Antiobesity and Hypolipidemic Potential of Nitraria retusa Extract in Overweight/Obese Women: A Randomized, Double-Blind, Placebo-Controlled Pilot Study

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Preparation of NRE and Placebo
2.4. Study Protocol
2.5. Nutritional Consultation
2.6. Primary/Secondary Outcomes
2.6.1. Primary Outcome
Body Weight Measurements
2.6.2. Secondary Outcomes
Anthropometric Measurements
Body Composition Measurements with Bioelectrical Impedance (BIA)
Lipid Blood Profile Analysis
Safety Analysis and Assessment
2.7. Compliance and Adverse Events
2.8. Ethical Statement
2.9. Statistical Analysis
3. Results
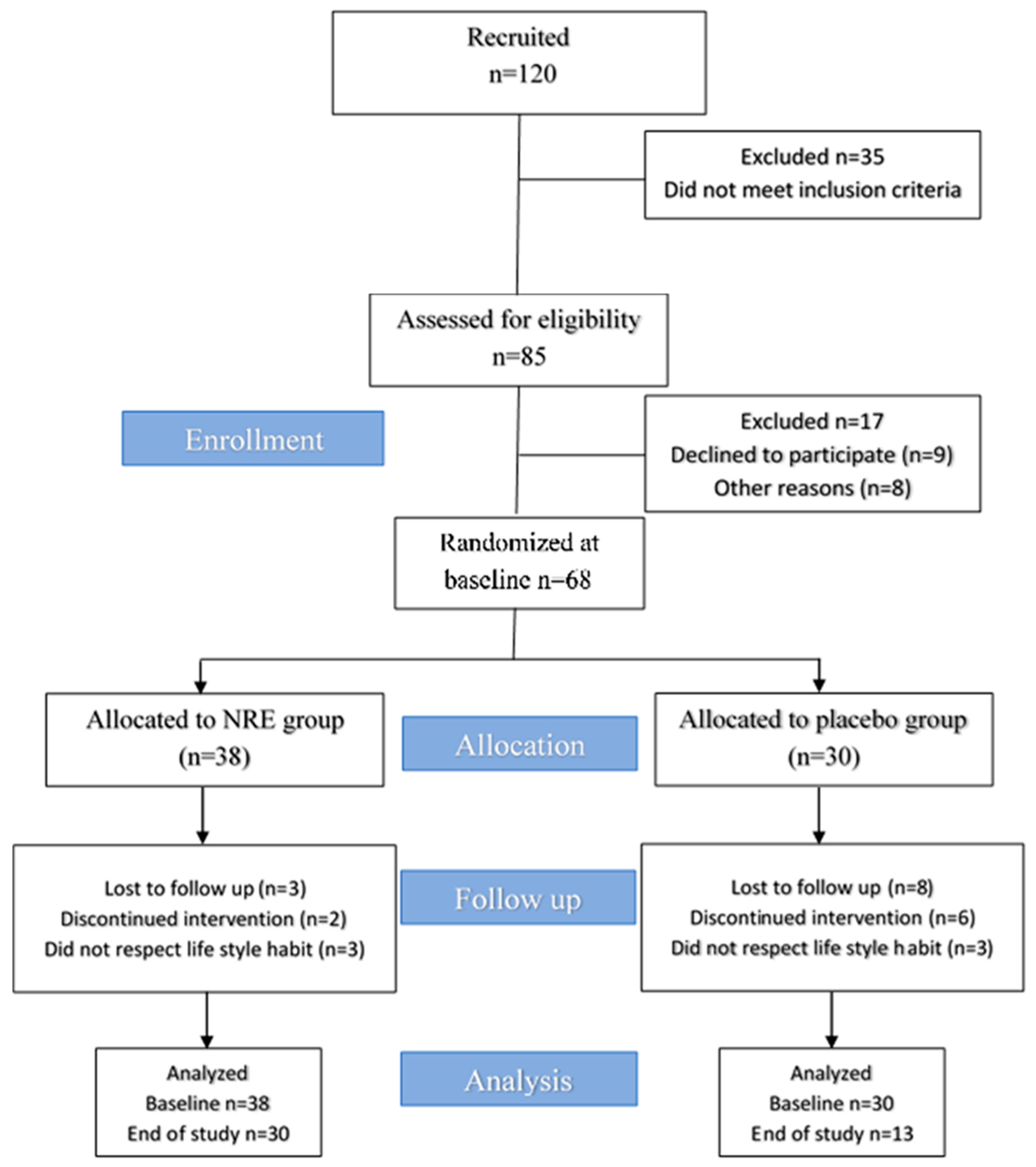
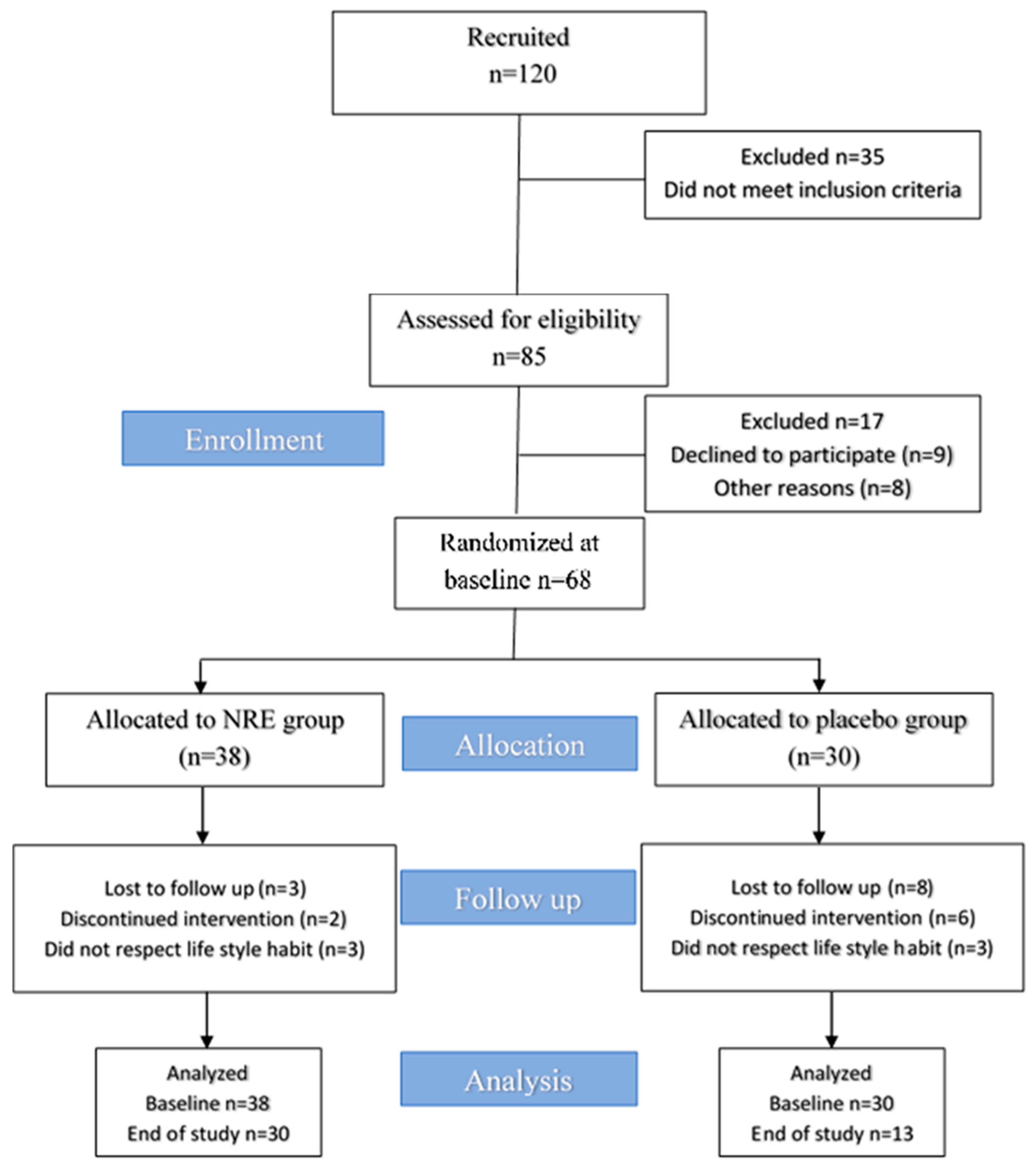
3.1. Study Flow and Participant Characteristics
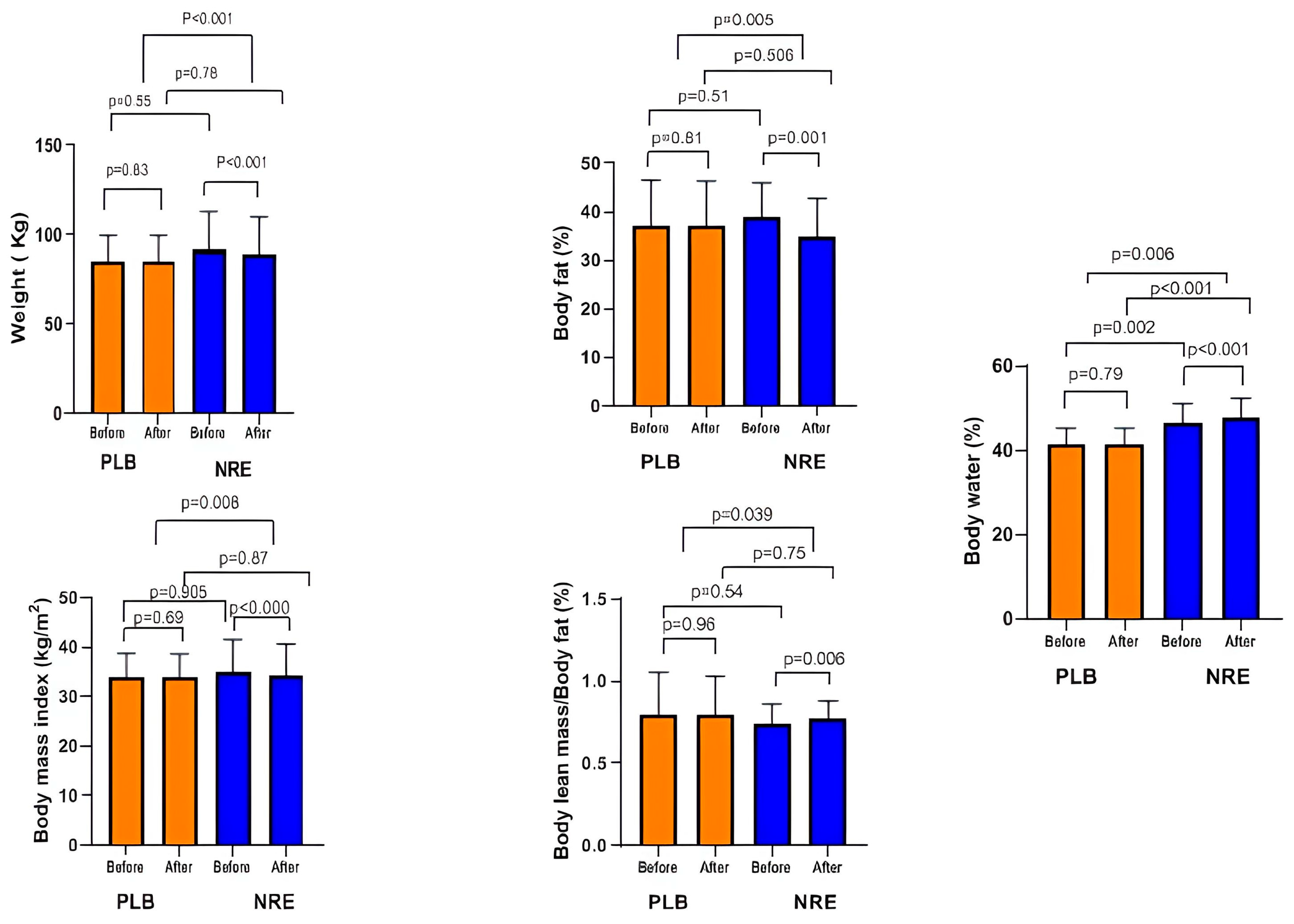
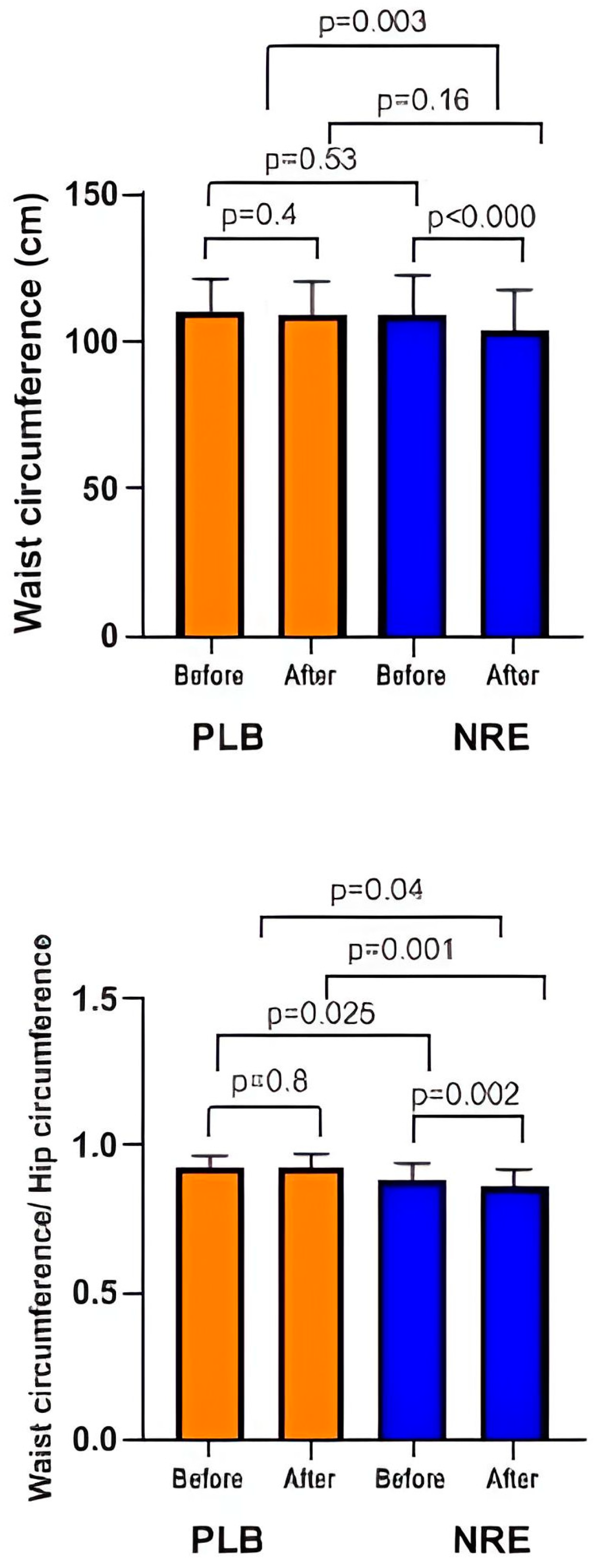
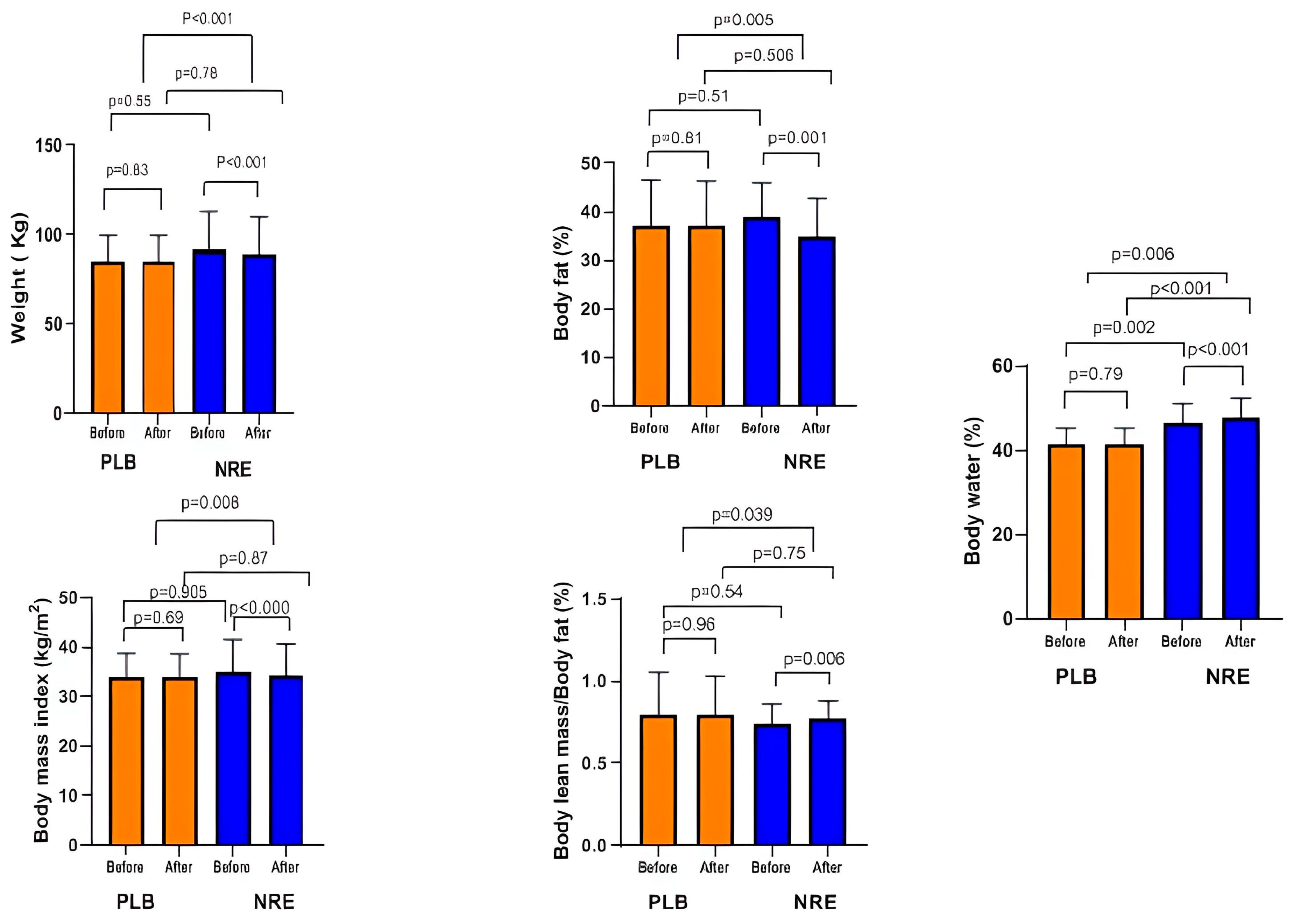
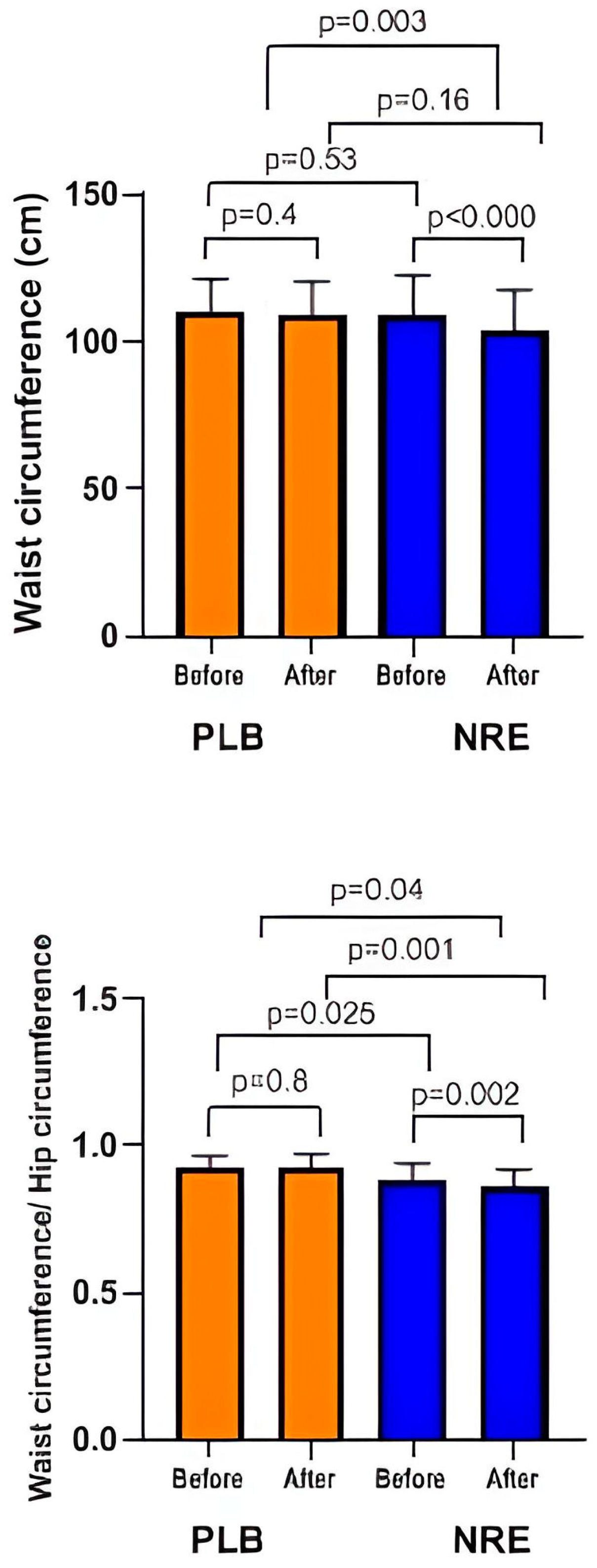
3.2. Effect of NRE Supplementation on Body Weight, Changes in Body Composition, and Anthropometric Parameters
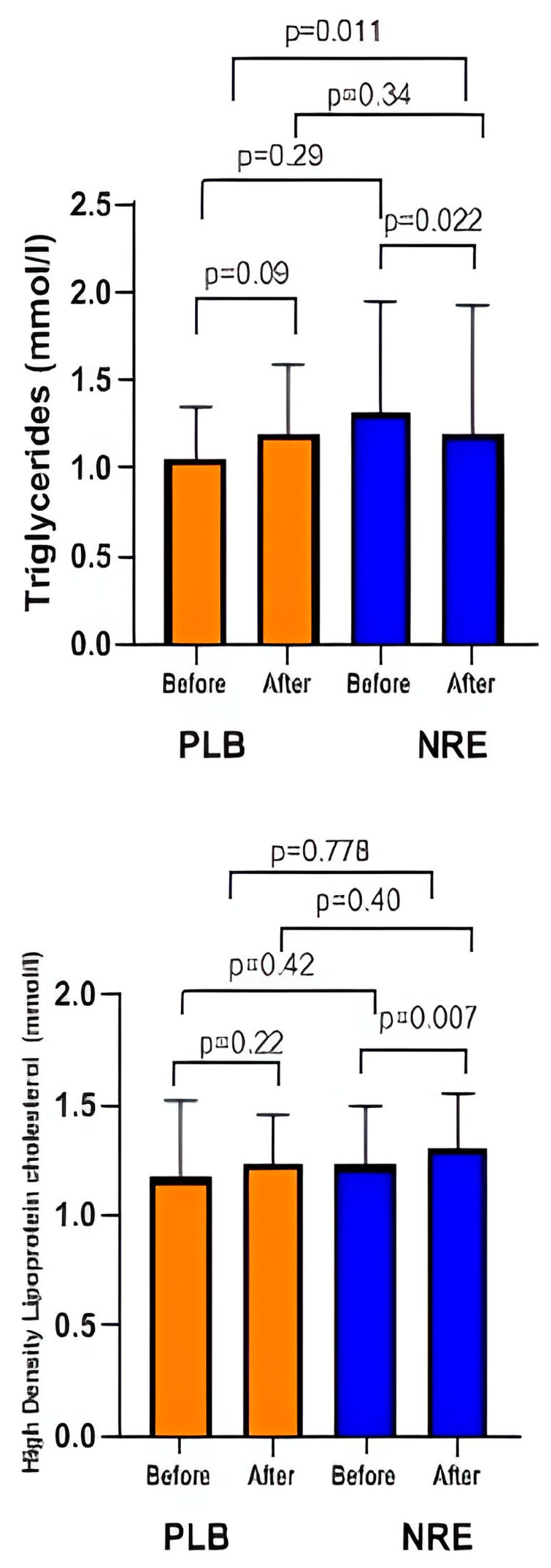
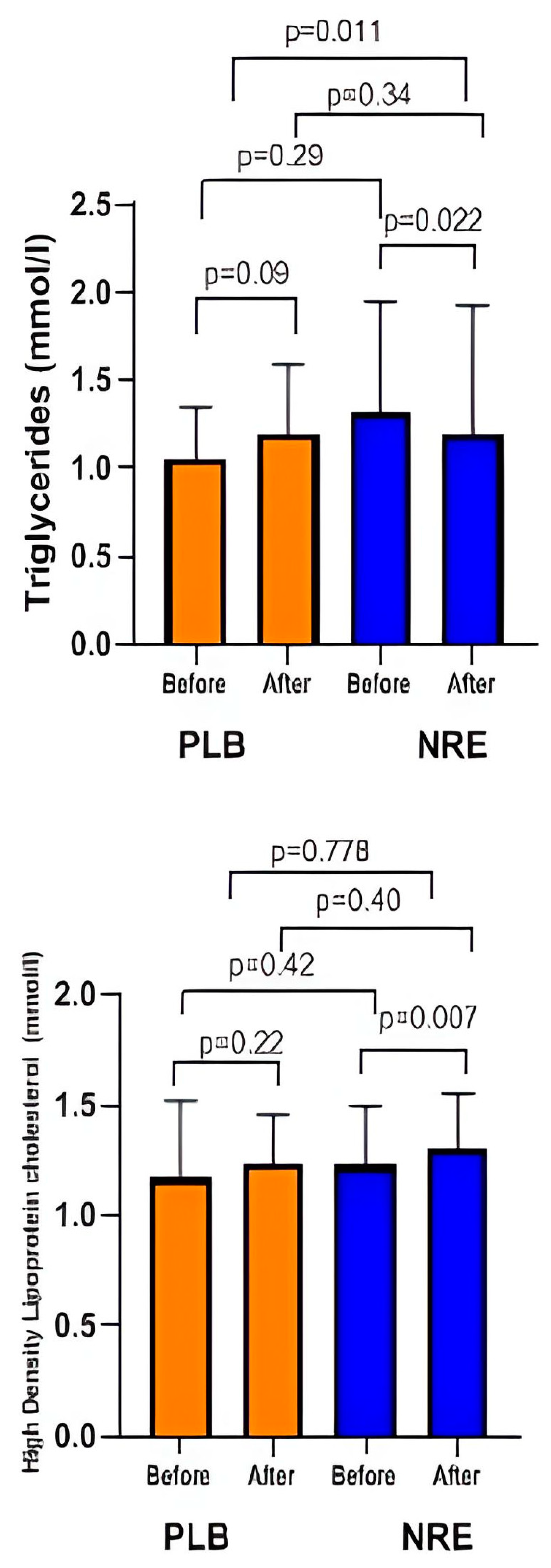
3.3. Effect of NRE Supplementation on Lipid Profile
3.4. Effect of BMI and Age on Responses to Interventions
3.5. Safety Issues and Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, B.; Choi, H.-N.; Yim, J.-E. Effect of diet on the gut microbiota associated with obesity. J. Obes. Metab. Syndr. 2019, 28, 216. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Suk, K.; Yu, R.; Kim, M.-S. Cellular contributors to hypothalamic inflammation in obesity. Mol. Cells 2020, 43, 431. [Google Scholar] [PubMed]
- Lin, Y.; Shi, D.; Su, B.; Wei, J.; Găman, M.A.; Sedanur Macit, M.; Borges do Nascimento, I.J.; Guimaraes, N.S. The effect of green tea supplementation on obesity: A systematic review and dose–response meta-analysis of randomized controlled trials. Phytother. Res. 2020, 34, 2459–2470. [Google Scholar] [CrossRef] [PubMed]
- Diels, S.; Vanden Berghe, W.; Van Hul, W. Insights into the multifactorial causation of obesity by integrated genetic and epigenetic analysis. Obes. Rev. 2020, 21, e13019. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kassie, A.M.; Abate, B.B. Prevalence of overweight/obesity among the adult population in Ethiopia: A systematic review and meta-analysis. BMJ Open 2020, 10, e039200. [Google Scholar] [CrossRef]
- Kolahi, A.-A.; Moghisi, A.; Ekhtiari, Y.S. Socio-demographic determinants of obesity indexes in Iran: Findings from a nationwide STEPS survey. Health Promot. Perspect. 2018, 8, 187. [Google Scholar] [CrossRef]
- Holdsworth, M.; El Ati, J.; Bour, A.; Kameli, Y.; Derouiche, A.; Millstone, E.; Delpeuch, F. Developing national obesity policy in middle-income countries: A case study from North Africa. Health Policy Plan. 2013, 28, 858–870. [Google Scholar] [CrossRef]
