
Resistance Training and Nutritional Supplementation in Older Adults with Sarcopenia after Acute Disease: A Feasibility Study

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Settings
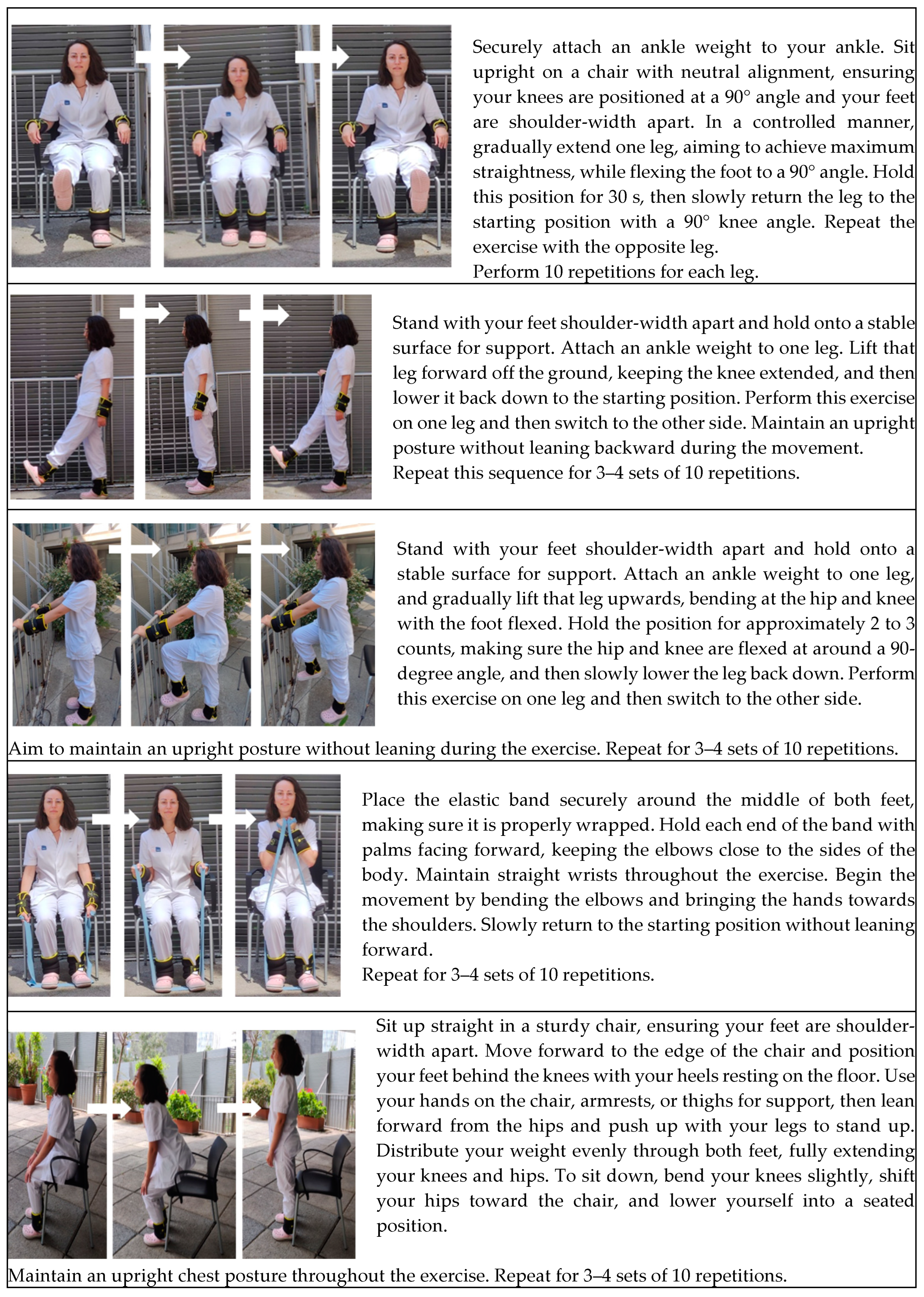
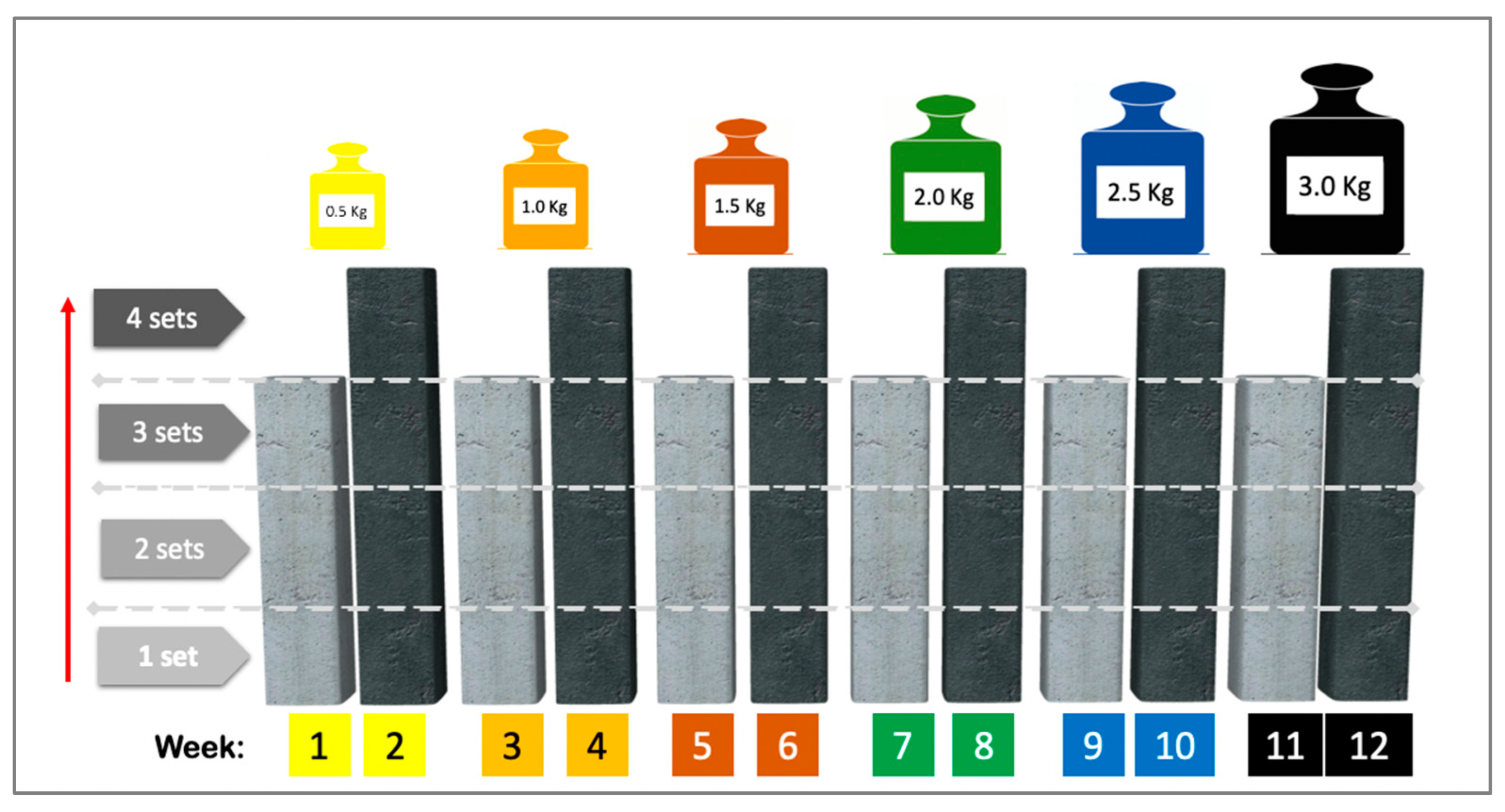
2.4. Intervention
2.5. Primary Outcome
2.6. Secondary Outcomes
2.7. Other Variables
2.8. Statistical Analysis
3. Results
- (a)
- The reasons for permanent treatment discontinuation were deterioration in general condition (two participants in each group), supplement had an unpleasant taste (two participants in each group), lack of interest in continuing (one participant in the control group), moving out of the city (one participant in the control group), fear of being infected by Coronavirus disease (COVID-19) (one participant in the control group); and lack of family support for attending the program (the second reason for one participant in the control group).
