
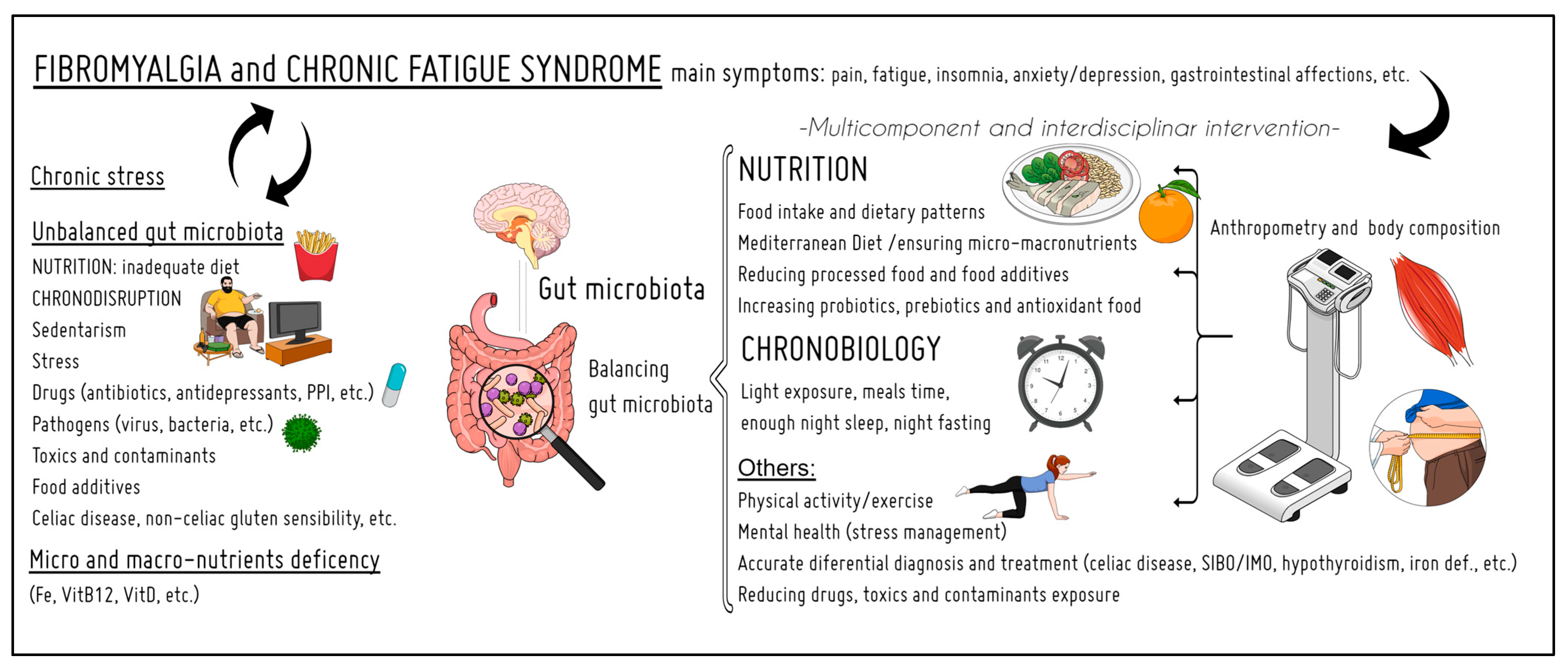
Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review

 , ,
, ,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Methods
3. Results
3.1. Nutrition
3.1.1. Dietary Patterns, Macronutrient Levels, and Nutritional Quality
3.1.2. Specific Diets
3.1.3. Micronutrient Levels in FM
3.1.4. Micronutrient Levels in CFS
3.2. Anthropometric Parameters and Body Composition
3.3. Gut Microbiota
3.3.1. Gut Microbiota in FM
3.3.2. Gut Microbiota in CFS
3.4. Supplementation
3.4.1. Supplementation in FM
3.4.2. Supplementation in CFS
3.5. Chronobiology
3.5.1. Chronobiology and FM
3.5.2. Chronobiology and CFS
4. Conclusions and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clauw, D.; Sarzi-Puttini, P.; Pellegrino, G.; Shoenfeld, Y. Is fibromyalgia an autoimmune disorder? Autoimmun. Rev. 2023, 103424. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, J.L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Angelats, R.C.; Gonçalves, A.Q.; Martín, C.A.; Sol, M.C.S.; Serra, G.G.; Casajuana, M.; Carrasco-Querol, N.; Fernández-Sáez, J.; Llorca, M.R.D.; Abellana, R.; et al. Effectiveness, cost-utility, and benefits of a multicomponent therapy to improve the quality of life of patients with fibromyalgia in primary care. Medicine 2019, 98, e17289. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Rollnik, J.D. Chronic Fatigue Syndrome: A Critical Review. Fortschr. Neurol. Psychiatr. 2017, 85, 79–85. [Google Scholar] [CrossRef]
- Pheby, D.F.H.; Araja, D.; Berkis, U.; Brenna, E.; Cullinan, J.; de Korwin, J.-D.; Gitto, L.; Hughes, D.A.; Hunter, R.M.; Trepel, D.; et al. The Development of a Consistent Europe-Wide Approach to Investigating the Economic Impact of Myalgic Encephalomyelitis (ME/CFS): A Report from the European Network on ME/CFS (EUROMENE). Healthcare 2020, 8, 88. [Google Scholar] [CrossRef]
- Komaroff, A.L. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Real Illness. Ann. Intern. Med. 2015, 162, 871–872. [Google Scholar] [CrossRef]
- Cheng, Y.; Xu, S.M.; Takenaka, K.; Lindner, G.; Curry-Hyde, A.; Janitz, M. A unique circular RNA expression pattern in the peripheral blood of myalgic encephalomyelitis/chronic fatigue syndrome patients. Gene 2023, 877, 147568. [Google Scholar] [CrossRef]
- Ollevier, A.; Vanneuville, I.; Carron, P.; Baetens, T.; Goderis, T.; Gabriel, L.; Van de Velde, D. A 12-week multicomponent therapy in fibromyalgia improves health but not in concomitant moderate depression, an exploratory pilot study. Disabil. Rehabil. 2019, 29, 1543361. [Google Scholar] [CrossRef]
- Serrat, M.; Almirall, M.; Musté, M.; Sanabria-Mazo, J.P.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Luciano, J.V.; Sanz, A. Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial. J. Clin. Med. 2020, 9, 3348. [Google Scholar] [CrossRef]
- Carrasco-Querol, N.; González Serra, G.; Bueno Hernández, N.; Gonçalves, A.Q.; Cazalla, M.P.; Pino, P.B.D.; Curto, P.M.; Angelats, R.C.; Anguera, I.F.; Sol, M.C.S.; et al. Effectiveness and health benefits of a nutritional, chronobiological and physical exercise primary care intervention in fibromyalgia and chronic fatigue syndrome: SYNCHRONIZE + mixed-methods study protocol. Medicine 2023, 102, E33637. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cabello, P.; Soriano-Maldonado, A.; Delgado-Fernandez, M.; Alvarez-Gallardo, I.C.; Segura-Jimenez, V.; Estevez-Lopez, F.; Camiletti-Moiron, D.; Aparicio, V.A. Association of Dietary Habits with Psychosocial Outcomes in Women with Fibromyalgia: The al-Andalus Project. J. Acad. Nutr. Diet. 2017, 117, 422–432.e1. [Google Scholar] [CrossRef] [PubMed]
- Cambras, T.; Castro-Marrero, J.; Zaragoza, M.C.; Díez-Noguera, A.; Alegre, J. Circadian rhythm abnormalities and autonomic dysfunction in patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis. PLoS ONE 2018, 13, e0198106. [Google Scholar] [CrossRef] [PubMed]
- Cambras, T.; Zerón-Rugerio, M.F.; Díez-Noguera, A.; Zaragozá, M.C.; Domingo, J.C.; Sanmartin-Sentañes, R.; Alegre-Martin, J.; Castro-Marrero, J. Skin Temperature Circadian Rhythms and Dysautonomia in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: The Role of Endothelin-1 in the Vascular Tone Dysregulation. Int. J. Mol. Sci. 2023, 24, 4835. [Google Scholar] [CrossRef] [PubMed]
- Borges-Cosic, M.; Aparicio, V.A.; Estevez-Lopez, F.; Soriano-Maldonado, A.; Acosta-Manzano, P.; Gavilan-Carrera, B.; Delgado-Fernandez, M.; Geenen, R.; Segura-Jimenez, V.; Estévez-López, F.; et al. Sedentary time, physical activity, and sleep quality in fibromyalgia: The al-Andalus project. Scand J. Med. Sci. Sport 2019, 29, 266–274. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Chirumbolo, S.; Aaseth, J. Fibromyalgia and nutrition: Therapeutic possibilities? Biomed. Pharmacother. 2018, 103, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Ozgocmen, S.; Ozyurt, H.; Sogut, S.; Akyol, O. Current concepts in the pathophysiology of fibromyalgia: The potential role of oxidative stress and nitric oxide. Rheumatol. Int. 2006, 26, 585–597. [Google Scholar] [CrossRef]