- Toselli, S.; Gualdi-Russo, E.; Boulos, D.N.; Anwar, W.A.; Lakhoua, C.; Jaouadi, I.; Khyatti, M.; Hemminki, K. Prevalence of overweight and obesity in adults from North Africa. Eur. J. Public Health 2014, 24, 31–39. [Google Scholar] [CrossRef]
- Tutunchi, H.; Ebrahimi-Mameghani, M.; Ostadrahimi, A.; Asghari-Jafarabadi, M. What are the optimal cut-off points of anthropometric indices for prediction of overweight and obesity? Predictive validity of waist circumference, waist-to-hip and waist-to-height ratios. Health Promot. Perspect. 2020, 10, 142. [Google Scholar] [CrossRef]
- Kheriji, N.; Dakhlaoui, T.; Kamoun Rebai, W.; Maatoug, S.; Thabet, M.T.; Mellah, T.; Mrad, M.; Trabelsi, H.; Soltani, M.; Kabbage, M. Prevalence and risk factors of diabetes mellitus and hypertension in North East Tunisia calling for efficient and effective actions. Sci. Rep. 2023, 13, 12706. [Google Scholar] [CrossRef] [PubMed]
- Hajer, G.R.; Van Haeften, T.W.; Visseren, F.L. Adipose tissue dysfunction in obesity, diabetes, and vascular diseases. Eur. Heart J. 2008, 29, 2959–2971. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.-H.; Liu, C.-Y.; Wang, L.-Y.; Huang, C.-J.; Hsu, C.-H. Effects of green tea extract on overweight and obese women with high levels of low density-lipoprotein-cholesterol (LDL-C): A randomised, double-blind, and cross-over placebo-controlled clinical trial. BMC Complement. Altern. Med. 2018, 18, 294. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.J.; Yeo, G.S. The genetics of obesity: From discovery to biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Mohajan, D.; Mohajan, H.K. Obesity and Its Related Diseases: A New Escalating Alarming in Global Health. J. Innov. Med. Res. 2023, 2, 12–23. [Google Scholar] [CrossRef]
- Ranganathan, S.; Krishnan, T.U.; Radhakrishnan, S. Comparison of dyslipidemia among the normal-BMI and high-BMI group of people of rural Tamil Nadu. Med. J. Dr. DY Patil Univ. 2015, 8, 149. [Google Scholar]
- Yang, M.; Liu, S.; Zhang, C. The related metabolic diseases and treatments of obesity. Healthcare 2022, 10, 1616. [Google Scholar] [CrossRef]
- Kim, K.-B.; Kim, K.; Kim, C.; Kang, S.-J.; Kim, H.J.; Yoon, S.; Shin, Y.-A. Effects of exercise on the body composition and lipid profile of individuals with obesity: A systematic review and meta-analysis. J. Obes. Metab. Syndr. 2019, 28, 278. [Google Scholar] [CrossRef]
- Roberts, C.A. Physical and psychological effects of bariatric surgery on obese adolescents: A review. Front. Pediatr. 2021, 8, 591598. [Google Scholar] [CrossRef]