- (b)
- Treatment interruption: Among the participants who completed 70% or more of the intervention, six participants (18.8%, four participants in the intervention group and two participants in the control group) interrupted the exercise program, while four (12.5%, two participants in each group) interrupted the supplementation. The causes were exacerbated chronic low back pain, COVID-19 onset, pulmonary disease exacerbation, and holidays. No significant differences were found between the groups.
- (c)
- Exercise dose modification: Six participants (18.8%, three participants in each group) required modification of some parameter of the progressive resistance exercise program; the reasons for this are listed in Table 5.
- (d)
- Early termination: Nine participants (28.1%) ended participation earlier than planned for the following reasons: sudden onset of COVID-19 (two patients in the intervention group and one in the control group), exacerbation of chronic disease (one patient in the control group), and reasons unrelated to the intervention, such as holidays and vacations (four in the intervention group and one in the control group).
- (e)
- Re-scheduling of missed sessions: Six participants rescheduled 21 sessions (18.8%, three patients in each group).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Bernabei, R.; Vellas, B.; Fielding, R.A.; Rooks, D.; Azzolino, D.; Mariani, J.; Oliva, A.A.; Bhasin, S.; Rolland, Y. Challenges in the Development of Drugs for Sarcopenia and Frailty—Report from the International Conference on Frailty and Sarcopenia Research (ICFSR) Task Force. J. Frailty Aging 2022, 11, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zou, L.; Chen, S.T.; Bae, J.H.; Kim, D.Y.; Liu, X.; Song, W. Effects and Moderators of Exercise on Sarcopenic Components in Sarcopenic Elderly: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 649748. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: A meta-analysis. Ageing Res. Rev. 2010, 9, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength. Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef] [PubMed]
- Costa Riela, N.A.; Alvim Guimarães, M.M.; Oliveira de Almeida, D.; Araujo, E.M.Q. Effects of Beta-Hydroxy-Beta-Methylbutyrate Supplementation on Elderly Body Composition and Muscle Strength: A Review of Clinical Trials. Ann. Nutr. Metab. 2021, 77, 16–22. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Bear, D.E.; Langan, A.; Dimidi, E.; Wandrag, L.; Harridge, S.D.R.; Hart, N.; Connolly, B.; Whelan, K. β-Hydroxy-β-methylbutyrate and its impact on skeletal muscle mass and physical function in clinical practice: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2019, 109, 1119–1132. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Ji, N.N.; Ma, J.X.; Dong, Q.; Ma, X.L. Effect of Resistance Training Combined with Beta-Hydroxy-Beta-Methylbutyric Acid Supplements in Elderly Patients with Sarcopenia after Hip Replacement. Orthop. Surg. 2022, 14, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, K.; Broom, D.; Bekhet, A.H.; de Caro, J.X.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-aged and Older-adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Aging. Four Types of Exercise Can Improve Your Health and Physical Ability. U.S. Department of Health and Human Services. Available online: https://www.nia.nih.gov/health/exercise-and-physical-activity/four-types-exercise-can-improve-your-health-and-physical (accessed on 10 March 2023).
- Kanach, F.A.; Pastva, A.M.; Hall, K.S.; Pavon, J.M.; Morey, M.C. Effects of Structured Exercise Interventions for Older Adults Hospitalized With Acute Medical Illness: A Systematic Review. J. Aging Phys. Act. 2018, 26, 284–303. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M. Language Matters. Phys. Ther. 2016, 96, 754–755. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M. Opening Up the Black Box of Peer Review. Phys. Ther. 2018, 98, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Argudo, N.; Rodó-Pin, A.; Martínez-Llorens, J.; Marco, E.; Visa, L.; Messaggi-Sartor, M.; Balañá-Corberó, A.; Ramón, J.M.; Rodríguez-Chiaradía, D.A.; Grande, L.; et al. Feasibility, tolerability, and effects of exercise-based prehabilitation after neoadjuvant therapy in esophagogastric cancer patients undergoing surgery: An interventional pilot study. Dis. Esophagus 2020, 34, doaa086. [Google Scholar] [CrossRef]
- Reginster, J.Y.; Beaudart, C.; Al-Daghri, N.; Avouac, B.; Bauer, J.; Bere, N.; Bruyère, O.; Cerreta, F.; Cesari, M.; Rosa, M.M.; et al. Update on the ESCEO recommendation for the conduct of clinical trials for drugs aiming at the treatment of sarcopenia in older adults. Aging Clin. Exp. Res. 2021, 33, 3–17. [Google Scholar] [CrossRef]
- Cambridge Dictionary. Feasibility Study. Available online: https://dictionary.cambridge.org/dictionary/english/feasibility-study (accessed on 1 February 2024).