- Favero, G.; Bonomini, F.; Franco, C.; Rezzani, R. Mitochondrial Dysfunction in Skeletal Muscle of a Fibromyalgia Model: The Potential Benefits of Melatonin. Int. J. Mol. Sci. 2019, 20, 765. [Google Scholar] [CrossRef]
- Assavarittirong, C.; Samborski, W.; Grygiel-Górniak, B. Oxidative Stress in Fibromyalgia: From Pathology to Treatment. Oxid. Med. Cell. Longev. 2022, 2022, 1582432. [Google Scholar] [CrossRef]
- Caxaria, S.; Bharde, S.; Fuller, A.M.; Evans, R.; Thomas, B.; Celik, P.; Dell’Accio, F.; Yona, S.; Gilroy, D.; Voisin, M.-B.; et al. Neutrophils infiltrate sensory ganglia and mediate chronic widespread pain in fibromyalgia. Proc. Natl. Acad. Sci. USA 2023, 120, e2211631120. [Google Scholar] [CrossRef]
- Ryabkova, V.A.; Gavrilova, N.Y.; Poletaeva, A.A.; Pukhalenko, A.I.; Koshkina, I.A.; Churilov, L.P.; Shoenfeld, Y. Autoantibody Correlation Signatures in Fibromyalgia and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Association with Symptom Severity. Biomedicines 2023, 11, 257. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, V.; Bazzichi, L.; Batticciotto, A.; Pellegrino, G.; Di Franco, M.; Sirotti, S.; Atzeni, F.; Alciati, A.; Salaffi, F.; Puttini, P.S. Fibromyalgia: One year in review 2023. Clin. Exp. Rheumatol. 2023, 41, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Zhang, N.; Wei, M.; Pan, Q.; Cheng, C.; Lu, K.-E.; Mo, J.; Chen, Y. Methylation factors as biomarkers of fibromyalgia. Ann. Transl. Med. 2023, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Almirall, M.; Martínez-Mateu, S.H.; Alegre, C.; Collado, A.; Ojeda, B.; Arias, A.; Calandre, E.P.; Hidalgo, J.; Carrillo, M.D.; Huguet, R.; et al. Dietary habits in patients with fibromyalgia: A cross-sectional study. Clin. Exp. Rheumatol. 2021, 39, S170–S173. [Google Scholar] [CrossRef]
- Ortancil, O.; Sanli, A.; Eryuksel, R.; Basaran, A.; Ankarali, H. Association between serum ferritin level and fibromyalgia syndrome. Eur. J. Clin. Nutr. 2010, 64, 308–312. [Google Scholar] [CrossRef]
- Regland, B.; Forsmark, S.; Halaouate, L.; Matousek, M.; Peilot, B.; Zachrisson, O.; Gottfries, C.G. Response to vitamin B12 and folic acid in myalgic encephalomyelitis and fibromyalgia. PLoS ONE 2015, 10, e0124648. [Google Scholar] [CrossRef]
- Batista, E.D.; Andretta, A.; De Miranda, R.C.; Nehring, J.; Paiva, E.d.S.; Schieferdecker, M.E.M. Food intake assessment and quality of life in women with fibromyalgia. Rev. Bras. Reumatol. 2016, 56, 105–110. [Google Scholar] [CrossRef]
- Aguilar-Aguilar, E.; Marcos-Pasero, H.; Ikonomopoulou, M.P.; Loria-Kohen, V. Food Implications in Central Sensitization Syndromes. J. Clin. Med. 2020, 9, 4106. [Google Scholar] [CrossRef]
- Boomershine, C.S.; Koch, T.A.; Morris, D. A Blinded, Randomized, Placebo-Controlled Study to Investigate the Efficacy and Safety of Ferric Carboxymaltose in Iron-Deficient Patients with Fibromyalgia. Rheumatol. Ther. 2017, 5, 271–281. [Google Scholar] [CrossRef]
- Karras, S.; Rapti, E.; Matsoukas, S.; Kotsa, K. Vitamin D in Fibromyalgia: A Causative or Confounding Biological Interplay? Nutrients 2016, 8, 343. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Pen, J.J.; Chirumbolo, S.; Aaseth, J. Chronic fatigue syndrome (CFS): Suggestions for a nutritional treatment in the therapeutic approach. Biomed. Pharmacother. 2019, 109, 1000–1007. [Google Scholar] [CrossRef]
- Masri, S.; Sassone-Corsi, P. The emerging link between cancer, metabolism, and circadian rhythms. Nat. Med. 2018, 24, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Logan, R.W.; McClung, C.A. Rhythms of life: Circadian disruption and brain disorders across the lifespan. Nat. Rev. Neurosci. 2019, 20, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Bulbul, F.; Koca, I.; Savas, E.; Dokuyucu, R. The Comparison of the Biological Rhythms of Patients with Fibromyalgia Syndrome with Biological Rhythms of Healthy Controls. Med. Sci. Monit. 2020, 26, e920462-1–e920462-6. [Google Scholar] [CrossRef] [PubMed]
- Elma, Ö.; Yilmaz, S.T.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. J. Clin. Med. 2020, 9, 702. [Google Scholar] [CrossRef] [PubMed]
- López-Rodríguez, M.M.; Granero Molina, J.; Fernández Medina, I.M.; Fernández Sola, C.; Ruiz Muelle, A. Patterns of food avoidance and eating behavior in women with fibromyalgia. Endocrinol. Diabetes Nutr. 2017, 64, 480–490. [Google Scholar] [CrossRef] [PubMed]
- Elkfury, J.L.; Antunes, L.C.; Angoleri, L.D.M.; Sipmann, R.B.; De Souza, A.; Da Silva Torres, I.L.; Caumo, W. Dysfunctional eating behavior in fibromyalgia and its association with serum biomarkers of brain plasticity (BDNF and S100B): An exploratory study. Arch. Endocrinol. Metab. 2021, 65, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Di Lollo, A.C.; Guzzo, M.P.; Giacomelli, C.; Atzeni, F.; Bazzichi, L.; Di Franco, M. Fibromyalgia and nutrition: What news? Clin. Exp. Rheumatol. 2015, 33, S117–S125. [Google Scholar]