- Pilitsi, E.; Farr, O.M.; Polyzos, S.A.; Perakakis, N.; Nolen-Doerr, E.; Papathanasiou, A.-E.; Mantzoros, C.S. Pharmacotherapy of obesity: Available medications and drugs under investigation. Metabolism 2019, 92, 170–192. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Oh, M.-R.; Kim, M.-G.; Chae, H.-J.; Chae, S.-W. Anti-obesity effects of Yerba Mate (Ilex Paraguariensis): A randomized, double-blind, placebo-controlled clinical trial. BMC Complement. Altern. Med. 2015, 15, 338. [Google Scholar] [CrossRef] [PubMed]
- Arya, A.; Nahar, L.; Khan, H.U.; Sarker, S.D. Anti-obesity natural products. In Annual Reports in Medicinal Chemistry; Academic Press: Cambridge, MA, USA, 2020; Volume 55, pp. 411–433. [Google Scholar]
- Kazemipoor, M.; Cordell, G.A.; Sarker, M.M.R.; Radzi, C.W.J.B.W.M.; Hajifaraji, M.; En Kiat, P. Alternative treatments for weight loss: Safety/risks and effectiveness of anti-obesity medicinal plants. Int. J. Food Prop. 2015, 18, 1942–1963. [Google Scholar] [CrossRef]
- Shende, P.; Narvenker, R. Herbal nanotherapy: A new paradigm over conventional obesity treatment. J. Drug Deliv. Sci. Technol. 2021, 61, 102291. [Google Scholar] [CrossRef]
- Cho, A.-S.; Jeon, S.-M.; Kim, M.-J.; Yeo, J.; Seo, K.-I.; Choi, M.-S.; Lee, M.-K. Chlorogenic acid exhibits anti-obesity property and improves lipid metabolism in high-fat diet-induced-obese mice. Food Chem. Toxicol. 2010, 48, 937–943. [Google Scholar] [CrossRef] [PubMed]
- Kamali, S.H.; Khalaj, A.R.; Hasani-Ranjbar, S.; Esfehani, M.M.; Kamalinejad, M.; Soheil, O.; Kamali, S.A. Efficacy of ‘Itrifal Saghir’, a combination of three medicinal plants in the treatment of obesity; A randomized controlled trial. DARU J. Pharm. Sci. 2012, 20, 33. [Google Scholar] [CrossRef]
- Perna, S.; Spadaccini, D.; Botteri, L.; Girometta, C.; Riva, A.; Allegrini, P.; Petrangolini, G.; Infantino, V.; Rondanelli, M. Efficacy of bergamot: From anti-inflammatory and anti-oxidative mechanisms to clinical applications as preventive agent for cardiovascular morbidity, skin diseases, and mood alterations. Food Sci. Nutr. 2019, 7, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Upadya, H.; Prabhu, S.; Prasad, A.; Subramanian, D.; Gupta, S.; Goel, A. A randomized, double blind, placebo controlled, multicenter clinical trial to assess the efficacy and safety of Emblica officinalis extract in patients with dyslipidemia. BMC Complement. Altern. Med. 2019, 19, 27. [Google Scholar] [CrossRef]
- Majd, F.S.; Talebi, S.S.; Ahmad Abadi, A.N.; Poorolajal, J.; Dastan, D. Efficacy of a standardized herbal product from Pistacia atlantica subsp. Kurdica in type 2 diabetic patients with hyperlipidemia: A triple-blind randomized clinical trial. Complement. Ther. Clin. Pract. 2022, 48, 101613. [Google Scholar] [CrossRef]
