
Association between Serum Fatty Acids Profile and MetScore in Women with Severe Obesity

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
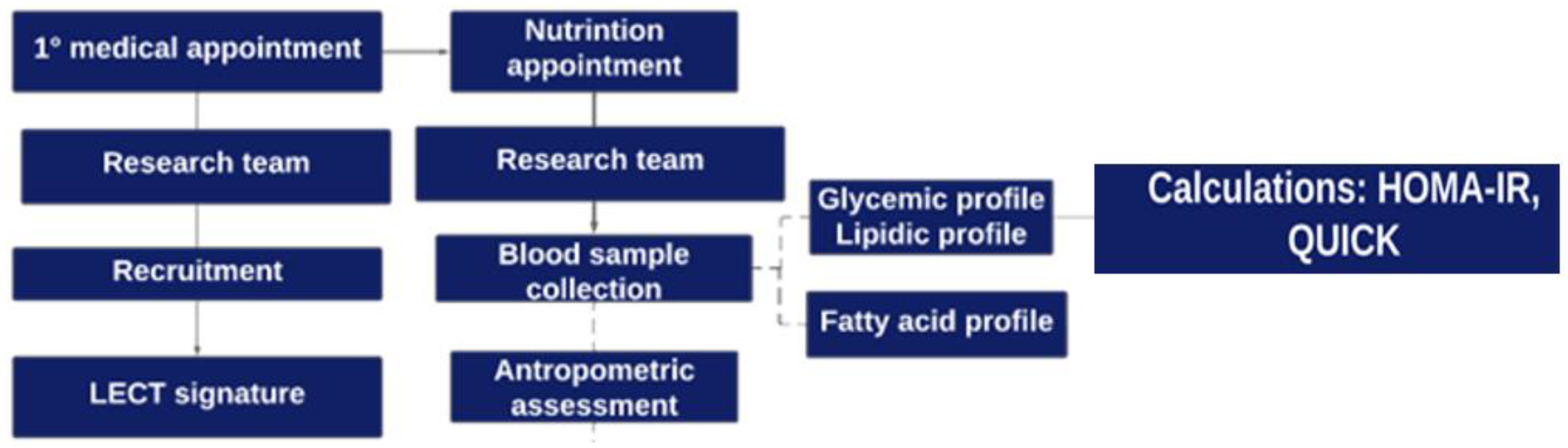
2.2. Study Design
2.3. Measurements
2.3.1. Anthropometric Assessment
2.3.2. Biochemical Exams
2.3.3. Blood Pressure
2.3.4. MetScore Calculation
2.4. Extraction and Determination of Serum Fatty Acids
2.4.1. Extraction and Methylation of Fatty Acids
2.4.2. Identification and Quantification of Fatty Acid Methyl Esters (FAMEs)
2.5. Desaturases Indexes
2.6. Statistical Analysis
3. Results
3.1. Sample Description and Lipidic, Glycemic Profile
3.2. Serum Fatty Acid Profile and Their Association with Cardiovascular Risk
4. Discussion
5. Conclusions
6. Future Recommendations
- (1)
- There is a need for longitudinal studies to determine the influence of fatty acids on cardiovascular risk over the years.
- (2)
- Clinical trials for dietary interventions should be conducted using different sources of carbohydrates and lipids to verify the influence of serum fatty acids and desaturating enzymes on cardiovascular risk. Furthermore, randomized clinical trials with fatty acid supplementation, which in the present study was shown to be cardioprotective, would help determine their influence on reducing cardiovascular risk.
- (3)
- Evaluation of different populations, mainly longitudinal studies in eutrophic individuals, should be conducted to show the MetS score as a good tool for early screening of cardiovascular risk, through changes in the GA profile over the years.
