
Assessing Acceptability: The Role of Understanding Participant, Neighborhood, and Community Contextual Factors in Designing a Community-Tailored Cooking Intervention

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Data Collection and Procedures
2.4. Thematic Analysis
2.5. Validation Interviews by Participants
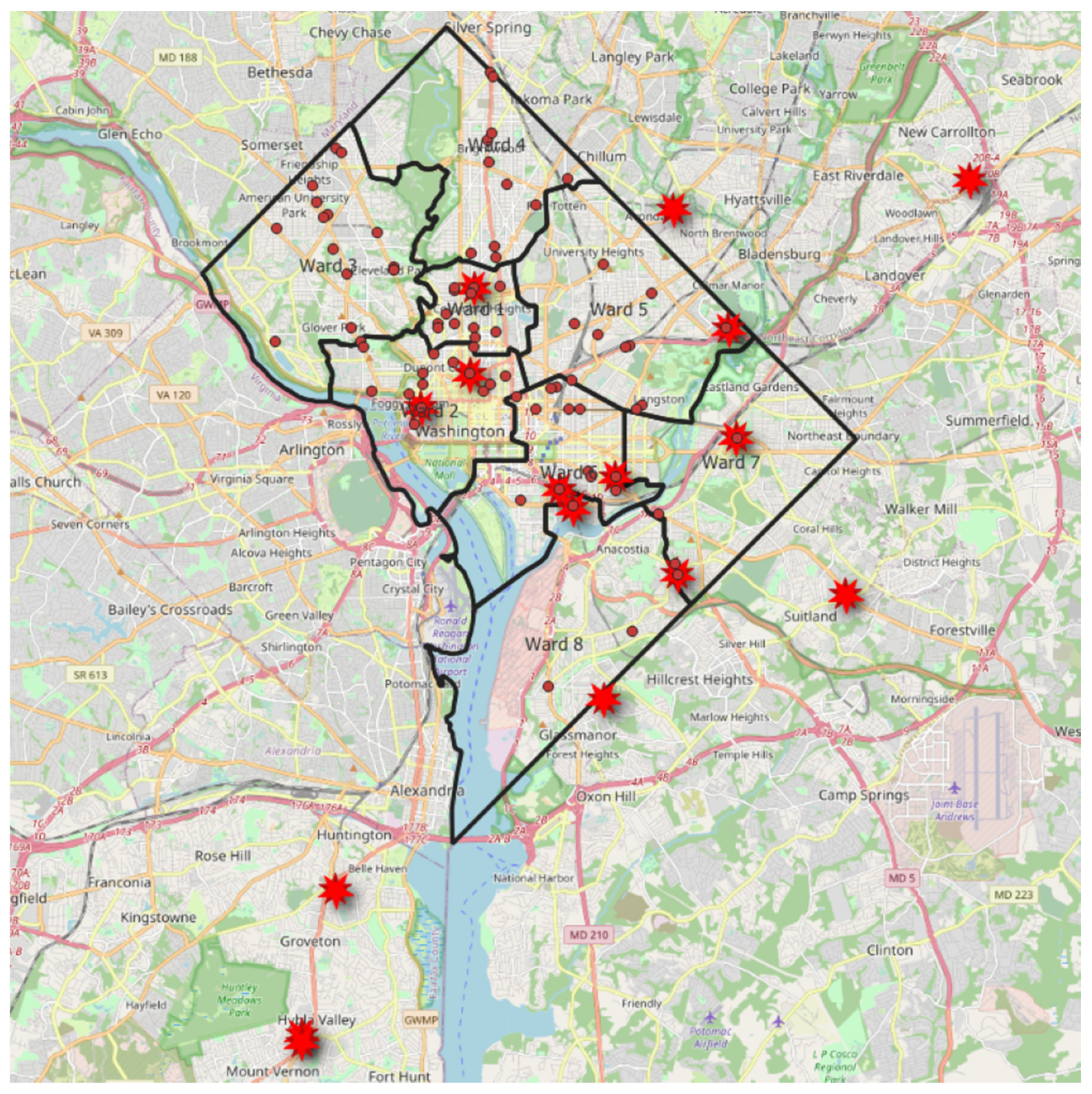
2.6. Construction of Participant-Identified Food Shopping Locations
2.7. Quantitative Data Analysis
3. Results
3.1. Survey Results
3.2. Qualitative Results
3.3. Barriers to Home Cooking
3.4. Motivators to Home Cooking
3.5. Strategies for Home Cooking
3.6. Neighborhood Factors
3.7. Acceptability of the Intervention
3.8. Participant Check-in Validation Interview Results
4. Discussion
4.1. Comparison of Our Findings with the Established Literature
4.2. Implications for Future Cooking Intervention Community Studies
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994, Erratum in Lancet 2019, 393, 132; Erratum in Lancet 2019, 393, e44. [Google Scholar] [CrossRef]
- Li, Y.; Xia, P.-F.; Geng, T.-T.; Tu, Z.-Z.; Zhang, Y.-B.; Yu, H.-C.; Zhang, J.-J.; Guo, K.; Yang, K.; Liu, G.; et al. Trends in Self-Reported Adherence to Healthy Lifestyle Behaviors Among US Adults, 1999 to March 2020. JAMA Netw. Open 2023, 6, e2323584. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, J.A.; Leung, C.W.; Richardson, C.R. More frequent cooking at home is associated with higher Healthy Eating Index-2015 score. Public Health Nutr. 2020, 23, 2384–2394. [Google Scholar] [CrossRef] [PubMed]
- Farmer, N.; Wallen, G.R.; Yang, L.; Middleton, K.R.; Kazmi, N.; Powell-Wiley, T.M. Household Cooking Frequency of Dinner Among Non-Hispanic Black Adults is Associated with Income and Employment, Perceived Diet Quality and Varied Objective Diet Quality, HEI (Healthy Eating Index): NHANES Analysis 2007–2010. Nutrients 2019, 11, 2057. [Google Scholar] [CrossRef] [PubMed]
- Reicks, M.; Gold, A.; Tran, N.; LeBlanc, K. Impacts of A Taste of African Heritage: A Culinary Heritage Cooking Course. J. Nutr. Educ. Behav. 2022, 54, 388–396. [Google Scholar] [CrossRef]
- Greenlee, H.; Gaffney, A.O.; Aycinena, A.C.; Koch, P.; Contento, I.; Karmally, W.; Richardson, J.M.; Lim, E.; Tsai, W.Y.; Crew, K.; et al. ¡Cocinar Para Su Salud!: Randomized Controlled Trial of a Culturally Based Dietary Intervention among Hispanic Breast Cancer Survivors. J. Acad. Nutr. Diet. 2015, 115, S42–S56.e3. [Google Scholar] [CrossRef]
- Condrasky, M.D.; Baruth, M.; Wilcox, S.; Carter, C.; Jordan, J.F. Cooks training for Faith, Activity, and Nutrition project with AME churches in SC. Eval. Program Plan. 2013, 37, 43–49. [Google Scholar] [CrossRef]
- Schoenberg, N.E.; Howell, B.M.; Swanson, M.; Grosh, C.; Bardach, S. Perspectives on healthy eating among Appalachian residents. J. Rural. Health 2013, 29, s25–s34. [Google Scholar] [CrossRef]
- Garcia, T.; Ford, B.; Pike, D.; Bryce, R.; Richardson, C.; Wolfson, J.A. Development and implementation of a community health centre-based cooking skills intervention in Detroit, MI. Public Health Nutr. 2021, 24, 549–560. [Google Scholar] [CrossRef]
