
Compliance with a Healthful Plant-Based Diet Is Associated with Kidney Function in Patients with Autosomal Dominant Polycystic Kidney Disease
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
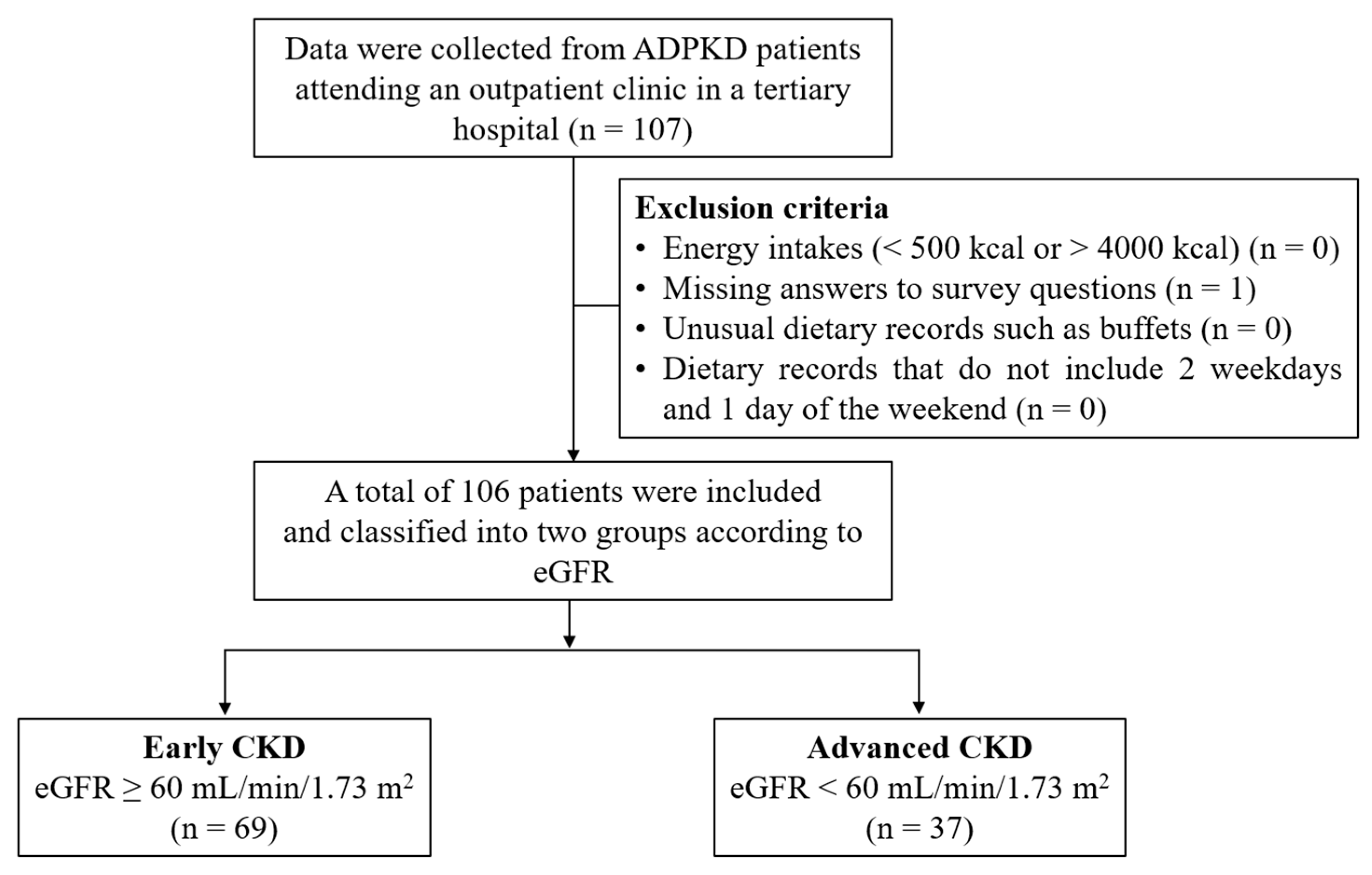
2.1. Study Participants
2.2. Clinical Variables
2.3. Dietary Assessment and PDIs
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Study Participants by eGFR
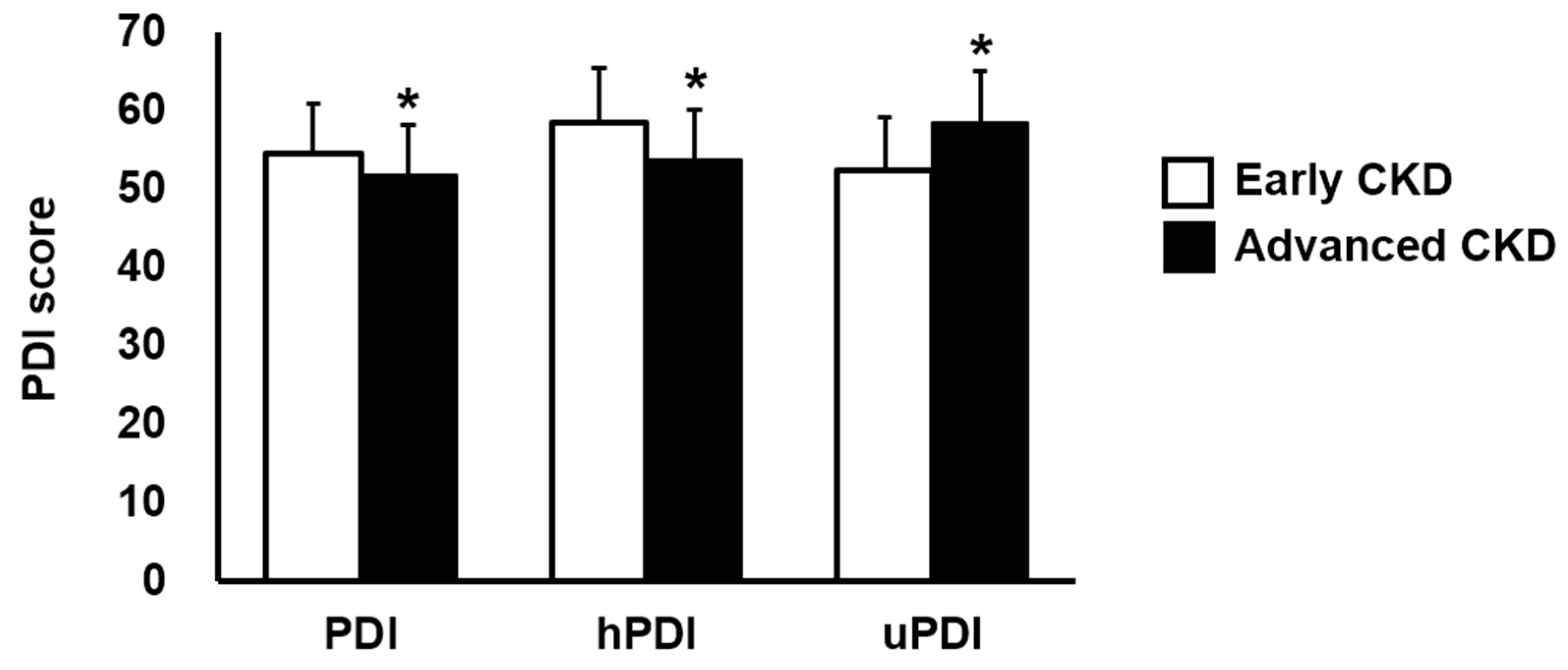
3.2. PDIs According to the eGFR and the Correlation between PDIs and Kidney Function
3.3. Associations between PDIs and Kidney Function
3.4. Dietary Intakes of Study Participants According to the Median Values of PDIs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nobakht, N.; Hanna, R.M.; Al-Baghdadi, M.; Ameen, K.M.; Arman, F.; Nobahkt, E.; Kamgar, M.; Rastogi, A. Advances in Autosomal Dominant Polycystic Kidney Disease: A Clinical Review. Kidney Med. 2020, 2, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Willey, C.J.; Blais, J.D.; Hall, A.K.; Krasa, H.B.; Makin, A.J.; Czerwiec, F.S. Prevalence of autosomal dominant polycystic kidney disease in the European Union. Nephrol. Dial. Transplant. 2017, 32, 1356–1363. [Google Scholar] [CrossRef] [PubMed]
