

Nutritional Management of Pediatric Gastrointestinal Motility Disorders


Abstract
1. Introduction
2. Materials and Methods
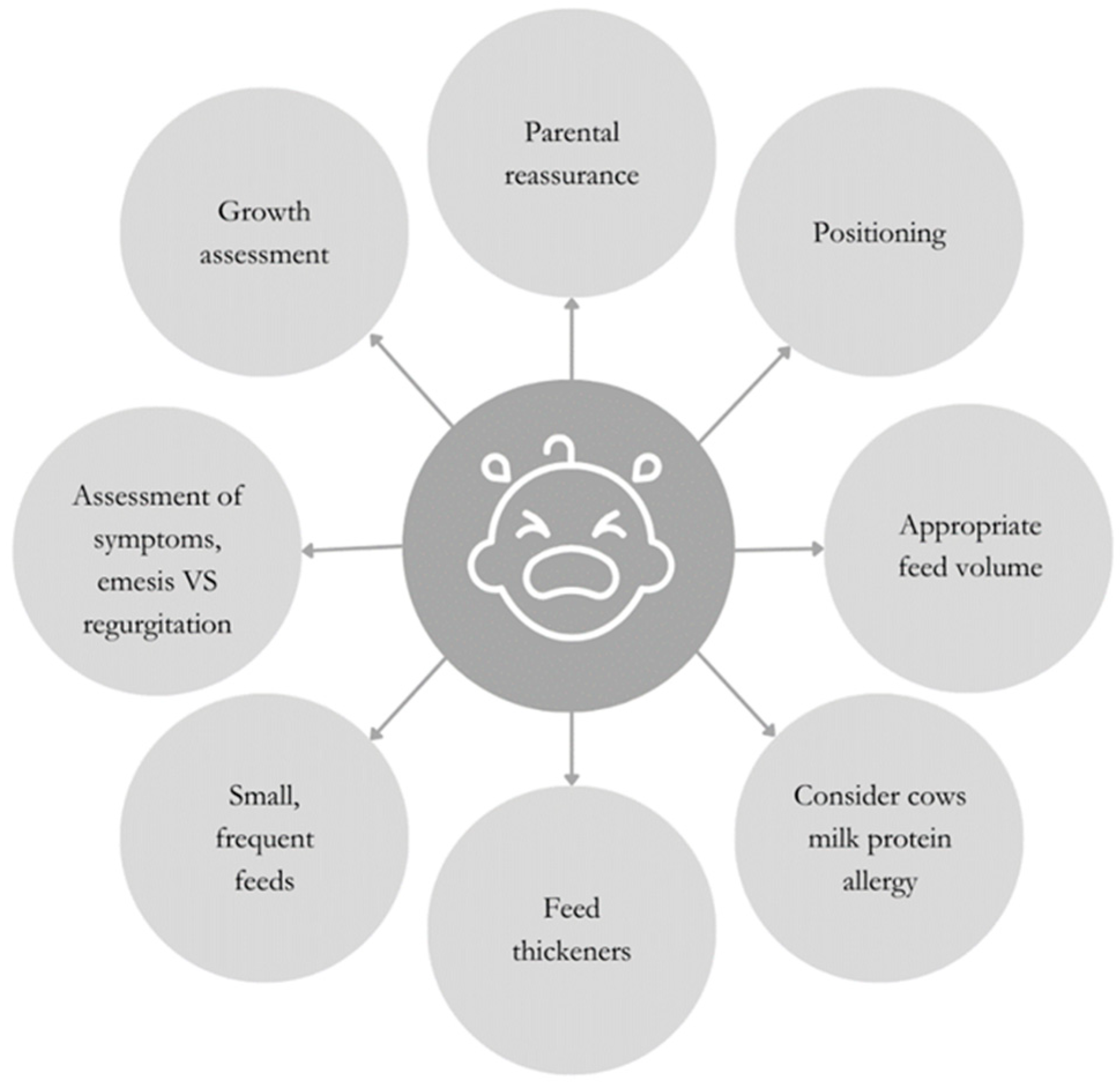
3. Gastroesophageal Reflux
4. Postural Modifications
5. Dietary Modification
5.1. Feeding Volume
5.2. Feed Thickeners
5.3. Cow’s Milk Protein Allergy
5.4. Feeding Difficulties
5.5. Children and Adolescents
6. Esophageal Atresia
6.1. Sham Feeding
6.2. Enteral Feeding
6.3. Oral Feeding
- Grating hard-texture fruit and vegetables such as carrot or apple;
- Cutting meat against the grain or opting for moist cuts of meat, such as dark chicken meat or minced meats;
- Avoiding certain foods that are tricky to manage, especially those with a “doughy” or “claggy” texture, such as white bread, rusks, and banana;
- Removing tough skins on foods such as sausages;
- Adding sauces or gravy to food to provide additional moisture to aid swallowing;
- Using energy-rich fluids such as milk, fruit juice, soup, gravy and sauces to puréed food, rather than water, helps to maintain the nutritional value of the food offered.
