
Association Between Maternal Weight Perception Before and During Pregnancy and Postpartum Depression Status in Southern China

 and
and
Abstract
1. Introduction
2. Methods
2.1. Study Participants and Design
2.2. Processes of Data Acquisition
2.2.1. Maternal Actual Weight
- x1 = first trimester measured weight (kg);
- x2 = gestational age (days) at first weight measurement;
- x3 = height (cm);
- x4 = maternal age at conception (years);
- x5 = parity.
2.2.2. Maternal Weight Perception
2.2.3. PPD Status
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
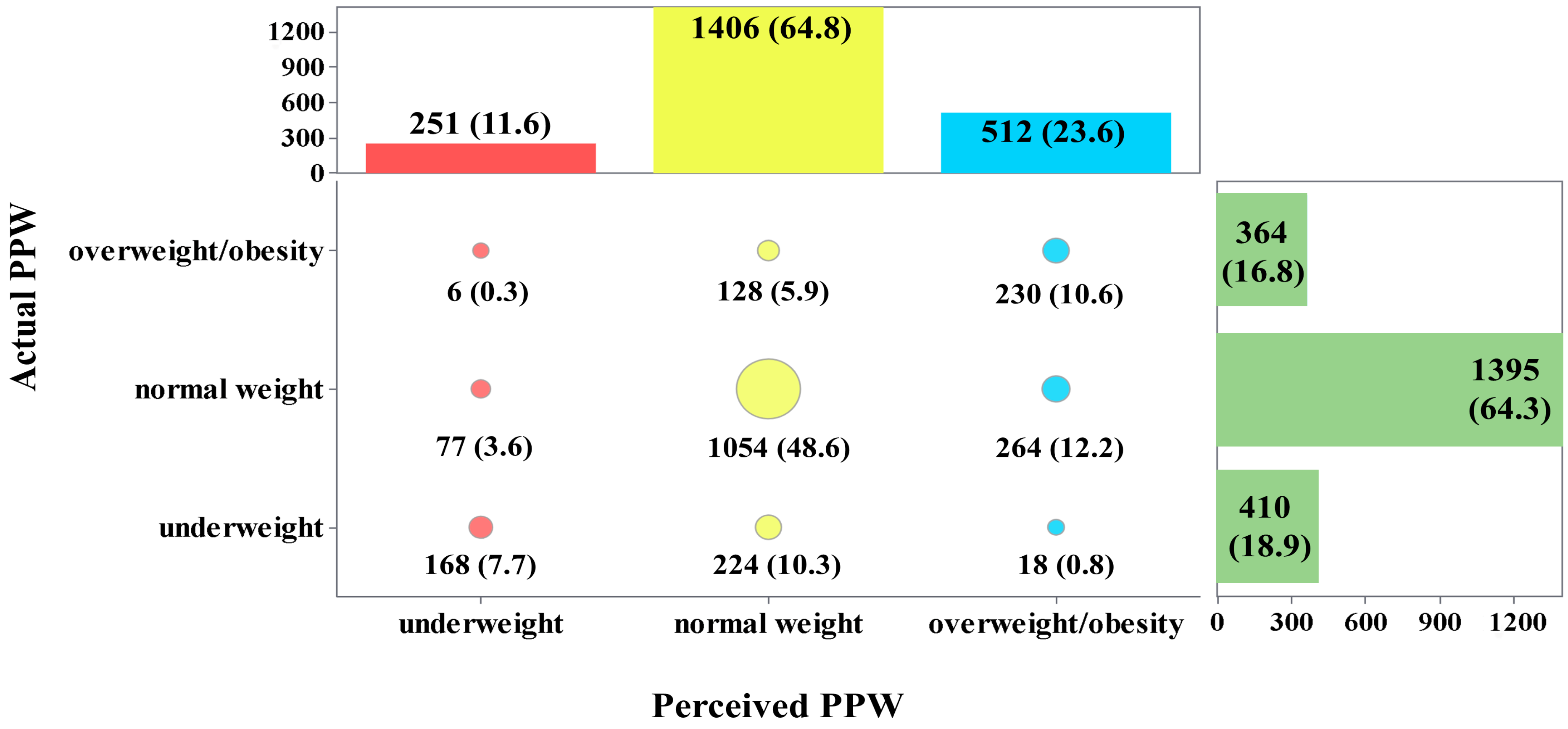
3.2. Agreements Between Maternal Actual and Perceived PPW
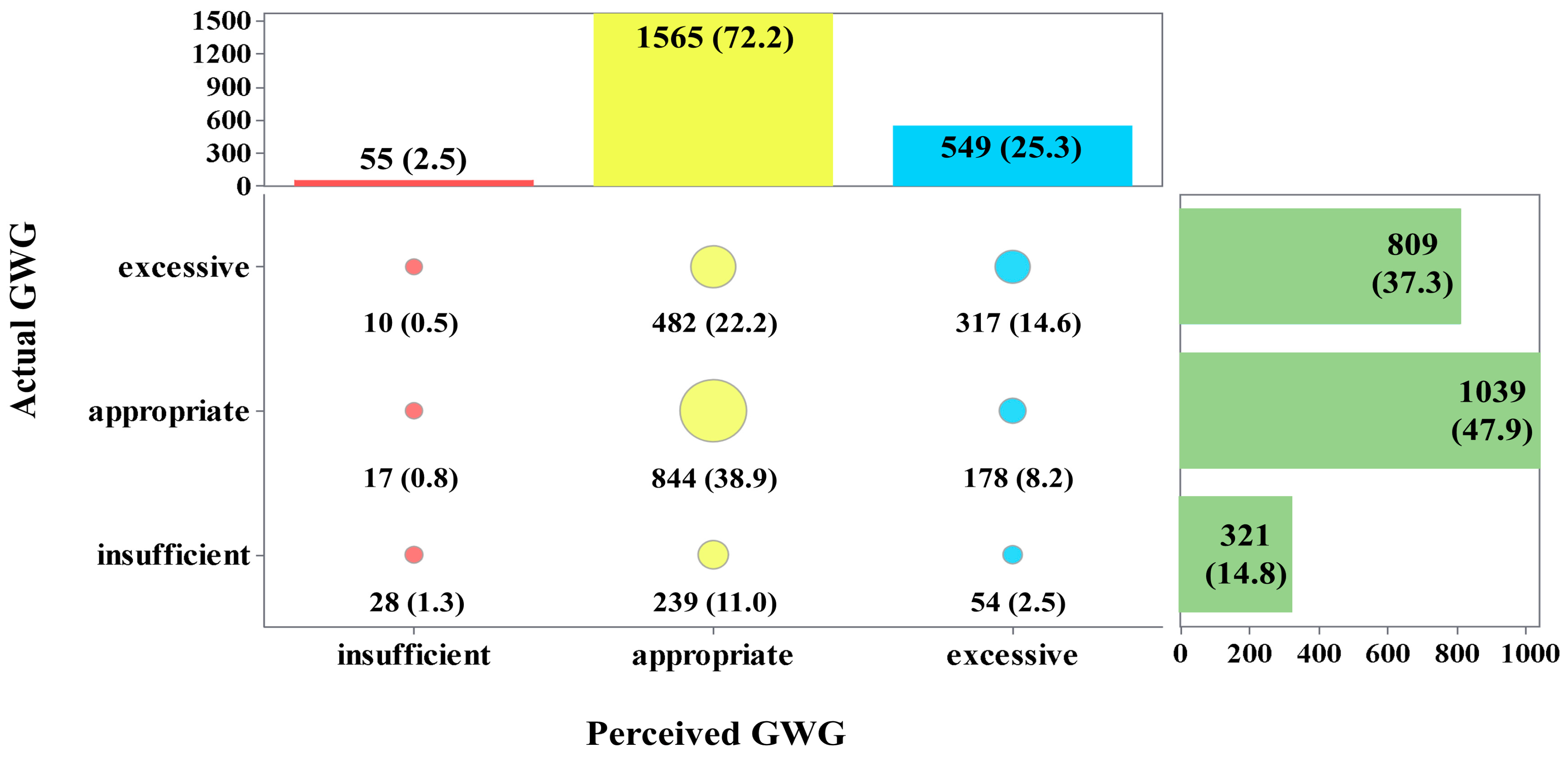
3.3. Agreements Between Maternal Actual and Perceived GWG
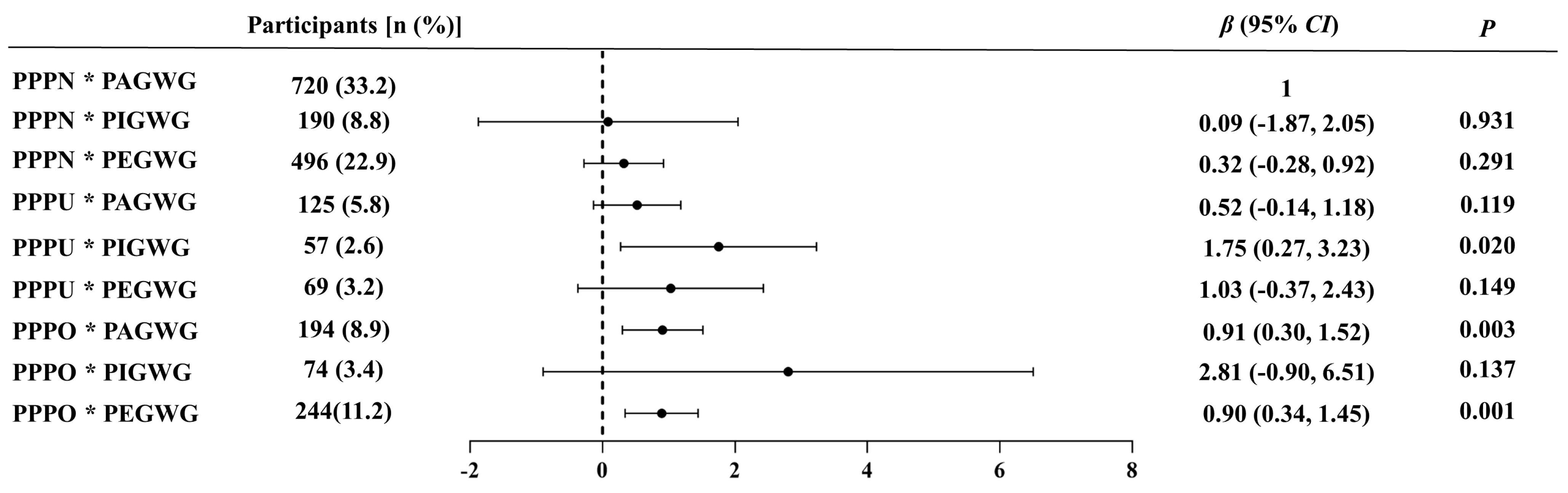
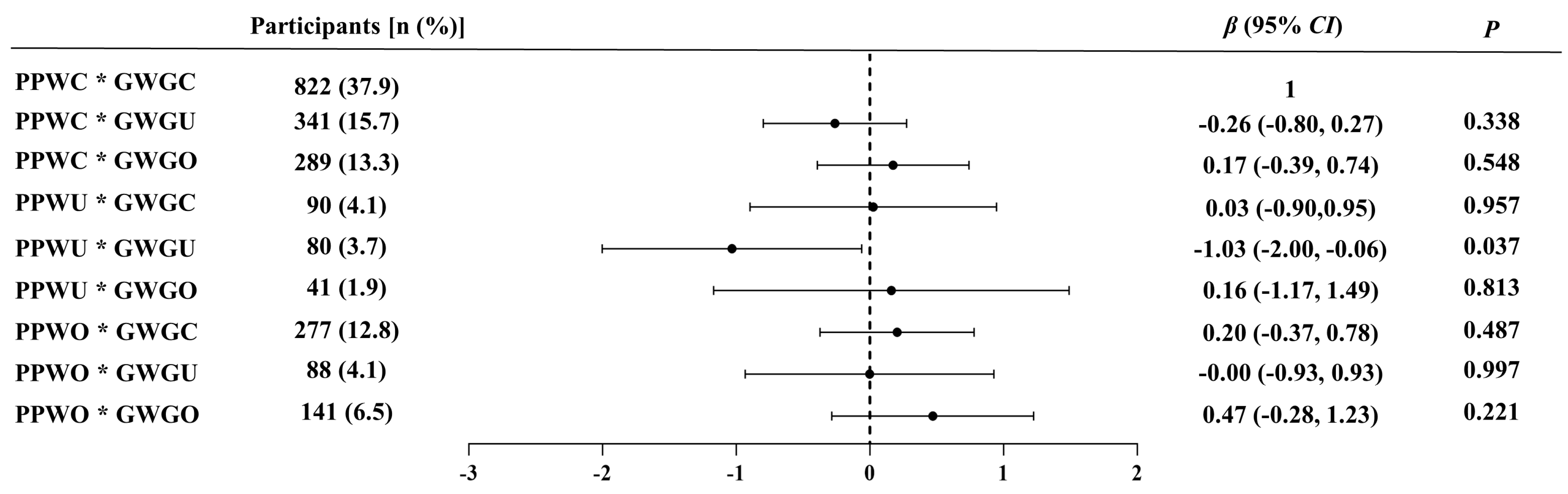
3.4. Preliminary Analysis of the Associations Between Perceived Bias in PPW or GWG and EPDS Scores
3.5. Adjusted Associations of Maternal Weight Perception with EPDS Scores
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bobo, W.V.; Yawn, B.P. Concise review for physicians and other clinicians: Postpartum depression. Mayo Clin. Proc. 2014, 89, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Yu, Y.; Li, J.; Liao, Q.; Zhou, W. Prevalence and influencing factors of postpartum depression in Chinese women: A meta-analysis. J. Mod. Med. Health 2023, 39, 3510–3515. [Google Scholar]
- Worthen, R.J.; Beurel, E. Inflammatory and neurodegenerative pathophysiology implicated in postpartum depression. Neurobiol. Dis. 2022, 165, 105646. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.; Wu, N.; Tu, Y.; Zang, T.; Bai, J.; Peng, G.; Liu, Y. Perinatal depression and infant and toddler neurodevelopment: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2024, 159, 105579. [Google Scholar] [CrossRef]
- Saharoy, R.; Potdukhe, A.; Wanjari, M.; Taksande, A.B. Postpartum Depression and Maternal Care: Exploring the Complex Effects on Mothers and Infants. Cureus 2023, 15, e41381. [Google Scholar] [CrossRef]
- Bloch, M.; Tevet, M.; Onn, R.; Fried-Zaig, I.; Aisenberg-Romano, G. The long-term course and prognosis of postpartum depression: A retrospective longitudinal cohort study. Arch. Women’s Ment. Health 2024, 27, 99–107. [Google Scholar] [CrossRef]
- Chithiramohan, T.; Eslick, G.D. Association Between Maternal Postnatal Depression and Offspring Anxiety and Depression in Adolescence and Young Adulthood: A Meta-Analysis. J. Dev. Behav. Pediatr. 2023, 44, e231–e238. [Google Scholar] [CrossRef]