- Lichtenstein, A.H.; Appel, L.J.; Vadiveloo, M.; Hu, F.B.; Kris-Etherton, P.M.; Rebholz, C.M.; Sacks, F.M.; Thorndike, A.N.; Van Horn, L.; Wylie-Rosett, J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 2021, 144, e472–e487. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, J.; Jacobs, A.G.; Ortiz, S.; Diaz Rios, L.K. A Systematic Review of Literature on the Representation of Racial and Ethnic Minority Groups in Clinical Nutrition Interventions. Adv. Nutr. 2022, 13, 1505–1528. [Google Scholar] [CrossRef]
- Tewahade, S.; Berrigan, D.; Slotman, B.; Stinchcomb, D.G.; Sayer, R.D.; Catenacci, V.A.; Ostendorf, D.M. Impact of the built, social, and food environment on long-term weight loss within a behavioral weight loss intervention. Obes. Sci. Pract. 2022, 9, 261–273. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M. Centering Patient Voices Through Community Engagement in Cardiovascular Research. Circulation 2023, 147, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Baumer, Y.; Baah, F.O.; Baez, A.S.; Farmer, N.; Mahlobo, C.T.; Pita, M.A.; Potharaju, K.A.; Tamura, K.; Wallen, G.R. Social Determinants of Cardiovascular Disease. Circ. Res. 2022, 130, 782–799. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Lachance, L.L.; Schulz, A.J.; Mentz, G.; Kannan, S.; Ridella, W. Neighborhood retail food environment and fruit and vegetable intake in a multiethnic urban population. Am. J. Health Promot. 2009, 23, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Castelo, A.F.M.; Schäfer, M.; Silva, M.E. Food practices as part of daily routines: A conceptual framework for analysing networks of practices. Appetite 2021, 157, 104978. [Google Scholar] [CrossRef] [PubMed]
- Raber, M.; Wolfson, J. The Challenging Task of Measuring Home Cooking Behavior. J. Nutr. Educ. Behav. 2021, 53, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.; White, M.; Brown, H.; Wrieden, W.; Kwasnicka, D.; Halligan, J.; Robalino, S.; Adams, J. Health and social determinants and outcomes of home cooking: A systematic review of observational studies. Appetite 2017, 111, 116–134. [Google Scholar] [CrossRef] [PubMed]
- Gooding, K.; Phiri, M.; Peterson, I.; Parker, M.; Desmond, N. Six dimensions of research trial acceptability: How much, what, when, in what circumstances, to whom and why? Soc. Sci. Med. 2018, 213, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Casale, M.; Somefun, O.; Haupt Ronnie, G.; Desmond, C.; Sherr, L.; Cluver, L. A conceptual framework and exploratory model for health and social intervention acceptability among African adolescents and youth. Soc. Sci. Med. 2023, 326, 115899. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef]
- Reimers, T.M.; Wacker, D.P. Parents’ Ratings of the Acceptability of Behavioral Treatment Recommendations Made in an Outpatient Clinic: A Preliminary Analysis of the Influence of Treatment Effectiveness. Behav. Disord. 1988, 14, 7–15. [Google Scholar] [CrossRef]