7. Achalasia
8. Gastroparesis
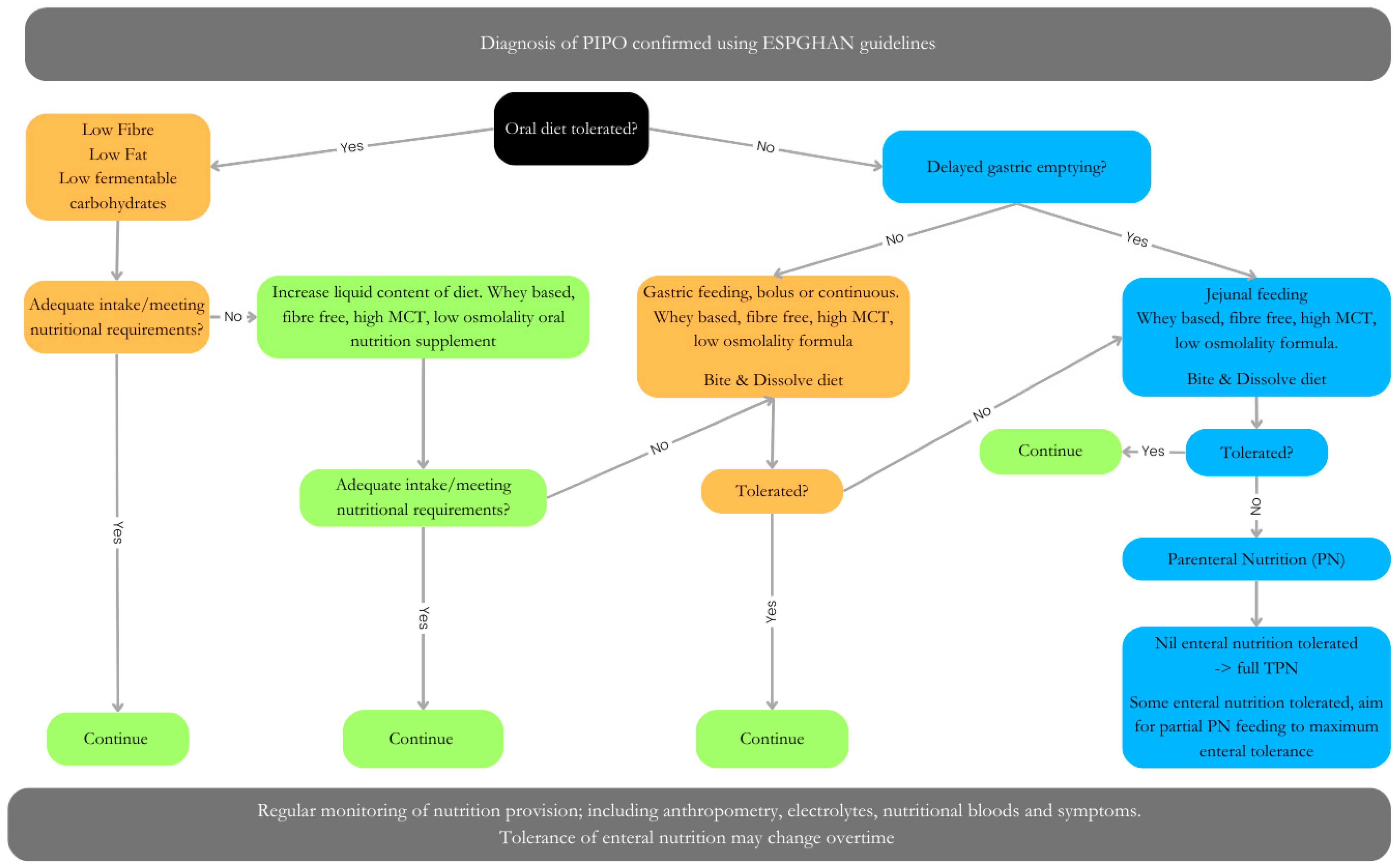
9. Pediatric Intestinal Pseudo-Obstructive Disorders
9.1. Fat
9.2. Fibers in PIPO
9.3. Carbohydrates
9.4. Protein
9.5. Micronutrients
9.6. Meal Composition
9.7. Enteral Tube Feeding
9.8. Parenteral Nutrition
10. Functional Constipation
- Onset of symptoms from birth or within the first few weeks of life;
- Delayed passage of meconium (>48 h after birth);
- Ribbon stools;
- Neurological involvement such as leg weakness;
- Abdominal distension with bilious vomiting;
- Bladder involvement.