- Takács, L.; Kandrnal, V.; Kaňková, Š.; Bartoš, F.; Mudrák, J. The effects of pre- and post-partum depression on child behavior and psychological development from birth to pre-school age: A protocol for a systematic review and meta-analysis. Syst. Rev. 2020, 9, 146. [Google Scholar] [CrossRef]
- Gruszka, W.; Owczarek, A.J.; Glinianowicz, M.; Bąk-Sosnowska, M.; Chudek, J.; Olszanecka-Glinianowicz, M. Perception of body size and body dissatisfaction in adults. Sci. Rep. 2022, 12, 1159. [Google Scholar] [CrossRef]
- Richmond, T.K.; Sonneville, K.R.; Milliren, C.E.; Thurston, I.B. Unraveling the meaning of weight misperception in a sample of college students: Unaware or body satisfied? Body Image 2022, 43, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Shabu, S.A.; Saka, M.H.; Boya, M.N.; Ahmed, H.M.; Zaki, S.M.; Hettinga, F.; Shabila, N.P. Association between body weight perception and actual body mass index among adult women in Erbil city, Iraq. J. Health Popul. Nutr. 2024, 43, 15. [Google Scholar] [CrossRef] [PubMed]
- Güven, A.; Özdede, M.; Çelik Eroğlu, B. Weight Misperception is Prevalent Among Turkish Adults and Associated with Higher Age, Body Mass Index and Lower Education Status. Diabetes Metab. Syndr. Obes. 2024, 17, 2831–2843. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Yu, X.; Tan, Y.; Yu, Z.; Zhu, J. Association between weight, weight perception, weight teasing and mental health among adolescents. Child Adolesc. Psychiatry Ment. Health 2024, 18, 39. [Google Scholar] [CrossRef] [PubMed]
- Kye, S.Y.; Park, K. Gender differences in factors associated with body weight misperception. Public Health Nutr. 2021, 24, 2483–2495. [Google Scholar] [CrossRef]
- Bergmeier, H.; Hill, B.; Haycraft, E.; Blewitt, C.; Lim, S.; Meyer, C.; Skouteris, H. Maternal body dissatisfaction in pregnancy, postpartum and early parenting: An overlooked factor implicated in maternal and childhood obesity risk. Appetite 2020, 147, 104525. [Google Scholar] [CrossRef]
- Edlund, K.; Johansson, F.; Lindroth, R.; Bergman, L.; Sundberg, T.; Skillgate, E. Body image and compulsive exercise: Are there associations with depression among university students? Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2022, 27, 2397–2405. [Google Scholar] [CrossRef]
- Satwik, R.; Sinha, D.; Tiwari, B. Prevalence of poor body image and its correlation with self-esteem and depression in middle-aged women. Climacteric 2024, 27, 202–209. [Google Scholar] [CrossRef]
- Park, E. Overestimation and Underestimation: Adolescents’ Weight Perception in Comparison to BMI-Based Weight Status and How It Varies Across Socio-Demographic Factors. J. Sch. Health 2011, 81, 57–64. [Google Scholar] [CrossRef]