- Zielinska-Blizniewska, H.; Sitarek, P.; Merecz-Sadowska, A.; Malinowska, K.; Zajdel, K.; Jablonska, M.; Sliwinski, T.; Zajdel, R. Plant Extracts and Reactive Oxygen Species as Two Counteracting Agents with Anti- and Pro-Obesity Properties. Int. J. Mol. Sci. 2019, 20, 4556. [Google Scholar] [CrossRef]
- Chaâbane, M.; Koubaa, M.; Soudani, N.; Elwej, A.; Grati, M.; Jamoussi, K.; Boudawara, T.; Ellouze Chaabouni, S.; Zeghal, N. Nitraria retusa fruit prevents penconazole-induced kidney injury in adult rats through modulation of oxidative stress and histopathological changes. Pharm. Biol. 2017, 55, 1061–1073. [Google Scholar] [CrossRef]
- Kalai, F.Z.; Boulaaba, M.; Ksouri, R.; Isoda, H. Identification of Main Phenolic Compounds of Nitraria Retusa Leaf and Stem Extracts and Evaluation of Their Anti-Adipogenic Activity in 3T3-L1 Cells. 2021; preprint. [Google Scholar] [CrossRef]
- Kalai, F.Z.; Han, J.; Ksouri, R.; Abdelly, C.; Isoda, H. Oral administration of Nitraria retusa ethanolic extract enhances hepatic lipid metabolism in db/db mice model ‘BKS. Cg-Dock7m+/+ Leprdb/J’through the modulation of lipogenesis–lipolysis balance. Food Chem. Toxicol. 2014, 72, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Zar Kalai, F.; Han, J.; Ksouri, R.; El Omri, A.; Abdelly, C.; Isoda, H. Antiobesity effects of an edible halophyte Nitraria retusa Forssk in 3T3-L1 preadipocyte differentiation and in C57B6J/L mice fed a high fat diet-induced obesity. Evid.-Based Complement. Altern. Med. 2013, 2013, 368658. [Google Scholar] [CrossRef] [PubMed]
- Boubaker, J.; Bhouri, W.; Sghaier, M.B.; Bouhlel, I.; Skandrani, I.; Ghedira, K.; Chekir-Ghedira, L. Leaf extracts from Nitraria retusa promote cell population growth of human cancer cells by inducing apoptosis. Cancer Cell Int. 2011, 11, 37. [Google Scholar] [CrossRef] [PubMed]
- Mariem, C.; Sameh, M.; Nadhem, S.; Soumaya, Z.; Najiba, Z.; Raoudha, E.G. Antioxidant and antimicrobial properties of the extracts from Nitraria retusa fruits and their applications to meat product preservation. Ind. Crops Prod. 2014, 55, 295–303. [Google Scholar] [CrossRef]
- Popiolek-Kalisz, J. The Impact of Dietary Flavonols on Central Obesity Parameters in Polish Adults. Nutrients 2022, 14, 5051. [Google Scholar] [CrossRef] [PubMed]
- Laouani, A.; Nasrallah, H.; Sassi, A.; Ferdousi, F.; Kalai, F.Z.; Hasni, Y.; Limem, K.; Isoda, H.; Saguem, S. Exploring the Effects of Short-Term Daily Intake of Nitraria retusa Tea on Lipid Profile: A Pre-Post, Uncontrolled Pilot Study in Both Healthy and Overweight/Obese Adults. Nutrients 2023, 15, 3649. [Google Scholar] [CrossRef] [PubMed]