10.1. Fibers in Constipation
10.2. Fluid
10.3. Probiotics
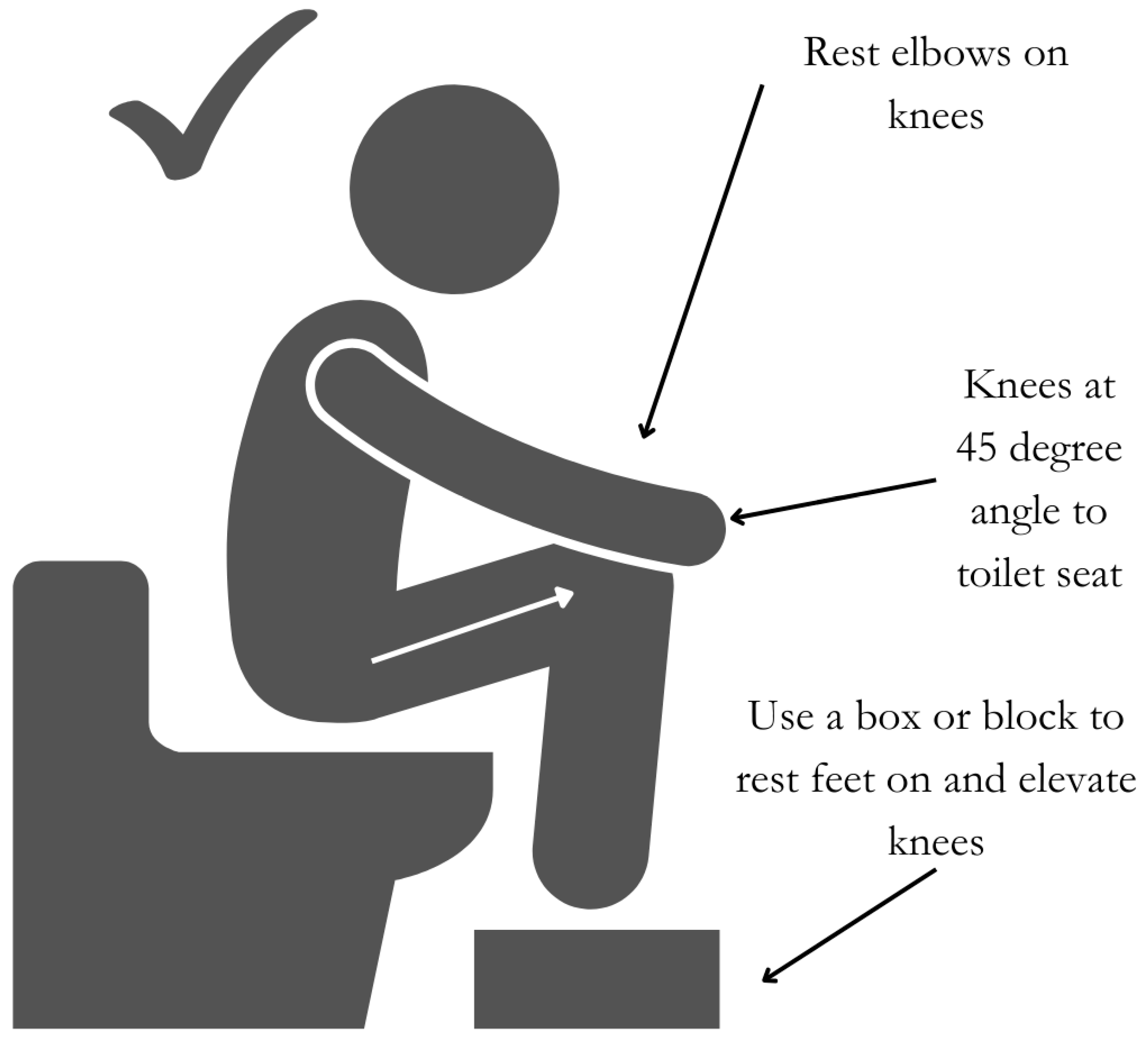
10.4. Posture
10.5. Physical Activity
10.6. Allergy
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lehmann, S.; Ferrie, S.; Carey, S. Nutrition Management in Patients with Chronic Gastrointestinal Motility Disorders: A Systematic Literature review. Nutr. Clin. Pract. 2019, 35, 219–230. [Google Scholar] [CrossRef]
- Rosen, R.; Vandenplas, Y.; Singendonk, M.; Cabana, M.; DiLorenzo, C.; Gottrand, F.; Gupta, S.; Langendam, M.; Staiano, A.; Thapar, N.; et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef] [PubMed]
- Friedman, C.; Sarantos, G.; Katz, S.; Geisler, S.M. Understanding gastroesophageal reflux disease in children. J. Am. Acad. Physician Assist. 2021, 34, 12–18. [Google Scholar] [CrossRef]
- Rybak, A.; Pesce, M.; Thapar, N.; Borrelli, O. Gastro-Esophageal reflux in children. Int. J. Mol. Sci. 2017, 18, 1671. [Google Scholar] [CrossRef] [PubMed]
- Omari, T.I.; Rommel, N.; Staunton, E.; Lontis, R.; Goodchild, L.; Haslam, R.R.; Dent, J.; Davidson, G.P. Paradoxical impact of body positioning on gastroesophageal reflux and gastric emptying in the premature neonate. J. Pediatr. 2004, 145, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Van Wijk, M.P.; Benninga, M.A.; Dent, J.; Lontis, R.; Goodchild, L.; McCall, L.M.; Haslam, R.; Davidson, G.P.; Omari, T. Effect of body position changes on postprandial gastroesophageal reflux and gastric emptying in the healthy premature neonate. J. Pediatr. 2007, 151, 585–590. [Google Scholar] [CrossRef]
- Corvaglia, L.; Rotatori, R.; Ferlini, M.; Aceti, A.; Ancora, G.; Faldella, G. The effect of body positioning on gastroesophageal reflux in premature infants: Evaluation by combined impedance and pH monitoring. J. Pediatr. 2007, 151, 591–596. [Google Scholar] [CrossRef]
- Ayerbe, J.I.G.; Hauser, B.; Salvatore, S.; Vandenplas, Y. Diagnosis and Management of Gastroesophageal Reflux Disease in Infants and Children: From Guidelines to Clinical Practice. Pediatr. Gastroenterol. Hepatol. Nutr. 2019, 22, 107–121. [Google Scholar] [CrossRef] [PubMed]
- NICE. Reflux in Babies|Information for the Public|Gastro-Oesophageal Reflux Disease in Children and Young People: Diagnosis and Management|Guidance|NICE. 14 January 2015. Available online: https://www.nice.org.uk/guidance/ng1/ifp/chapter/reflux-in-babies (accessed on 15 July 2024).
