



Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
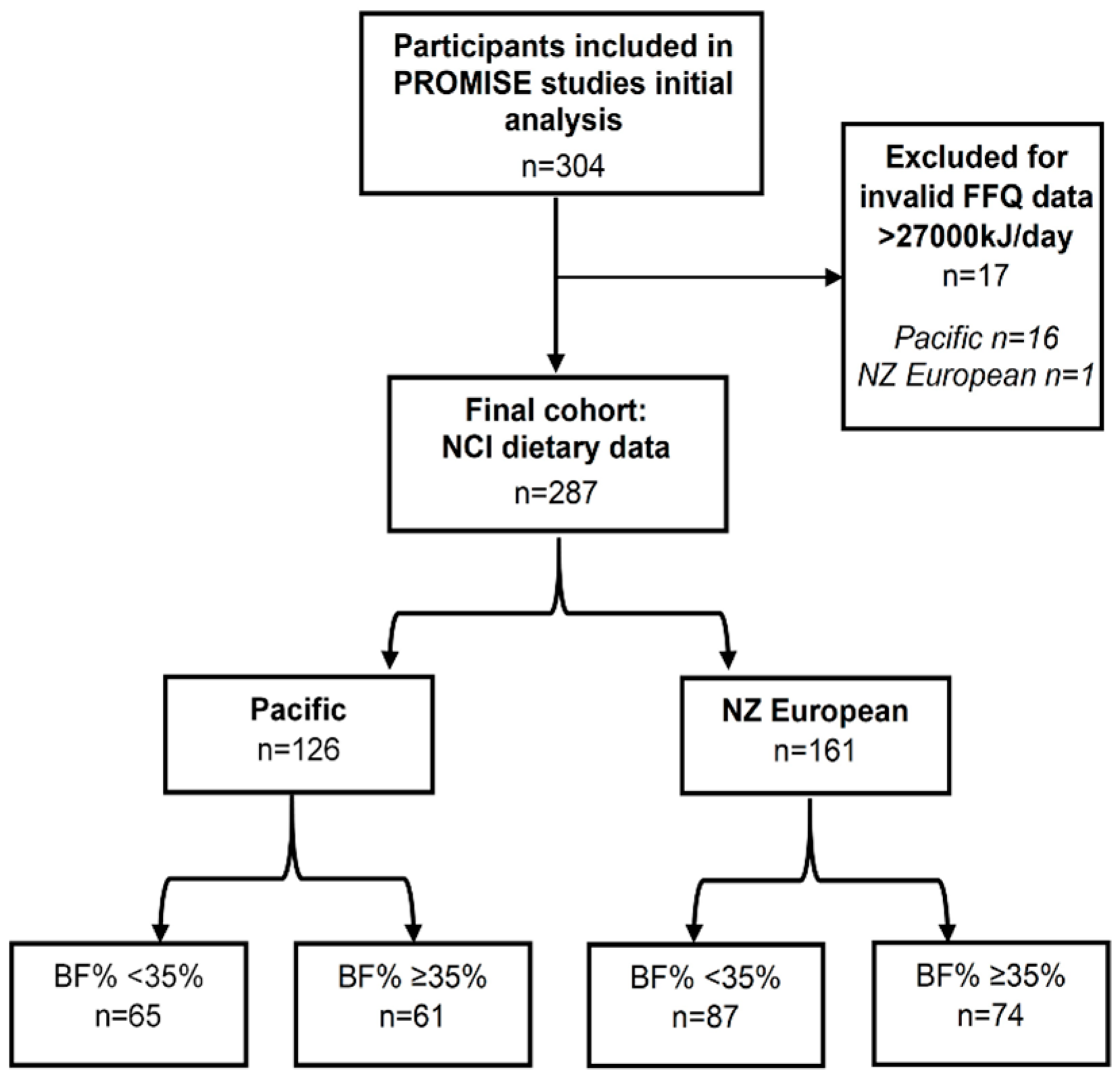
2.1. Study Design
2.2. Assessment of Demographic, Anthropometric and Metabolic Risk Factors
2.3. Dietary Assessment
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Participants
3.2. Dietary Fibre Intake
Nutrient Intake
3.3. Association between Dietary Fibre Intake, Metabolic Risk Factors and Metabolic Syndrome
3.4. Main Food Sources of Dietary Fibre
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Methods
Blood Analyses
Appendix A.2. Power Calculation
Appendix A.3. Dietary Assessment
Appendix A.4. Habitual Dietary Intake
Appendix A.5. Physical Activity
References
- Ministry of Health. New Zealand Health Survey 2020/21: Body Size: Obese: BMI of 30.0 or Greater. Available online: https://www.health.govt.nz/nz-health-statistics/health-statistics-and-data-sets/obesity-statistics (accessed on 18 July 2024).