- Johan Sebastian, V.-G.; Camila, P.-Z.M.; Helena, G.-C.C. Total body water in Colombian older adults through bioelectrical impedance analysis. Int. J. Bioelectromagn. 2022, 24, 178. [Google Scholar]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The Role of Water Homeostasis in Muscle Function and Frailty: A Review. Nutrients 2019, 11, 1857. [Google Scholar] [CrossRef]
- Laja García, A.I.; Moráis-Moreno, C.; Samaniego-Vaesken, M.L. Influence of Water Intake and Balance on Body Composition in Healthy Young Adults from Spain. Nutrients 2019, 11, 1923. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Lorenzo, I.; Papiol, M.; Palomera, E.; Bartolomé, M.; Pleguezuelos, E.; Burdoy, E. Intracellular Water Content in Lean Mass as an Indicator of Muscle Quality in an Older Obese Population. J. Clin. Med. 2020, 9, 1580. [Google Scholar] [CrossRef]
- Bonora, E. Relationship between regional fat distribution and insulin resistance. Int. J. Obes. 2000, 24, S32–S35. [Google Scholar] [CrossRef] [PubMed]
- Ness-Abramof, R.; Apovian, C.M. Waist circumference measurement in clinical practice. Nutr. Clin. Pract. 2008, 23, 397–404. [Google Scholar] [CrossRef]
- Ganbold, M.; Owada, Y.; Ozawa, Y.; Shimamoto, Y.; Ferdousi, F.; Tominaga, K.; Zheng, Y.-W.; Ohkohchi, N.; Isoda, H. Isorhamnetin alleviates steatosis and fibrosis in mice with nonalcoholic steatohepatitis. Sci. Rep. 2019, 9, 16210. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.-Y.; Jung, U.J.; Park, T.; Yun, J.W.; Choi, M.-S. Luteolin attenuates hepatic steatosis and insulin resistance through the interplay between the liver and adipose tissue in mice with diet-induced obesity. Diabetes 2015, 64, 1658–1669. [Google Scholar] [CrossRef] [PubMed]
- Ono, M.; Fujimori, K. Antiadipogenic Effect of Dietary Apigenin through Activation of AMPK in 3T3-L1 Cells. J. Agric. Food Chem. 2011, 59, 13346–13352. [Google Scholar] [CrossRef] [PubMed]
- Varshney, R.; Mishra, R.; Das, N.; Sircar, D.; Roy, P. A comparative analysis of various flavonoids in the regulation of obesity and diabetes: An in vitro and in vivo study. J. Funct. Foods 2019, 59, 194–205. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, C.; Torres, N.; Gutiérrez-Uribe, J.A.; Noriega, L.G.; Torre-Villalvazo, I.; Leal-Díaz, A.M.; Antunes-Ricardo, M.; Márquez-Mota, C.; Ordaz, G.; Chavez-Santoscoy, R.A. The effect of isorhamnetin glycosides extracted from Opuntia ficus-indica in a mouse model of diet induced obesity. Food Funct. 2015, 6, 805–815. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Gu, M.; Cai, W.; Yu, L.; Feng, L.; Zhang, L.; Zang, Q.; Wang, Y.; Wang, D.; Chen, H. Dietary component isorhamnetin is a PPARγ antagonist and ameliorates metabolic disorders induced by diet or leptin deficiency. Sci. Rep. 2016, 6, 19288. [Google Scholar] [CrossRef]