- Corvaglia, L.; Ferlini, M.; Rotatori, R.; Paoletti, V.; Alessandroni, R.; Cocchi, G.; Faldella, G. Starch thickening of human milk is ineffective in reducing the gastroesophageal reflux in preterm infants: A crossover study using intraluminal impedance. J. Pediatr. 2006, 148, 265–268. [Google Scholar] [CrossRef]
- Cavataio, F.; Iacono, G.; Montalto, G.; Soresi, M.; Tumminello, M.; Campagna, P.; Notarbartolo, A.; Carroccio, A. Gastroesophageal reflux associated with cow’s milk allergy in infants: Which diagnostic examinations are useful? Am. J. Gastroenterol. 1996, 91, 1215–1220. [Google Scholar]
- Schäppi, M.G.; Borrelli, O.; Knafelz, D.; Williams, S.; Smith, V.V.; Milla, P.J.; Lindley, K.J. Mast cell-nerve interactions in children with functional dyspepsia. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 472–480. [Google Scholar] [CrossRef]
- Meyer, R.; Vandenplas, Y.; Lozinsky, A.C.; Vieira, M.C.; Canani, R.B.; Dupont, C.; Uysal, P.; Cavkaytar, O.; Knibb, R.; Fleischer, D.M.; et al. Diagnosis and management of food allergy-associated gastroesophageal reflux disease in young children-EAACI position paper. Pediatr. Allergy Immunol. 2022, 33, e13856. [Google Scholar] [CrossRef]
- Hill, S.; Nurmatov, U.; DunnGalvin, A.; Reese, I.; Vieira, M.C.; Rommel, N.; Dupont, C.; Venter, C.; Cianferoni, A.; Walsh, J.; et al. Feeding difficulties in children with food allergies: An EAACI Task Force Report. Pediatr. Allergy Immunol. 2024, 35, e14119. [Google Scholar] [CrossRef] [PubMed]
- Grossbauer, A.; Mnatsakanian, A.; Costeloe, A.; Thottam, P.J. The effects of untreated reflux on the incidence of dysphagia, oral aversion, and feeding difficulty in the NICU population. Int. J. Pediatr. Otorhinolaryngol. 2023, 174, 111734. [Google Scholar] [CrossRef] [PubMed]
- Newberry, C.; Lynch, K. The role of diet in the development and management of gastroesophageal reflux disease: Why we feel the burn. J. Thorac. Dis. 2019, 11, 1594–1601. [Google Scholar] [CrossRef]
- Traini, I.; Menzies, J.; Hughes, J.; Leach, S.T.; Krishnan, U. Oesophageal atresia: The growth gap. World J. Gastroenterol. 2020, 26, 1262–1272. [Google Scholar] [CrossRef]
- Krishnan, U. Eosinophilic Esophagitis in Esophageal Atresia. Front. Pediatr. 2019, 7, 497. [Google Scholar] [CrossRef] [PubMed]
- Svoboda, E.; Fruithof, J.; Widenmann-Grolig, A.; Slater, G.; Armand, F.; Warner, B.; Eaton, S.; De Coppi, P.; Hannon, E. A patient led, international study of long term outcomes of esophageal atresia: EAT 1. J. Pediatr. Surg. 2018, 53, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Puntis, J.W.; Ritson, D.G.; Holden, C.E.; Buick, R.G. Growth and feeding problems after repair of oesophageal atresia. Arch. Dis. Child. 1990, 65, 84–88. [Google Scholar] [CrossRef]
- Mahoney, L.; Rosen, R. Feeding Problems and Their Underlying Mechanisms in the Esophageal Atresia-Tracheoesophageal Fistula Patient. Front. Pediatr. 2017, 5, 127. [Google Scholar] [CrossRef]
- Hollis, J.L.; Crozier, S.R.; Inskip, H.M.; Cooper, C.; Godfrey, K.M.; Robinson, S.M.; Southampton Women’s Survey Study Group. Age at introduction of solid foods and feeding difficulties in childhood: Findings from the Southampton Women’s Survey. Br. J. Nutr. 2016, 116, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, U.; Mousa, H.; Dall’Oglio, L.; Homaira, N.; Rosen, R.; Faure, C.; Gottrand, F. ESPGHAN-NASPGHAN Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children with Esophageal Atresia-Tracheoesophageal Fistula. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 550–570. [Google Scholar] [CrossRef] [PubMed]
- Holschneider, P.; Dübbers, M.; Engelskirchen, R.; Trompelt, J.; Holschneider, A. Results of the operative treatment of gastroesophageal reflux in childhood with particular focus on patients with esophageal atresia. Eur. J. Pediatr. Surg. 2007, 17, 163–175. [Google Scholar] [CrossRef]
- Tucker, A.; Huang, E.Y.; Peredo, J.; Weems, M.F. Pilot Study of Sham Feeding in Postoperative Neonates. Am. J. Perinatol. 2022, 39, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Tollne, A.; Nilsson, T.; Svensson, J.F.; Almström, M.; Öst, E. Parents’ experiences of sham feeding their child with esophageal atresia at home while awaiting reconstructive surgery. A qualitative interview study. Pediatr. Surg. Int. 2024, 40, 61. [Google Scholar] [CrossRef]
- Menzies, J.; Hughes, J.; Leach, S.; Belessis, Y.; Krishnan, U. Prevalence of Malnutrition and Feeding Difficulties in Children with Esophageal Atresia. J. Pediatr. Gastroenterol. Nutr. 2017, 64, e100–e105. [Google Scholar] [CrossRef]