- Yingling, L.R.; Brooks, A.T.; Wallen, G.R.; Peters-Lawrence, M.; McClurkin, M.; Cooper-McCann, R.; Wiley, K.L., Jr.; Mitchell, V.; Saygbe, J.N.; Johnson, T.D.; et al. Community engagement to optimize the use of web-based and wearable technology in a cardiovascular health and needs assessment study: A mixed methods approach. JMIR mHealth uHealth 2016, 4, e38. [Google Scholar] [CrossRef]
- Thomas, S.; Yingling, L.; Adu-Brimpong, J.; Mitchell, V.; Ayers, C.R.; Wallen, G.R.; Powell-Wiley, T.M. Mobile health technology can objectively capture physical activity (PA) targets among African-American women within resource-limited communities—The Washington, DC cardiovascular health and needs assessment. J. Racial Ethn. Health Disparities 2017, 4, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Farmer, N.; Powell-Wiley, T.M.; Middleton, K.R.; Roberson, B.; Flynn, S.; Brooks, A.T.; Kazmi, N.; Mitchell, V.; Collins, B.; Hingst, R.; et al. A community feasibility study of a cooking behavior intervention in African-American adults at risk for cardiovascular disease: DC COOKS (DC Community Organizing for Optimal culinary Knowledge Study) with heart. Pilot Feasibility Stud. 2020, 6, 158. [Google Scholar] [CrossRef]
- Farmer, N.; Tuason, R.T.; Kazmi, N.; Flynn, S.; Mitchell, V.; Middleton, K.; Cox, R.; Franklin, K.; Gordon, T.; Baginski, A.; et al. Going virtual during the COVID-19 pandemic: Adaptation of a mixed-methods dietary behavior study within a community-based participatory research study of African-American adults at risk for cardiovascular disease. BMC Med. Res. Methodol. 2022, 22, 330. [Google Scholar] [CrossRef] [PubMed]
- D.C. Health Matters, Ward 7. Available online: https://www.dchealthmatters.org/demographicdata?id=131494 (accessed on 1 January 2024).
- D.C. Health Mattes, Ward 8. Available online: https://www.dchealthmatters.org/demographicdata?id=131495 (accessed on 1 January 2024).
- King, C.J.; Buckley, B.O.; Maheshwari, R.; Griffith, D.M. Race, Place, And Structural Racism: A Review Of Health And History in Washington, D.C. Health Aff. 2022, 41, 273–280. [Google Scholar] [CrossRef]
- DC Health Department Report. Obesity in the District of Columbia. 2014. Available online: https://dchealth.dc.gov/publication/obesity-report-2014 (accessed on 1 February 2023).
- Farmer, N.; Powell-Wiley, T.M.; Middleton, K.R.; Brooks, A.T.; Mitchell, V.; Troncoso, M.; Ceasar, J.; Claudel, S.E.; Andrews, M.R.; Kazmi, N.; et al. Use of a focus group-based cognitive interview methodology to validate a cooking behavior survey among African-American adults. Front. Nutr. 2022, 9, 1000258. [Google Scholar] [CrossRef] [PubMed]
- Ames, N.J.; Peng, C.; Powers, J.H.; Leidy, N.K.; Miller-Davis, C.; Rosenberg, A.; VanRaden, M.; Wallen, G.R. Beyond intuition: Patient fever symptom experience. J. Pain Symptom Manag. 2013, 46, 807–816. [Google Scholar] [CrossRef]
- Open Data DC. Available online: https://opendata.dc.gov/ (accessed on 1 February 2023).