- Tavakoli, M.; Hasanpoor-Azghady, S.B.; Farahani, L.A. Predictors of mothers’ postpartum body dissatisfaction based on demographic and fertility factors. BMC Pregnancy Childbirth 2021, 21, 8. [Google Scholar] [CrossRef]
- Roomruangwong, C.; Kanchanatawan, B.; Sirivichayakul, S.; Maes, M. High incidence of body image dissatisfaction in pregnancy and the postnatal period: Associations with depression, anxiety, body mass index and weight gain during pregnancy. Sex. Reprod. Healthc. 2017, 13, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-L.; Chang, S.-R. The relationship between body dissatisfaction and postpartum depressive symptoms: A cross-sectional study. J. Affect. Disord. 2023, 324, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Champion, M.L.; Harper, L.M. Gestational Weight Gain: Update on Outcomes and Interventions. Curr. Diabetes Rep. 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Montvignier Monnet, A.; Savoy, D.; Préaubert, L.; Hoffmann, P.; Bétry, C. In Underweight Women, Insufficient Gestational Weight Gain Is Associated with Adverse Obstetric Outcomes. Nutrients 2022, 15, 57. [Google Scholar] [CrossRef] [PubMed]
- Rokicki, S.; McGovern, M.; Von Jaglinsky, A.; Reichman, N.E. Depression in the Postpartum Year and Life Course Economic Trajectories. Am. J. Prev. Med. 2022, 62, 165–173. [Google Scholar] [CrossRef]
- Bradshaw, H.; Riddle, J.N.; Salimgaraev, R.; Zhaunova, L.; Payne, J.L. Risk factors associated with postpartum depressive symptoms: A multinational study. J. Affect. Disord. 2022, 301, 345–351. [Google Scholar] [CrossRef]
- Zedan, H.S.; Baattaiah, B.A.; Alashmali, S.; Almasaudi, A.S. Risk of Postpartum Depression: The Considerable Role of Maternal Health Status and Lifestyle. Healthcare 2023, 11, 2074. [Google Scholar] [CrossRef]
- Thomas, D.M.; Oken, E.; Rifas-Shiman, S.L.; Téllez-Rojo, M.; Just, A.; Svensson, K.; Deierlein, A.L.; Chandler-Laney, P.C.; Miller, R.C.; McNamara, C.; et al. Do Women Know Their Prepregnancy Weight? Obesity 2019, 27, 1161–1167. [Google Scholar] [CrossRef]
- Criteria of Weight for Adults. National Health Commission of the People’s Republic of China. 2014. Available online: http://www.nhc.gov.cn/zwgkzt/yingyang/201308/a233d450fdbc47c5ad4f08b7e394d1e8.shtml (accessed on 10 October 2024).
- Standard of Recommendation for Weight Gain During Pregnancy Period. National Health Commission of the People’s Republic of China. 2022. Available online: http://www.nhc.gov.cn/wjw/fyjk/202208/864ddc16511148819168305d3e576de9.shtml (accessed on 10 October 2024).