- Stewart, A.; Smith, C.H.; Govender, R.; Eaton, S.; De Coppi, P.; Wray, J. Parents’ experiences of feeding children born with oesophageal atresia/tracheo-oesophageal fistula. J. Pediatr. Surg. 2022, 57, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.; Govender, R.; Eaton, S.; Smith, C.H.; De Coppi, P.; Wray, J. The characteristics of eating, drinking and oro-pharyngeal swallowing difficulties associated with repaired oesophageal atresia/tracheo-oesophageal fistula: A systematic review and meta-proportional analysis. Orphanet J. Rare Dis. 2024, 19, 253. [Google Scholar] [CrossRef]
- Gatzinsky, V.; Jönsson, L.; Johansson, C.; Göthberg, G.; Sillén, U.; Friberg, L.G. Dysphagia in adults operated on for esophageal atresia–use of a symptom score to evaluate correlated factors. Eur. J. Pediatr. Surg. 2011, 21, 94–98. [Google Scholar] [CrossRef]
- Maybee, J.; Deck, J.; Jensen, E.; Ruiz, A.; Kinder, S.; DeBoer, E. Feeding and Swallowing Characteristics of Children with Esophageal Atresia and Tracheoesophageal Fistula. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 288–294. [Google Scholar] [CrossRef]
- van Lennep, M.; Gottrand, F.; Faure, C.; Omari, T.I.; Benninga, M.A.; van Wijk, M.P.; Krishnan, U. Management of Gastroesophageal Reflux Disease in Esophageal Atresia Patients: A Cross-Sectional Survey amongst International Clinicians. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Vaezi, M.F.; Pandolfino, J.E.; Yadlapati, R.H.; Greer, K.B.; Kavitt, R.T. ACG Clinical Guidelines: Diagnosis and Management of Achalasia. Am. J. Gastroenterol. 2020, 115, 1393–1411. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, R.O.; Zaninotto, G.; Roman, S.; Boeckxstaens, G.; Fockens, P.; Langendam, M.; Plumb, A.; Smout, A.; Targarona, E.; Trukhmanov, A.; et al. European guidelines on achalasia: United European Gastroenterology and European Society of Neurogastroenterology and Motility recommendations. United Eur. Gastroenterol. J. 2020, 8, 13–33. [Google Scholar] [CrossRef] [PubMed]
- Nurko, S. Motility Disorders in Children. Pediatr. Clin. N. Am. 2017, 64, 593–612. [Google Scholar] [CrossRef] [PubMed]
- Jarzębicka, D.; Czubkowski, P.; Sieczkowska-Gołub, J.; Kierkuś, J.; Kowalski, A.; Stefanowicz, M.; Oracz, G. Achalasia in Children-Clinical Presentation, Diagnosis, Long-Term Treatment Outcomes, and Quality of Life. J. Clin. Med. 2021, 10, 3917. [Google Scholar] [CrossRef]
- Mohammed, S.H.; Hegedüs, V. Dislodgement of impacted oesophageal foreign bodies with carbonated beverages. Clin. Radiol. 1986, 37, 589–592. [Google Scholar] [CrossRef]
- Karanjia, N.D.; Rees, M. The use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture. Ann. R. Coll. Surg. Engl. 1993, 75, 94–95. [Google Scholar]
- Koumi, A.; Panos, M.Z. Oesophageal food impaction in achalasia treated with Coca-Cola and nifedipine. Case Rep. 2010, 2010, bcr0520091891. [Google Scholar] [CrossRef]
- Krasaelap, A.; Kovacic, K.; Goday, P.S. Nutrition Management in Pediatric Gastrointestinal Motility Disorders. Nutr. Clin. Pract. 2020, 35, 265–272. [Google Scholar] [CrossRef]
- Schol, J.; Wauters, L.; Dickman, R.; Drug, V.; Mulak, A.; Serra, J.; Enck, P.; Tack, J.; ESNM Gastroparesis Consensus Group. United European Gastroenterology (UEG) and European Society for Neurogastroenterology and Motility (ESNM) consensus on gastroparesis. Neurogastroenterol. Motil. 2021, 33, e14237. [Google Scholar] [CrossRef]
- Bharadwaj, S.; Meka, K.; Tandon, P.; Rathur, A.; Rivas, J.M.; Vallabh, H.; Jevenn, A.; Guirguis, J.; Sunesara, I.; Nischnick, A.; et al. Management of gastroparesis-associated malnutrition. J. Dig. Dis. 2016, 17, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, A.; Malagelada, C.; Serra, J. Nutritional challenges in patients with gastroparesis. Curr. Opin. Clin. Nutr. Metab. Care 2022, 25, 360–363. [Google Scholar] [CrossRef]
- Eseonu, D.; Su, T.; Lee, K.; Chumpitazi, B.P.; Shulman, R.J.; Hernaez, R. Dietary Interventions for Gastroparesis: A Systematic Review. Adv. Nutr. 2022, 13, 1715–1724. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.S.; Mogensen, K.M. Recommending Small, Frequent Meals in the Clinical Care of Adults: A Review of the Evidence and Important Considerations. Nutr. Clin. Pract. 2017, 32, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Limketkai, B.N.; LeBrett, W.; Lin, L.; Shah, N.D. Nutritional approaches for gastroparesis. Lancet Gastroenterol. Hepatol. 2020, 5, 1017–1026. [Google Scholar] [CrossRef]