- Orsmond, G.I.; Cohn, E.S. The Distinctive Features of a Feasibility Study: Objectives and Guiding Questions. Occup. Ther. J. Res. 2015, 35, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Kharaghani, R.; Shariati, M.; Yunesian, M.; Keramat, A.; Moghisi, A. Feasibility Study of the Pregnancy Risk Assessment Monitoring System in Iran. Iran. J. Public Health 2014, 43, 1669–1679. [Google Scholar]
- van Lummel, E.V.T.J.; Savelkoul, C.; Stemerdink, E.L.E.; Tjan, D.H.T.; van Delden, J.J.M. The development and feasibility study of Multidisciplinary Timely Undertaken Advance Care Planning conversations at the outpatient clinic: The MUTUAL intervention. BMC Palliat. Care 2022, 21, 119. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Sánchez-Rodríguez, D.; Messaggi-Sartor, M.; Muñoz-Redondo, E.; Morgado-Pérez, A.; Tejero-Sánchez, M.; De Jaime-Gil, E.; Leiva-Banuelos, N.; Marco, E. Supplementation with β-hydroxy-β-methylbutyrate after resistance training in post-acute care patients with sarcopenia: A randomized, double-blind placebo-controlled trial. Arch. Gerontol. Geriatr. 2023, 119, 105323. [Google Scholar] [CrossRef] [PubMed]
- Tuvemo Johnson, S.; Anens, E.; Johansson, A.C.; Hellström, K. The Otago Exercise Program with or without Motivational Interviewing for Community-Dwelling Older Adults: A 12-Month Follow-Up of a Randomized, Controlled Trial. J. Appl. Gerontol. 2021, 40, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, D.; Marco, E.; Ronquillo-Moreno, N.; Miralles, R.; Mojal, S.; Vázquez-Ibar, O.; Escalada, F.; Muniesa, J.M. The PSSMAR study. Postacute sarcopenia: Supplementation with β-hydroxyMethylbutyrate after resistance training: Study protocol of a randomized, double-blind controlled trial. Maturitas 2016, 94, 117–124. [Google Scholar] [CrossRef]
- Schutz, Y.; Kyle, U.U.; Pichard, C. Fat-free mass index and fat mass index percentiles in Caucasians aged 18–98 y. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 953–960. [Google Scholar] [CrossRef]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Minetto, M.A.; Lanfranco, F.; Motta, G.; Allasia, S.; Arvat, E.; D’Antona, G. Steroid myopathy: Some unresolved issues. J. Endocrinol. Investig. 2011, 34, 370–375. [Google Scholar] [CrossRef]
- Nilsson, M.I.; Mikhail, A.; Lan, L.; Di Carlo, A.; Hamilton, B.; Barnard, K.; Hettinga, B.P.; Hatcher, E.; Tarnopolsky, M.G.; Nederveen, J.P.; et al. A Five-Ingredient Nutritional Supplement and Home-Based Resistance Exercise Improve Lean Mass and Strength in Free-Living Elderly. Nutrients 2020, 12, 2391. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. Bmj 2014, 348, g1687. [Google Scholar] [CrossRef]
- Drljaca, D.P.; Latinovic, B. Using TELOS for the planning of the information system audit. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Hunedoara, Romania, 10–12 May 2017; Volume 294, p. 012022. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Sánchez-Rodríguez, D.; Perkisas, S.; Duran, X.; Bastijns, S.; Dávalos-Yerovi, V.; Da Costa, E.; Marco, E. The feasibility and reliability of measuring forearm muscle thickness by ultrasound in a geriatric inpatient setting: A cross-sectional pilot study. BMC Geriatr. 2022, 22, 137. [Google Scholar] [CrossRef]