- Matboli, M.; Saad, M.; Hasanin, A.H.; Saleh, L.A.; Baher, W.; Bekhet, M.M.; Eissa, S. New insight into the role of isorhamnetin as a regulator of insulin signaling pathway in type 2 diabetes mellitus rat model: Molecular and computational approach. Biomed. Pharmacother. 2021, 135, 111176. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.; Jung, E.; Hwang, W.; Kim, Y.-S.; Park, D. Isorhamnetin-induced anti-adipogenesis is mediated by stabilization of β-catenin protein. Life Sci. 2010, 86, 416–423. [Google Scholar] [CrossRef]
- Lee, J.; Jung, E.; Lee, J.; Kim, S.; Huh, S.; Kim, Y.; Kim, Y.; Byun, S.Y.; Kim, Y.S.; Park, D. Isorhamnetin represses adipogenesis in 3T3-L1 cells. Obesity 2009, 17, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Farias-Pereira, R.; Savarese, J.; Yue, Y.; Lee, S.-H.; Park, Y. Fat-lowering effects of isorhamnetin are via NHR-49-dependent pathway in Caenorhabditis elegans. Curr. Res. Food Sci. 2020, 2, 70–76. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Placebo Group (n = 13) 13 Women | NRE Group (n = 30) 30 Women | p Value a | |||
|---|---|---|---|---|---|
| Variables | Mean | (SD) | Mean | (SD) | |
| Age, y (range) | 45.92 | (33–59) | 39.33 | (24–59) | 0.034 |
| Height, cm | 158.08 | (1.79) | 161.13 | (1.16) | 0.55 |
| Weight, kg | 84.83 | (4.11) | 91.43 | (3.93) | 0.322 |
| BMI, kg/m2 | 33.86 | (1.33) | 34.84 | (1.22) | 0.905 |
| Variables (Units) | Placebo Group a (n = 13) | NRE Group a (n = 30) | Between Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | After 12 Weeks | Δ b | p-Value c | Baseline | After 12 Weeks | Δ b | p-Value c | Δ d | p-Value e | Adjusted p-Value f | |
| Body composition | |||||||||||
| Weight (kg) | 84.83 (4.11) | 84.91 (4.13) | +0.08 (0.39) | 0.835 | 91.47 (3.9) | 89.20 (3.81) | −2.27 (0.31) | <0.001 | −2.35 (0.08) | <0.001 | <0.001 |
| BMI (kg/m2) | 33.86 (1.33) | 33.78 (1.33) | −0.076 (0.191) | 0.696 | 34.84 (1.22) | 34.08 (1.19) | −0.76 (0.139) | <0.001 | −0.684 (0.052) | 0.008 | 0.006 |
| BF (%) | 36.95 (2.72) | 36.95 (2.72) | +0.028 (0.23) | 0.811 | 40.31 (1.03) | 39.39 (0.91) | −0.92 (0.24) | 0.001 | −0.948 (0.01) | 0.005 | 0.047 |
| BLM (%) | 27.28 (0.71) | 27.40 (0.63) | +0.11 (0.17) | 0.676 | 29.62 (0.54) | 29.9 (0.53) | +0.27 (0.125) | 0.045 | 0.259 (0.05) | 0.058 | 0.071 |
| BLM/BF | 0.79 (0.007) | 0.79 (0.06) | −0.0025 (0.009) | 0.960 | 0.74 (0.03) | 0.76 (0.029) | +0.023 (0.006) | 0.006 | 0.0255 (0.054) | 0.039 | 0.056 |
| BW (%) | 41.50 (1.10) | 41.55 (1.08) | +0.05 (0.18) | 0.794 | 44.05 (0.88) | 44.83 (0.76) | +0.78 (0.18) | <0.001 | 0.73 (0.001) | 0.006 | 0.005 |
| Anthropometric parameters | |||||||||||
| WC (cm) | 109.8 (3.2) | 108.88 (3.2) | −0.92 (1.06) | 0.405 | 108.75 (2.52) | 104.25 (2.45) | −4.5 (0.59) | <0.001 | −3.58 (0.47) | 0.003 | 0.012 |