- Wang, Y.; Guo, X.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef]
- Hu, B.; Lin, L.F.; Zhuang, M.Q.; Yuan, Z.Y.; Li, S.Y.; Yang, Y.J.; Lu, M.; Yu, S.Z.; Jin, L.; Ye, W.M.; et al. Reliability and relative validity of three physical activity questionnaires in Taizhou population of China: The Taizhou Longitudinal Study. Public Health 2015, 129, 1211–1217. [Google Scholar] [CrossRef]
- Silverman, M.E.; Reichenberg, A.; Savitz, D.A.; Cnattingius, S.; Lichtenstein, P.; Hultman, C.M.; Larsson, H.; Sandin, S. The risk factors for postpartum depression: A population-based study. Depress. Anxiety 2017, 34, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Chen, W.-L.; Ma, L.; Jing, X.-Y.; Yuan, Z.-W.; Fan, J. Analysis of the correlation between general postpartum well-being and depression in primiparas: A cross-sectional study. Medicine 2024, 103, e37658. [Google Scholar] [CrossRef] [PubMed]
- Mori, E.; Tsuchiya, M.; Maehara, K.; Iwata, H.; Sakajo, A.; Tamakoshi, K. Fatigue, depression, maternal confidence, and maternal satisfaction during the first month postpartum: A comparison of Japanese mothers by age and parity. Int. J. Nurs. Pract. 2017, 23, e12508. [Google Scholar] [CrossRef] [PubMed]
- Ali, E. Women’s experiences with postpartum anxiety disorders: A narrative literature review. Int. J. Women’s Health 2018, 10, 237–249. [Google Scholar] [CrossRef]
- Putri, A.S.; Wurisastuti, T.; Suryaputri, I.Y.; Mubasyiroh, R. Postpartum Depression in Young Mothers in Urban and Rural Indonesia. J. Prev. Med. Public Health 2023, 56, 272–281. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, M. Postpartum depression and risk factors among working women one year after delivery in Beijing, China: A cross-sectional study. Front. Public Health 2024, 12, 1346583. [Google Scholar] [CrossRef]
- Nisar, A.; Yin, J.; Waqas, A.; Bai, X.; Wang, D.; Rahman, A.; Li, X. Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 1022–1037. [Google Scholar] [CrossRef]
- Matsumura, K.; Hamazaki, K.; Tsuchida, A.; Kasamatsu, H.; Inadera, H. Education level and risk of postpartum depression: Results from the Japan Environment and Children’s Study (JECS). BMC Psychiatry 2019, 19, 419. [Google Scholar] [CrossRef]
- Kołomańska-Bogucka, D.; Mazur-Bialy, A.I. Physical Activity and the Occurrence of Postnatal Depression—A Systematic Review. Medicina 2019, 55, 560. [Google Scholar] [CrossRef]
