
Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials

 ,
,  ,
, 
Abstract
1. Introduction
- ➢
- What aging-related outcomes have been examined in RCTs of IF and CR?
- ➢
- What are the within-study effects of IF and CR on cardiometabolic, cancer-specific, and neurocognitive outcomes compared with controls in adults?
- ➢
- What are the differences in the effects of CR versus IF RCT interventions on neurocognitive, cardiometabolic, and cancer domain-specific outcomes in adults?
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Search
2.3. Eligibility Criteria
2.4. Screening and Data Extraction
3. Results
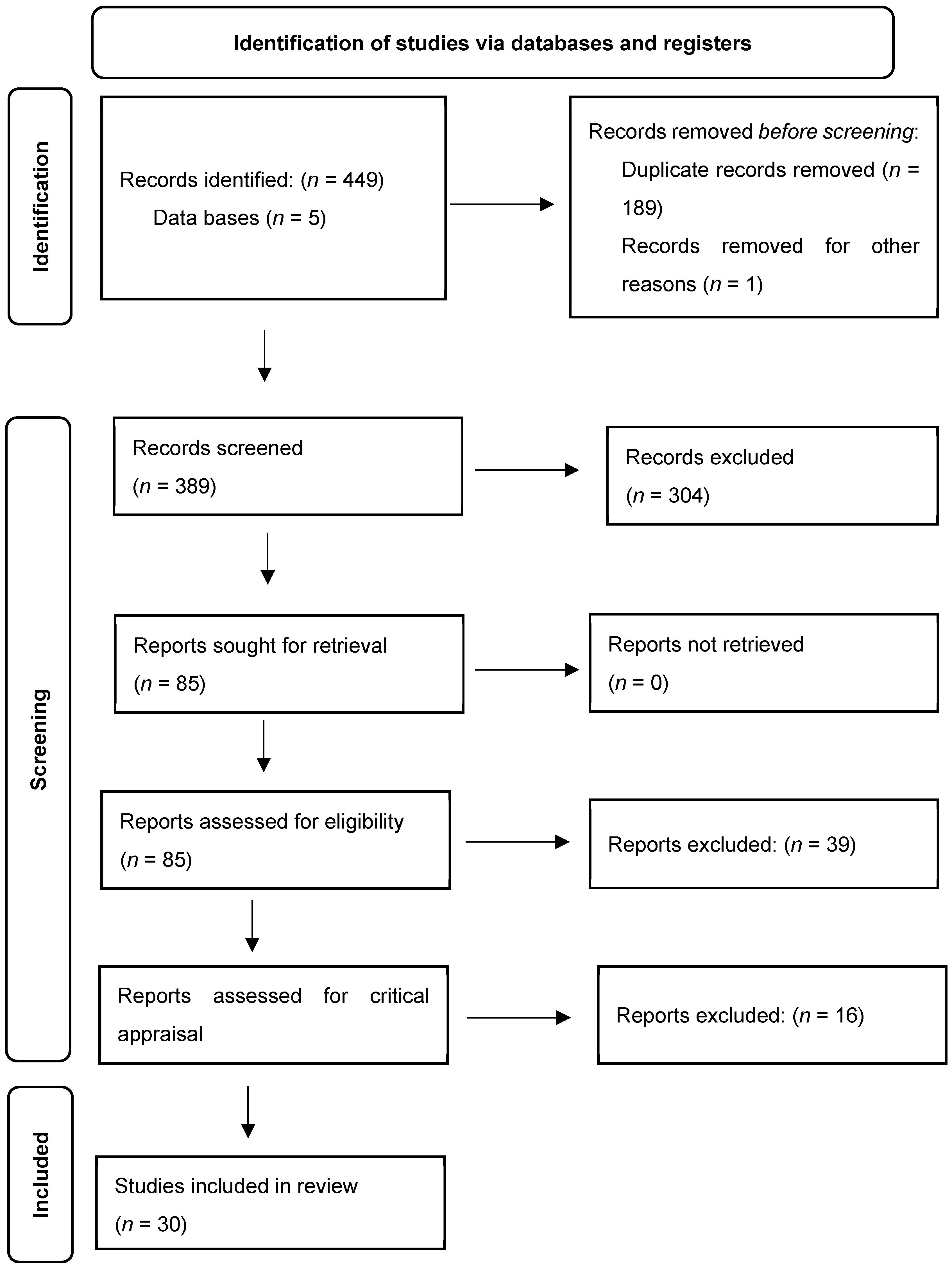
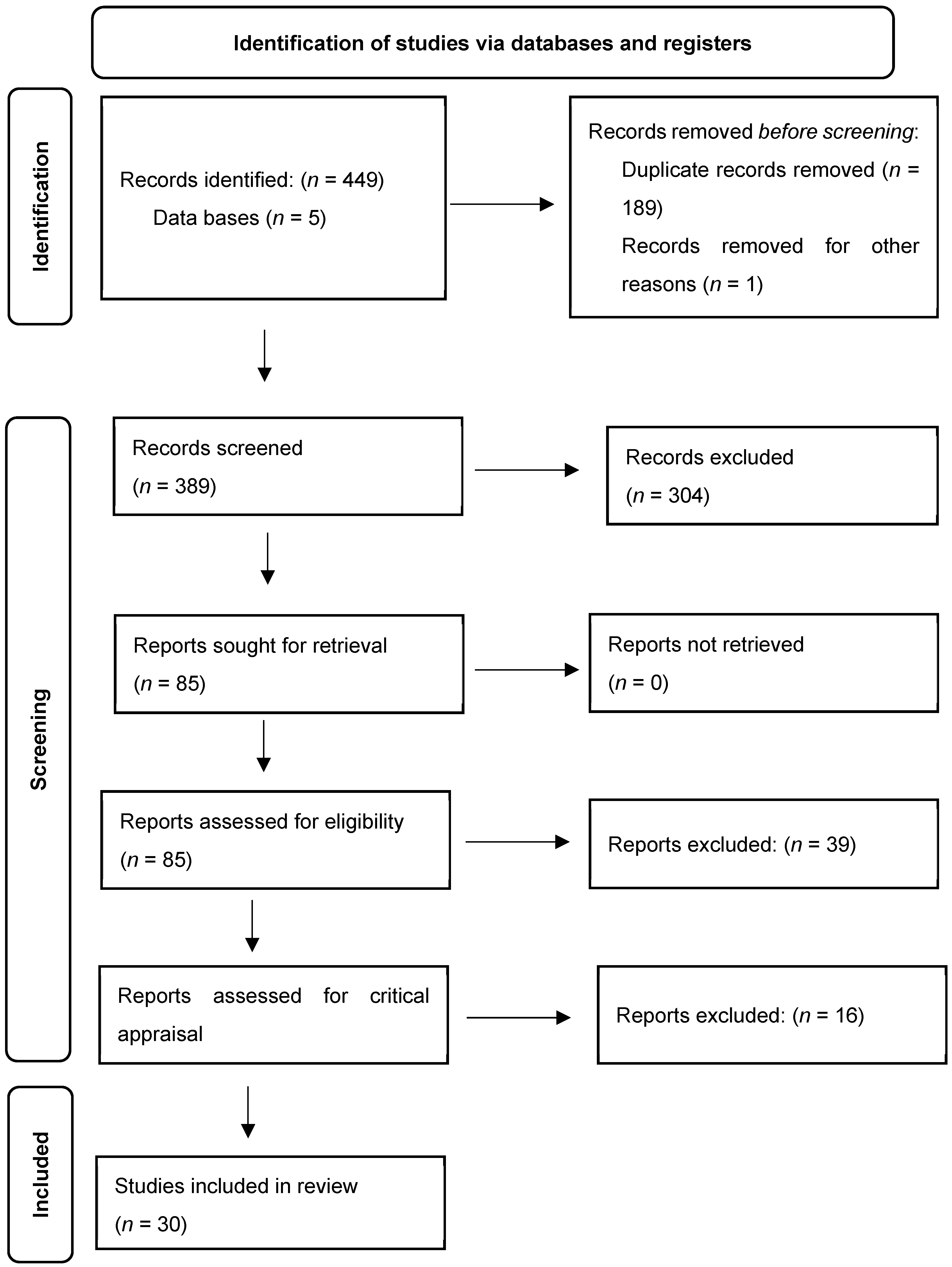
3.1. Search Results
3.2. Study Characteristics
3.3. CR Interventions

{kind=link}
| Reference | Participant Characteristics a | Intervention(s) | Duration | Design | Outcome(s) b |
|---|---|---|---|---|---|
| ~Calorie Restriction (n = 10)~ | |||||
| Dengo et al., 2010 [28] | Healthy individuals, n = 36 (CR, n = 25/CON, n = 11); 55–75 yrs.; 58% F; BMI: CR, 30.0 ± 0.6 kg/m2/CON, 31.8 ± 1.4 kg/m2 | Hypocaloric diet (1200–1500 kcal), based on the US Department of Agriculture food pyramid guidelines | 3 mo | Parallel-group RCT | ↓ Body weight ↓ Body fat ↓ Abdominal adiposity ↓ Blood pressure ↓ Β-Stiffness index ↓ Carotid-femoral pulse wave velocity |
| Fontana et al., 2007 [29] | Healthy, nonobese individuals, n = 46 (CR, n = 18/HL, n = 10); 50–60 yrs.; 63% F; BMI: 23.5–29.9 kg/m2 | ↓ kcal intake 16% first 3 mo.; ↓ kcal intake 20% remaining 9 mo. | 12 mo | Parallel-group RCT | ↓ Body fat ↓ LDL-cholesterol ↓ Total cholesterol/HDL ratio ↓ HOMA-IR index ↓ CRP |
| Pierce et al., 2008 [32] | Overweight/obese, non-diabetic individuals, n = 40 (CR, n = 26/CON, n = 14); 21–69 yrs.; CR, 42% F/CON, 36% F; BMI: ≥25–<40 kg/m2 | ↓ kcal intake designed to meet a goal of 10% weight loss/12 weeks (>1200 kcal/day) | 4 mo | Parallel-group RCT | ↓ Body weight ↓ Total and abdominal body fat ↓ Plasma leptin ↓ Oxidized low-density lipoprotein ↑ Brachial artery flow-mediated dilation |
| Ravussin et al., 2015 [33] | Healthy, nonobese individuals, n = 218 (CR, n = 143/CON, n = 75); 21–51 yrs.; 69.7% F; BMI: 21.9–28.0 kg/m2 | ↓ kcal intake 25% | 24 mo | Parallel-group RCT | CR achieved 11.7 ± 0.7% ↓ kcal intake ↓ 10.4 ± 0.4% weight loss ↓ Triiodothyronine ↓ TNF-α No adverse effects on quality of life |
| Redman et al., 2018 [34] | Healthy, nonobese individuals n = 53 (CR, n = 34/CON, n = 19); 39.8 ± 6.3 yrs.; 68% F; BMI: 22.0–27.9 kg/m2 | ↓ kcal intake 25% | 24 mo | Parallel-group RCT | ↓ Body weight ↓ Energy expenditure (sleep) ↓ Triiodothyronine ↓ Urinary F2-isoprostane |
| Tam et al., 2012 [37] | Healthy, overweight individuals, n = 23 (CR, n = 12/CON, n = 11); CR, 38.4 ± 1.6 yrs./CON, 37.7 ± 2.2 yrs.; 54% F; BMI: 27.8 ± 0.7 kg/m2 | ↓ kcal intake 25% | 6 mo | Parallel-group RCT | ↓ Body weight ↓ Fat mass ↓ Visceral fat ↑ Insulin sensitivity ↓ Leptin |
| Wei et al., 2017 [39] | Healthy individuals, n = 100 (FMD, n = 52/CON, n = 48); FMD, 42.2 ± 12.5 years/CON, 43.3 ± 11.7 years; FMD, 62.5% F/CON, 63.5% F; BMI: FMD, 27.8 ± 5.1/CON, 26.6 ± 4.9 kg/m2 | FMD, low in calories, sugars, and protein but high in unsaturated fats | 3 mo | Parallel-group RCT | ↓ Body weight ↓ Trunk fat ↓ Total body fat ↓ Blood pressure ↓ IGF-1 |