- Lavelle, F.; McGowan, L.; Hollywood, L.; Surgenor, D.; McCloat, A.; Mooney, E.; Caraher, M.; Raats, M.; Dean, M. The development and validation of measures to assess cooking skills and food skills. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 118. [Google Scholar] [CrossRef]
- United States Department of Agriculture Household Food Security Module. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-u-s/survey-tools/#household (accessed on 1 February 2023).
- Lahne, J.; Wolfson, J.A.; Trubek, A. Development of the Cooking and Food Provisioning Action Scale (CAFPAS): A new measurement tool for individual cooking practice. Food Qual. Prefer. 2017, 62, 96–105. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Ramsing, R.; Richardson, C.R.; Palmer, A. Barriers to healthy food access: Associations with household income and cooking behavior. Prev. Med. Rep. 2019, 13, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Bisogni, C.A.; Jastran, M.; Shen, L.; Devine, C.M. A biographical study of food choice capacity: Standards, circumstances, and food management skills. J. Nutr. Educ. Behav. 2005, 37, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Blake, C.E.; Bisogni, C.A.; Sobal, J.; Jastran, M.; Devine, C.M. How adults construct evening meals. Scripts for food choice. Appetite 2008, 51, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Widener, M.J.; Smith, L.G.; Farber, S.; Gesink, D.; Minaker, L.M.; Patterson, Z.; Larsen, K.; Gilliland, J. Who’s cooking tonight? A time-use study of coupled adults in Toronto, Canada. Time Soc. 2022, 31, 480–507. [Google Scholar] [CrossRef] [PubMed]
- Laila, A.; Leme, A.C.; Hou, S.; Ma, D.W.L.; Haines, J. Perceived challenges and strategies to achieve Canada’s Food Guide recommendation to “Cook more often”: Findings from parents of young children. Appetite 2023, 182, 106413. [Google Scholar] [CrossRef]
- Utter, J.; Larson, N.; Berge, J.M.; Eisenberg, M.E.; Fulkerson, J.A.; Neumark-Sztainer, D. Family meals among parents: Associations with nutritional, social and emotional wellbeing. Prev Med. 2018, 113, 7–12. [Google Scholar] [CrossRef]
- Ashby, S.; Kleve, S.; McKechnie, R.; Palermo, C. Measurement of the dimensions of food insecurity in developed countries: A systematic literature review. Public Health Nutr. 2016, 19, 2887–2896. [Google Scholar] [CrossRef]
- Bartelmeß, T.; Jasiok, S.; Kühnel, E.; Yildiz, J. A scoping review of the social dimensions in food insecurity and poverty assessments. Front. Public Health 2022, 10, 994368. [Google Scholar] [CrossRef]
- Bader, M.D.M.; Purciel, M.; Yousefzadeh, P.; Neckerman, K.M. Disparities in Neighborhood Food Environments: Implications of Measurement Strategies. Econ. Geogr. 2010, 86, 409–430. Available online: http://www.jstor.org/stable/40929682 (accessed on 14 November 2023). [CrossRef]
- Gie, S.; Borthwick, F. Gentrification and Food Environments: A Rapid Evidence Assessment. medRxiv 2013. medRxiv:2023.03.07.23286919. [Google Scholar] [CrossRef]
- Ong, V.; Skinner, K.; Minaker, L.M. Life stories of food agency, health, and resilience in a rapidly gentrifying urban centre: Building a multidimensional concept of food access. Soc. Sci. Med. 2021, 280, 114074. [Google Scholar] [CrossRef]
- Tran, L.D.; Rice, T.H.; Ong, P.M.; Banerjee, S.; Liou, J.; Ponce, N.A. Impact of gentrification on adult mental health. Health Serv. Res. 2020, 55, 432–444. [Google Scholar] [CrossRef]
- Hines, A.L.; Brody, R.; Zhou, Z.; Collins, S.V.; Omenyi, C.; Miller, E.R., 3rd; Cooper, L.A.; Crews, D.C. Contributions of Structural Racism to the Food Environment: A Photovoice Study of Black Residents With Hypertension in Baltimore, MD. Circ Cardiovasc. Qual Outcomes 2022, 15, e009301. [Google Scholar] [CrossRef]
- Lillquist, S.; Ruiz Barnecett, G.; Flexman, N.; Mikati, N. Recipes for Health: A Community-Based Nutrition and Culinary Intervention. Cureus 2022, 14, e32322. [Google Scholar] [CrossRef]
- Sharma, S.V.; McWhorter, J.W.; Chow, J.; Danho, M.P.; Weston, S.R.; Chavez, F.; Moore, L.S.; Almohamad, M.; Gonzalez, J.; Liew, E.; et al. Impact of a Virtual Culinary Medicine Curriculum on Biometric Outcomes, Dietary Habits, and Related Psychosocial Factors among Patients with Diabetes Participating in a Food Prescription Program. Nutrients 2021, 13, 4492. [Google Scholar] [CrossRef] [PubMed]
- Carman, K.; Sweeney, L.H.; House, L.A.; Mathews, A.E.; Shelnutt, K.P. Acceptability and Willingness to Pay for a Meal Kit Program for African American Families with Low Income: A Pilot Study. Nutrients 2021, 13, 2881. [Google Scholar] [CrossRef] [PubMed]
- D.C. Policy Center. Food Access in D.C is Deeply Connected to Poverty and Transportation. 2019. Available online: https://www.dcpolicycenter.org/publications/food-access-dc-deeply-connected-poverty-transportation/ (accessed on 1 January 2024).