- Dipietro, L.; Evenson, K.R.; Bloodgood, B.; Sprow, K.; Troiano, R.P.; Piercy, K.L.; Vaux-Bjerke, A.; Powell, K.E. Benefits of Physical Activity during Pregnancy and Postpartum: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1292–1302. [Google Scholar] [CrossRef]
- Wang, D.; Ding, W.; Ding, C.; Chen, H.; Zhao, W.; Sun, B.; Wang, Z. Higher Peripheral Cholesterol and a Positive Correlation with Risk for Large-For-Gestational-Age Neonates in Pre-Pregnancy Underweight Women. Front. Endocrinol. 2021, 12, 760934. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Lu, J.; Yan, S.; Tao, F.; Huang, K. Maternal Pre-Pregnancy Body Mass Index, Gestational Weight Gain and Children’s Cognitive Development: A Birth Cohort Study. Nutrients 2022, 14, 4613. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.P.R.D.; Viana, T.G.F.; Duarte, C.K.; Inácio, M.L.C.; Velasquez-Melendez, G.; Pessoa, M.C.; Mendes, L.L.; Matozinhos, F.P. Environmental factors associated with excessive gestational weight gain: A meta-analysis and systematic review. Ciência Saúde Coletiva 2023, 28, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Dachew, B.A.; Ayano, G.; Betts, K.; Alati, R. The impact of pre-pregnancy BMI on maternal depressive and anxiety symptoms during pregnancy and the postpartum period: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 321–330. [Google Scholar] [CrossRef]
- Qiu, X.; Zhang, S.; Yan, J. Gestational weight gain and risk of postpartum depression: A meta-analysis of observational studies. Psychiatry Res. 2022, 310, 114448. [Google Scholar] [CrossRef]
- Zanardo, V.; Giliberti, L.; Giliberti, E.; Grassi, A.; Perin, V.; Parotto, M.; Soldera, G.; Straface, G. The role of gestational weight gain disorders in symptoms of maternal postpartum depression. Int. J. Gynaecol. Obstet. 2021, 153, 234–238. [Google Scholar] [CrossRef]
- Schlaff, R.A.; Baruth, M.; Gherke, J.T.; Deere, S.J. Pre-pregnancy body dissatisfaction and weight-related outcomes and behaviors during pregnancy. Health Care Women Int. 2021, 42, 446–461. [Google Scholar] [CrossRef]
- Ogawa, K.; Morisaki, N.; Sago, H.; Fujiwara, T.; Horikawa, R. Association between women’s perceived ideal gestational weight gain during pregnancy and pregnancy outcomes. Sci. Rep. 2018, 8, 11574. [Google Scholar] [CrossRef]
- Watson, B.; Broadbent, J.; Skouteris, H.; Fuller-Tyszkiewicz, M. A qualitative exploration of body image experiences of women progressing through pregnancy. Women Birth 2016, 29, 72–79. [Google Scholar] [CrossRef]
- Riquin, E.; Lamas, C.; Nicolas, I.; Dugre Lebigre, C.; Curt, F.; Cohen, H.; Legendre, G.; Corcos, M.; Godart, N. A key for perinatal depression early diagnosis: The body dissatisfaction. J. Affect. Disord. 2019, 245, 340–347. [Google Scholar] [CrossRef]