| Prehn et al., 2017 [43] | Obese, postmenopausal, n = 37 (CR, n = 19/CON, n = 18); CR, 61 ± 4 yrs./CON, 61 ± 6 yrs.; 100% F; BMI: CR, 35.0 ± 3.7 kg/m2/CON, 34.7 ± 4.3 kg/m2 | Wks. 1–8: low-caloric formula diet (800 kcal/day); Wks. 9–12: energy-reduced diet | 4 mo | Parallel-group RCT | ↓ Body weight ↑ Recognition memory ↑ Gray matter volume in the inferior frontal gyrus and hippocampus ↑ Hippocampal resting-state functional connectivity to parietal areas |
| Weiss et al., 2006 [40] | Healthy sedentary individuals, n = 34 (CR, n = 21/CON, n = 13); 50–60 yrs.; CR, 61% F/CON, 60% F; BMI: 23.5–29.9 kg/m2 | ↓ kcal intake 16% first 3 mo.; ↓ kcal intake 20% remaining 9 mo. | 12 mo | Parallel-group RCT | ↑ Insulin sensitivity index ↓ Glucose and insulin AUC ↑ Adiponectin ↓ TNF-α/adiponectin |
| Coutinho et al., 2018 [51] | Obese individuals, n = 35 (IER, n = 18/CR, n = 17); 39 ± 9 yrs.; 93% F; BMI: 36 ± 4 kg/m2 | ↓ kcal intake 33% | 3 mo | Parallel-group RCT | ↓ Resting metabolic rate (IER) ↑ Basal and postprandial ghrelin (IER) ↓ Basal active GLP-1 (CR) |
3.4. IF Interventions
| Reference | Participant Characteristics a | Intervention(s) | Duration | Design | Outcome(s) b |
|---|---|---|---|---|---|
| ~Intermittent Fasting (n = 12)~ | |||||
| Cienfuegos et al., 2020 [27] | Healthy, overweight individuals, n = 49 (4 h IF, n = 16/6 h IF, n = 19/CON, n = 14); 4 h IF, 49 ± 2 yrs./6h IF, 46 ± 3 yrs./CON, 45 ± 2 yrs.; 4 h IF, 88% F/6 h IF 95% F/CON 86% F; BMI: 4 h IF, 36 ± 1 kg/m2/6 h IF 37 ± 1 kg/m2/CON 36 ± 1 kg/m2 | 4 h and 6 h restricted feeding (TRF) | 2.5 mo | Parallel-group RCT | ↓ Body weight (4 h IF and 6 h IF) ↓ insulin resistance (4 h IF and 6 h IF) ↓ oxidative stress (4 h IF and 6 h IF) |
| Lowe et al., 2020 [30] | n = 116 (IF, n = 59/CON, n = 57); IF, 46.5 ± 10.5 yrs./CON, 46.1 ± 10.3 yrs.; IF, 40.7% F/CON 38.6% F; BMI: IF, 32.9 ± 4.9 kg/m2/CON, 32.6 ± 3.4 kg/m2 | 16:8 time-restricted eating, eat ad libitum from 12:00 PM–8:00 PM; abstain from caloric intake from 8:00 PM–12:00 PM the following day. | 4 mo | Parallel-group RCT | ↓ Body weight ↓ Appendicular lean mass |
| Martens et al., 2020 [31] | Healthy individuals, n = 22; 55–79 yrs.; BMI: 24.7 ± 0.6 kg/m2 | Time-restricted feeding, <8 h/day | 1.5 mo | Randomized crossover | ↓ hunger No influence on lean mass No influence on bone density ↑ Functional capacity improved ↑ Glucose tolerance improved |
| Stote et al., 2007 [35] | Healthy normal-weight adults, n = 15; 40–50 yrs.; 66.66% F; BMI: 23.4 ± 0.529 kg/m2 | ↓ meal frequency diet; 1 meal/day. | 2 mo | Randomized crossover | ↑ hunger ↓ fat mass ↑ BP ↑ LDL ↑ HDL ↓ Cortisol |
| Sutton et al., 2018 [36] | Overweight men with prediabetes, n = 8; 56 ± 9 yrs.; BMI: 32.2 ± 4.4 kg/m2 | eTRF schedule (6-h daily eating period, with dinner before 15:00 h). | 1.25 mo | Randomized crossover | ↑ Insulin sensitivity ↑ β cell responsiveness ↑ BP |
| Xie et al., 2022 [49] | Overweight individuals, n = 82 (eTRF, n = 28/mTRF, n = 26/CON, n = 28); eTRF, 28.7 ± 3.1 yrs./mTRF, 31.1 ± 8.4 yrs./CON, 33.6 ± 11.6 yrs.; eTRF, 85.7% F/mTRF 73.1% F/CON 75% F; BMI: eTRF, 22.7 ± 3.1 kg/m2/mTRF, 21.4 ± 2.2 kg/m2/CON, 21.5 ± 2.9 kg/m2 | eTRF, mTRF | 1.25 mo | Parallel-group RCT | ↑ Insulin sensitivity ↑ fasting glucose (eTRF) ↓ body mass (eTRF) ↓ adiposity (eTRF) ↓ inflammation (eTRF) ↑ gut microbial diversity (eTRF) |
| Domaszewski et al., 2020 [53] | Non-smoking women, age > 60, n = 45 (IF, n = 25/CON, n = 20); IF, 65 ± 4.0 yrs./CON, 66 ± 4.7 yrs.; 65 ± 5 yrs.; IF, 100% F/CON 100% F; BMI: 72.4 ± 12.6 kg/m2 | Abstinence from food intake for 16h/day, from 20:00 p.m. to 12:00 a.m. (the next day) | 1.5 mo | Parallel-group RCT | ↓ Body weight ↓ Fat Mass |