- Yu, D.; Zhao, Z.; Osuagwu, U.L.; Pickering, K.; Baker, J.; Cutfield, R.; Orr-Walker, B.J.; Cai, Y.; Simmons, D. Ethnic Differences in Mortality and Hospital Admission Rates between Māori, Pacific, and European New Zealanders with Type 2 Diabetes between 1994 and 2018: A Retrospective, Population-Based, Longitudinal Cohort Study. Lancet Glob. Health 2020, 9, e209–e217. [Google Scholar] [CrossRef] [PubMed]
- Coppell, K.J.; Mann, J.I.; Williams, S.M.; Jo, E.; Drury, P.L.; Miller, J.; Parnell, W.R. Prevalence of Diagnosed and Undiagnosed Diabetes and Prediabetes in New Zealand: Findings from the 2008/09 Adult Nutrition Survey. N. Z. Med. J. 2013, 126, 23–42. [Google Scholar] [PubMed]
- Health New Zealand Te Whatu Ora. Aotearoa New Zealand Health Status Report. 2023. Available online: https://www.tewhatuora.govt.nz/publications/health-status-report/ (accessed on 18 July 2024).
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. 2018. Available online: https://www.wcrf.org/dietandcancer/summary-third-expert-report (accessed on 20 August 2024).
- Ministry of Health. Eating and Activity Guidelines for New Zealand Adults: Updated 2020. Wellington. 2020. Available online: https://www.health.govt.nz/system/files/documents/publications/eating-activity-guidelines-new-zealand-adults-updated-2020-jul21.pdf (accessed on 2 September 2024).
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a WHO Study Group [Meeting Held in Geneva from 6–13 March 1989]. Geneva. 1990. Available online: https://iris.who.int/handle/10665/39426 (accessed on 18 July 2024).
- National Health and Medical Research Council; Australian Government Department of Health and Ageing; New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand; National Health and Medical Research Council: Canberra, Australia, 2006.
- University of Otago and Ministry of Health. A Focus on Nutrition: Key Findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011.
- Ministry of Health. Adults’ Dietary Habits—Findings from the 2018/19 and 2019/20 New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2022.
- Eriksson, J.G.; Sandboge, S.; Salonen, M.K.; Kajantie, E.; Osmond, C. Long-Term Consequences of Maternal Overweight in Pregnancy on Offspring Later Health: Findings from the Helsinki Birth Cohort Study. Ann. Med. 2014, 46, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Renall, N.; Merz, B.; Douwes, J.; Corbin, M.; Slater, J.; Tannock, G.W.; Firestone, R.; Kruger, R.; Breier, B.H.; Te Morenga, L. Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women. Proc. Nutr. Soc. 2024, 83, E21. [Google Scholar] [CrossRef]
- Oliveros, E.; Somers, V.K.; Sochor, O.; Goel, K.; Lopez-Jimenez, F. The Concept of Normal Weight Obesity. Prog. Cardiovasc. Dis. 2014, 56, 426–433. [Google Scholar] [CrossRef]
- Kramer, C.; Zinman, B.; Retnakaran, R. Are Metabolically Healthy Overweight and Obesity Benign Conditions? A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2013, 159, 758–769. [Google Scholar] [CrossRef]
- Dickey, R.A.; Bartuska, D.G.; Bray, G.W.; Callaway, C.W.; Davidson, E.T.; Feld, S.; Ferraro, R.T.; Hodgson, S.F.; Jellinger, P.S.; Kennedy, F.P.; et al. AACE/ACE Position Statement on the Prevention, Diagnosis, and Treatment of Obesity (1998 Revision) AACE/ACE Obesity Task Force. Endocr. Pract. 1998, 4, 297–350. [Google Scholar]
- Jo, A.; Mainous, A.G. Informational Value of Percent Body Fat with Body Mass Index for the Risk of Abnormal Blood Glucose: A Nationally Representative Cross-Sectional Study. BMJ Open 2018, 8, e019200. [Google Scholar] [CrossRef]
- Kindleysides, S.; Kruger, R.; Douwes, J.; Tannock, G.; Renall, N.; Slater, J.; Lawley, B.; McGill, A.-T.; Brennan, N.; Manukia, M.; et al. PRedictors Linking Obesity and the Gut MIcrobiomE (The PROMISE Study): Protocol and Recruitment Strategy of a Cross-Sectional Study on Pathways That Affect the Gut Microbiome and Its Impact on Obesity. JMIR Res. Protoc. 2019, 8, e14529. [Google Scholar] [CrossRef]
- Atkinson, J.; Salmond, C.; Crampton, P. NZDep2013 Index of Deprivation; Department of Public Health, University of Otago: Wellington, New Zealand, 2014. [Google Scholar]
- Ministry of Health. Clinical Guidelines for Weight Management in New Zealand Adults; Ministry of Health: Wellington, New Zealand, 2017.