- Meléndez-Fernández, O.H.; Liu, J.A.; Nelson, R.J. Circadian Rhythms Disrupted by Light at Night and Mistimed Food Intake Alter Hormonal Rhythms and Metabolism. Int. J. Mol. Sci. 2023, 24, 3392. [Google Scholar] [CrossRef]
- Goedendorp, M.M.; Knoop, H.; Schippers, G.M.; Bleijenberg, G. The lifestyle of patients with chronic fatigue syndrome and the effect on fatigue and functional impairments. J. Hum. Nutr. Diet. 2009, 22, 226–231. [Google Scholar] [CrossRef]
- Jones, K.; Probst, Y. Role of dietary modification in alleviating chronic fatigue syndrome symptoms: A systematic review. Aust. N. Z. J. Public Health 2017, 41, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Marum, A.P.; Moreira, C.; Tomas-Carus, P.; Saraiva, F.; Guerreiro, C.S. A low fermentable oligo-di-mono-saccharides and polyols (FODMAP) diet is a balanced therapy for fibromyalgia with nutritional and symptomatic benefits. Nutr. Hosp. 2017, 34, 667–674. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Silva, A.R.; Bernardo, A.; Costa, J.; Cardoso, A.; Santos, P.; de Mesquita, M.F.; Vaz Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. Dietary interventions in fibromyalgia: A systematic review. Ann. Med. 2019, 51, 2–14. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Arguelles, J.M.; Caceres, O.; Blanco, M.; Maestu, C.; Martin, F. Improvement of digestive symptoms in fibromyalgia patients following a diet modification according to histamine release test—An observational study. Reumatologia 2022, 60, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.R.; Bernardo, A.; de Mesquita, M.F.; Vaz-Patto, J.; Moreira, P.; Silva, M.L.; Padrão, P. An anti-inflammatory and low fermentable oligo, di, and monosaccharides and polyols diet improved patient reported outcomes in fibromyalgia: A randomized controlled trial. Front. Nutr. 2022, 9, 856216. [Google Scholar] [CrossRef] [PubMed]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary interventions in the management of fibromyalgia: A systematic review and best-evidence synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Giangrandi, I.; Dinu, M.; Sofi, F.; Colombini, B. Nutritional interventions in the management of fibromyalgia syndrome. Nutrients 2020, 12, 2525. [Google Scholar] [CrossRef]
- Almirall, M.; Casellas, F.; Dot, J.; de Torres, I.; Segurola, H.; Marsal, S. Prevalence of non-coeliac gluten sensitivity and assessment of the response to gluten-free diet in a cohort of patients with fibromyalgia. Rheumatology 2023, 62, 1069–1077. [Google Scholar] [CrossRef]
- Martín, F.; Blanco-Suárez, M.; Zambrano, P.; Cáceres, O.; Almirall, M.; Alegre-Martín, J.; Lobo, B.; González-Castro, A.M.; Santos, J.; Domingo, J.C.; et al. Increased gut permeability and bacterial translocation are associated with fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome: Implications for disease-related biomarker discovery. Front. Immunol. 2023, 14, 1253121. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Leyva-Vela, B.; Martínez-García, A.; Nadal-Nicolás, Y. Effects of lacto-vegetarian diet and stabilization core exercises on body composition and pain in women with fibromyalgia: Randomized controlled trial. Nutr. Hosp. 2018, 35, 392–399. [Google Scholar] [CrossRef]
- Martínez-Rodríguez, A.; Rubio-Arias, J.; Ramos-Campo, D.J.; Reche-García, C.; Leyva-Vela, B.; Nadal-Nicolás, Y. Psychological and sleep effects of tryptophan and magnesium-enriched mediterranean diet in women with fibromyalgia. Int. J. Environ. Res. Public Health 2020, 17, 2227. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, A.; Harte, S.; Clauw, D.J.; Williams, D.A.; Mcafee, J.; Miller, N.; Brown, M.; Med, C.N.; Rothberg, A.; Schrepf, A. Early Relationships of a Low-Energy Diet With Symptoms of Fibromyalgia. ACR Open Rheumatol. 2022, 4, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Kadayifci, F.Z.; Bradley, M.J.; Onat, A.M.; Shi, H.N.; Zheng, S. Review of nutritional approaches to fibromyalgia. Nutr. Rev. 2022, 80, 2260–2274. [Google Scholar] [CrossRef] [PubMed]
- Kucuk, A.; Baykara, R.A.; Tuzcu, A.; Omma, A.; Cure, M.C.; Cure, E.; Acet, G.K.; Dogan, E. Could ferritin, vitamin B12, and vitamin D play a role in the etiopathogenesis of fibromyalgia syndrome? Rom. J. Intern. Med. 2021, 59, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.C.; Chen, H.J.; Leong, K.H.; Chang, K.L.; Wang, Y.T.T.; Wu, L.C.; Tung, P.Y.; Kuo, C.F.; Lin, C.C.; Tsai, S.Y. The risk of fibromyalgia in patients with iron deficiency anemia: A nationwide population-based cohort study. Sci. Rep. 2021, 11, 10496. [Google Scholar] [CrossRef] [PubMed]
- Pamuk, G.E.; Pamuk, Ö.N.; Set, T.; Harmandar, O.; Yeşil, N. An increased prevalence of fibromyalgia in iron deficiency anemia and thalassemia minor and associated factors. Clin. Rheumatol. 2008, 27, 1103–1108. [Google Scholar] [CrossRef]