| Ezpeleta et al., 2023 [42] | Individuals with obesity and NAFLD, n = 39 (ADF, n = 19/CON, n = 20); ADF, 44 ± 16 yrs./CON, 44 ± 12 yrs.; ADF, 80% F/CON 80% F; BMI: ADF, 36 ± 8 kg/m2/CON, 37 ± 5 kg/m2 | ADF | 3 mo | Parallel-group RCT | ↓ Body weight ↓ Fat mass ↓ BMI ↓Fasting insulin ↓HOMA-IR ↓Fasting glucose |
| Cho et al., 2019 [54] | Overweight/obese individuals, n = 31 (IF, n = 9/CON, n = 5); IF, 33.5 ± 5 yrs./CON, 42.6 ± 10.6 yrs.; IF 75% F/CON 40% F; BMI: IF, 27.8 ± 3.4 kg/m2/CON 25.8 ± 3.4 kg/m2 | ADF | 2 mo | Parallel-group RCT | ↓ Body weight ↓ Fasting glucose ↑ Cholesterol metabolisms |
| Stekovic et al., 2019 [55] | Healthy, non-obese individuals, n = 90 (IF, n = 30/CON, n = 60) | ADF | 1 mo | Parallel-group RCT | ↓ fat mass ↑ fat-to-lean ratio ↓ LDL ↓ triodothyronine |
| Holmer et al., 2021 [52] | Individuals with w/non-alcoholic fatty liver disease, n = 49 (IF, n = 25/CON, n = 24); IF, 57 ± 10 yrs./CON, 56 ±9 yrs.; IF, 48% F/CON 71% F; BMI: IF, 32.3 ± 2.7 kg/m2/CON, 32.9 ± 5.2 kg/m2 | 5:2 Diet | 3 mo | Parallel-group RCT | ↓ steatosis ↓ Body weight ↓ LDL levels ↑ liver stiffness |
| Bartholomew et al., 2021 [26] | Overweight individuals, n = 103 (IF, n = 50/CR, n = 53); IF, 49.3 ± 12.0 yrs./CON, 47.0 ± 9.8 yrs.; IF, 66% F/CON 67.9% F | 24 h water-only fast | 6.5 mo (4 weeks: 2×/week; 22 weeks: 1/week) | Parallel-group RCT | ↓ HOMA-IR Weight NS BDNF NS |
3.5. IF and CR Interventions Combined and Compared
| Reference | Participant Characteristics a | Intervention(s) | Duration | Design | Outcome(s) b |
|---|---|---|---|---|---|
| ~Combined Calorie Restriction and Intermittent Fasting (n = 8)~ | |||||
| Trepanowski et al., 2017 [38] | Overweight/obese individuals, n = 79 (ADF, n = 22/CR, n= 29/CON, n = 25); ADF, 46 ± 2 yrs./CR, 44 ± 2 yrs./CON, 44 ± 2 yrs.; ADF, 88% F/CR, 79%F/CON, 84%F; BMI: ADF, 34 ± 1. kg/m2/CR, 35 ± 1 kg/m2/CON, 34 ± 1 kg/m2 | ↓ kcal intake 25%; ADF, 25% of energy needs on fast days, 125% of energy needs on alternating “feast days” | 12 mo | Parallel-group RCT | ↑ FFM: total mass ratio (ADF and CR) ↓Circulating leptin (ADF and CR) |
| Lin et al., 2023 [41] | Individuals with obesity, n = 77 (TRE, n = 26/CR, n = 25/CON, n = 26); TRE, 44 ± 12 yrs./CR, 44 ± 9 yrs./CON 44 ± 13 yrs.; TRE, 25% F/CR, 24% F/CON 25% F; BMI: TRE, 37 ± 6 kg/m2/CR, 37 ± 5 kg/m2/CON, 38 ± 5 kg/m2 | TRE, eating between noon and 8:00 p.m. only, CR, daily energy deficit ↓ 25% | 12 mo | Parallel-group RCT | ↓ Fat mass (TRE and CR) ↓ Waist circumference (TRE and CR) ↓ BMI (TRE and CR) ↑ Insulin sensitivity (TRE) |
| Schübel et al., 2018 [44] | Overweight/obese non-smokers, n = 150 (ICR, n = 49/CCR, n= 49/CON, n = 52); ADF, 49.4 ± 9.0 yrs./CCR, 50.5 ± 8.0 yrs./CON, 50.7 ± 7.1 yrs.; ICR, 49% F/CCR, 49%F/CON, 52%F; BMI: ICR, 32.0 ± 3.8 kg/m2/CCR, 31.2 ± 4.0 kg/m2/CON, 31.1 ± 3.6 kg/m2 | ICR, 5:2 diet, (5 d without energy restriction and 2 d with ↓ 75% energy deficit; CCR, daily energy deficit ↓ 20% | 12.5 mo | Parallel-group RCT | No significant differences between ICR and CCR regarding various circulating metabolic biomarkers. |
| Teng et al., 2011 [45] | Healthy men, n = 25 (FCR, n = 12/CON, n = 13); FCR, 59.3 ± 3.4 yrs./CON, 58.3 ± 6.3 yrs.; 0% F; BMI: FCR, 27.0 ± 1.7 kg/m2, CON, 25.0 ± 2.9 kg/m2 | ↓ kcal intake to 300–500/day; 2×/week Muslim sunnah fasting (FCR) | 3 mo | Parallel-group RCT | ↓ Body weight ↓ BMI ↓ Body fat percentage ↓ depression ↑ energy |