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Beck, K.L.; Houston, Z.L.; McNaughton, S.A.; Kruger, R. Development and Evaluation of a Food Frequency Questionnaire to Assess Nutrient Intakes of Adult Women in New Zealand. Nutr. Diet. 2018, 77, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Kipnis, V.; Midthune, D.; Buckman, D.W.; Dodd, K.W.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Tooze, J.A.; Carroll, R.J.; Freedman, L.S. Modeling Data with Excess Zeros and Measurement Error: Application to Evaluating Relationships between Episodically Consumed Foods and Health Outcomes. Biometrics 2009, 65, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A New Statistical Method for Estimating the Usual Intake of Episodically Consumed Foods with Application to Their Distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef]
- Beck, K.L.; Jones, B.; Ullah, I.; McNaughton, S.A.; Haslett, S.J.; Stonehouse, W. Associations between Dietary Patterns, Socio-Demographic Factors and Anthropometric Measurements in Adult New Zealanders: An Analysis of Data from the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Nutr. 2018, 57, 1421–1433. [Google Scholar] [CrossRef]
- Ministry of Health. New Zealand Health Survey 2020/2021: Nutrition: Vegetable and Fruit Intake. Indicator: Eating 3+ Servings of Vegetables and 2+ Servings of Fruit per Day. Available online: https://www.health.govt.nz/publication/annual-update-key-results-2021-22-new-zealand-health-survey (accessed on 18 July 2024).
- Tucker, L.A.; Thomas, K.S. Increasing Total Fiber Intake Reduces Risk of Weight and Fat Gains in Women. J. Nutr. 2009, 139, 576–581. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate Quality and Human Health: A Series of Systematic Reviews and Meta-Analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef]
- McRorie, J.W.; McKeown, N.M. Understanding the Physics of Functional Fibers in the Gastrointestinal Tract: An Evidence-Based Approach to Resolving Enduring Misconceptions about Insoluble and Soluble Fiber. J. Acad. Nutr. Diet. 2017, 117, 251–264. [Google Scholar] [CrossRef]
- Valdes, A.M.; Walter, J.; Segal, E.; Spector, T.D. Role of the Gut Microbiota in Nutrition and Health. BMJ 2018, 361, k2179. [Google Scholar] [CrossRef]
- Tannock, G.W. Modulating the Gut Microbiota of Humans by Dietary Intervention with Plant Glycans. Appl. Environ. Microbiol. 2021, 87, e02757-20. [Google Scholar] [CrossRef]
- Renall, N.; Lawley, B.; Vatanen, T.; Merz, B.; Douwes, J.; Corbin, M.; Te Morenga, L.; Kruger, R.; Breier, B.H.; Tannock, G.W. The Fecal Microbiotas of Women of Pacific and New Zealand European Ethnicities Are Characterized by Distinctive Enterotypes That Reflect Dietary Intakes and Fecal Water Content. Gut Microbes 2023, 15, 2178801. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [PubMed]