- (4)
- It is important to conduct controlled and randomized clinical trials involving the supplementation of key fatty acids discussed in this study in order to investigate their potential as a therapeutic option for attenuating inflammation and reducing cardiometabolic alterations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsdenh, H.; Calvilloi, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef] [PubMed]
- Wrzosek, M.; Zawadzka, Z.; Sawicka, A.; Bobrowska-Korczak, B.; Białek, A. Impact of Fatty Acids on Obesity-Associated Diseases and Radical Weight Reduction. Obes. Surg. 2022, 32, 428. [Google Scholar] [CrossRef] [PubMed]
- Silveira, E.A.; Kliemann, N.; Noll, M.; Sarrafzadegan, N.; Oliveira, C. Visceral obesity and incident cancer and cardiovascular disease: An integrative review of the epidemiological evidence. Obes. Rev. 2021, 22, e13088. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Geisler, C. Defining obesity as a disease. Eur. J. Clin. Nutr. 2017, 71, 1256–1258. [Google Scholar] [CrossRef] [PubMed]
- Wijayatunga, N.N.; Sams, V.G.; Dawson, J.A.; Mancini, M.L.; Mancini, G.J.; Moustaid-Moussa, N. Roux-en-Y gastric bypass surgery alters serum metabolites and fatty acids in patients with morbid obesity. Diabetes Metab. Res. Rev. 2018, 34, e3045. [Google Scholar] [CrossRef]
- Walle, P.; Takkunen, M.; Männistö, V.; Vaittinen, M.; Lankinen, M.; Kärjä, V.; Käkelä, P.; Ågren, J.; Tiainen, M.; Schwab, U.; et al. Fatty acid metabolism is altered in non-alcoholic steatohepatitis independent of obesity. Metabolism 2016, 65, 655–666. [Google Scholar] [CrossRef]
- IDF Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Thivel, D.; Malina, R.M.; Isacco, L.; Aucouturier, J.; Meyer, M.; Duché, P. Metabolic syndrome in obese children and adolescents: Dichotomous or continuous? Metab. Syndr. Relat. Disord. 2009, 7, 549–555. [Google Scholar] [CrossRef]
- Malta, D.C.; da Silva, A.G.; Tonaco, L.A.B.; de Fátima Freitas, M.I.; Velasquez-Melendez, G. Tendência temporal da prevalência de obesidade mórbida na população adulta brasileira entre os anos de 2006 e 2017. Cad. Saúde Pública 2019, 35, e00223518. [Google Scholar] [CrossRef]
- Williamson, K.; Nimegeer, A.; Lean, M. Rising prevalence of BMI ≥40 kg/m2: A high-demand epidemic needing better documentation. Obes. Rev. 2020, 21, e12986. [Google Scholar] [CrossRef]
- Kaikkonen, J.E.; Jula, A.; Viikari, J.S.A.; Juonala, M.; Hutri-Kähönen, N.; Kähönen, M.; Lehtimäki, T.; Raitakari, O.T. Associations of Serum Fatty Acid Proportions with Obesity, Insulin Resistance, Blood Pressure, and Fatty Liver: The Cardiovascular Risk in Young Finns Study. J. Nutr. 2021, 151, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Anjos, C.A.; Clemente, M.; de Fátima Gaspari Dias, J.; Burci, L.M.; de Oliveira Leite, R.; Miguel, M.D. Quality of Life of Elderly People Living in Different Types of Long-term Care Facilities. Braz. J. Pharm. Sci. 2022, 58, e20117. [Google Scholar] [CrossRef]
- Fett, C.A.; Fett, W.C.R.; Marchini, J.S. Comparação entre bioimpendância e antropometria e a relação de índices corporais ao gasto energético de repouso e marcadores bioquímicos sanguíneos em mulheres da normalidade à obesidade. Rev. Bras. Cineantropom Desempenho Hum. 2006, 8, 29–36. [Google Scholar]