- Tan, A.C.; Jaaniste, T.; Champion, D. Chronic Widespread Pain and Fibromyalgia Syndrome: Life-Course Risk Markers in Young People. Pain Res. Manag. 2019, 2019, 6584753. [Google Scholar] [CrossRef]
- Munipalli, B.; Strothers, S.; Rivera, F.; Malavet, P.; Mitri, G.; Abu Dabrh, A.M.; Dawson, N.L. Association of Vitamin B12, Vitamin D, and Thyroid-Stimulating Hormone with Fatigue and Neurologic Symptoms in Patients With Fibromyalgia. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 6, 381–387. [Google Scholar] [CrossRef]
- Ellis, S.D.; Kelly, S.T.; Shurlock, J.H.; Hepburn, A.L.N. The role of vitamin D testing and replacement in fibromyalgia: A systematic literature review. BMC Rheumatol. 2018, 2, 28. [Google Scholar] [CrossRef]
- Plotnikoff, G.A.; Quigley, J.M. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin. Proc. 2003, 78, 1463–1470. [Google Scholar] [CrossRef]
- Rezende, R.M.; Natali, A.J.; Franceschini, S.D.C.C. The hidden hunger and fibromyalgia: A systematic review. Rev. Chil. Nutr. 2019, 46, 160–167. [Google Scholar] [CrossRef]
- Ali, O.M.E. Prevalence of Vitamin D Deficiency and Its Relationship with Clinical Outcomes in Patients with Fibromyalgia: A Systematic Review of the Literature. SN Compr. Clin. Med. 2022, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Zabihiyeganeh, M.; Amini Kadijani, A.; Akbari, A.; Yahyazadeh, H.; Mirzaei, A. Association of serum vitamin D status with serum pro-inflammatory cytokine levels and clinical severity of fibromyalgia patients. Clin. Nutr. ESPEN 2023, 55, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Çıracıoğlu, A.M.; Armağan, O.; Uslu, S.; Berkan, F.; Özgen, M.; Dal Erdoğan, S.; Çolak, E. Vitamin K levels in Fibromyalgia Syndrome Patients and Their Associations with Pain, Disease Activity, Quality of Life and Inflammatory Cytokines. Pain Manag. Nurs. 2023, 24, 60–67. [Google Scholar] [CrossRef]
- Malczewska-Lenczowska, J.; Sitkowski, D.; Surała, O.; Orysiak, J.; Szczepańska, B.; Witek, K. The association between iron and vitamin D status in female elite athletes. Nutrients 2018, 10, 167. [Google Scholar] [CrossRef]
- Tel Adıgüzel, K.; Köroğlu, Ö.; Yaşar, E.; Kenan Tan, A.; Samur, G. The relationship between dietary total antioxidant capacity, clinical parameters, and oxidative stress in fibromyalgia syndrome: A novel point of view. Turk. J. Phys. Med. Rehabil. 2022, 68, 262–270. [Google Scholar] [CrossRef]
- Correa-Rodríguez, M.; Rueda-Medina, B.; Casas-Barragán, A.; Tapia-Haro, R.M.; Molina, F.; Aguilar-Ferrándiz, M.E. Dietary Intake Assessment, Severity of Symptoms, and Pain in Women with Fibromyalgia. Clin. Nurs. Res. 2021, 30, 1164–1173. [Google Scholar] [CrossRef]
- Anderson, G.; Maes, M. Mitochondria and immunity in chronic fatigue syndrome. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 103, 109976. [Google Scholar] [CrossRef]
- Bazzichi, L.; Palego, L.; Giannaccini, G.; Rossi, A.; De Feo, F.; Giacomelli, C.; Betti, L.; Giusti, L.; Mascia, G.; Bombardieri, S.; et al. Altered amino acid homeostasis in subjects affected by fibromyalgia. Clin. Biochem. 2009, 42, 1064–1070. [Google Scholar] [CrossRef]
- Schwarz, M.J.; Offenbaecher, M.; Neumeister, A.; Ackenheil, M. Experimental evaluation of an altered tryptophan metabolism in fibromyalgia. Adv. Exp. Med. Biol. 2003, 527, 265–275. [Google Scholar] [CrossRef]
- Shukla, V.; Das, S.K.; Mahdi, A.A.; Agarwal, S.; Alok, R.; Ansari, J.A.; Khandpur, S. Metal-induced oxidative stress level in patients with fibromyalgia syndrome and its contribution to the severity of the disease: A correlational study. J. Back Musculoskelet. Rehabil. 2021, 34, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Andretta, A.; Dias Batista, E.; Madalozzo Schieferdecker, M.E.; Rasmussen Petterle, R.; Boguszewski, C.L.; Dos Santos Paiva, E. Relation between magnesium and calcium and parameters of pain, quality of life and depression in women with fibromyalgia. Adv. Rheumatol. 2019, 59, 55. [Google Scholar] [CrossRef] [PubMed]
- Razzaque, M.S. Magnesium: Are We Consuming Enough? Nutrients 2018, 10, 1863. [Google Scholar] [CrossRef] [PubMed]
- Boulis, M.; Boulis, M.; Clauw, D. Magnesium and Fibromyalgia: A Literature Review. J. Prim. Care Community Health 2021, 12, 21501327211038433. [Google Scholar] [CrossRef] [PubMed]
- Berkovitz, S.; Ambler, G.; Jenkins, M.; Thurgood, S. Serum 25-hydroxy vitamin D levels in chronic fatigue syndrome: A retrospective survey. Int. J. Vitam. Nutr. Res. 2009, 79, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Mihaylova, I.; Leunis, J.-C. In Chronic Fatigue Syndrome, the Decreased Levels of Omega-3 Poly-Unsaturated Fatty Acids Are Related to Lowered Serum Zinc and Defects in T Cell Activation. Available online: https://pubmed.ncbi.nlm.nih.gov/16380690/ (accessed on 21 November 2023).