- Marco, E.; Ramírez-Sarmiento, A.L.; Coloma, A.; Sartor, M.; Comin-Colet, J.; Vila, J.; Enjuanes, C.; Bruguera, J.; Escalada, F.; Gea, J.; et al. High-intensity vs. sham inspiratory muscle training in patients with chronic heart failure: A prospective randomized trial. Eur. J. Heart Fail. 2013, 15, 892–901. [Google Scholar] [CrossRef]
- Messaggi-Sartor, M.; Guillen-Solà, A.; Depolo, M.; Duarte, E.; Rodríguez, D.A.; Barrera, M.C.; Barreiro, E.; Escalada, F.; Orozco-Levi, M.; Marco, E. Inspiratory and expiratory muscle training in subacute stroke: A randomized clinical trial. Neurology 2015, 85, 564–572. [Google Scholar] [CrossRef]
- Jacques, R.M.; Ahmed, R.; Harper, J.; Ranjan, A.; Saeed, I.; Simpson, R.M.; Walters, S.J. Recruitment, consent and retention of participants in randomised controlled trials: A review of trials published in the National Institute for Health Research (NIHR) Journals Library (1997–2020). BMJ Open 2022, 12, e059230. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, T.S.; Scott, J.M.; Michalski, M.; Capaci, C.; Thomas, S.; Herndon, J.E., 2nd; Sasso, J.; Eves, N.D.; Jones, L.W. Novel Methods for Reporting of Exercise Dose and Adherence: An Exploratory Analysis. Med. Sci. Sports Exerc. 2018, 50, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Agency, E.M. Clinical Safety Data Management: Definitions and Standards for Expedited Reporting. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/international-conference-harmonisation-technical-requirements-registration-pharmaceuticals-human-use_en-15.pdf (accessed on 7 February 2023).
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Glasheen, W.P.; Cordier, T.; Gumpina, R.; Haugh, G.; Davis, J.; Renda, A. Charlson Comorbidity Index: ICD-9 Update and ICD-10 Translation. Am. Health Drug Benefits 2019, 12, 188–197. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Reginster, J.Y.; Geerinck, A.; Locquet, M.; Bruyère, O. Current review of the SarQoL®: A health-related quality of life questionnaire specific to sarcopenia. Exp. Rev. Pharmacoecon. Outcomes Res. 2017, 17, 335–341. [Google Scholar] [CrossRef]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Guralnik, J.; Bandeen-Roche, K.; Bhasin, S.A.R.; Eremenco, S.; Landi, F.; Muscedere, J.; Perera, S.; Reginster, J.Y.; Woodhouse, L.; Vellas, B. Clinically Meaningful Change for Physical Performance: Perspectives of the ICFSR Task Force. J. Frailty Aging 2020, 9, 9–13. [Google Scholar] [CrossRef]
- Feike, Y.; Zhijie, L.; Wei, C. Advances in research on pharmacotherapy of sarcopenia. Aging Med. 2021, 4, 221–233. [Google Scholar] [CrossRef]
- Bauer, J.; Morley, J.E.; Schols, A.M.W.J.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; et al. Sarcopenia: A Time for Action. An SCWD Position Paper. J. Cachexia Sarcopenia Muscle 2019, 10, 956–961. [Google Scholar] [CrossRef]
- Chan, H.C.N.; Fei, X.; Leung, E.L.Y.; Langston, K.; Marshall, S.; van der Meij, B.S. Post-discharge consequences of protein-energy malnutrition, sarcopenia, and frailty in older adults admitted to rehabilitation: A systematic review. Clin. Nutr. ESPEN 2023, 54, 382–397. [Google Scholar] [CrossRef] [PubMed]
- Collado-Mateo, D.; Lavín-Pérez, A.M.; Peñacoba, C.; Del Coso, J.; Leyton-Román, M.; Luque-Casado, A.; Gasque, P.; Fernández-Del-Olmo, M.; Amado-Alonso, D. Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 2023. [Google Scholar] [CrossRef] [PubMed]