- Pescarin, M.; Day, H.; Thapar, N.; Jackman, L.; Saliakellis, E.; Lindley, K.J.; Nikaki, K.; Hill, S.; Köglmeier, J.; Rybak, A.; et al. Optimizing nutrition in pediatric intestinal pseudo-obstruction syndrome. Neurogastroenterol. Motil. 2023, 35, e14562. [Google Scholar] [CrossRef] [PubMed]
- Schwankovsky, L.; Mousa, H.; Rowhani, A.; Di Lorenzo, C.; Hyman, P.E. Quality of life outcomes in congenital chronic intestinal pseudo-obstruction. Dig. Dis. Sci. 2002, 47, 1965–1968. [Google Scholar] [CrossRef] [PubMed]
- Hyman, P.; Thapar, N. Gastrointestinal motility and functional disorders in children. In Pediatric Neurogastroenterology; Faure, C., Thapar, N., Di Lorenzo, C., Eds.; Springer Inc.: Berlin/Heidelberg, Germany, 2013; pp. 257–270. [Google Scholar]
- Thapar, N.; Saliakellis, E.; Benninga, M.A.; Borrelli, O.; Curry, J.; Faure, C.; De Giorgio, R.; Gupte, G.; Knowles, C.H.; Staiano, A.; et al. Paediatric Intestinal Pseudo-obstruction: Evidence and Consensus-based Recommendations From an ESPGHAN-Led Expert Group. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 991–1019. [Google Scholar] [CrossRef]
- Pakarinen, M.P.; Kurvinen, A.; Koivusalo, A.I.; Ruuska, T.; Mäkisalo, H.; Jalanko, H.; Rintala, R.J. Surgical treatment and outcomes of severe pediatric intestinal motility disorders requiring parenteral nutrition. J. Pediatr. Surg. 2013, 48, 333–338. [Google Scholar] [CrossRef]
- Siegel, M.; Krantz, B.; Lebenthal, E. Effect of fat and carbohydrate composition on the gastric emptying of isocaloric feedings in premature infants. Gastroenterology 1985, 89, 785–790. [Google Scholar] [CrossRef]
- Wanders, A.J.; Jonathan, M.C.; Borne, J.J.G.C.v.D.; Mars, M.; Schols, H.A.; Feskens, E.J.M.; de Graaf, C. The effects of bulking, viscous and gel-forming dietary fibres on satiation. Br. J. Nutr. 2013, 109, 1330–1337. [Google Scholar] [CrossRef]
- Thondre, P.S.; Shafat, A.; Clegg, M.E. Molecular weight of barley β-glucan influences energy expenditure, gastric emptying and glycaemic response in human subjects. Br. J. Nutr. 2013, 110, 2173–2179. [Google Scholar] [CrossRef] [PubMed]
- Fabregat, M.I.P.; Gardner, R.M.; Hassan, M.A.; Kapphahn, K.; Yeh, A.M. Small Intestinal Bacterial Overgrowth in Children: Clinical Features and Treatment Response. JPGN Rep. 2022, 3, e185. [Google Scholar] [CrossRef]
- Schreiner, R.L.; Brady, M.S.; Ernst, J.A.; Lemons, J.A. Lack of lactobezoars in infants given predominantly whey protein formulas. Am. J. Dis. Child. 1982, 136, 437–439. [Google Scholar] [CrossRef]
- Tang, P.; Lu, L.; Yan, W.; Tao, Y.; Feng, H.; Cai, W.; Wang, Y. Long-term follow-up for pediatric intestinal pseudo-obstruction patients in China. Nutr. Clin. Pract. 2023, 38, 648–656. [Google Scholar] [CrossRef]
- Homko, C.J.; Duffy, F.; Friedenberg, F.K.; Boden, G.; Parkman, H.P. Effect of dietary fat and food consistency on gastroparesis symptoms in patients with gastroparesis. Neurogastroenterol. Motil. 2015, 27, 501–508. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Flores, A.F.; Buie, T.; Hyman, P.E. Intestinal motility and jejunal feeding in children with chronic intestinal pseudo-obstruction. Gastroenterology 1995, 108, 1379–1385. [Google Scholar] [CrossRef]
- Mihatsch, W.A.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Desci, T.; Domellöf, M.; Embleton, N.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition. Clin. Nutr. 2018, 37, 2303–2305. [Google Scholar] [CrossRef]
- Domellöf, M.; Szitanyi, P.; Simchowitz, V.; Franz, A.; Mimouni, F. ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Iron and trace minerals. Clin. Nutr. 2018, 37, 2354–2359. [Google Scholar] [CrossRef]
- Hartman, C.; Shamir, R.; Simchowitz, V.; Lohner, S.; Cai, W.; Decsi, T.; Braegger, C.; Bronsky, J.; Campoy, C.; Carnielli, V.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Complications. Clin. Nutr. 2018, 37, 2418–2429. [Google Scholar] [CrossRef]
- Hill, S.; Ksiazyk, J.; Prell, C.; Tabbers, M.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Home parenteral nutrition. Clin. Nutr. 2018, 37, 2401–2408. [Google Scholar] [CrossRef]
- Jochum, F.; Moltu, S.J.; Senterre, T.; Nomayo, A.; Goulet, O.; Iacobelli, S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Fluid and electrolytes. Clin. Nutr. 2018, 37, 2344–2353. [Google Scholar] [CrossRef]
- Joosten, K.; Embleton, N.; Yan, W.; Senterre, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Energy. Clin. Nutr. 2018, 37, 2309–2314. [Google Scholar] [CrossRef]