| WHR | 0.926 (0.11) | 0.928 (0.121) | +0.002 (0.11) | 0.805 | 0.886 (0.01) | 0.86 (0.01) | −0.21 (0.006) | 0.002 | −0.212 (0.104) | 0.04 | 0.056 |
| Mid-thigh (cm) | 57.23 (1.13) | 57 (1.02) | −0.23 (0.68) | 0.741 | 60.05 (1.31) | 57.31 (1.27) | −2.73 (0.45) | 0.002 | −2.5 (0.23) | 0.004 | 0.004 |
| Half arm (cm) | 36.92 (1.3) | 36.30 (1.43) | −0.61 (0.72) | 0.416 | 35.93 (1.04) | 33.49 (1.48) | −2.43 (1.2) | <0.001 | −1.82 (0.48) | 0.51 | 0.240 |
| Variables (Units) | Placebo Group a (n = 13) | NRE Group a (n = 30) | Between Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | After 12 Weeks | Δ b | p-Value c | Baseline | After 12 Weeks | Δ b | p-Value c | Δ d | p Value e | Adjusted p-Value f | |
| Lipid profile | |||||||||||
| HDL, mmol/L | 1.17 (0.096) | 1.228 (0.06) | +0.057 (0.07) | 0.224 | 1.22 (0.04) | 1.29 (0.046) | +0.07 (0.02) | 0.007 | 0.013 (0.05) | 0.778 | 0.985 |
| TG, mmol/L | 1.056 (0.081) | 1.19 (0.111) | +0.13 (0.07) | 0.095 | 1.32 (0.11) | 1.19 (0.13) | −0.127 (0.056) | 0.022 | −0.257 (0.014) | 0.011 | 0.016 |
| LDL, mmol/L | 3.30 (0.211) | 3.29 (0.17) | −0.006 (0.16) | 0.968 | 3.28 (0.12) | 3.25 (0.14) | −0.027 (0.10) | 0.805 | −0.021 (0.06) | 0.92 | 0.875 |
| TC, mmol/L | 4.93 (0.260) | 5.03 (0.197) | +0.09 (0.20) | 0.648 | 5.11 (0.182) | 5.12 (0.19) | +0.1 (0.09) | 0.902 | 0.01 (0.11) | 0.68 | 0.558 |
| Variables (Units) | Placebo Group a (n = 13) | NRE Group a (n = 30) | Between Groups | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | After 12 Weeks | Δ b | p-Value c | Baseline | After 12 Weeks | Δ b | p-Value c | Δ d | p-Value d | |
| Clinical parameters | ||||||||||
| SBP, mmHg | 122.31 (3.78) | 125.38 (3.511) | 3.07 (2.08) | 0.157 | 117.67 (2.97) | 119.78 (2.93) | 2.11 (1.85) | 0.860 | −0.96 (0.23) | 0.176 |
| DBP, mmHg | 73.08 (3.028) | 77.69 (3.028) | 4.61 (6.16) | 0.468 | 69.33 (1.97) | 72.67 (1.72) | 3.33 (2.1) | 0.105 | −1.28 (4.06) | 0.98 |
| Pulse rate | 73.08 (1.98) | 71.92 (2.49) | −1.15 (2.05) | 0.586 | 79.03 (1.76) | 79.77 (1.59) | 0.73 (1.54) | 0.638 | 1.88 (0.51) | 0.49 |
| Hematological parameters | ||||||||||
| RBC, 1012/L | 4.40 (0.117) | 4.298 (0.111) | −1.02 (0.09) | 0.289 | 4.35 (0.07) | 4.4 (0.09) | 0.054 (0.06) | 0.387 | 1.074 (0.03) | 0.169 |
| WBC, 109/L | 6.762 (0.504) | 6.077 (0.415) | −0.68 (0.54) | 0.230 | 6.45 (0.28) | 6.57 (0.275) | 0.123 (0.149) | 0.415 | 0.803 (0.39) | 0.172 |
| Hb, gm/dL | 12.354 (0.362) | 12.269 (0.369) | −0.08 (0.25) | 0.748 | 13.2 (0.77) | 12.18 (0.26) | −1.02 (0.70) | 0.115 | −0.94 (0.45) | 0.39 |
| Ht, % | 36.4 (0.975) | 35.85 (0.958) | −0.54 (0.72) | 0.465 | 36.76 (0.7) | 37.45 (0.68) | 0.69 (0.51) | 0.553 | 1.23 (0.21) | 0.8 |