- Ayala, G.X.; Elder, J.P. Qualitative methods to ensure acceptability of behavioral and social interventions to the target population. J. Public Health Dent. 2011, 71, S69–S79. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | |
|---|---|
| Age | 60.3 (9.3) |
| Sex (%) | n (%) |
| Female | 20 (100) |
| Annual household income | n (%) |
| ≤$29,999 | 7 (35) |
| $30,000–$69,999 | 6 (30) |
| ≥$70,000 | 7 (35) |
| Household size | 1.8 (1.4) |
| Weekly frequency of cooking dinner | 4.0 (2.4) |
| Food skill score | 47.4 (10.8) |
| Cooking skill score | 29.8 (6.1) |
| Cardiovascular risk factor (* not mutually exclusive) | n (%) |
| Obesity/overweight | 18 (90) |
| Hyperlipidemia | 9 (45) |
| Hypertension/pre-Hypertension | 14 (70) |
| Type 2 diabetes/pre-diabetes | 4 (20) |
| Current or prior smoker (any type) | 8 (40) |
| Employment status | n (%) |
| Full-time | 5 (25) |
| Part-time | 2 (10) |
| Unemployed | 3 (15) |
| Retired | 10 (50) |
| Marital status | n (%) |
| Married | 10 (50) |
| Single | 4 (20) |
| Divorced/widowed | 6 (30) |
| Education status | n (%) |
| Some college education and below | 5 (25) |
| College degree | 8 (40) |
| Graduate or post-graduate degree | 7 (35) |
| Food security status | n (%) |
| Full food security | 14 (70) |
| Marginal food security | 3 (15) |
| Low food security | 1 (5) |
| Very low food security | 2 (10) |
| Personal transportation access | n (%) |
| Drive | 14 (70) |
| Not drive | 6 (30) |
| Age, started to cook | 13 (3.9) |
| Use of batch cooking at home ** | n (%) |
| Yes | 12 (60) |
| No | 8 (40) |
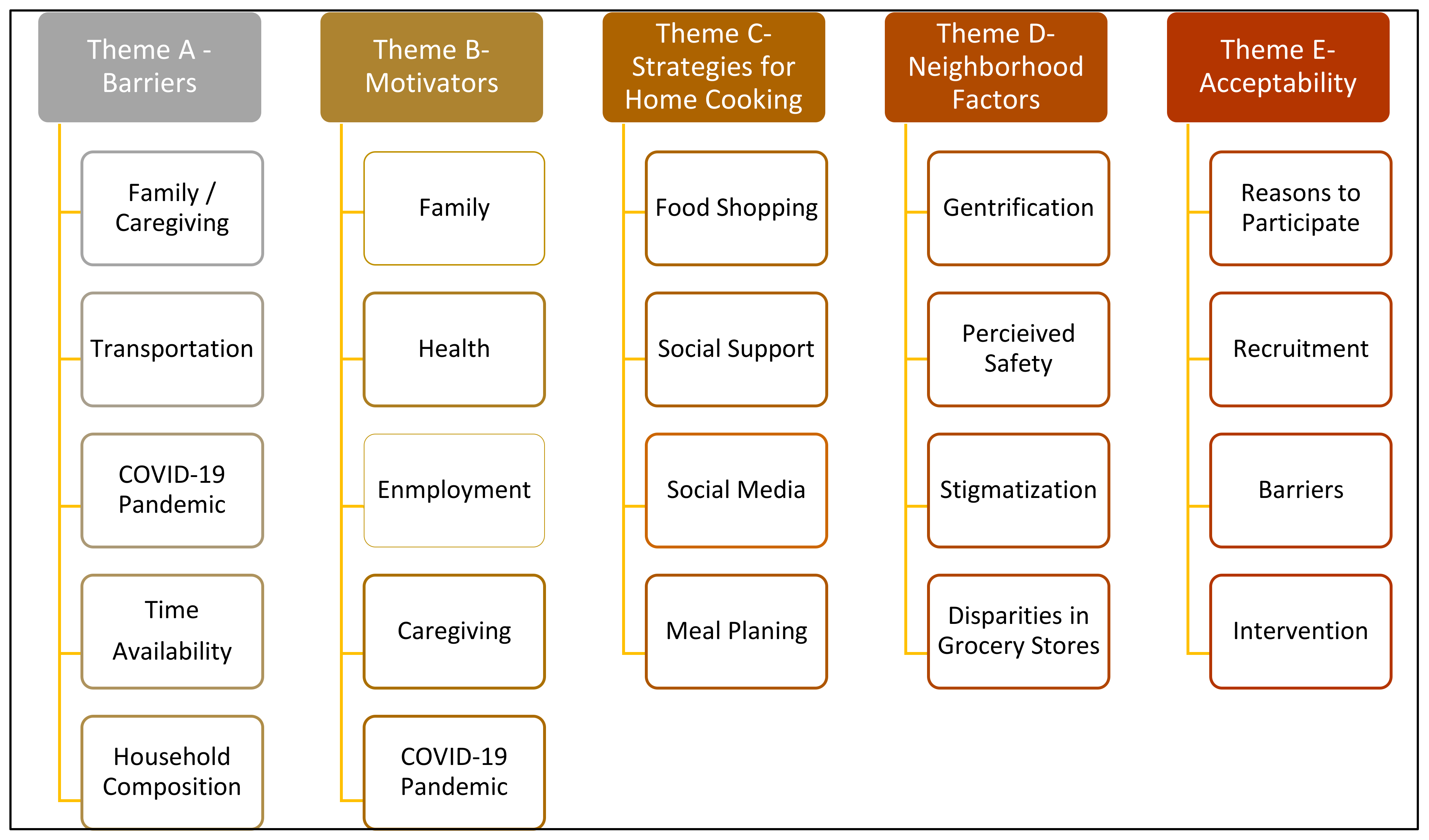
| Theme A: Barriers to Home Cooking | ||||
|---|---|---|---|---|
| A1: Family and Caregiving “I was saying, for me, there are some challenges. The first is I have young kids. And so, it’s a time and energy. Sometimes I’m just like tired. And in particular since the pandemic and being home with the kids all the time, I’m feeling like I am always in the kitchen.” | A2: Transportation “By the time you go to the store and get back, I feel like—you might not feel like cooking what you planned on cooking”…“That might happen, maybe, I would say, within a week, I am going. maybe once out of a week. Seven days, once out of the week. I catch the bus, two bus—more so two buses, yes. Maybe we’ll go down the street to safeway and bring it on the bus. And it’s what I planned to eat that day, you know, and I just don’t feel like it.” “With me, before and during the pandemic, uhm getting to the stores because I don’t drive. So, therefore, you know, even walking, catching the bus, and get into particular stores that I want to go to where I will have that ask someone to take me.” | A3: COVID-19 Pandemic “Like why is somebody always asking me (to cook)—like the worst question you can ask me, especially if I didn’t have a plan is what’s for lunch or what’s for dinner. Didn’t I just feed you? They’re like no. I just fed you. I was just in the kitchen, yeah. So, that has been extremely challenging, very frustrating.” | A4: Time Availability “By the time I’m coming to cook, it’s like—and even when I go to Costco, I usually bring a pizza home, I’m not even going to lie. Because you’ve done all that work. We all know. [unintelligible] the job, the planning, the getting the stuff, standing in line. Then, by the time you get home, it’s like, I’ve got to put these together to make a meal? [laugh]” “But with my timing and if I haven’t cooked by, have dinner ready by 5:00 you can forget it. You better be on your way out to get something.” | A5: Household Composition “Because eating by yourself, I don’t have any problems with it, but I think I would be more apt to cook if, it was more than just me. You know, because I waste a lot of food, too. Because a lot of times, I can’t really prepare for one. Sometimes, depending on what you’re cooking, for example, spaghetti. Not that I make a huge pot of what I make. (But) after two times, I’m done. I really don’t think about freezing and that kind of thing.” |
| Theme B: Motivators to Home Cooking | ||||