- ABESO. Diretrizes Brasileiras de Obesidade—2016; ABESO: São Paulo, Brazil, 2016. [Google Scholar]
- Hingorjo, M.R.; Zehra, S.; Imran, E.; Qureshi, M. Neck circumference: A supplemental tool for the diagnosis of metabolic syndrome. JPMA 2016, 66, 1221–1226. [Google Scholar]
- Stern, S.E.; Williams, K.; Ferrannini, E.; DeFronzo, R.A.; Bogardus, C.; Stern, M.P. Identification of Individuals With Insulin Resistance Using Routine Clinical Measurements. Diabetes 2005, 54, 333–339. [Google Scholar] [CrossRef]
- Placzkowska, S.; Pawlik-Sobecka, L.; Kokot, I.; Piwowar, A. Indirect insulin resistance detection: Current clinical trends and laboratory limitations. Biomed. Pap. 2019, 163, 187–199. [Google Scholar] [CrossRef]
- Faludi, A.A.; Izar, M.C.O.; Saraiva, J.F.K.; Bianco, H.T.; Chacra, A.P.M. Atualização da Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose. Arq. Bras. Cardiol. 2017, 109, 1–76. [Google Scholar] [CrossRef]
- Drehmer, M.; Pereira, M.A.; Schmidt, M.I.; Alvim, S.; Lotufo, P.A.; Luft, V.C.; Bruce, D. Total and full-fat, but not low-fat, dairy product intakes are inversely associated with metabolic syndrome in adults. J. Nutr. 2016, 146, 81–89. [Google Scholar] [CrossRef]
- Ichihara, K.; Fukubayashi, Y. Preparation of fatty acid methyl esters for gas-liquid chromatography. J. Lipid Res. 2010, 51, 635–640. [Google Scholar] [CrossRef]
- Christie, W. Lipid Analysis; Pergamon Press: Oxford, UK, 1982. [Google Scholar]
- García-Serrano, S.; Moreno-Santos, I.; Garrido-Sánchez, L.; Gutierrez-Repiso, C.; García-Almeida, J.M.; García-Arnés, J.; Rivas-Marín, J.; Gallego-Perales, J.L.; García-Escobar, E.; Rojo-Martinez, G.; et al. Stearoyl-CoA Desaturase-1 Is Associated with Insulin Resistance in Morbidly Obese Subjects. Mol. Med. 2011, 17, 273. [Google Scholar] [CrossRef]
- Lancaster, G.I.; Langley, K.G.; Berglund, N.A.; Kammoun, H.L.; Reibe, S.; Estevez, E.; Weir, J.; Mellett, N.A.; Pernes, G.; Conway, J.R.W.; et al. Evidence that TLR4 Is Not a Receptor for Saturated Fatty Acids but Mediates Lipid-Induced Inflammation by Reprogramming Macrophage Metabolism. Cell Metab. 2018, 27, 1096–1110.e5. [Google Scholar] [CrossRef] [PubMed]
- Perna, M.; Hewlings, S. Saturated Fatty Acid Chain Length and Risk of Cardiovascular Disease: A Systematic Review. Nutrients 2023, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Korbecki, J.; Bajdak-Rusinek, K. The effect of palmitic acid on inflammatory response in macrophages: An overview of molecular mechanisms. Inflamm. Res. 2019, 68, 915–932. [Google Scholar] [CrossRef] [PubMed]
- Rogero, M.; Calder, P. Obesity, Inflammation, Toll-Like Receptor 4 and Fatty Acids. Nutrients 2018, 10, 432. [Google Scholar] [CrossRef] [PubMed]
- Wenjie, M.; Wu, J.H.Y.; Wang, Q.; Lemaitre, R.N.; Mukamal, K.J.; Djoussé, L.; Irena, K.; Xiaoling, S.; Mary, B.; Joseph, D.; et al. Prospective association of fatty acids in the de novo lipogenesis pathway with risk of type 2 diabetes: The Cardiovascular Health Study. Am. J. Clin. Nutr. 2015, 101, 153. [Google Scholar] [CrossRef]