- Kolaček, S.; Puntis, J.W.L.; Hojsak, I.; ESPGHAN/ESPEN/ESPR/CSPEN Working Group on Pediatric Parenteral Nutrition; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Venous access. Clin. Nutr. 2018, 37, 2379–2391. [Google Scholar] [CrossRef] [PubMed]
- Lapillonne, A.; Mis, N.F.; Goulet, O.; van den Akker, C.H.; Wu, J.; Koletzko, B.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Lipids. Clin. Nutr. 2018, 37, 2324–2336. [Google Scholar] [CrossRef]
- Mesotten, D.; Joosten, K.; van Kempen, A.; Verbruggen, S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Carbohydrates. Clin. Nutr. 2018, 37, 2337–2343. [Google Scholar] [CrossRef] [PubMed]
- Mihatsch, W.; Fewtrell, M.; Goulet, O.; Molgaard, C.; Picaud, J.C.; Senterre, T.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Calcium, phosphorus and magnesium. Clin. Nutr. 2018, 37, 2360–2365. [Google Scholar] [CrossRef] [PubMed]
- Puntis, J.W.; Hojsak, I.; Ksiazyk, J.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Organisational aspects. Clin. Nutr. 2018, 37, 2392–2400. [Google Scholar] [CrossRef]
- Riskin, A.; Picaud, J.C.; Shamir, R.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Standard versus individualized parenteral nutrition. Clin. Nutr. 2018, 37, 2409–2417. [Google Scholar] [CrossRef]
- Van Goudoever, J.B.; Carnielli, V.; Darmaun, D.; de Pipaon, M.S.; Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Decsi, T.; Domellöf, M.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Amino acids. Clin. Nutr. 2018, 37, 2315–2323. [Google Scholar] [CrossRef]
- Lambe, C.; Talbotec, C.; Kapel, N.; Barbot-Trystram, L.; Brabant, S.; Nader, E.A.; Pigneur, B.; Payen, E.; Goulet, O. Long-term treatment with teduglutide: A 48-week open-label single-center clinical trial in children with short bowel syndrome. Am. J. Clin. Nutr. 2023, 117, 1152–1163. [Google Scholar] [CrossRef] [PubMed]
- Zeevenhooven, J.; Koppen, I.J.N.; Benninga, M.A. The New Rome IV Criteria for Functional Gastrointestinal Disorders in Infants and Toddlers. Pediatr. Gastroenterol. Hepatol. Nutr. 2017, 20, 1–13. [Google Scholar] [CrossRef]
- Vriesman, M.H.; Koppen, I.J.N.; Camilleri, M.; Di Lorenzo, C.; Benninga, M.A. Management of functional constipation in children and adults. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Steurbaut, L.; Levy, E.I.; De Geyter, C.; Buyse, S.; Vandenplas, Y. A narrative review on the diagnosis and management of constipation in infants. Expert Rev. Gastroenterol. Hepatol. 2023, 17, 769–783. [Google Scholar] [CrossRef]
- Bae, S.H. Diets for constipation. Pediatr. Gastroenterol. Hepatol. Nutr. 2014, 17, 203–208. [Google Scholar] [CrossRef] [PubMed]
- van Mill, M.J.; Koppen, I.J.N.; Benninga, M.A. Controversies in the Management of Functional Constipation in Children. Curr. Gastroenterol. Rep. 2019, 21, 23. [Google Scholar] [CrossRef]
- Axelrod, C.H.; Saps, M. The Role of Fiber in the Treatment of Functional Gastrointestinal Disorders in Children. Nutrients 2018, 10, 1650. [Google Scholar] [CrossRef]
- de Mello, P.P.; Eifer, D.A.; de Mello, E.D. Use of fibers in childhood constipation treatment: Systematic review with meta-analysis. J. Pediatr. (Rio J.) 2018, 94, 460–470. [Google Scholar] [CrossRef]
- Wegh, C.A.; Baaleman, D.F.; Tabbers, M.M.; Smidt, H.; Benninga, M.A. Nonpharmacologic Treatment for Children with Functional Constipation: A Systematic Review and Meta-analysis. J. Pediatr. 2022, 240, 136–149.e5. [Google Scholar] [CrossRef]
- Tabbers, M.M.; Di Lorenzo, C.; Berger, M.Y.; Faure, C.; Langendam, M.W.; Nurko, S.; Staiano, A.; Vandenplas, Y.; Benninga, M.A. Evaluation and treatment of functional constipation in infants and children: Evidence-based recommendations from ESPGHAN and NASPGHAN. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 258–274. [Google Scholar] [CrossRef]
- Gill, S.K.; Rossi, M.; Bajka, B.; Whelan, K. Dietary fibre in gastrointestinal health and disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 101–116. [Google Scholar] [CrossRef]
- Gearry, R.; Fukudo, S.; Barbara, G.; Kuhn-Sherlock, B.; Ansell, J.; Blatchford, P.; Eady, S.; Wallace, A.; Butts, C.; Cremon, C.; et al. Consumption of 2 green kiwifruits daily improves constipation and abdominal comfort—Results of an international multicenter randomized controlled trial. Am. J. Gastroenterol. 2022, 118, 1058–1068. [Google Scholar] [CrossRef]
- Wilkinson-Smith, V.; Dellschaft, N.; Ansell, J.; Hoad, C.; Marciani, L.; Gowland, P.; Spiller, R. Mechanisms underlying effects of kiwifruit on intestinal function shown by MRI in Healthy Volunteers. Aliment. Pharmacol. Ther. 2019, 49, 759–768. [Google Scholar] [CrossRef]