| PLT, 109/L | 312.62 (20.44) | 277.54 (25.88) | −35.07 (32.84) | 0.307 | 268.83 (10.5) | 263.6 (10.6) | −5.23 (8.87) | 0.560 | 29.84 (23.97) | 0.195 |
| Liver Function Test | ||||||||||
| ALT, UI/L | 10.05 (1.19) | 10.08 (0.79) | 0.03 (1.18) | 0.89 | 10.4 (1.01) | 11.93 (1.24) | 1.53 (0.93) | 0.67 | 1.5 (0.25) | 0.51 |
| AST, UI/L | 18.15 (2.41) | 20.85 (0.629) | 2.69 (2.32) | 0.269 | 19.43 (0.81) | 19.8 (0.988) | 0.36 (1.15) | 0.623 | −2.33 (1.17) | 0.32 |
| ALP, UI/L | 64.69 (5.64) | 73.92 (5.50) | 9.23 (4.41) | 0.058 | 57.17 (2.53) | 60.47 (2.86) | 3.3 (1.44) | 0.166 | −5.93 (2.97) | 0.314 |
| GGT, UI/L | 22.38 (2.94) | 21.15 (0.40) | −1.23 (2.18) | 0.40 | 19.57 (2.84) | 21.37 (2.87) | 1.8 (1.69) | 0.12 | 3.03 (0.49) | 0.312 |
| BT, μmol/L | 4.92 (0.431) | 5.38 (0.488) | 0.46 (0.75) | 0.645 | 6.5 (0.649) | 6.8 (0.63) | 0.3 (0.55) | 0.035 | −0.16 (0.2) | 0.95 |
| BD, μmol/L | 1.8 (1.3) | 1.9 (1.1) | 0.1 (1.2) | 0.85 | 1.43 (0.196) | 1.46 (0.149) | 0.03 (0.45) | 0.24 | −0.07 (0.75) | 0.65 |
| sAlb, g/L | 38.15 (1.39) | 41.08 (0.738) | 2.92 (1.62) | 0.181 | 40.94 (0.41) | 40.58 (1.31) | −0.36 (1.41) | 0.113 | −3.28 (0.21) | 0.49 |
| Renal Function Test | ||||||||||
| sCr, μmol/L | 59.15 (2.71) | 56.38 (3.48) | −2.76 (3.4) | 0.166 | 58.03 (1.7) | 56.77 (1.57) | −1.26 (1.18) | 0.296 | 1.5 (2.22) | 0.64 |
| BUN, mmol/L | 4.41 (0.33) | 4.64 (0.40) | 0.23 (0.83) | 0.38 | 4.03 (0.2) | 4.42 (0.32) | 0.39 (0.45) | 0.066 | 0.16 (0.38) | 0.341 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laouani, A.; Nasrallah, H.; Sassi, A.; Ferdousi, F.; Kalai, F.Z.; Hasni, Y.; Isoda, H.; Saguem, S. Antiobesity and Hypolipidemic Potential of Nitraria retusa Extract in Overweight/Obese Women: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Nutrients 2024, 16, 317. https://doi.org/10.3390/nu16020317
Laouani A, Nasrallah H, Sassi A, Ferdousi F, Kalai FZ, Hasni Y, Isoda H, Saguem S. Antiobesity and Hypolipidemic Potential of Nitraria retusa Extract in Overweight/Obese Women: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Nutrients. 2024; 16(2):317. https://doi.org/10.3390/nu16020317
Chicago/Turabian StyleLaouani, Aicha, Hana Nasrallah, Awatef Sassi, Farhana Ferdousi, Feten Zar Kalai, Yosra Hasni, Hiroko Isoda, and Saad Saguem. 2024. "Antiobesity and Hypolipidemic Potential of Nitraria retusa Extract in Overweight/Obese Women: A Randomized, Double-Blind, Placebo-Controlled Pilot Study" Nutrients 16, no. 2: 317. https://doi.org/10.3390/nu16020317
APA StyleLaouani, A., Nasrallah, H., Sassi, A., Ferdousi, F., Kalai, F. Z., Hasni, Y., Isoda, H., & Saguem, S. (2024). Antiobesity and Hypolipidemic Potential of Nitraria retusa Extract in Overweight/Obese Women: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Nutrients, 16(2), 317. https://doi.org/10.3390/nu16020317