- Silveira, M.L.; Ertel, K.A.; Dole, N.; Chasan-Taber, L. The role of body image in prenatal and postpartum depression: A critical review of the literature. Arch. Women’s Ment. Health 2015, 18, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Han, S.-Y.; Brewis, A.A.; Wutich, A. Body image mediates the depressive effects of weight gain in new mothers, particularly for women already obese: Evidence from the Norwegian Mother and Child Cohort Study. BMC Public Health 2016, 16, 664. [Google Scholar] [CrossRef] [PubMed]
- Berenson, A.B.; Pohlmeier, A.M.; Laz, T.H.; Rahman, M.; Saade, G. Obesity Risk Knowledge, Weight Misperception, and Diet and Health-Related Attitudes among Women Intending to Become Pregnant. J. Acad. Nutr. Diet. 2016, 116, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Khair, H.; Bataineh, M.a.F.; Zaręba, K.; Alawar, S.; Maki, S.; Sallam, G.S.; Abdalla, A.; Mutare, S.; Ali, H.I. Pregnant Women’s Perception and Knowledge of the Impact of Obesity on Prenatal Outcomes—A Cross-Sectional Study. Nutrients 2023, 15, 2420. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-M.; Seo, M.-S.; Shim, J.-Y.; Lee, Y.-J. Body weight status misperception and its association with weight control behaviours, depressive mood and psychological distress in nulliparous normal-weight young women. Ann. Human. Biol. 2015, 42, 528–532. [Google Scholar] [CrossRef]
- Coyne, S.M.; Liechty, T.; Collier, K.M.; Sharp, A.D.; Davis, E.J.; Kroff, S.L. The Effect of Media on Body Image in Pregnant and Postpartum Women. Health Commun. 2018, 33, 793–799. [Google Scholar] [CrossRef]
- Papini, N.M.; Mason, T.B.; Herrmann, S.D.; Lopez, N.V. Self-compassion and body image in pregnancy and postpartum: A randomized pilot trial of a brief self-compassion meditation intervention. Body Image 2022, 43, 264–274. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, J.I. Predictive validity of the Edinburgh postnatal depression scale and other tools for screening depression in pregnant and postpartum women: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2023, 307, 1331–1345. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 2169) | PPD (n = 391) | Non-PPD (n = 1778) | χ2 | p |
|---|---|---|---|---|---|
| Postpartum age (years) | 9.402 | 0.002 | |||
| <35 | 1812 (83.5) | 347 (88.7) | 1465 (82.4) | ||
| ≥35 | 357 (16.5) | 44 (11.3) | 313 (17.6) | ||
| Ethnicity | 2.367 | 0.124 | |||
| Han | 1801 (83.0) | 335 (85.7) | 1466 (82.5) | ||