| B1: Family and Sharing “As much as I do enjoy cooking, it’s not about the cooking per se. The enjoyment comes from cooking food that other people enjoy and appreciate. So, I don’t know if I love cooking as much as I do love cooking for people who are like foodies, who are going to appreciate like, “Oh man, I can taste this,” or like people who can get into the experience of the food with me is more enjoyable than just cooking. Like the art of it to me is both the cooking and the partaking of the meal.” | B2: Health “Because when you’re cooking at home, you know what’s coming, it’s not just flavor, but if you have high blood pressure, you’re always monitoring your sodium intake. So, uhm, cooking at home, at least you know. At least you know what you’re putting in and stuff and so, yeah.” | B3: Enjoyment “For everything, you use your mind and your hands, and you know, it’s not about the measuring spoons when you cook, you know, you just have your own way of doing it and it still comes out right.” “You could create your own recipes, or you can modify like certain things I don’t eat, I may not put it in that particular dish, or, you know…, take something out, put something in, season it to your taste. Because most recipes have all the spices you’re supposed to use, I’ll add something a little different—lemon pepper versus regular pepper, something like that.” | B4: Caregiving “As much as I do enjoy cooking, it’s not about the cooking per se. The enjoyment comes from cooking food that other people enjoy and appreciate. So, I don’t know if I love cooking as much as I do love cooking for people who are like foodies, who are going to appreciate like, “Oh man, I can taste this,” or like people who can get into the experience of the food with me is more enjoyable than just cooking. Like the art of it to me is both the cooking and the partaking of the meal.” | B5: COVID-19 Pandemic “Since this pandemic, I kind of changed my outlook on cooking. I do more of it now than what I did in the past. I will cook probably three to four times a week, and I do more planning because that’s my biggest issue is planning. If I plan, I can do it.” |
| Theme C: Strategies for Home Cooking | ||||
| C1: Food Shopping “We’re living in Ward 7 with only one supermarket. And I have to go out of my neighborhood to go grocery shopping. Not that I don’t go to that place very occasionally but I hate to have to go out of my neighborhood but I do.” | C2: Social Support “So my friends, one of my ministers, we talk about sharing recipes. So we try each other’s recipes. And so that kind of motivates you to do something a little bit different.” | C3: Social Media “Well, another site for great recipes, Pinterest, they have a whole lot of good stuff there. One of my great favorite is the noodles and then I had a dish of um, like, a seven-bean um, salad. Once you cook your noodles and rinse them, and then add the seven-bean salad to it, and then heat it up at very low temperature and add your favorite sauce of any kind, it might be, for example, a chili, um green chili sauce. Oh, my husband just laid that out. ‘Oh, this was really good.’” | C4: Meal Planning “I just like to cook or I plan, even when I’m laying down thinking the next day of everything I need to do and how to ah… juggle it all, and… now with someone coming, they’re going wanna eat, so I cook.” | |
| Theme D: Neighborhood Factors | ||||
| D1: Gentrification “And the people that do care, there like they said, they just want to get our property and get (us) away. Like I say, it’s ridiculous how D.C. treats the people who were here when it was—the older people and the original people who were here, who stayed here through all of the mess and dealt with the foolishness and how they don’t look out for the people who are here.” | D2: Perceived Safety “I’m not going to lie, I’m nervous to get out the car. When I’m going to the neighborhood corner store, that would be for soda or something unhealthy. I’m looking for real groceries to feed my family.” | D3: Stigmatization “In this city, that’s what they think of Ward 7 and 8 and stigmatize it a lot.” (Referring to questions on