- Wen, H.; Gris, D.; Lei, Y.; Jha, S.; Zhang, L.; Huang, M.T.H.; Brickey, W.J.; Ting, J.P. Fatty acid-induced NLRP3-PYCARD inflammasome activation interferes with insulin signaling. Nat. Immunol. 2011, 12, 408. [Google Scholar] [CrossRef]
- Hodson, L.; Skeaff, C.M.; Fielding, B.A. Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog. Lipid Res. 2008, 47, 348–380. [Google Scholar] [CrossRef]
- Ravaut, G.; Légiot, A.; Bergeron, K.F.; Mounier, C. Monounsaturated Fatty Acids in Obesity-Related Inflammation. Int. J. Mol. Sci. 2021, 22, 330. [Google Scholar] [CrossRef]
- Alsharari, Z.D.; Leander, K.; Sjögren, P.; Carlsson, A.; Cederholm, T.; de Faire, U.; Hellenius, M.-L.; Marklund, M.; Risérus, U. Association between carbohydrate intake and fatty acids in the de novo lipogenic pathway in serum phospholipids and adipose tissue in a population of Swedish men. Eur. J. Nutr. 2020, 59, 2089–2097. [Google Scholar] [CrossRef]
- Warensjö, E.; Rosell, M.; Hellenius, M.L.; Vessby, B.; De Faire, U.; Risérus, U. Associations between estimated fatty acid desaturase activities in serum lipids and adipose tissue in humans: Links to obesity and insulin resistance. Lipids Health Dis. 2009, 8, 37. [Google Scholar] [CrossRef]
- Mayneris-Perxachs, J.; Guerendiain, M.; Castellote, A.I.; Estruch, R.; Covas, M.I.; Fitó, M.; Salas-Salvadó, J.; Martínez-González, M.A.; Aros, F.; Lamuela-Raventós, R.M.; et al. Plasma fatty acid composition, estimated desaturase activities, and their relation with the metabolic syndrome in a population at high risk of cardiovascular disease. Clin. Nutr. 2014, 33, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Balatskyi, V.V.; Dobrzyn, P. Role of Stearoyl-CoA Desaturase 1 in Cardiovascular Physiology. Int. J. Mol. Sci. 2023, 24, 5531. [Google Scholar] [CrossRef] [PubMed]
- Kalupahana, N.S.; Wang, S.; Rahman, S.M.; Moustaid-Moussa, N. Function and Regulation of Macrophage Stearoyl-CoA Desaturase in Metabolic Disorders. In Stearoyl-CoA Desaturase Genes in Lipid Metabolism; Springer: New York, NY, USA, 2013; pp. 61–71. [Google Scholar] [CrossRef]
- Popeijus, H.E.; Saris, W.H.M.; Mensink, R.P. Role of stearoyl-CoA desaturases in obesity and the metabolic syndrome. Int. J. Obes. 2008, 32, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.A.; Escoula, Q.; Veillette, C.; Bergeron, K.F.; Ntambi, J.M.; Mounier, C. SCD1 deficiency protects mice against ethanol-induced liver injury. Biochim. Biophys. Acta (BBA)—Mol. Cell Biol. Lipids 2016, 1861, 1662–1670. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, K.; Olsen, T.; Nordstrand Rusvik, T.C.; Ulven, S.M.; Holven, K.B.; Retterstøl, K.; Telle-Hansen, V.H. Fatty acid profile and estimated desaturase activities in whole blood are associated with metabolic health. Lipids Health Dis. 2020, 19, 102. [Google Scholar] [CrossRef]
- Domínguez-López, I.; Arancibia-Riveros, C.; Tresserra-Rimbau, A.; Castro-Barquero, S.; Casas, R.; Vázquez-Ruiz, Z.; Ros, E.; Fitó, M.; Estruch, R.; López-Sabate, M.C.; et al. Relationship between estimated desaturase enzyme activity and metabolic syndrome in a longitudinal study. Front. Nutr. 2022, 9, 991277. [Google Scholar] [CrossRef]