- Wei, B.; Liu, Y.; Lin, X.; Fang, Y.; Cui, J.; Wan, J. Dietary Fiber Intake and Risk of Metabolic Syndrome: A Meta-Analysis of Observational Studies. Clin. Nutr. 2018, 37, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Contribution of Food Prices and Diet Cost to Socioeconomic Disparities in Diet Quality and Health: A Systematic Review and Analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Herforth, A.; Bai, Y.; Venkat, A.; Mahrt, K.; Ebel, A.; Masters, W.A. Cost and Affordability of Healthy Diets across and within Countries: Background Paper for the State of Food Security and Nutrition in the World 2020; FAO: Rome, Italy, 2020. [Google Scholar] [CrossRef]
- Pearce, J.; Blakely, T.; Witten, K.; Bartie, P. Neighborhood Deprivation and Access to Fast-Food Retailing. Am. J. Prev. Med. 2007, 32, 375–382. [Google Scholar] [CrossRef]
- Sui, Z.; Wong, W.K.; Louie, J.C.Y.; Rangan, A. Discretionary Food and Beverage Consumption and Its Association with Demographic Characteristics, Weight Status, and Fruit and Vegetable Intakes in Australian Adults. Public Health Nutr. 2017, 20, 274–281. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; Cassettari, T.; Tuck, K.; McConnell, A.; Petocz, P. Dietary Fibre Intake in Australia. Paper I: Associations with Demographic, Socio-Economic, and Anthropometric Factors. Nutrients 2018, 10, 599. [Google Scholar] [CrossRef]
- Sushil, Z.; Vandevijvere, S.; Exeter, D.J.; Swinburn, B. Food Swamps by Area Socioeconomic Deprivation in New Zealand: A National Study. Int. J. Public Health 2017, 62, 869–877. [Google Scholar] [CrossRef]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing Current Criticism Regarding the Value of Self-Report Dietary Data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef]
- Cade, J.E.; Warthon-Medina, M.; Albar, S.; Alwan, N.A.; Ness, A.; Roe, M.; Wark, P.A.; Greathead, K.; Burley, V.J.; Finglas, P.; et al. DIET@NET: Best Practice Guidelines for Dietary Assessment in Health Research. BMC Med. 2017, 15, 202. [Google Scholar] [CrossRef]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar] [CrossRef]
- Gemming, L.; Jiang, Y.; Swinburn, B.; Utter, J.; Mhurchu, C.N. Under-Reporting Remains a Key Limitation of Self-Reported Dietary Intake: An Analysis of the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Clin. Nutr. 2014, 68, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, P.A.; Scragg, R.R.K.; Schaaf, D.; Dyall, L.; Black, P.N.; Jackson, R. Dietary Intakes of European, Māori, Pacific and Asian Adults Living in Auckland: The Diabetes, Heart and Health Study. Aust. N. Z. J. Public Health 2008, 32, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Slater, J.; Kruger, R.; Douwes, J.; O’Brien, W.J.; Corbin, M.; Miles-Chan, J.L.; Breier, B.H. Objectively Measured Physical Activity Is Associated with Body Composition and Metabolic Profiles of Pacific and New Zealand European Women with Different Metabolic Disease Risks. Front. Physiol. 2021, 12, 684782. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Pacific | NZ European | |||