- De Lorenzo, F.; Hargreaves, J.; Kakkar, V.V. Phosphate diabetes in patients with chronic fatigue syndrome. Postgrad. Med. J. 1998, 74, 229–232. [Google Scholar] [CrossRef][Green Version]
- Núñez-Nevárez, K.; López-Betancourt, A.; Cisneros-Pérez, V.; Rodríguez-Márquez, C.N.; Galvan, G.Z.; Luis, A.C.; Escorza, M.A.Q. Relationship Between Weight and Severity of Fibromyalgia. Mo. Med. 2023, 120, 83. [Google Scholar]
- Álvarez-Nemegyei, J.; Pacheco-Pantoja, E.L.; Olán-Centeno, L.J.; Angulo-Ramírez, A.; Rodríguez-Magaña, F.E.; Aranda-Muiña, J.F. Association between fibromyalgia syndrome clinical severity and body composition. A principal component analysis. Reumatol. Clin. 2022, 18, 538–545. [Google Scholar] [CrossRef]
- Da Silva, S.G.L.; Sarni, R.O.S.; De Souza, F.I.S.; Molina, J.; Terreri, M.T.R.A.; Hilário, M.O.E.; Len, C.A. Assessment of nutritional status and eating disorders in female adolescents with fibromyalgia. J. Adolesc. Health 2012, 51, 524–527. [Google Scholar] [CrossRef]
- Kapuczinski, A.; Soyfoo, M.S.; De Breucker, S.; Margaux, J. Assessment of sarcopenia in patients with fibromyalgia. Rheumatol. Int. 2022, 42, 279–284. [Google Scholar] [CrossRef]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- Ghafouri, B.; Edman, E.; Löf, M.; Lund, E.; Leinhard, O.D.; Lundberg, P.; Forsgren, M.F.; Gerdle, B.; Dong, H.J. Fibromyalgia in women: Association of inflammatory plasma proteins, muscle blood flow, and metabolism with body mass index and pain characteristics. Pain Rep. 2022, 7, E1042. [Google Scholar] [CrossRef]
- Serpas, D.G.; Zettel-Watson, L.; Cherry, B.J. Fibromyalgia status and depressive symptoms are linked to body mass index and physical performance in mid to late life. Psychol. Health Med. 2023, 28, 1230–1243. [Google Scholar] [CrossRef] [PubMed]
- Minerbi, A.; Gonzalez, E.; Brereton, N.J.B.; Anjarkouchian, A.; Dewar, K.; Fitzcharles, M.A.; Chevalier, S.; Shir, Y. Altered microbiome composition in individuals with fibromyalgia. Pain 2019, 160, 2589–2602. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Mazzola, M.; Bosco, V.; Tomasello, G.; Damiani, P.; Sinagra, E.; Carini, F. Intestinal dysbiosis and hormonal neuroendocrine secretion in the fibromyalgic patient. Biomed. Pap. 2018, 164, 258–262. [Google Scholar] [CrossRef]
- Hazra, S.; Venkataraman, S.; Handa, G.; Yadav, S.L.; Wadhwa, S.; Singh, U.; Kochhar, K.P.; Deepak, K.K.; Sarkar, K. A Cross-Sectional Study on Central Sensitization and Autonomic Changes in Fibromyalgia. Front. Neurosci. 2020, 14, 788. [Google Scholar] [CrossRef]
- Malkova, A.M.; Shoenfeld, Y. Autoimmune autonomic nervous system imbalance and conditions: Chronic fatigue syndrome, fibromyalgia, silicone breast implants, COVID and post-COVID syndrome, sick building syndrome, post-orthostatic tachycardia syndrome, autoimmune diseases and autoimmune/inflammatory syndrome induced by adjuvants. Autoimmun. Rev. 2023, 22, 103230. [Google Scholar] [CrossRef]
- Pimentel, M.; Wallace, D.; Hallegua, D.; Chow, E.; Kong, Y.; Park, S.; Lin, H.C. A link between irritable bowel syndrome and fibromyalgia may be related to findings on lactulose breath testing. Ann. Rheum. Dis. 2004, 63, 450–452. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Shukla, R.; Ghoshal, U. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome: A Bridge between Functional Organic Dichotomy. Gut Liver 2017, 11, 196–208. [Google Scholar] [CrossRef]
- Takakura, W.; Pimentel, M. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome—An Update. Front. Psychiatry 2020, 11, 664. [Google Scholar] [CrossRef]
- Erdrich, S.; Hawrelak, J.A.; Myers, S.P.; Harnett, J.E. A systematic review of the association between fibromyalgia and functional gastrointestinal disorders. Therap. Adv. Gastroenterol. 2020, 13, 1756284820977402. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.; Eslick, E.M.; Eslick, G.D. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur. J. Nutr. 2016, 55, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Wielgosz-Grochowska, J.P.; Domanski, N.; Drywień, M.E. Efficacy of an Irritable Bowel Syndrome Diet in the Treatment of Small Intestinal Bacterial Overgrowth: A Narrative Review. Nutrients 2022, 14, 3382. [Google Scholar] [CrossRef] [PubMed]
- Efremova, I.; Maslennikov, R.; Poluektova, E.; Vasilieva, E.; Zharikov, Y.; Suslov, A.; Letyagina, Y.; Kozlov, E.; Levshina, A.; Ivashkin, V. Epidemiology of small intestinal bacterial overgrowth. World J. Gastroenterol. 2023, 29, 3400–3421. [Google Scholar] [CrossRef] [PubMed]
- Minerbi, A.; Gonzalez, E.; Brereton, N.; Fitzcharles, M.A.; Chevalier, S.; Shir, Y. Altered serum bile acid profile in fibromyalgia is associated with specific gut microbiome changes and symptom severity. Pain 2023, 164, E66–E76. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, G.T.; Kang, J. Microbial Composition and Stool Short Chain Fatty Acid Levels in Fibromyalgia. Int. J. Environ. Res. Public Health 2023, 20, 3183. [Google Scholar] [CrossRef]
- Weber, T.; Tatzl, E.; Kashofer, K.; Holter, M.; Trajanoski, S.; Berghold, A.; Heinemann, A.; Holzer, P.; Herbert, M.K. Fibromyalgia-associated hyperalgesia is related to psychopathological alterations but not to gut microbiome changes. PLoS ONE 2022, 17, e0274026. [Google Scholar] [CrossRef]
- Ford, A.C.; Mahadeva, S.; Carbone, M.F.; Lacy, B.E.; Talley, N.J. Functional dyspepsia. Lancet 2020, 396, 1689–1702. [Google Scholar] [CrossRef]