- Yu, E.A.; Hu, P.J.; Mehta, S. Plasma fatty acids in de novo lipogenesis pathway are associated with diabetogenic indicators among adults: NHANES 2003–2004. Am. J. Clin. Nutr. 2018, 108, 622. [Google Scholar] [CrossRef]
- Crewe, C.; An, Y.A.; Scherer, P.E. The ominous triad of adipose tissue dysfunction: Inflammation, fibrosis, and impaired angiogenesis. J. Clin. Investig. 2017, 127, 74–82. [Google Scholar] [CrossRef]
- Patel, P.S.; Sharp, S.J.; Jansen, E.; Luben, R.N.; Khaw, K.T.; Wareham, N.J.; Nita, G.F. Fatty acids measured in plasma and erythrocyte-membrane phospholipids and derived by food-frequency questionnaire and the risk of new-onset type 2 diabetes: A pilot study in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk cohort. Am. J. Clin. Nutr. 2010, 92, 1214–1222. [Google Scholar] [CrossRef]
- Wang, L.; Folsom, A.R.; Zheng, Z.-J.; Pankow, J.S.; Eckfeldt, J.H. Plasma fatty acid composition and incidence of diabetes in middle-aged adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Clin. Nutr. 2003, 78, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Zhang, J.; Li, M.; Shang, J.; Bai, X.; Zhang, H.; Wang, Y.; Chen, H.; Song, X. Serum fatty acid profiles associated with metabolic risk in women with polycystic ovary syndrome. Front. Endocrinol. 2023, 14, 1077590. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Leung, J.C.K.; Chan, L.Y.Y.; Yiu, W.H.; Tang, S.C.W. A global perspective on the crosstalk between saturated fatty acids and Toll-like receptor 4 in the etiology of inflammation and insulin resistance. Prog. Lipid Res. 2020, 77, 101020. [Google Scholar] [CrossRef] [PubMed]
- Cobas, R.; Rodacki, M.; Giacaglia, L.; Calliari, L.E.P.; Noronha, R.M.; Valerio, C.; Custodio, J.S., Jr.; Scharf, M.; Barcellos, C.R.G.; Tomarchio, M.P.; et al. Diagnóstico do diabetes e rastreamento do diabetes tipo 2. In Diretriz Oficial da Sociedade Brasileira de Diabetes; Conectando Pessoas: Brasília, Brazil, 2022. [Google Scholar] [CrossRef]
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. Omega-6 fatty acids and inflammation. Prostaglandins Leukot. Essent. Fat. Acids 2018, 132, 41–48. [Google Scholar] [CrossRef]
- Surette, M.E.; Koumenis, I.L.; Edens, M.B.; Tramposch, K.M.; Chilton, F.H. Inhibition of leukotriene synthesis, pharmacokinetics, and tolerability of a novel dietary fatty acid formulation in healthy adult subjects. Clin. Ther. 2003, 25, 948–971. [Google Scholar] [CrossRef]
- Johnson, M.M.; Swan, D.D.; Surette, M.E.; Stegner, J.; Chilton, T.; Fonteh, A.N.; Chilton, F.H. Dietary Supplementation with γ-Linolenic Acid Alters Fatty Acid Content and Eicosanoid Production in Healthy Humans. J. Nutr. 1997, 127, 1435–1444. [Google Scholar] [CrossRef]
- Barham, J.B.; Edens, M.B.; Fonteh, A.N.; Johnson, M.M.; Easter, L.; Chilton, F.H. Addition of Eicosapentaenoic Acid to γ-Linolenic Acid–Supplemented Diets Prevents Serum Arachidonic Acid Accumulation in Humans. J. Nutr. 2000, 130, 1925–1931. [Google Scholar] [CrossRef]