| Minority | 368 (17.0) | 56 (14.3) | 312 (17.5) | ||
| Region of residence | 37.157 | <0.001 | |||
| Urban | 1051 (48.5) | 244 (62.4) | 807 (45.4) | ||
| Rural | 1118 (51.5) | 147 (37.6) | 971 (54.6) | ||
| Per capita monthly income (RMB) | 33.742 | <0.001 | |||
| <5000 | 1167 (53.8) | 165 (42.2) | 1002 (56.4) | ||
| 5000~10,000 | 595 (27.4) | 151 (38.6) | 444 (25.0) | ||
| >=10,000 | 407 (18.8) | 75 (19.2) | 332 (18.6) | ||
| Educational level | 6.522 | 0.038 | |||
| Senior high school and below | 1105 (50.9) | 177 (45.3) | 928 (52.2) | ||
| Junior college/vocational university | 551 (25.4) | 107 (27.4) | 444 (25.0) | ||
| Bachelor’s degree or above | 513 (23.7) | 107 (27.4) | 406 (22.8) | ||
| Employment | 1.171 | 0.279 | |||
| Unemployed | 952 (43.9) | 162 (41.4) | 790 (44.4) | ||
| Employed | 1217 (56.1) | 229 (58.6) | 988 (55.6) | ||
| Parity | 13.687 | <0.001 | |||
| Primiparous | 1070 (49.3) | 226 (57.8) | 844 (47.5) | ||
| Multiparous | 1099 (50.7) | 165 (42.2) | 934 (52.5) | ||
| Mode of delivery | 1.124 | 0.289 | |||
| Spontaneous labor | 1540 (71.0) | 269 (68.8) | 1271 (71.5) | ||
| Cesarean section | 629 (29.0) | 122 (31.2) | 507 (28.5) | ||
| Gestational age at birth | 0.505 | 0.478 | |||
| Preterm | 260 (12.0) | 51 (13.0) | 209 (11.8) | ||
| Term | 1909 (88.0) | 340 (87.0) | 1569 (88.2) | ||
| Passive smoking status | 0.073 | 0.788 | |||
| Yes | 154 (7.1) | 29 (7.4) | 125 (7.0) | ||
| No | 2015 (92.9) | 362 (92.6) | 1653 (93.0) | ||
| Physical activity levels | 44.091 | <0.001 | |||
| High/moderate | 1161 (53.5) | 150 (38.4) | 1011 (56.9) | ||
| Low | 1008 (46.5) | 241 (61.6) | 767 (43.1) | ||
| Weight Perception | n | EPDS Scores | Z | p |
|---|---|---|---|---|
| Perceived PPW | 43.350 | <0.001 | ||
| Underweight | 251 | 6 (4, 10) | ||
| Normal weight | 1406 | 5 (3, 9) | ||
| Overweight/obesity | 512 | 7 (4, 10) | ||
| Perceived GWG | 21.080 | <0.001 | ||
| Insufficient | 55 | 7 (4, 10) | ||
| Appropriate | 1565 | 5 (3, 9) | ||
| Excessive | 549 | 6 (4, 10) | ||
| Agreement of actual and perceived PPW | 6.332 | 0.042 | ||
| Underestimation | 211 | 5 (3, 9) | ||
| Consistency | 1452 | 6 (3, 9) | ||
| Overestimation | 506 | 6 (3, 9) | ||
| Agreement of actual and perceived GWG | 17.130 | <0.001 | ||
| Underestimation | 509 | 5 (3, 8) | ||
| Consistency | 1189 | 6 (3, 9) | ||
| Overestimation | 471 | 6 (3, 10) | ||
| Characteristics | Unadjusted Model | Adjusted Model | ||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| Actual PPW | ||||
| Normal weight | Ref. | Ref. | ||
| Underweight | 0.15 (−0.35, 0.64) | 0.566 | 0.19 (−0.27, 0.66) | 0.441 |