| Teng et al., 2013 [46] | Healthy men, n = 56 (FCR, n = 28/CON, n = 28); FCR, 59.6 ± 5.4 yrs./CON, 59.1 ± 6.2 yrs.; 58.8 ± 5.1 yrs.; 0% F; BMI: FCR, 26.8 ± 1.7 kg/m2, CON, 26.7 ± 2.3 kg/m2 | ↓ kcal intake to 300–500/day; 2×/week Muslim sunnah fasting (FCR) | 3 mo | Parallel-group RCT | ↓ Energy intake (~18%) ↓ Body weight ↓ BMI ↓ Fat percentage ↓ Fat mass ↓ Blood Pressure ↓Total cholesterol ↓ Low-density lipoprotein cholesterol ↓ Ratio of total cholesterol/high-density lipoprotein cholesterol ↓ DNA rejoining cells ↓MDA |
| Johari et al., 2020 [47] | Individuals w/non-alcoholic fatty liver disease, n = 43 (MACR, n = 33/CON, n = 10); MACR, 45.33 ± 10.77 yrs./CON, 52.60 ± 12.03 yrs.; MACR, 27% F/CON, 10% F; BMI: MACR, 31.60 ± 5.19 kg/m2/CON, 28.21 ± 3.32 kg/m2 | MACR | 2 mo | Parallel-group RCT | ↓ Body weight ↓ BMI |
| Cai et al., 2019 [48] | Individuals w/non-alcoholic fatty liver disease, n = 264 (ADF, n = 90/TRF, n= 95/CON, n = 79); ADF, 35.5 ± 4.417 yrs./TRF, 33.56 ± 6.23 yrs./CON, 34.54 ± 6.96 yrs.; ADF, 66% F/TRF, 69%F/CON, 52%F; BMI: ADF, 75.32 ± 8.53 kg/m2/TRF, 74.98 ± 8.02 kg/m2/CON, 72.94 ± 8.00 kg/m2 | ADF, TRF | 3 mo | Parallel-group RCT | ↓ Body weight (ADF and TRF) ↓ Fat mass (ADF and TRF) ↓ Total cholesterol (ADF) ↓ Serum triglycerides (ADF and TRF) |
| Hajek et al., 2021 [50] | Obese individuals, n = 284 (5:2SH, n = 95/5:2G, n= 94/CON, n = 95); 5:2SH, 51 ± 13 yrs./5:2G, 47 ± 13 yrs./CON, 47 ± 13 yrs.; 5:2SH, 68% F/5:2G, 67%F/SBA, 64%F; BMI: 5:2SH, 33.4 ± (31.7–37.7) kg/m2/5:2G, 34.0 ± (31.7–37.7) kg/m2/CON, 34.0 ± (30.7–37.7) kg/m2 | 5:2 Diet | 12 mo | Parallel-group RCT | ↓ Body weight (5:2SH, 5:2G, and CON) |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Crittenden, A.N.; Schnorr, S.L. Current Views on Hunter-gatherer Nutrition and the Evolution of the Human Diet. Am. J. Phys. Anthropol. 2017, 162, 84–109. [Google Scholar] [CrossRef] [PubMed]
- Vynck, J.C.D.; Anderson, R.; Atwater, C.; Cowling, R.M.; Fisher, E.C.; Marean, C.W.; Walker, R.S.; Hill, K. Return Rates from Intertidal Foraging from Blombos Cave to Pinnacle Point: Understanding Early Human Economies. J. Hum. Evol. 2016, 92, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Bloomer, R.J. The Impact of Religious Fasting on Human Health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of Intermittent Fasting on Health and Disease Processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Most, J.; Tosti, V.; Redman, L.M.; Fontana, L. Calorie Restriction in Humans: An Update. Ageing Res. Rev. 2017, 39, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Holben, D.H.; Marshall, M.B. Position of the Academy of Nutrition and Dietetics: Food Insecurity in the United States. J. Acad. Nutr. Diet. 2017, 117, 1991–2002. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef]
- Longo, V.D.; Tano, M.D.; Mattson, M.P.; Guidi, N. Intermittent and Periodic Fasting, Longevity and Disease. Nat. Aging 2021, 1, 47–59. [Google Scholar] [CrossRef]
- Heilbronn, L.K.; de Jonge, L.; Frisard, M.I.; DeLany, J.P.; Larson-Meyer, D.E.; Rood, J.; Nguyen, T.; Martin, C.K.; Volaufova, J.; Most, M.M.; et al. Effect of 6-Month Calorie Restriction on Biomarkers of Longevity, Metabolic Adaptation, and Oxidative Stress in Overweight Individuals: A Randomized Controlled Trial. JAMA 2006, 295, 1539–1548. [Google Scholar] [CrossRef]
- Redman, L.M.; Heilbronn, L.K.; Martin, C.K.; Alfonso, A.; Smith, S.R.; Ravussin, E.; Team, P.C. Effect of Calorie Restriction with or without Exercise on Body Composition and Fat Distribution. J. Clin. Endocrinol. Metab. 2007, 92, 865–872. [Google Scholar] [CrossRef]