|---|---|---|---|---|
| Low-BF% n = 65 | High-BF% n = 61 | Low-BF% n = 87 | High-BF% n = 74 | |
| Age (y) | 23 [20, 29] | 23 [21, 29] | 29 [24, 36] † | 35 [28, 40] *† |
| NZDep2013 a | 7 [5, 9] | 8 [7, 9] | 3 [2, 6] † | 5 [3, 6] *† |
| Body composition | ||||
| Weight (kg) | 72.4 [67.3, 79.1] | 97.0 [87.4, 109.9] * | 62.4 [58.1, 66.6] † | 94.1 [86.8, 101.7] * |
| BMI (kg/m2) | 25.0 [23.6, 27.6] | 33.8 [31.1, 39.9] * | 22.5 [20.9, 23.5] † | 33.5 [31.7, 36.3] * |
| Waist circumference (cm) | 78.1 [75.1, 84.6] | 97.0 [89.0, 108.3] * | 73.1 [69.5, 75.8] † | 97.0 [91.9, 102.8] * |
| Body fat (%) | 29.6 [27.9, 32.3] | 39.5 [36.6, 42.4] * | 28.0 [24.2, 31.9] † | 40.3 [38.7, 44.2] *† |
| Visceral fat (%) | 26.8 [23.1, 31.4] | 40.3 [35.6, 43.3] * | 21.5 [16.8, 27.3] † | 39.7 [35.7, 44.0] * |
| Metabolic Syndrome (n [%]) | 5 (8%) | 23 (38%) | 0 (0%) | 29 (39%) |
| Blood pressure | ||||
| Systolic (mmHg) | 113 [106, 119] | 117 [111, 128] * | 113 [105, 119] | 120 [111, 128] * |
| Diastolic (mmHg) | 71 [65, 74] | 77 [71, 84] * | 69 [66, 76] | 80 [74, 85] * |
| Metabolic markers b | ||||
| TC (mmol/L) | 4.5 [4.1, 5.1] | 4.6 [4.2, 5.1] | 4.9 [4.3, 5.4] † | 5.2 [4.7, 6.1] *† |
| HDL-C (mmol/L) | 1.5 [1.3, 1.8] | 1.3 [1.2, 1.6] * | 1.8 [1.6, 2.0] † | 1.4 [1.3, 1.7] *† |
| LDL-C (mmol/L) | 2.8 [2.4, 3.2] | 3.0 [2.5, 3.3] | 2.8 [2.4, 3.4] | 3.4 [2.7, 4.1] *† |
| TAG (mmol/L) | 0.8 [0.7, 1.1] | 1.0 [0.9, 1.5] * | 0.7 [0.6, 0.9] | 1.1 [0.8, 1.5] * |
| HbA1c (mmol/L) | 32.1 [30.5, 33.8] | 34.8 [32.3, 36.7] * | 30.6 [29.0, 31.9] † | 31.0 [29.8, 33.3] *† |
| Fasting Glucose (mmol/L) | 5.3 [5.0, 5.5] | 5.4 [5.1, 5.9] * | 5.1 [4.9, 5.3] † | 5.5 [5.1, 5.7] * |
| Fasting Insulin (uU/mL) | 11.2 [7.9, 16.0] | 21.4 [13.1, 31.9] * | 7.1 [5.2, 8.7] † | 12.6 [10.0, 17.9] *† |
| Nutrient intake | ||||
| Energy (kJ/day) | 8749 [8405, 8986] | 8555 [8045, 8894] | 8307 [8033, 8660] † | 8634 [8188, 8858] * |
| Protein (E %/day) | 15.1 [13.5, 17.2] | 15.9 [14.0, 18.4] | 16.7 [15.4, 18.1] † | 16.9 [15.2, 18.1] |
| Total fat (E %/day) | 39.2 [33.7, 45.1] | 39.1 [31.5, 44.0] | 41.1 [35.7, 47.1] | 39.3 [34.5, 45.9] |
| SFA (E %/day) | 14.9 [12.8, 17.4] | 15.5 [12.8, 16.9] | 14.8 [12.4, 17.4] | 15.1 [13.8, 17.8] |
| PUFA (E %/day) | 5.3 [4.1, 6.0] | 4.7 [3.9, 5.8] | 6.0 [5.0, 7.0] † | 5.3 [4.3, 6.1] *† |
| MUFA (E %/day) | 14.9 [12.7, 16.4] | 14.3 [12.3, 17.0] | 15.6 [13.2, 17.7] | 14.5 [12.4, 17.2] |
| CHO (E %/day) | 40.6 [34.1, 47.5] | 42.7 [33.8, 45.6] | 35.5 [30.4, 40.3] † | 35.8 [31.5, 40.5] † |
| Sugar (g/day) c | 82.5 [74.0, 102.7] | 78.9 [66.1, 96.2] | 80.2 [66.0, 89.5] † | 79.8 [68.8, 95.8] |
| Starch (g/day) | 125.7 [105.1, 145.2] | 128.1 [109.1, 146.3] | 102.5 [82.0, 119.0] † | 104.7 [84.9, 119.8] † |
| Dietary Fibre (g/day) | 18.8 [15.6, 22.1] | 17.8 [15.0, 20.8] | 23.7 [20.1, 29.9] † | 20.9 [19.4, 24.9] *† |
| Dietary Fibre (g/MJ/day) | 2.1 [1.8, 2.5] | 2.1 [1.8, 2.4] | 2.9 [2.5, 3.5] † | 2.5 [2.2, 3.0] *† |