| Overweight/obesity | 0.19 (−0.33, 0.70) | 0.484 | 0.17 (−0.32, 0.66) | 0.502 |
| Perceived PPW | ||||
| Normal weight | Ref. | Ref. | ||
| Underweight | 0.97 (0.37, 1.57) | 0.001 | 0.70 (0.13, 1.27) | 0.016 |
| Overweight/obesity | 1.32 (0.87, 1.77) | <0.001 | 0.86 (0.43, 1.29) | <0.001 |
| Agreement of actual and perceived PPW | ||||
| Consistency | Ref. | Ref. | ||
| Underestimation | −0.50 (−1.15, 0.14) | 0.127 | −0.32 (−0.94, 0.29) | 0.302 |
| Overestimation | 0.39 (−0.06, 0.85) | 0.090 | 0.27 (−0.16, 0.70) | 0.219 |
| Characteristics | Unadjusted Model | Adjusted Model | ||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| Actual GWG | ||||
| Appropriate | Ref. | Ref. | ||
| Insufficient | 0.91 (0.35, 1.47) | 0.001 | 0.39 (−0.14, 0.92) | 0.151 |
| Excessive | 0.12 (−0.29, 0.54) | 0.553 | −0.02 (−0.41, 0.37) | 0.937 |
| Perceived GWG | ||||
| Appropriate | Ref. | Ref. | ||
| Insufficient | 1.24 (0.03, 2.44) | 0.044 | 1.11 (−0.02, 2.25) | 0.054 |
| Excessive | 0.92 (0.48, 1.35) | <0.001 | 0.47 (0.05, 0.88) | 0.028 |
| Agreement of actual and perceived GWG | ||||
| Consistency | Ref. | Ref. | ||
| Underestimation | −0.61 (−1.08, −0.15) | 0.010 | −0.39 (−0.83, 0.05) | 0.085 |
| Overestimation | 0.50 (0.03, 0.98) | 0.039 | 0.21 (−0.24, 0.67) | 0.356 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Qiu, M.; Guo, L.; Li, Y.; Xie, Z.; Yang, W.; Ouyang, L.; Yin, J.; Zhou, Y.; Fu, M.; et al. Association Between Maternal Weight Perception Before and During Pregnancy and Postpartum Depression Status in Southern China. Nutrients 2024, 16, 3696. https://doi.org/10.3390/nu16213696
Zhang Q, Qiu M, Guo L, Li Y, Xie Z, Yang W, Ouyang L, Yin J, Zhou Y, Fu M, et al. Association Between Maternal Weight Perception Before and During Pregnancy and Postpartum Depression Status in Southern China. Nutrients. 2024; 16(21):3696. https://doi.org/10.3390/nu16213696
Chicago/Turabian StyleZhang, Qin, Menglu Qiu, Laidi Guo, Yuanyuan Li, Zhencheng Xie, Wanyi Yang, Lishan Ouyang, Jia Yin, Yun Zhou, Minghan Fu, and et al. 2024. "Association Between Maternal Weight Perception Before and During Pregnancy and Postpartum Depression Status in Southern China" Nutrients 16, no. 21: 3696. https://doi.org/10.3390/nu16213696
APA StyleZhang, Q., Qiu, M., Guo, L., Li, Y., Xie, Z., Yang, W., Ouyang, L., Yin, J., Zhou, Y., Fu, M., Ding, Y., & Wang, Z. (2024). Association Between Maternal Weight Perception Before and During Pregnancy and Postpartum Depression Status in Southern China. Nutrients, 16(21), 3696. https://doi.org/10.3390/nu16213696