a survey that were skipped by some participants). “Hypothetically, thinking, perhaps the reason why they were skipped is because that people have a lot of hidden agendas when you go into these neighborhoods. And like I said gentrification is here, and it’s real. And perhaps they don’t know who going to get hold to this information, this survey, and the reason why… But we don’t know where this information is going to go to. And people always have hidden agendas when you come into a community that’s full of Black and Brown people” | D4: Disparities in Grocery Stores “Yeah. It’s very true. Or even going, like she said, across the bridge. I work on 14th St. I shop at the (X Grocery store name) right there. It’s a total difference than when you go to Alabama Ave., which has its own issues. You don’t know if you’re going to honestly go in there and get robbed or shot or you’re going to come out with quality food or is it going to last.” | |
| Theme E: Acceptability of the Intervention | ||||
| E1: Reasons to Participate “I can think of quite a few people that would be interested in that. And, and it would be a good thing for those who want to change their health condition or health situation. So they can enjoy their food even more. And some people cook and they say they don’t like how their food tastes but they’d rather have someone else’s food.” “Ward 7 needs it. I’m concerned about my people. They need to stay out of McDonalds.” “I think would they enjoy… whoever is getting the class—they would enjoy learning how to cook different things.” | E2: Recruitment “I would also think about involving more people that are like young adults. We have children now. The other two ladies and myself, you know, we’re retired or, you know, older. So, our cooking may be different. But younger adults, young families, making sure that they have a better understanding of preparing nutritional meals for their children because I’m seeing—I have a friend that works in the school system and sometimes I go there to volunteer. And the children seem to not have an appreciation of the lunch, you know. They pick over things and then throw them away. You know, so, maybe more young adults with families.” | E3: Barriers “The costs typically associated with healthier food options. And that definitely can be a hindrance, it never make sense to me that the healthier food options cost more than the unhealthy stuff when, you know, it should be the flip side. And so, I guess I’d love as a part of this conversation or part of your study if we spent some time to get some like tricks to getting cost saving healthy items including produce organic, when necessary.” | E4: Intervention (Regarding the study)” Is it going to be face to face, or is it going to be virtual, and (what is) the time period that you are going to use?” (Referencing prior virtual cooking class) “And she (chef) out all the things that we need, she sent out the recipe that we were going to be cooking and whatever and she demonstrated and whatever, it was really good too, so. Because we was on Zoom and in our kitchen… And it was really good because you saw other people cooking and giving their feedback and whatever.” “Yes. I guess I assumed that either ingredients would be provided or gift card to get the items like a list of shopping items that we will have to get.” “I only have a kitchenette so—space, you know. That’s why I say, how simple would it be? Will I be all in the dining room, in the living room trying to be all over the place cooking because my kitchen is so small?” | |
| Component of Phase 2 D.C. COOKS | Summarized Suggestions from the Focus Groups | Planned Modifications | Related Participant Barrier, Motivator, or Strategy |
|---|---|---|---|