- Rúa-Alonso, M.; Bovolini, A.; Costa-Brito, A.R.; Vaz, C.; Marques, E.; Serra, N.; Lopes, V.P.; Vila-Chã, C. Exploring Perceived Barriers to Physical Activity among Older Adults Living in Low-Population Density Regions: Gender Differences and Associations with Activity Dimensions. Healthcare 2023, 11, 2948. [Google Scholar] [CrossRef] [PubMed]
- Moschny, A.; Platen, P.; Klaassen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to physical activity in older adults in Germany: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 121. [Google Scholar] [CrossRef]
- Kilgour, A.H.M.; Rutherford, M.; Higson, J.; Meredith, S.J.; McNiff, J.; Mitchell, S.; Wijayendran, A.; Lim, S.E.R.; Shenkin, S.D. Barriers and motivators to undertaking physical activity in adults over 70-a systematic review of the quantitative literature. Age Ageing 2024, 53, afae080. [Google Scholar] [CrossRef] [PubMed]
- Sedrak, M.S.; Freedman, R.A.; Cohen, H.J.; Muss, H.B.; Jatoi, A.; Klepin, H.D.; Wildes, T.M.; Le-Rademacher, J.G.; Kimmick, G.G.; Tew, W.P.; et al. Older adult participation in cancer clinical trials: A systematic review of barriers and interventions. CA Cancer J. Clin. 2021, 71, 78–92. [Google Scholar] [CrossRef] [PubMed]
- Agwara, E.; Martyn, K.; Macaninch, E.; Nyaga, W.; Buckner, L.; Lepre, B.; Laur, C.; Ray, S. Finding the place for nutrition in healthcare education and practice. BMJ Nutr. Prev. Health 2024, 7, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Cass, A.R.; Charlton, K.E. Prevalence of hospital-acquired malnutrition and modifiable determinants of nutritional deterioration during inpatient admissions: A systematic review of the evidence. J. Hum. Nutr. Diet. 2022, 35, 1043–1058. [Google Scholar] [CrossRef] [PubMed]
- Bross, R.; Genter, P.; Lu, Y.; Serpas, L.; Campa, D.; Ipp, E. Barriers to Healthy Eating and Diabetes Diet Education: Divergent Perspectives of Patients and Their Providers. Health Educ. Behav. 2022, 49, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Hurst, C.; Dismore, L.; Granic, A.; Tullo, E.; Noble, J.M.; Hillman, S.J.; Witham, M.D.; Sayer, A.A.; Dodds, R.M.; Robinson, S.M. Attitudes and barriers to resistance exercise training for older adults living with multiple long-term conditions, frailty, and a recent deterioration in health: Qualitative findings from the Lifestyle in Later Life—Older People’s Medicine (LiLL-OPM) study. BMC Geriatr. 2023, 23, 772. [Google Scholar] [CrossRef]
- Rosko, A.; Huang, Y.; Jones, D.; Presley, C.J.; Jaggers, J.; Owens, R.; Naughton, M.; Krok-Schoen, J.L. Feasibility of implementing an exercise intervention in older adults with hematologic malignancy. J. Geriatr. Oncol. 2022, 13, 234–240. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Schoufour, J.; Wang, D.D.; Dhana, K.; Pan, A.; Liu, X.; Song, M.; Liu, G.; Shin, H.J.; Sun, Q.; et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: Prospective cohort study. BMJ 2020, 368, l6669. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Better Noncommunicable Disease Outcomes: Challenges and Opportunities for Health Systems: Assessment Guide; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2014; Available online: https://iris.who.int/handle/10665/375006 (accessed on 18 July 2024).