- Rueda-Ruzafa, L.; Cruz, F.; Cardona, D.; Hone, A.J.; Molina-Torres, G.; Sánchez-Labraca, N.; Roman, P. Opioid system influences gut-brain axis: Dysbiosis and related alterations. Pharmacol. Res. 2020, 159, 104928. [Google Scholar] [CrossRef]
- DE Bastiani, R.; Lopetuso, L.R.; DE Bastiani, M.; Bacchin, P.; Benedetto, E.; Boscariolo, L.; Caneve, R.; Chesani, F.; Chiumeo, F.; Civic, Z.; et al. Assessment of small intestinal bacterial overgrowth and methane production in patients on chronic proton-pump inhibitor treatment: Prevalence and role of rifaximin in its management in primary care. Minerva Gastroenterol. 2023, 69. [Google Scholar] [CrossRef]
- Ait Chait, Y.; Mottawea, W.; Tompkins, T.A.; Hammami, R. Unravelling the antimicrobial action of antidepressants on gut commensal microbes. Sci. Rep. 2020, 10, 17878. [Google Scholar] [CrossRef] [PubMed]
- Winslow, B.T.; Vandal, C.; Dang, L. Fibromyalgia: Diagnosis and Management. Am. Fam. Physician 2023, 107, 137–144. [Google Scholar] [PubMed]
- Guo, C.; Che, X.; Briese, T.; Ranjan, A.; Allicock, O.; Yates, R.A.; Cheng, A.; March, D.; Hornig, M.; Komaroff, A.L.; et al. Deficient butyrate-producing capacity in the gut microbiome is associated with bacterial network disturbances and fatigue symptoms in ME/CFS. Cell Host Microbe 2023, 31, 288–304.e8. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M. Intestinal bacteria associated with irritable bowel syndrome and chronic fatigue. Neurogastroenterol. Motil. 2023, 35, e14621. [Google Scholar] [CrossRef] [PubMed]
- Sampson, T.R. Revealing gut microbiome associations with CFS. Cell Host Microbe 2023, 31, 171–172. [Google Scholar] [CrossRef] [PubMed]
- Elmassry, M.M.; Zayed, A.; Farag, M.A. Gut homeostasis and microbiota under attack: Impact of the different types of food contaminants on gut health. Crit. Rev. Food Sci. Nutr. 2022, 62, 738–763. [Google Scholar] [CrossRef]
- Balaguer-Trias, J.; Deepika, D.; Schuhmacher, M.; Kumar, V. Impact of Contaminants on Microbiota: Linking the Gut-Brain Axis with Neurotoxicity. Int. J. Environ. Res. Public Health 2022, 19, 1368. [Google Scholar] [CrossRef]
- Scaturro, D.; Vitagliani, F.; Tomasello, S.; Filippetti, M.; Picelli, A.; Smania, N.; Mauro, G.L. Can the Combination of Rehabilitation and Vitamin D Supplementation Improve Fibromyalgia Symptoms at All Ages? J. Funct. Morphol. Kinesiol. 2022, 7, 51. [Google Scholar] [CrossRef]
- Lozano-Plata, L.I.; Vega-Morales, D.; Esquivel-Valerio, J.A.; Garza-Elizondo, M.A.; Galarza-Delgado, D.A.; Silva-Luna, K.; Serna-Peña, G.; Sifuentes-Ramírez, J.; Garza-Guerra, A.d.J.; de Rivera, R.D.-N. Efficacy and safety of weekly vitamin D3 in patients with fibromyalgia: 12-week, double-blind, randomized, controlled placebo trial. Clin. Rheumatol. 2021, 40, 3257–3264. [Google Scholar] [CrossRef]
- Lombardo, M.; Feraco, A.; Ottaviani, M.; Rizzo, G.; Camajani, E.; Caprio, M.; Armani, A. The Efficacy of Vitamin D Supplementation in the Treatment of Fibromyalgia Syndrome and Chronic Musculoskeletal Pain. Nutrients 2022, 14, 3010. [Google Scholar] [CrossRef]
- Yang, C.C.; Tsai, S.T.; Ting, B.; Cheng, Y.C.; Wang, C.K.; Chang, J.P.C.; Su, K.P. Psychological Outcomes and Quality of Life of Fibromyalgia Patients with Vitamin D Supplementation-A Meta-Analysis. J. Clin. Med. 2023, 12, 2750. [Google Scholar] [CrossRef] [PubMed]
- Erkilic, B.; Dalgic, G.S. The preventive role of vitamin D in the prevention and management of Fibromyalgia syndrome. Nutr. Health 2023, 29, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Ghavidel-Parsa, B.; Naeimi, A.; Gharibpoor, F.; Sattari, N.; Jafari, A.; Masooleh, I.S.; Montazeri, A. Effect of vitamin B6 on pain, disease severity, and psychological profile of fibromyalgia patients; a randomized, double-blinded clinical trial. BMC Musculoskelet. Disord. 2022, 23, 664. [Google Scholar] [CrossRef] [PubMed]
- Sall Hansson, K.; Lindqvist, G.; Stening, K.; Fohlman, J.; Wojanowski, A.; Ponten, M.; Jensen, K.; Gerdle, B.; Elmqvist, C. Efficacy of mecobalamin (vitamin B12) in the treatment of long-term pain in women diagnosed with fibromyalgia: Protocol for a randomised, placebo-controlled trial. BMJ Open 2023, 13, e066987. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.J.; Na, H.S.; Do, S.H. Magnesium and pain. Nutrients 2020, 12, 2184. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Andretta, A.; Schieferdecker, M.E.M.; Petterle, R.R.; Dos Santos Paiva, E.; Boguszewski, C.L. Relations between serum magnesium and calcium levels and body composition and metabolic parameters in women with fibromyalgia. Adv. Rheumatol. 2020, 60, 18. [Google Scholar] [CrossRef]
- Macian, N.; Dualé, C.; Voute, M.; Leray, V.; Courrent, M.; Bodé, P.; Giron, F.; Sonneville, S.; Bernard, L.; Joanny, F.; et al. Short-Term Magnesium Therapy Alleviates Moderate Stress in Patients with Fibromyalgia: A Randomized Double-Blind Clinical Trial. Nutrients 2022, 14, 2088. [Google Scholar] [CrossRef]
- Haddad, H.W.; Mallepalli, N.R.; Scheinuk, J.E.; Bhargava, P.; Cornett, E.M.; Urits, I.; Kaye, A.D. The Role of Nutrient Supplementation in the Management of Chronic Pain in Fibromyalgia: A Narrative Review. Pain Ther. 2021, 10, 827–848. [Google Scholar] [CrossRef]