- Kraus, W.E.; Bhapkar, M.; Huffman, K.M.; Pieper, C.F.; Das, S.K.; Redman, L.M.; Villareal, D.T.; Rochon, J.; Roberts, S.B.; Ravussin, E.; et al. 2 Years of Calorie Restriction and Cardiometabolic Risk (CALERIE): Exploratory Outcomes of a Multicentre, Phase 2, Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Lamos, E.M.; Malek, R.; Munir, K.M. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2020, 382, 1771–1774. [Google Scholar] [CrossRef] [PubMed]
- Romashkan, S.V.; Das, S.K.; Villareal, D.T.; Ravussin, E.; Redman, L.M.; Rochon, J.; Bhapkar, M.; Kraus, W.E.; Group, C.S. Safety of Two-Year Caloric Restriction in Non-Obese Healthy Individuals. Oncotarget 2016, 7, 19124–19133. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Huang, Y.; Huang, C.; Yang, S.; Wei, X.; Zhang, P.; Guo, D.; Lin, J.; Xu, B.; Li, C.; et al. Calorie Restriction with or without Time-Restricted Eating in Weight Loss. N. Engl. J. Med. 2022, 386, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Meyer, T.E.; Klein, S.; Holloszy, J.O. Long-Term Calorie Restriction Is Highly Effective in Reducing the Risk for Atherosclerosis in Humans. Proc. Natl. Acad. Sci. USA 2004, 101, 6659–6663. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Klein, S.; Holloszy, J.O. Effects of Long-Term Calorie Restriction and Endurance Exercise on Glucose Tolerance, Insulin Action, and Adipokine Production. Age 2010, 32, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Antoni, R.; Johnston, K.L.; Collins, A.L.; Robertson, M.D. Intermittent v. Continuous Energy Restriction: Differential Effects on Postprandial Glucose and Lipid Metabolism Following Matched Weight Loss in Overweight/Obese Participants. Br. J. Nutr. 2018, 119, 507–516. [Google Scholar] [CrossRef]
- Abdulsada, M.M.; Wilhelm, Z.R.; Opekun, A.R.; Devaraj, S.; Jalal, P.K.; Mindikoglu, A.L. The Effect of Four-Week Intermittent Fasting from Dawn to Sunset on Circulating Brain-Derived Neurotrophic Factor Levels in Subjects with Metabolic Syndrome and Healthy Subjects. Metab. Open 2021, 9, 100070. [Google Scholar] [CrossRef]
- Bagherniya, M.; Butler, A.E.; Barreto, G.E.; Sahebkar, A. The Effect of Fasting or Calorie Restriction on Autophagy Induction: A Review of the Literature. Ageing Res. Rev. 2018, 47, 183–197. [Google Scholar] [CrossRef]
- Duszka, K.; Gregor, A.; Guillou, H.; König, J.; Wahli, W. Peroxisome Proliferator-Activated Receptors and Caloric Restriction—Common Pathways Affecting Metabolism, Health, and Longevity. Cells 2020, 9, 1708. [Google Scholar] [CrossRef]
- Zhao, Y.; Jia, M.; Chen, W.; Liu, Z. The Neuroprotective Effects of Intermittent Fasting on Brain Aging and Neurodegenerative Diseases via Regulating Mitochondrial Function. Free Radic. Biol. Med. 2022, 182, 206–218. [Google Scholar] [CrossRef]
- Mohr, A.E.; McEvoy, C.; Sears, D.D.; Arciero, P.J.; Sweazea, K.L. Impact of Intermittent Fasting Regimens on Circulating Markers of Oxidative Stress in Overweight and Obese Humans: A Systematic Review of Randomized Controlled Trials. Adv. Redox Res. 2021, 3, 100026. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Available online: www.training.cochrane.org/handbook (accessed on 21 July 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, C.L.; Muhlestein, J.B.; May, H.T.; Le, V.T.; Galenko, O.; Garrett, K.D.; Brunker, C.; Hopkins, R.O.; Carlquist, J.F.; Knowlton, K.U.; et al. Randomized Controlled Trial of Once-Per-Week Intermittent Fasting for Health Improvement: The WONDERFUL Trial. Eur. Heart J. Open 2021, 1, oeab026. [Google Scholar] [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Wiseman, E.; Pavlou, V.; Lin, S.; Oliveira, M.L.; Varady, K.A. Effects of 4- and 6-h Time-Restricted Feeding on Weight and Cardiometabolic Health: A Randomized Controlled Trial in Adults with Obesity. Cell Metab. 2020, 32, 366–378.e3. [Google Scholar] [CrossRef] [PubMed]