- Vognar, L.; Mujahid, N. Healthcare transitions of older adults: An overview for the general practitioner. R. I. Med. J. 2014, 98, 15–18. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 32) | |
|---|---|
| Age (years), (mean ± SD) | 81.6 ± 9.3 |
| Sex, women (%) | 24 (75%) |
| Body mass index (kg/m2), (mean ± SD) | 24.2 ± 4.5 (women); 21.6 ± 3.3 (men) |
| Handgrip strength (kg), (mean ± SD) | 12.9 ± 4.2 (women); 22.7 (± 4.1) (men) |
| Fat-free mass index (kg/m2), (mean ± SD) | 12.9 ± 1.8 (women); 14.0 ± 2.0 (men) |
| Physical performance: | |
| Short Physical Performance Battery (/12), (mean ± SD) | 7.2 ± 2.9 |
| 4 m gait speed (m/s), (mean ± SD) | 0.7 ± 0.3 |
| Severe sarcopenia (n, %) | 26 (81.3%) |
| Malnutrition according to GLIM criteria (n, %) | 17 (63%) |
| Charlson comorbidity index, (mean ± SD) | 5 ± 2 |
| Barthel index (/100), (mean ± SD) | 91 ± 11 |
| Lawton index (/8), (mean ± SD) | 6 ± 2 |
| Quality of Life—SarQoL (/100), (mean ± SD) | |
| SarQoL D1: Physical and mental health | 63.9 ± 17.4 |
| SarQoL D2: Locomotion | 56.4 ± 21.0 |
| SarQoL D3: Body composition | 65.0 ± 20.0 |
| SarQoL D4: Functionality | 62.8 ± 19.4 |
| SarQoL D5: Activities of daily living | 48.1 ± 22.8 |
| SarQoL D6: Leisure activities | 31.2 ± 21.4 |
| SarQoL D7: Fears | 71.9 ± 24.2 |
| Overall QoL score | 57.1 ± 17.1 |
| Changes in Women after a 12-Week Intervention Based on an Intragroup Intention-to-Treat Analysis | ||||||
|---|---|---|---|---|---|---|
| Intervention Group (n = 14): | Control Group (n = 10): | |||||
| Baseline | 12-Week Follow-Up | p | Baseline | 12-Week Follow-Up | p | |
| Physical performance | ||||||
| SPPB—Balance test (/4) | 2.4 (SD 1.2) | 3.3 (SD 0.8) | 0.068 | 3.7 (SD 0.7) | 3.2 (SD 0.8) | 0.104 |
| SPPB—Gait speed test (/4) | 2.3 (SD 1.1) | 2.9 (SD 1.2) | 0.193 | 2.2 (SD 1.5) | 2.4 (SD 1.3) | 0.169 |
| SPPB—Chair stand test (/4) | 1.1 (SD 0.7) | 1.8 (SD 1.0) | 0.045 | 1.7 (SD 1.5) | 1.8 (SD 1.4) | 0.347 |
| Total SPPB (/12) | 5.9 (SD 2.6) | 8.0 (SD 2.3) | 0.025 | 7.6 (SD 3.3) | 7.4 (SD 3.4) | 0.681 |
| 4 m gait speed test (m/s) | 0.6 (SD 0.3) | 0.7 (SD 0.2) | 0.419 | 0.6 (SD 0.3) | 0.7 (SD 0.3) | 0.485 |
| Muscle strength | ||||||
| Handgrip (kg) | 12.4 (SD 4.0) | 16.1 (SD 3.9) | 0.042 | 14.8 (SD 3.8) | 15.8 (SD 4.0) | 0.012 |
| Intergroup Analysis of Changes in Primary Outcomes in Women after the 12-Week Intervention | ||||||
| Intervention Group (n = 14) | Control Group (n = 10) | Mean Difference (95%CI) | p | |||
| Physical performance | ||||||
| SPPB—Balance test (/4) | 0.9 (SD 1.4) | −0.4 (0.7) | 1.3 (0.3 to 2.4) | 0.018 | ||
| SPPB—Gait speed test (/4) | 0.6 (SD 1.3) | 0.2 (0.4) | 0.4 (0.4 to −0.6) | 0.42 | ||
| SPPB—Chair stand test (/4) | 0.7 (SD 0.9) | 0.1 (0.3) | 0.6 (−0.1 to 1.3) | 0.092 | ||
| Total SPPB (/12) | 2.1 (SD 2.5) | −0.1 (0.8) | 2.2 (0.4 to 4.0) | 0.021 | ||
| 4 m gait speed test (m/s) | 0.1 (SD 0.3) | 0.3 (0.8) | −0.2 (−0.7 to 0.3) | 0.409 | ||
| Muscle strength | ||||||
| Handgrip (kg) | 3.7 (SD 5.6) | 1.0 (0.9) | 2.8 (−0.8 to 6.4) | 0.119 | ||
| Components 1 | Questions to Be Considered | Expected Answer | Reported Answer | Actions to Address Potential Barriers 1 |
|---|---|---|---|---|
| Technology | Is the required equipment available? | Yes | Yes | - |
| Are staff properly trained to conduct the intervention? | Yes | Yes | - | |
| Economics | Are all the costs well defined? | Yes | Yes | - |
| Is the intervention expensive? | No | No | - | |
| Is the time cost acceptable? | Yes | Unknown | Transportation costs should be affordable for patients. | |
| Legal requirements | Does the intervention conflict with legal requirements? | No | No | - |
| Are the standards of good clinical practice followed? | Yes | Yes | - | |