- Sergeant, S.; Rahbar, E.; Chilton, F.H. Gamma-linolenic acid, Dihommo-gamma linolenic, Eicosanoids and Inflammatory Processes. Eur. J. Pharmacol. 2016, 785, 77–86. [Google Scholar] [CrossRef]
- Guo, X.F.; Li, X.; Shi, M.; Li, D. n-3 Polyunsaturated Fatty Acids and Metabolic Syndrome Risk: A Meta-Analysis. Nutrients 2017, 9, 703. [Google Scholar] [CrossRef]
- Jang, H.; Park, K. Omega-3 and omega-6 polyunsaturated fatty acids and metabolic syndrome: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 765–773. [Google Scholar] [CrossRef]
- Scorletti, E.; Byrne, C.D. Omega-3 fatty acids and non-alcoholic fatty liver disease: Evidence of efficacy and mechanism of action. Mol. Asp. Med. 2018, 64, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.L. Princípios de bioquímica de Lehninger, 6th ed; Artmed Editora: Porto Alegre, Brazil, 2014. [Google Scholar]
- Borghi, C.; Cicero, A.F.G. Omega-3 polyunsaturated fatty acids: Their potential role in blood pressure prevention and management. Heart Int. 2006, 2, 330–337. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Mean Total Sample ± SD | Low Risk (<−0.05) Mean ± SD | High Risk (≥−0.05) Mean ± SD | p 1 | High Risk OR (95% CI) | p 2 |
|---|---|---|---|---|---|---|
| Age (years) | 40.22 ± 8.31 | 37.65 ± 9.10 | 42.67 ± 6.83 | 0.042 * | 1.08 (0.99–1.18) | 0.058 |
| Height (m) | 1.59 ± 0.05 | 1.60 ± 0.05 | 1.58 ± 0.05 | 0.167 | 5.21−4 (7.25−29–37.4) | 0.185 |
| Weight (kg) | 122.71 ± 17.98 | 124.33 ± 31.30 | 121.17 ± 16.76 | 0.551 | 0.99 (0.96–1.03) | 0.571 |
| BMI (kg/m2) | 48.38 ± 6.66 | 48.22 ± 6.89 | 48.53 ± 6.60 | 0.878 | 1.05 (0.91–1.11) | 0.881 |
| AC (cm) | 131.46 ± 12.52 | 127.33 ± 9.54 | 135.41 ± 13.91 | - | - | - |
| HC (cm) | 145.32 ± 13.33 | 145.41 ± 14.30 | 145.25 ± 12.70 | 0.967 | 0.99 (0.95–1.05) | 0.968 |
| WHR | 0.90 ± 0.06 | 0.88 ± 0.07 | 0.93 ± 0.05 | - | - | - |
| NC (cm) | 41.63 ± 3.23 | 41.50 ± 3.77 | 41.77 ± 2.71 | 0.789 | 1.03 (0.85–1.24) | 0.791 |
| Fasting glucose (mg/dL) | 110.87 ± 35.13 | 95.25 ± 8.60 | 125.76 ± 43.83 | - | - | - |
| HbA1c (%) | 6.24 ± 1.10 | 5.82 ± 0.36 | 6.65 ± 1.39 | 0.002 * | 5.24 (1.01–27.05) | 0.048 * |
| HOMA-IR | 6.92 ± 3.48 | 5.64 ± 2.60 | 8.15 ± 3.82 | 0.011 * | 1.30 (1.02–1.64) | 0.031 * |
| QUICKI | 0.28 ± 0.24 | 0.30 ± 0.02 | 0.28 ± 0.02 | 0.006 * | 3.86−19 (6.17−35–0.00) | 0.022 * |
| Insulin | 27.55 ± 14.42 | 27.7 ± 16.14 | 27.40 ± 12.99 | 0.945 | 0.99 (0.96–1.04) | 0.943 |
| TG (mg/dL) | 145.17 ± 68.19 | 108.70 ± 36.50 | 179.91 ± 73.75 | - | - | - |
| LDL-C (mg/dL) | 105.4 ± 28.21 | 108.80 ± 32.44 | 101.86 ± 23.82 | 0.418 | 0.99 (0.98–1.01) | 0.429 |
| HDL-C (mg/dL) | 46.75 ± 10.31 | 50.65± 10.84 | 43.05 ± 8.46 | - | - | - |
| VLDL-C | 21.00 ± 5.06 | 21.00 ± 5.06 | 29.24 ± 9.76 | 0.000 * | 1.23 (1.06–1.41) | 0.005 * |
| SBP (mmHg) | 138.68 ± 15.09 | 132.25 ± 14.29 | 144.81 ± 13.46 | - | - | - |
| DBP (mmHg) | 86.02 ± 9.93 | 82.80 ± 9.83 | 89.10 ± 9.23 | 0.032 | 1.08 (0.99–1.18) | 0.059 |
| MetScore | −0.10 ± 0.51 | - | - | - | - | |
| Medications in use (n (%)) | ||||||
| Antihypertensive | 0.437 3 | - | - | |||
| Yes | 21 (51.2%) | 9 (22.0%) | 12 (29.3%) | |||
| No | 20 (48.8%) | 11 (26.8%) | 9 (22.0%) | |||