- Dengo, A.L.; Dennis, E.A.; Orr, J.S.; Marinik, E.L.; Ehrlich, E.; Davy, B.M.; Davy, K.P. Arterial Destiffening With Weight Loss in Overweight and Obese Middle-Aged and Older Adults. Hypertension 2010, 55, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Villareal, D.T.; Weiss, E.P.; Racette, S.B.; Steger-May, K.; Klein, S.; Holloszy, J.O.; Group W.U.S. of M.C. Calorie Restriction or Exercise: Effects on Coronary Heart Disease Risk Factors. A Randomized, Controlled Trial. Am. J. Physiol.-Endocrinol. Metab. 2007, 293, E197–E202. [Google Scholar] [CrossRef] [PubMed]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men with Overweight and Obesity. JAMA Intern. Med. 2020, 180, 1491–1499. [Google Scholar] [CrossRef]
- Martens, C.R.; Rossman, M.J.; Mazzo, M.R.; Jankowski, L.R.; Nagy, E.E.; Denman, B.A.; Richey, J.J.; Johnson, S.A.; Ziemba, B.P.; Wang, Y.; et al. Short-Term Time-Restricted Feeding Is Safe and Feasible in Non-Obese Healthy Midlife and Older Adults. Geroscience 2020, 42, 667–686. [Google Scholar] [CrossRef]
- Pierce, G.L.; Beske, S.D.; Lawson, B.R.; Southall, K.L.; Benay, F.J.; Donato, A.J.; Seals, D.R. Weight Loss Alone Improves Conduit and Resistance Artery Endothelial Function in Young and Older Overweight/Obese Adults. Hypertension 2008, 52, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Ravussin, E.; Redman, L.M.; Rochon, J.; Das, S.K.; Fontana, L.; Kraus, W.E.; Romashkan, S.; Williamson, D.A.; Meydani, S.N.; Villareal, D.T.; et al. A 2-Year Randomized Controlled Trial of Human Caloric Restriction: Feasibility and Effects on Predictors of Health Span and Longevity. J. Gerontol. Ser. A 2015, 70, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Redman, L.M.; Smith, S.R.; Burton, J.H.; Martin, C.K.; Il’yasova, D.; Ravussin, E. Metabolic Slowing and Reduced Oxidative Damage with Sustained Caloric Restriction Support the Rate of Living and Oxidative Damage Theories of Aging. Cell Metab. 2018, 27, 805–815.e4. [Google Scholar] [CrossRef] [PubMed]
- Stote, K.S.; Baer, D.J.; Spears, K.; Paul, D.R.; Harris, G.K.; Rumpler, W.V.; Strycula, P.; Najjar, S.S.; Ferrucci, L.; Ingram, D.K.; et al. A Controlled Trial of Reduced Meal Frequency without Caloric Restriction in Healthy, Normal-Weight, Middle-Aged Adults. Am. J. Clin. Nutr. 2007, 85, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Covington, J.D.; Ravussin, E.; Redman, L.M.; Team, P.C. Little Evidence of Systemic and Adipose Tissue Inflammation in Overweight Individuals. Front. Genet. 2012, 3, 58. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.C.; Bhutani, S.; Hoddy, K.K.; Gabel, K.; Freels, S.; Rigdon, J.; Rood, J.; et al. Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults: A Randomized Clinical Trial. JAMA Intern. Med. 2017, 177, 930–938. [Google Scholar] [CrossRef]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C.W.; Budniak, J.; Groshen, S.; Mack, W.J.; Guen, E.; Biase, S.D.; et al. Fasting-Mimicking Diet and Markers/Risk Factors for Aging, Diabetes, Cancer, and Cardiovascular Disease. Sci. Transl. Med. 2017, 9, eaai8700. [Google Scholar] [CrossRef]
- Weiss, E.P.; Racette, S.B.; Villareal, D.T.; Fontana, L.; Steger-May, K.; Schechtman, K.B.; Klein, S.; Holloszy, J.O. Improvements in Glucose Tolerance and Insulin Action Induced by Increasing Energy Expenditure or Decreasing Energy Intake: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2006, 84, 1033–1042. [Google Scholar] [CrossRef]