| Variable | All Participants a β (95% CI) n = 284 | p Value | Pacific β (95% CI) n = 124 | p Value | NZ European β (95% CI) n = 160 | p Value |
|---|---|---|---|---|---|---|
| Body composition | ||||||
| Weight (kg) | −1.10 [−1.53, −0.66] | p < 0.001 | −1.61 [−2.59, −0.63] | p = 0.014 | −1.06 [−1.53, −0.59] | p < 0.001 |
| BMI (kg/m2) | −0.38 [−0.53, −0.24] | p < 0.001 | −0.53 [−0.86, −0.21] | p = 0.017 | −0.38 [−0.53, −0.22] | p < 0.001 |
| Waist Circumference | −0.80 [−1.11, −0.49] | p < 0.001 | −1.01 [−1.69, −0.33] | p = 0.004 | −0.80 [−1.16, −0.45] | p < 0.001 |
| Total body fat % | −0.47 [−0.62, −0.31] | p < 0.001 | −0.48 [−0.77, −0.19] | p = 0.016 | −0.48 [−0.68, −0.28] | p < 0.001 |
| Visceral fat % | −0.61 [−0.82, −0.40] | p < 0.001 | −0.59 [−1.01, −0.18] | p = 0.006 | −0.64 [−0.90, −0.37] | p < 0.001 |
| Metabolic markers b,c | ||||||
| TC (mmol/L) | −0.04 [−0.06, −0.01] | p = 0.001 | −0.02 [−0.05, 0.02] | p = 0.328 | −0.04 [−0.06, −0.01] | p = 0.016 |
| HDL-C (mmol/L) | 0.0004 [−0.01, 0.01] | p = 0.910 | 0.003 [−0.01, 0.02] | p = 0.700 | 0.001 [−0.01, 0.01] | p = 0.897 |
| LDL-C (mmol/L) | −0.03 [−0.05, −0.01] | p = 0.002 | −0.01 [−0.05, 0.02] | p = 0.521 | −0.04 [−0.06, −0.01] | p = 0.015 |
| TAG (mmol/L) | −0.01 [−0.02, 0.01] | p = 0.304 | −0.01 [−0.04, 0.01] | p = 0.333 | −0.04 [−0.02, 0.01] | p = 0.511 |
| HbA1c (mmol/L) d | −0.005 [−0.07, 0.06] | p = 0.882 | −0.05 [−0.21, 0.10] | p = 0.488 | −0.01 [−0.08, 0.06] | p = 0.829 |
| Fasting Glucose (mmol/L) | −0.02 [−0.02, 0.0005] | p = 0.061 | −0.01 [−0.04, 0.01] | p = 0.370 | −0.01 [−0.02, 0.002] | p = 0.125 |
| Fasting Insulin e | 0.99 [0.98, 1.00] | p = 0.101 | 0.97 [0.94, 1.00] | p = 0.046 | 0.99 [0.98, 1.01] | p = 0.226 |
| Metabolic syndrome (OR) f | 0.91 [0.84, 0.98] | p = 0.010 | 0.93 [0.81, 1.05] | p = 0.238 | 0.90 [0.82, 0.98] | p = 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renall, N.; Merz, B.; Douwes, J.; Corbin, M.; Slater, J.; Tannock, G.W.; Firestone, R.; Kruger, R.; Te Morenga, L. Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women. Nutrients 2024, 16, 3399. https://doi.org/10.3390/nu16193399
Renall N, Merz B, Douwes J, Corbin M, Slater J, Tannock GW, Firestone R, Kruger R, Te Morenga L. Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women. Nutrients. 2024; 16(19):3399. https://doi.org/10.3390/nu16193399
Chicago/Turabian StyleRenall, Nikki, Benedikt Merz, Jeroen Douwes, Marine Corbin, Joanne Slater, Gerald W. Tannock, Ridvan Firestone, Rozanne Kruger, and Lisa Te Morenga. 2024. "Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women" Nutrients 16, no. 19: 3399. https://doi.org/10.3390/nu16193399
APA StyleRenall, N., Merz, B., Douwes, J., Corbin, M., Slater, J., Tannock, G. W., Firestone, R., Kruger, R., & Te Morenga, L. (2024). Dietary Fibre Intake, Adiposity, and Metabolic Disease Risk in Pacific and New Zealand European Women. Nutrients, 16(19), 3399. https://doi.org/10.3390/nu16193399