| Operational needs | Is the intervention properly defined? | Yes | Yes | - |
| Do patients and relatives accept the intervention? | Yes | Unknown | Relatives must be involved in the rehabilitation process. | |
| Does patient enrollment represent a barrier to the accomplishment of the research objectives? | No | Yes | Educational strategies are needed to promote the importance and benefit of participating in research studies. | |
| Is a third party required to attend the intervention program? | No | Yes | The known benefits of exercise should be explained to the patients and their relatives. | |
| Are there any social limitations to the participation of older adults? | No | Yes | Additional support from professionals and relatives could be necessary. | |
| Are training costs assessed? | No | No | ||
| Scheduling | Given our current experience, is the intervention realistic in a post-hospitalization period? | Yes | Unknown | The patient should be informed about the need for timely treatment of sarcopenia. |
| Will the intervention result in meaningful benefits for patients? | Yes | Unknown | The benefits of HMB for the patient have been studied in a parallel research study. |
| Total Sample (n = 32) | |
|---|---|
| Tolerability, n (%) | |
| Permanent treatment discontinuation | 11 (34.4) |
| Treatment interruption: exercise | 6 (18.8) |
| Treatment interruption: supplementation | 4 (12.5) |
| Exercise dose modification | 6 (18.8) |
| Early termination | 9 (28.1) |
| Re-scheduling of missed sessions | 6 (18.8) |
| Lost to follow-up | 14 (43.8) |
| Attendance (number of attended sessions)/36, (mean ± SD) | 23 ± 12.0 |
| Nutritional compliance (number of sachets)/84, (mean ± SD) | 56 ± 32.6 |
| Safety (n, %) | |
| Adverse events | 21 (65.6) |
| Adverse reactions to resistance exercise | 7 (21.9) |
| Adverse reactions to nutritional supplementation | 0 |
| Unexpected adverse reactions | 0 |
| Serious adverse reactions | 0 |
| Type of Modification of Resistance Exercise | Explanation |
|---|---|
| Pain: Patient with osteoarthrosis of the shoulder and sequelae of right humerus fracture. |
| Weakness: Fatigue due to physical decline. |
| Pain associated with exercise. |
| Pain associated with exercise. |
| Weakness: upper limb lymphedema. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meza-Valderrama, D.; Sánchez-Rodríguez, D.; Peña, Y.C.; Ramírez-Fuentes, C.; Muñoz-Redondo, E.; Morgado-Pérez, A.; Ortíz-Agurto, N.; Finis-Gallardo, P.; Marco, E. Resistance Training and Nutritional Supplementation in Older Adults with Sarcopenia after Acute Disease: A Feasibility Study. Nutrients 2024, 16, 3053. https://doi.org/10.3390/nu16183053
Meza-Valderrama D, Sánchez-Rodríguez D, Peña YC, Ramírez-Fuentes C, Muñoz-Redondo E, Morgado-Pérez A, Ortíz-Agurto N, Finis-Gallardo P, Marco E. Resistance Training and Nutritional Supplementation in Older Adults with Sarcopenia after Acute Disease: A Feasibility Study. Nutrients. 2024; 16(18):3053. https://doi.org/10.3390/nu16183053
Chicago/Turabian StyleMeza-Valderrama, Delky, Dolores Sánchez-Rodríguez, Yulibeth Curbelo Peña, Cindry Ramírez-Fuentes, Elena Muñoz-Redondo, Andrea Morgado-Pérez, Norma Ortíz-Agurto, Paola Finis-Gallardo, and Ester Marco. 2024. "Resistance Training and Nutritional Supplementation in Older Adults with Sarcopenia after Acute Disease: A Feasibility Study" Nutrients 16, no. 18: 3053. https://doi.org/10.3390/nu16183053
APA StyleMeza-Valderrama, D., Sánchez-Rodríguez, D., Peña, Y. C., Ramírez-Fuentes, C., Muñoz-Redondo, E., Morgado-Pérez, A., Ortíz-Agurto, N., Finis-Gallardo, P., & Marco, E. (2024). Resistance Training and Nutritional Supplementation in Older Adults with Sarcopenia after Acute Disease: A Feasibility Study. Nutrients, 16(18), 3053. https://doi.org/10.3390/nu16183053