- Lin, S.; Cienfuegos, S.; Ezpeleta, M.; Gabel, K.; Pavlou, V.; Mulas, A.; Chakos, K.; McStay, M.; Wu, J.; Tussing-Humphreys, L.; et al. Time-Restricted Eating Without Calorie Counting for Weight Loss in a Racially Diverse Population: A Randomized Controlled Trial. Ann. Intern. Med. 2023, 176, 885–895. [Google Scholar] [CrossRef]
- Ezpeleta, M.; Gabel, K.; Cienfuegos, S.; Kalam, F.; Lin, S.; Pavlou, V.; Song, Z.; Haus, J.M.; Koppe, S.; Alexandria, S.J.; et al. Effect of Alternate Day Fasting Combined with Aerobic Exercise on Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Cell Metab. 2023, 35, 56–70.e3. [Google Scholar] [CrossRef]
- Prehn, K.; von Schwartzenberg, R.J.; Mai, K.; Zeitz, U.; Witte, A.V.; Hampel, D.; Szela, A.-M.; Fabian, S.; Grittner, U.; Spranger, J.; et al. Caloric Restriction in Older Adults—Differential Effects of Weight Loss and Reduced Weight on Brain Structure and Function. Cereb. Cortex 2017, 27, 1765–1778. [Google Scholar] [CrossRef] [PubMed]
- Schübel, R.; Nattenmüller, J.; Sookthai, D.; Nonnenmacher, T.; Graf, M.E.; Riedl, L.; Schlett, C.L.; von Stackelberg, O.; Johnson, T.; Nabers, D.; et al. Effects of Intermittent and Continuous Calorie Restriction on Body Weight and Metabolism over 50 Wk: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2018, 108, 933–945. [Google Scholar] [CrossRef] [PubMed]
- Teng, N.I.M.F.; Shahar, S.; Manaf, Z.A.; Das, S.K.; Taha, C.S.C.; Ngah, W.Z.W. Efficacy of Fasting Calorie Restriction on Quality of Life among Aging Men. Physiol. Behav. 2011, 104, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Teng, N.I.M.F.; Shahar, S.; Rajab, N.F.; Manaf, Z.A.; Johari, M.H.; Ngah, W.Z.W. Improvement of Metabolic Parameters in Healthy Older Adult Men Following a Fasting Calorie Restriction Intervention. Aging Male 2013, 16, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Johari, M.I.; Yusoff, K.; Haron, J.; Nadarajan, C.; Ibrahim, K.N.; Wong, M.S.; Hafidz, M.I.A.; Chua, B.E.; Hamid, N.; Arifin, W.N.; et al. Author Correction: A Randomised Controlled Trial on the Effectiveness and Adherence of Modified Alternate-Day Calorie Restriction in Improving Activity of Non-Alcoholic Fatty Liver Disease. Sci. Rep. 2020, 10, 10599. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Qin, Y.-L.; Shi, Z.-Y.; Chen, J.-H.; Zeng, M.-J.; Zhou, W.; Chen, R.-Q.; Chen, Z.-Y. Effects of Alternate-Day Fasting on Body Weight and Dyslipidaemia in Patients with Non-Alcoholic Fatty Liver Disease: A Randomised Controlled Trial. BMC Gastroenterol. 2019, 19, 219. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Sun, Y.; Ye, Y.; Hu, D.; Zhang, H.; He, Z.; Zhao, H.; Yang, H.; Mao, Y. Randomized Controlled Trial for Time-Restricted Eating in Healthy Volunteers without Obesity. Nat. Commun. 2022, 13, 1003. [Google Scholar] [CrossRef]
- Hajek, P.; Przulj, D.; Pesola, F.; McRobbie, H.; Peerbux, S.; Phillips-Waller, A.; Bisal, N.; Smith, K.M. A Randomised Controlled Trial of the 5:2 Diet. PLoS ONE 2021, 16, e0258853. [Google Scholar] [CrossRef]
- Coutinho, S.R.; Halset, E.H.; Gåsbakk, S.; Rehfeld, J.F.; Kulseng, B.; Truby, H.; Martins, C. Compensatory Mechanisms Activated with Intermittent Energy Restriction: A Randomized Control Trial. Clin. Nutr. 2018, 37, 815–823. [Google Scholar] [CrossRef]
- Holmer, M.; Lindqvist, C.; Petersson, S.; Moshtaghi-Svensson, J.; Tillander, V.; Brismar, T.B.; Hagström, H.; Stål, P. Treatment of NAFLD with Intermittent Calorie Restriction or Low-Carb High-Fat Diet—A Randomised Controlled Trial. JHEP Rep. 2021, 3, 100256. [Google Scholar] [CrossRef] [PubMed]