- Çİn, N.N.A.; Açik, M.; Tertemİz, O.F.; Aktan, Ç.; Akçali, D.T.; Çakiroğlu, F.P.; Özçelİk, A.Ö. Effect of prebiotic and probiotic supplementation on reduced pain in patients with fibromyalgia syndrome: A double-blind, placebo-controlled randomized clinical trial. Psychol. Health Med. 2023, 2023, 2216464. [Google Scholar] [CrossRef]
- Hinchado, M.D.; Quero-Calero, C.D.; Otero, E.; Gálvez, I.; Ortega, E. Synbiotic Supplementation Improves Quality of Life and Inmunoneuroendocrine Response in Patients with Fibromyalgia: Influence of Codiagnosis with Chronic Fatigue Syndrome. Nutrients 2023, 15, 1591. [Google Scholar] [CrossRef] [PubMed]
- Roman, P.; Estevez, A.F.; Miras, A.; Sanchez-Labraca, N.; Canadas, F.; Vivas, A.B.; Cardona, D.; Estévez, A.F.; Miras, A.; Sánchez-Labraca, N.; et al. A Pilot Randomized Controlled Trial to Explore Cognitive and Emotional Effects of Probiotics in Fibromyalgia. Sci. Rep. 2018, 8, 10965. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Maraver, J.; Cordero, M.D.; Oropesa-Avila, M.; Fernandez Vega, A.; De La Mata, M.; Delgado Pavon, A.; Alcocer-Gomez, E.; Perez Calero, C.; Villanueva Paz, M.; Alanis, M.; et al. Clinical applications of coenzyme Q10. Front. Biosci. 2014, 19, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Arranz, L.I.; Canela, M.Á.; Rafecas, M. Fibromyalgia and nutrition, what do we know? Rheumatol. Int. 2011, 30, 1417–1427. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cordero, M.D.; Alcocer-Gómez, E.; Culic, O.; Carrión, A.M.; De Miguel, M.; Díaz-Parrado, E.; Pérez-Villegas, E.M.; Bullón, P.; Battino, M.; Sánchez-Alcazar, J.A. NLRP3 inflammasome is activated in fibromyalgia: The effect of coenzyme Q10. Antioxid. Redox Signal. 2014, 20, 1169–1180. [Google Scholar] [CrossRef]
- Sawaddiruk, P.; Apaijai, N.; Paiboonworachat, S.; Kaewchur, T.; Kasitanon, N.; Jaiwongkam, T.; Kerdphoo, S.; Chattipakorn, N.; Chattipakorn, S.C. Coenzyme Q10 supplementation alleviates pain in pregabalin-treated fibromyalgia patients via reducing brain activity and mitochondrial dysfunction. Free Radic. Res. 2019, 53, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, I.P.; Mantle, D. Targeted Treatment of Age-Related Fibromyalgia with Supplemental Coenzyme Q10. Adv. Exp. Med. Biol. 2021, 1286, 77–85. [Google Scholar] [CrossRef]
- de Carvalho, J.F.; Skare, T.L. Melatonin supplementation improves rheumatological disease activity: A systematic review. Clin. Nutr. ESPEN 2023, 55, 414–419. [Google Scholar] [CrossRef]
- Pekarovics, S.; Beres, A.; Kelly, C.; Billes, S.K.; Heaton, A.L. Stress-associated weight gain, fibromyalgia symptoms, cardiometabolic markers, and human growth hormone suppression respond to an amino acid supplement blend: Results of a prospective, cohort study. Front. Endocrinol. 2023, 14, 1053692. [Google Scholar] [CrossRef]
- Salaffi, F.; Farah, S.; Sarzi-Puttini, P.; Di Carlo, M. Palmitoylethanolamide and acetyl-L-carnitine act synergistically with duloxetine and pregabalin in fibromyalgia: Results of a randomised controlled study. Clin. Exp. Rheumatol. 2023, 41, 1323–1331. [Google Scholar] [CrossRef]
- Mehrabani, S.; Askari, G.; Miraghajani, M.; Tavakoly, R.; Arab, A. Effect of coenzyme Q10 supplementation on fatigue: A systematic review of interventional studies. Complement. Ther. Med. 2019, 43, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Castro-Marrero, J.; Cordero, M.D.; Segundo, M.J.; Sáez-Francàs, N.; Calvo, N.; Román-Malo, L.; Aliste, L.; Fernández De Sevilla, T.; Alegre, J. Does oral coenzyme Q10 plus NADH supplementation improve fatigue and biochemical parameters in chronic fatigue syndrome? Antioxid. Redox Signal. 2015, 22, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Barnish, M.; Sheikh, M.; Scholey, A. Nutrient Therapy for the Improvement of Fatigue Symptoms. Nutrients 2023, 15, 2154. [Google Scholar] [CrossRef] [PubMed]
- Bentler, S.E.; Hartz, A.J.; Kuhn, E.M. Prospective observational study of treatments for unexplained chronic fatigue. J. Clin. Psychiatry 2005, 66, 625–632. [Google Scholar] [CrossRef]
- Maric, D.; Brkic, S.; Mikic, A.N.; Tomic, S.; Cebovic, T.; Turkulov, V. Multivitamin mineral supplementation in patients with chronic fatigue syndrome. Med. Sci. Monit. 2014, 20, 47–53. [Google Scholar] [CrossRef]
- Sullivan, Å.; Nord, C.E.; Evengård, B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr. J. 2009, 8, 4–6. [Google Scholar] [CrossRef]
- Groeger, D.; O’Mahony, L.; Murphy, E.F.; Bourke, J.F.; Dinan, T.G.; Kiely, B.; Shanahan, F.; Quigley, E.M.M. Bifidobacterium infantis 35624 modulates host inflammatory processes beyond the gut. Gut Microbes 2013, 4, 325–339. [Google Scholar] [CrossRef]
- Venturini, L.; Bacchi, S.; Capelli, E.; Lorusso, L.; Ricevuti, G.; Cusa, C. Modification of Immunological Parameters, Oxidative Stress Markers, Mood Symptoms, and Well-Being Status in CFS Patients after Probiotic Intake: Observations from a Pilot Study. Oxid. Med. Cell. Longev. 2019, 2019, 1684198. [Google Scholar] [CrossRef]
- König, R.S.; Albrich, W.C.; Kahlert, C.R.; Bahr, L.S.; Löber, U.; Vernazza, P.; Scheibenbogen, C.; Forslund, S.K. The Gut Microbiome in Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Front. Immunol. 2022, 12, 628741. [Google Scholar] [CrossRef]
- Corbitt, M.; Campagnolo, N.; Staines, D.; Marshall-Gradisnik, S. A Systematic Review of Probiotic Interventions for Gastrointestinal Symptoms and Irritable Bowel Syndrome in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME). Probiotics Antimicrob. Proteins 2018, 10, 466–477. [Google Scholar] [CrossRef]
