery… So, a big, big focus on kind of their healthy omega 3s, and a reduction in obviously their pro-inflammatory omega 6s [PN 6] | |
| 4. Potential barrier | 1. athletes’ attitudes | I would say that the physical ones… they are probably more… (shaking head) open to the fact that nutrition can play (emphasised tone) a role immediately… Whereas the likes of the concussions, as you said, like it’s not visible… So maybe a little bit more towards the towards the physical ones… [PN 17] |
| 2. athletes’ nutrition adherence | …they are obviously fine, but like they… Well, see, I don’t know if that they are actually taken it! But the guys who have been concussed recently… I definitely know one of them 100% was because he was looking for more creatine and everything, you know because he was loading up on it… [PN 12] | |
| 5. Novel nutrition protocol implementation post-concussion | Acute creatine intake | Again, I’ve done a little bit of research into it, and there is a small bit around concussion and creatine. [PN 8] Yeah. [E.F.] So, a lot of our athletes would take creatine. But if they haven’t or around a concussion, potentially increasing that creatine intake, ehmm… In that period of concussion, to help with that energy availability side of things. Ehmm, if the brain can’t fully use their glucose efficiently. So, I have trialled that; again, there was a little bit of research around it. But ehmm, aside from that, no there is nothing else. [PN 8] |
| Carbohydrate-energy availability | Matthew Frakes is a researcher in Pittsburgh. I think he spoke about the energy availability and that like they compared guys that I don’t know-was it like 4 or 500 g of carbs in the 5 days, after concussion versus the guys that had a low carbohydrate diet and the symptoms for the guys that had more carbohydrates were got back to baseline that bit quicker. So, that’s kind of something I have been doing; it’s like, well, if a guy is in a gradual return to play protocol, then can you eat enough food? [PN 2] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finnegan, E.; Daly, E.; Ryan, L. Nutritional Considerations of Irish Performance Dietitians and Nutritionists in Concussion Injury Management. Nutrients 2024, 16, 497. https://doi.org/10.3390/nu16040497
Finnegan E, Daly E, Ryan L. Nutritional Considerations of Irish Performance Dietitians and Nutritionists in Concussion Injury Management. Nutrients. 2024; 16(4):497. https://doi.org/10.3390/nu16040497
Chicago/Turabian StyleFinnegan, Emma, Ed Daly, and Lisa Ryan. 2024. "Nutritional Considerations of Irish Performance Dietitians and Nutritionists in Concussion Injury Management" Nutrients 16, no. 4: 497. https://doi.org/10.3390/nu16040497
APA StyleFinnegan, E., Daly, E., & Ryan, L. (2024). Nutritional Considerations of Irish Performance Dietitians and Nutritionists in Concussion Injury Management. Nutrients, 16(4), 497. https://doi.org/10.3390/nu16040497