- Domaszewski, P.; Konieczny, M.; Pakosz, P.; Bączkowicz, D.; Sadowska-Krępa, E. Effect of a Six-Week Intermittent Fasting Intervention Program on the Composition of the Human Body in Women over 60 Years of Age. Int. J. Environ. Res. Public Health 2020, 17, 4138. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.-R.; Moon, J.-Y.; Kim, S.; An, K.-Y.; Oh, M.; Jeon, J.Y.; Jung, D.-H.; Choi, M.H.; Lee, J.-W. Effects of Alternate Day Fasting and Exercise on Cholesterol Metabolism in Overweight or Obese Adults: A Pilot Randomized Controlled Trial. Metabolism 2019, 93, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Stekovic, S.; Hofer, S.J.; Tripolt, N.; Aon, M.A.; Royer, P.; Pein, L.; Stadler, J.T.; Pendl, T.; Prietl, B.; Url, J.; et al. Alternate Day Fasting Improves Physiological and Molecular Markers of Aging in Healthy, Non-Obese Humans. Cell Metab. 2019, 30, 462–476.e6. [Google Scholar] [CrossRef] [PubMed]
- Christopoulos, P.F.; Msaouel, P.; Koutsilieris, M. The Role of the Insulin-like Growth Factor-1 System in Breast Cancer. Mol. Cancer 2015, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Weroha, S.J.; Haluska, P. The Insulin-Like Growth Factor System in Cancer. Endocrinol. Metab. Clin. N. Am. 2012, 41, 335–350. [Google Scholar] [CrossRef] [PubMed]
- Kalm, L.M.; Semba, R.D. They Starved So That Others Be Better Fed: Remembering Ancel Keys and the Minnesota Experiment. J. Nutr. 2005, 135, 1347–1352. [Google Scholar] [CrossRef]
| Caloric restriction: | Overall reduction in calories compared with normative energy intake, generally involving the reduction in energy intake >20% daily without malnutrition. |
| Intermittent fasting: | Voluntary abstinence of caloric consumption over periods of hours and/or days. |
| Prolonged nightly fasting: | Daily eating within a timeframe that is in alignment with the biological circadian rhythm (i.e., food/beverage caloric consumption during the active waking hours and abstinence during the nighttime). |
| Alternate day fasting: | Ingestion of ad libitum energy intake on alternating days coupled with fasting days (i.e., no food/beverage caloric consumption). |
| Time-restricted eating: | A specific, although flexible, window for daily timing restrictions on eating and fasting. |
| Periodic fasting: 5:2 | May involve fasting for several days (e.g., 2 to 7 days) repeated once per month or heavy restriction of a specific macronutrient (i.e., protein). Routine eating for 5 days followed by 2 (non-consecutive) days of caloric restriction (500–600 calories/day). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
James, D.L.; Hawley, N.A.; Mohr, A.E.; Hermer, J.; Ofori, E.; Yu, F.; Sears, D.D. Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials. Nutrients 2024, 16, 316. https://doi.org/10.3390/nu16020316
James DL, Hawley NA, Mohr AE, Hermer J, Ofori E, Yu F, Sears DD. Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials. Nutrients. 2024; 16(2):316. https://doi.org/10.3390/nu16020316
Chicago/Turabian StyleJames, Dara L., Nanako A. Hawley, Alex E. Mohr, Janice Hermer, Edward Ofori, Fang Yu, and Dorothy D. Sears. 2024. "Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials" Nutrients 16, no. 2: 316. https://doi.org/10.3390/nu16020316
APA StyleJames, D. L., Hawley, N. A., Mohr, A. E., Hermer, J., Ofori, E., Yu, F., & Sears, D. D. (2024). Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials. Nutrients, 16(2), 316. https://doi.org/10.3390/nu16020316