- Wei, X.; Xin, J.; Chen, W.; Wang, J.; Lv, Y.; Wei, Y.; Li, Z.; Ding, Q.; Shen, Y.; Xu, X.; et al. Astragalus polysaccharide ameliorated complex factor-induced chronic fatigue syndrome by modulating the gut microbiota and metabolites in mice. Biomed. Pharmacother. 2023, 163, 114862. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Long, M.; Wang, Y.; Li, Y.; Li, Z.; Jiao, J. Fibromyalgia in China: Sleep quality is related to symptoms, quality of life and especially mental health. Clin. Exp. Rheumatol. 2023, 41, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, A.A.; Fatima, G.; Das, S.K.; Verma, N.S. Abnormality of circadian rhythm of serum melatonin and other biochemical parameters in fibromyalgia syndrome. Indian J. Biochem. Biophys. 2011, 48, 82–87. [Google Scholar] [PubMed]
- Matre, D.; Knardahl, S.; Nilsen, K.B. Night-shift work is associated with increased pain perception. Scand. J. Work. Environ. Health 2017, 43, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Wei, T.; Li, C.; Heng, Y.; Gao, X.; Zhang, G.; Wang, H.; Zhao, X.; Meng, Z.; Zhang, Y.; Hou, H. Association between night-shift work and level of melatonin: Systematic review and meta-analysis. Sleep Med. 2020, 75, 502–509. [Google Scholar] [CrossRef]
- Catalá, P.; Gutiérrez, L.; Écija, C.; Peñacoba, C. Pathological Cycle between Pain, Insomnia, and Anxiety in Women with Fibromyalgia and its Association with Disease Impact. Biomedicines 2023, 11, 148. [Google Scholar] [CrossRef]
- Sarwar, A.; Agu, E.O.; Polcari, J.; Ciroli, J.; Nephew, B.; King, J. PainRhythms: Machine learning prediction of chronic pain from circadian dysregulation using actigraph data—A preliminary study. Smart Health 2022, 26, 100344. [Google Scholar] [CrossRef]
- Knezevic, N.N.; Nader, A.; Pirvulescu, I.; Pynadath, A.; Rahavard, B.B.; Candido, K.D. Circadian pain patterns in human pain conditions—A systematic review. Pain Pract. 2023, 23, 94–109. [Google Scholar] [CrossRef]
- Burgess, H.J.; Bahl, S.; Wilensky, K.; Spence, E.; Jouppi, R.J.; Rizvydeen, M.; Goldstein, C.; Kim, H.M.; Williams, D.A.; Burns, J.W. A 4-week morning light treatment with stable sleep timing for individuals with fibromyalgia: A randomized controlled trial. Pain Med. 2023, 24, 787–795. [Google Scholar] [CrossRef]
- Charlot, A.; Hutt, F.; Sabatier, E.; Zoll, J. Beneficial Effects of Early Time-Restricted Feeding on Metabolic Diseases: Importance of Aligning Food Habits with the Circadian Clock. Nutrients 2021, 13, 1405. [Google Scholar] [CrossRef]
- Paoli, A.; Tinsley, G.; Bianco, A.; Moro, T. The Influence of Meal Frequency and Timing on Health in Humans: The Role of Fasting. Nutrients 2019, 11, 719. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.Z.; Andersen, T.; Radovic, S.; Del Fante, P.; Kwiatek, R.; Calhoun, V.; Bhuta, S.; Hermens, D.F.; Lagopoulos, J.; Shan, Z.Y. Objective sleep measures in chronic fatigue syndrome patients: A systematic review and meta-analysis. Sleep Med. Rev. 2023, 69, 101771. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhan, S.; Tian, Z.; Li, N.; Li, T.; Wu, D.; Zeng, Z.; Zhuang, X. Food Additives Associated with Gut Microbiota Alterations in Inflammatory Bowel Disease: Friends or Enemies? Nutrients 2022, 14, 3049. [Google Scholar] [CrossRef] [PubMed]
- Hou, K.; Wu, Z.X.; Chen, X.Y.; Wang, J.Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in health and diseases. Signal Transduct. Target. Ther. 2022, 7, 135. [Google Scholar] [CrossRef]
- Lotti, S.; Dinu, M.; Colombini, B.; Amedei, A.; Sofi, F. Circadian rhythms, gut microbiota, and diet: Possible implications for health. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1490–1500. [Google Scholar] [CrossRef]


{kind=link}
| Nutritional and Chronobiologic Recommendations |
|---|
Nutrition
|
Chronobiology
|
Others
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrasco-Querol, N.; Cabricano-Canga, L.; Bueno Hernández, N.; Gonçalves, A.Q.; Caballol Angelats, R.; Pozo Ariza, M.; Martín-Borràs, C.; Montesó-Curto, P.; Castro Blanco, E.; Dalmau Llorca, M.R.; et al. Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review. Nutrients 2024, 16, 182. https://doi.org/10.3390/nu16020182
Carrasco-Querol N, Cabricano-Canga L, Bueno Hernández N, Gonçalves AQ, Caballol Angelats R, Pozo Ariza M, Martín-Borràs C, Montesó-Curto P, Castro Blanco E, Dalmau Llorca MR, et al. Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review. Nutrients. 2024; 16(2):182. https://doi.org/10.3390/nu16020182
Chicago/Turabian StyleCarrasco-Querol, Noèlia, Lorena Cabricano-Canga, Nerea Bueno Hernández, Alessandra Queiroga Gonçalves, Rosa Caballol Angelats, Macarena Pozo Ariza, Carme Martín-Borràs, Pilar Montesó-Curto, Elisabet Castro Blanco, Maria Rosa Dalmau Llorca, and et al. 2024. "Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review" Nutrients 16, no. 2: 182. https://doi.org/10.3390/nu16020182
APA StyleCarrasco-Querol, N., Cabricano-Canga, L., Bueno Hernández, N., Gonçalves, A. Q., Caballol Angelats, R., Pozo Ariza, M., Martín-Borràs, C., Montesó-Curto, P., Castro Blanco, E., Dalmau Llorca, M. R., & Aguilar Martín, C. (2024). Nutrition and Chronobiology as Key Components of Multidisciplinary Therapeutic Interventions for Fibromyalgia and Associated Chronic Fatigue Syndrome: A Narrative and Critical Review. Nutrients, 16(2), 182. https://doi.org/10.3390/nu16020182