| Hypoglycemic agents | 0.089 3 | - | - | |||
| Yes | 6 (14.6%) | 1 (2.4%) | 5 (12.2%) | |||
| No | 35 (85.4%) | 19 (46.3%) | 16 (39.0%) | |||
| Statins | 0.300 3 | - | - | |||
| Yes | 1 (2.4%) | 1 (2.4%) | 0 (0%) | |||
| No | 40 (97.6%) | 19 (46.3%) | 21 (51.2%) |
| Variable (MetScore) | Mean (%) ± SD | Low Risk (<−0.05) Mean ± SD | High Risk (≥−0.05) Mean ± SD | p 1 | High Risk OR (95% CI) | p 2 |
|---|---|---|---|---|---|---|
| SFA total % | 56.18 ± 5.63 | 56.89 ± 4.78 | 55.51 ± 6.39 | 0.417 | 0.96 (0.85–1.07) | 0.432 |
| C12:0 (lauric) | 26.42 ± 8.35 | 28.61 ± 7.18 | 24.35 ± 9.02 | 0.089 | 0.94 (0.86–1.01) | 0.109 |
| C14:0 (myristic) | 4.26 ± 1.45 | 4.69 ± 1.27 | 3.87 ± 1.54 | 0.058 | 0.65 (0.41–1.05) | 0.076 |
| C16:0 (palmitic) | 15.61 ± 4.75 | 13.77 ± 3.75 | 17.38 ± 5.03 | 0.008 * | 1.20 (1.03–1.40) | 0.020 * |
| C18:0 (stearic) | 9.18 ± 1.05 | 9.08 ± 1.04 | 9.28 ± 1.08 | 0.526 | 1.21 (0.67–2.20) | 0.530 |
| C20:0 (arachidic) | 0.55 ± 0.14 | 0.59 ± 0.12 | 0.52 ± 0.16 | 0.108 | 0.03 (3.12−4–2.64) | 0.124 |
| C22:0 (behenic) | 0.13 ± 0.13 | 0.16 ± 0.13 | 0.12 ± 0.13 | 0.369 | 0.118 (0.01–13.25) | 0.375 |
| MUFA% | 17.15 ± 2.99 | 15.84 ± 1.87 | 18.41 ± 3.35 | 0.002 * | 1.42 (1.09–1.86) | 0.011 * |
| C14:1n[5] (myristoleic) | 3.17 ± 1.01 | 3.47 ± 0.90 | 2.90 ± 1.06 | 0.058 | 0.55 (0.28–1.07) | 0.078 |
| C16:1n[7] (palmitoleic) | 0.90 ± 0.24 | 0.95 ± 0.23 | 0.86 ± 0.26 | 0.225 | 0.22 (0.02–2.99) | 0.253 |
| C18:1n[9] (oleic) | 11.23 ± 3.92 | 9.65 ± 2.62 | 12.75 ± 4.40 | 0.005 * | 1.27 (1.04–1.43) | 0.017 * |
| C18:1n[7] (vacenic) | 1.11 ± 0.35 | 1.00 ± 0.31 | 1.22 ± 0.37 | 0.042 * | 6.43 (0.90–45.52) | 0.062 |
| C20:1n[9] (eicosenoic) | 0.72 ± 0.22 | 0.77 ± 0.21 | 0.68 ± 0.24 | 0.238 | 0.19 (0.01–3.11) | 0.243 |
| Total PUFA (%) | 26.64 ± 4.04 | 27.25 ± 3.76 | 26.07 ± 4.30 | 0.338 | 0.93 (0.79–1.09) | 0.350 |
| Omega 6 total % | 21.68 ± 4.41 | 22.06 ± 3.86 | 21.33 ± 4.95 | 0.589 | 0.96 (0.84–1.11) | 0.592 |
| C18:2n[6] (LA; linoleic) | 14.47 ± 5.16 | 14.38 ± 4.73 | 14.57 ± 5.66 | 0.906 | 1.01 (0.89–1.14) | 0.906 |
| C18:3n[6] (GLA; gamma-linolenic) | 3.45 ± 1.05 | 3.90 ± 1.08 | 3.03 ± 0.86 | 0.003 * | 0.37 (0.16–0.82) | 0.015 * |
| C20:2n[6] (eicosadienoic) | 1.73 ± 0.69 | 1.85 ± 0.76 | 1.63 ± 0.62 | 0.275 | 0.62 (0.24–1.59) | 0.317 |
| C20:4n[6] (AA; arachidonic) | 0.44 ± 0.78 | 0.61 ± 1.33 | 0.28 ± 1.07 | 0.172 | 0.52 (0.17–1.53) | 0.234 |
| C20:3n[6] (DGLA; dihomo-gamma-linolenic) | 0.32 ± 0.99 | 0.07 ± 0.30 | 0.57 ± 1.33 | 0.089 | 2.21 (0.66–7.36) | 0.198 |
| C22:2n[6] (docosadienoic) | 1.25 ± 0.55 | 1.26 ± 0.56 | 1.25 ± 0.57 | 0.924 | 0.95 (0.31–2.89) | 0.924 |
| Omega 3 total% | 4.96 ± 1.99 | 5.19 ± 1.71 | 4.75 ± 2.25 | 0.455 | 0.89 (0.65–1.22) | 0.469 |
| C18:3n[3] (ALA; alfa-linolenic) | 2.78 ± 1.30 | 3.03 ± 1.18 | 2.54 ± 1.41 | 0.180 | 0.73 (0.44–1.22) | 0.234 |
| C18:4n[3] (stearidonic) | 0.50 ± 0.24 | 0.49 ± 0.12 | 0.52 ± 0.33 | 0.649 | 1.64 (0.12–22.04) | 0.708 |
| C20:3n[3] (eicosatrienoic) | 0.76 ± 0.69 | 0.69 ± 0.67 | 0.83 ± 0.72 | 0.413 | 1.36 (0.54–3.44) | 0.517 |
| C20:4n[3] (eicosatetraenoic) | 0.27 ± 0.11 | 0.31 ± 0.07 | 0.24 ± 0.14 | 0.038 * | 0.002 (2.09−6–1.53) | 0.066 |