| Recipes | Provide nutritional information for recipes, including sodium content. Provide information on potentially unhealthful ingredients that people may use and showcase where more healthful options are used. Provide cost information. | Interventionist will provide information during classes highlighting healthful substitutions made within recipes compared with unhealthy ones. Nutritional information for recipes were planned but will be highlighted as part of the shared meal discussion during classes, including the use of organic foods. Cost information for ingredients will be provided in class. | Health concerns of participant and family members. Economic concerns directly from food pricing or from indirect costs related to traveling for food shopping. |
| Delivery of intervention | Provide in-person and virtual options for participants. | Hybrid design for classes will occur with three in-person and thre virtual classes. | Reduced barrier for time and transportation concerns to community site to promote the interest of family and household members. |
| Community site or setting | Choose location known to study participants and that is easily accessible. | Community kitchen site was discussed with participants during validation interviews and the majority of participants were knowledgeable of the site and agreed on its accessibility for those who have personal transportation. Transportation for those with personal needs will be provided to and from the community site. | Community support network as a motivator for cooking, with a reduction in transportation and safety. concerns. |
| Food supplies to participants | Provide ingredients for recipes and assist with the measured amounts needed. | Research team will utilize food pantry infrastructure within the community kitchen site to provide ingredients for virtual sessions. Recipes for these sessions were selected based on seasonal availability through the community site. The community site will be the pick-up location for ingredients for the three weeks of virtual classes. | Access and availability of foods and reducing the need to travel for ingredients. |
| Cooking behavior diaries | Understand the importance of motivators and barriers to cooking at home. | Questions asked through a diary regarding enjoyment, use of creativity, and people whom participants cooked with or for were added. | Inquire about participants’ stated motivators and barriers for cooking at home. |
| Grocery store receipts | Privacy and feasibility concerns regarding submitting food receipts to the research team due to many participants using electronic receipt phone applications. | Research questions will ask for a self-report of the prior 30-day food expenditures at grocery stores. | Avoid privacy and logistic issues reported by participants that would increase participant burden. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farmer, N.; Tuason, R.; Middleton, K.R.; Ude, A.; Tataw-Ayuketah, G.; Flynn, S.; Kazmi, N.; Baginski, A.; Mitchell, V.; Powell-Wiley, T.M.; et al. Assessing Acceptability: The Role of Understanding Participant, Neighborhood, and Community Contextual Factors in Designing a Community-Tailored Cooking Intervention. Nutrients 2024, 16, 463. https://doi.org/10.3390/nu16030463
Farmer N, Tuason R, Middleton KR, Ude A, Tataw-Ayuketah G, Flynn S, Kazmi N, Baginski A, Mitchell V, Powell-Wiley TM, et al. Assessing Acceptability: The Role of Understanding Participant, Neighborhood, and Community Contextual Factors in Designing a Community-Tailored Cooking Intervention. Nutrients. 2024; 16(3):463. https://doi.org/10.3390/nu16030463
Chicago/Turabian StyleFarmer, Nicole, Ralph Tuason, Kimberly R. Middleton, Assumpta Ude, Gladys Tataw-Ayuketah, Sharon Flynn, Narjis Kazmi, Alyssa Baginski, Valerie Mitchell, Tiffany M. Powell-Wiley, and et al. 2024. "Assessing Acceptability: The Role of Understanding Participant, Neighborhood, and Community Contextual Factors in Designing a Community-Tailored Cooking Intervention" Nutrients 16, no. 3: 463. https://doi.org/10.3390/nu16030463
APA StyleFarmer, N., Tuason, R., Middleton, K. R., Ude, A., Tataw-Ayuketah, G., Flynn, S., Kazmi, N., Baginski, A., Mitchell, V., Powell-Wiley, T. M., & Wallen, G. R. (2024). Assessing Acceptability: The Role of Understanding Participant, Neighborhood, and Community Contextual Factors in Designing a Community-Tailored Cooking Intervention. Nutrients, 16(3), 463. https://doi.org/10.3390/nu16030463