- Tran, D.L.; Sintusek, P. Functional constipation in children: What physicians should know. World J. Gastroenterol. 2023, 29, 1261–1288. [Google Scholar] [CrossRef]
- Constipation in Children and Young People: Diagnosis and Management. In NICE Guideline CG99 [Internet]; National Institute for Health and Care Excellence (NICE): London, UK, 2010. [PubMed]
- de Meij, T.G.; de Groot, E.F.; Eck, A.; Budding, A.E.; Kneepkens, C.F.; Benninga, M.A.; van Bodegraven, A.A.; Savelkoul, P.H. Characterization of Microbiota in Children with Chronic Functional Constipation. PLoS ONE 2016, 11, e0164731. [Google Scholar] [CrossRef]
- Wallace, C.; Sinopoulou, V.; Gordon, M.; Akobeng, A.K.; Llanos-Chea, A.; Hungria, G.; Febo-Rodriguez, L.; Fifi, A.; Valdes, L.F.; Langshaw, A.; et al. Probiotics for treatment of chronic constipation in children. Cochrane Database Syst. Rev. 2022, 3, CD014257. [Google Scholar]
- Seidenfaden, S.; Ormarsson, O.T.; Lund, S.H.; Bjornsson, E.S. Physical activity may decrease the likelihood of children developing constipation. Acta Paediatr. 2018, 107, 151–155. [Google Scholar] [CrossRef]
- Harrington, K.L.; Haskvitz, E.M. Managing a patient’s constipation with physical therapy. Phys. Ther. 2006, 86, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R.; Vandenplas, Y.; Lozinsky, A.C.; Vieira, M.C.; Berni Canani, R.; du Toit, G.; Dupont, C.; Giovannini, M.; Uysal, P.; Cavkaytar, O.; et al. Diagnosis and management of food allergy-induced constipation in young children-An EAACI position paper. Pediatr. Allergy Immunol. 2024, 35, e14163. [Google Scholar] [CrossRef] [PubMed]
- Miceli Sopo, S.; Arena, R.; Greco, M.; Bergamini, M.; Monaco, S. Constipation and cow’s milk allergy: A review of the literature. Int. Arch. Allergy Immunol. 2014, 164, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Iacono, G.; Bonventre, S.; Scalici, C.; Maresi, E.; Di Prima, L.; Soresi, M.; Di Ges, G.; Noto, D.; Carroccio, A. Food intolerance and chronic constipation: Manometry and histology study. Eur. J. Gastroenterol. Hepatol. 2006, 18, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Iacono, G. Review article: Chronic constipation and food hypersensitivity—An intriguing relationship. Aliment. Pharmacol. Ther. 2006, 24, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, O.; Barbara, G.; Di Nardo, G.; Cremon, C.; Lucarelli, S.; Frediani, T.; Paganelli, M.; De Giorgio, R.; Stanghellini, V.; Cucchiara, S. Neuroimmune interaction and anorectal motility in children with food allergy-related chronic constipation. Am. J. Gastroenterol. 2009, 104, 454–463. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptoms | Functional Constipation | Infant Dyschezia |
|---|---|---|
| Behavior before passing stool | Distress on stooling/straining Bleeding associated with hard stool | Straining/crying/turning red in the face with effort |
| Type of stool passed | Hard large stool Rabbit droppings BSC * Type 1–3 | Soft stool |
| Frequency of stooling | Fewer than three complete stools per week | Usually daily (eventually) |
| Onset of symptoms | First few weeks of life (not from birth) | First few months of life |
| Treatment | Dietary interventions Osmotic laxative treatment | Resolves spontaneously within a few weeks |
| Age | Total Fluid per Day (mL) |
|---|---|
| 0–6 months | 700 (breastmilk/formula milk) |
| 7–12 months | 800 (milk and complementary foods and beverages) |
| 1–3 years | 1300 |
| 4–8 years | 1700 |
| Boys: 9–13 years | 2400 |
| Girls: 9–13 years | 2100 |
| Boys: 14–18 years | 3300 |
| Girls: 14–18 years | 2300 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackman, L.; Arpe, L.; Thapar, N.; Rybak, A.; Borrelli, O. Nutritional Management of Pediatric Gastrointestinal Motility Disorders. Nutrients 2024, 16, 2955. https://doi.org/10.3390/nu16172955
Jackman L, Arpe L, Thapar N, Rybak A, Borrelli O. Nutritional Management of Pediatric Gastrointestinal Motility Disorders. Nutrients. 2024; 16(17):2955. https://doi.org/10.3390/nu16172955
Chicago/Turabian StyleJackman, Lucy, Lauren Arpe, Nikhil Thapar, Anna Rybak, and Osvaldo Borrelli. 2024. "Nutritional Management of Pediatric Gastrointestinal Motility Disorders" Nutrients 16, no. 17: 2955. https://doi.org/10.3390/nu16172955
APA StyleJackman, L., Arpe, L., Thapar, N., Rybak, A., & Borrelli, O. (2024). Nutritional Management of Pediatric Gastrointestinal Motility Disorders. Nutrients, 16(17), 2955. https://doi.org/10.3390/nu16172955