| C20:5n[3] (EPA; eicosapentaenoic) | 0.08 ± 0.32 | 0.03 ± 0.11 | 0.13 ± 0.45 | 0.348 | 3.63 (0.13–97.89) | 0.443 |
| C22:6n[3] (DHA; docosahexaenoic) | 0.55 ± 0.56 | 0.63 ± 0.68 | 0.48 ± 0.44 | 0.398 | 0.60 (0.17–2.11) | 0.426 |
| omega 3/6 ratio | 0.24 ± 0.13 | 0.25 ± 0.10 | 0.25 ±0.17 | 0.930 | 1.21 (0.02–107.11) | 0.934 |
| omega 6/3 ratio | 5.23 ± 2.51 | 4.82 ± 2.07 | 5.63 ± 2.87 | 0.307 | 1.14 (0.89–1.47) | 0.301 |
| SFA/PUFA Ratio | 2.19 ± 0.63 | 2.15 ± 0.50 | 2.24 ± 0.75 | 0.606 | 1.26 (0.47–3.42) | 0.645 |
| SFA/MUFA ratio | 3.41 ± 0.89 | 3.66 ± 0.69 | 3.18 ± 1.01 | 0.061 | 0.512 (0.24–1.11) | 0.091 |
| SCD-16C | 0.07 ± 0.04 | 0.08 ± 0.04 | 0.06 ± 0.05 | 0.127 | 4.82−5 (1.58−11–147.13) | 0.192 |
| SCD-18C | 1.23 ± 0.43 | 1.06 ± 0.27 | 1.39 ± 0.51 | 0.011 * | 7.73 (1.32–45.25) | 0.023 * |
| Variable | p-Value | High Risk OR (95%CI) |
|---|---|---|
| C16:0 | 0.030 * | 1.36(1.03–1.79) |
| MUFA Total | 0.032 * | 1.52 (1.03–2.26) |
| C18:1n[9] | 0.045 * | 1.36 (1.05–1.83) |
| C18:3n[6] | 0.051 * | 0.27 (0.07–1.01) |
| SCD-18C | 0.060 | 13.50 (0.90–202.51) |
| Variable | p-Value | Correlation Coefficient | |
|---|---|---|---|
| HOMA-IR | Metscore | 0.001 | 0.481 |
| HbA1c | Metscore | <0.001 | 0.526 |
| VLDL-C | Metscore | <0.001 | 0.556 |
| c16:0 | Metscore | 0.041 | 0.320 |
| c18:1n[9] | Metscore | 0.003 | 0.334 |
| Total MUFA | Metscore | 0.002 | 0.360 |
| SCD-18 | Metscore | 0.004 | 0.316 |
| HDL-C | Metscore | 0.001 | −0.514 |
| QUICKI | Metscore | 0.005 | −0.430 |
| Omega 6 | Metscore | 0.004 | −0.313 |
| c18:3n[6] | Metscore | 0.003 | −0.313 |
| c18:1n[7] | QUICKI | 0.013 | −0.389 |
| c18:1n[9] | QUICKI | 0.002 | −0.477 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, E.S.; Kattah, F.M.; Lima, G.C.; Horst, M.A.; Figueiredo, N.; Lima, G.B.; Whitton, R.G.M.; de Souza, G.I.d.M.H.; Oyama, L.M.; Silveira, E.A.; et al. Association between Serum Fatty Acids Profile and MetScore in Women with Severe Obesity. Nutrients 2024, 16, 3508. https://doi.org/10.3390/nu16203508
Oliveira ES, Kattah FM, Lima GC, Horst MA, Figueiredo N, Lima GB, Whitton RGM, de Souza GIdMH, Oyama LM, Silveira EA, et al. Association between Serum Fatty Acids Profile and MetScore in Women with Severe Obesity. Nutrients. 2024; 16(20):3508. https://doi.org/10.3390/nu16203508
Chicago/Turabian StyleOliveira, Emilly Santos, Fabiana Martins Kattah, Glaucia Carielo Lima, Maria Aderuza Horst, Nayra Figueiredo, Gislene Batista Lima, Renata Guimarães Moreira Whitton, Gabriel Inacio de Morais Honorato de Souza, Lila Missae Oyama, Erika Aparecida Silveira, and et al. 2024. "Association between Serum Fatty Acids Profile and MetScore in Women with Severe Obesity" Nutrients 16, no. 20: 3508. https://doi.org/10.3390/nu16203508
APA StyleOliveira, E. S., Kattah, F. M., Lima, G. C., Horst, M. A., Figueiredo, N., Lima, G. B., Whitton, R. G. M., de Souza, G. I. d. M. H., Oyama, L. M., Silveira, E. A., & Corgosinho, F. C. (2024). Association between Serum Fatty Acids Profile and MetScore in Women with Severe Obesity. Nutrients, 16(20), 3508. https://doi.org/10.3390/nu16203508