- Lanktree, M.B.; Haghighi, A.; Guiard, E.; Iliuta, I.A.; Song, X.; Harris, P.C.; Paterson, A.D.; Pei, Y. Prevalence Estimates of Polycystic Kidney and Liver Disease by Population Sequencing. J. Am. Soc. Nephrol. 2018, 29, 2593–2600. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Torres, V.E. Autosomal Dominant Polycystic Kidney Disease: Core Curriculum 2016. Am. J. Kidney Dis. 2016, 67, 792–810. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Zhou, X.; Garbinsky, D.; Davenport, E.; Nunna, S.; Oberdhan, D.; Fernandes, A. Tolvaptan and Kidney Function Decline in Older Individuals with Autosomal Dominant Polycystic Kidney Disease: A Pooled Analysis of Randomized Clinical Trials and Observational Studies. Kidney Med. 2023, 5, 100639. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.B.; Devuyst, O.; Eckardt, K.U.; Gansevoort, R.T.; Harris, T.; Horie, S.; Kasiske, B.L.; Odland, D.; Pei, Y.; Perrone, R.D.; et al. Autosomal-dominant polycystic kidney disease (ADPKD): Executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2015, 88, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Pickel, L.; Iliuta, I.A.; Scholey, J.; Pei, Y.; Sung, H.K. Dietary Interventions in Autosomal Dominant Polycystic Kidney Disease. Adv. Nutr. 2022, 13, 652–666. [Google Scholar] [CrossRef]
- Capelli, I.; Lerario, S.; Aiello, V.; Provenzano, M.; Di Costanzo, R.; Squadrani, A.; Vella, A.; Vicennati, V.; Poli, C.; La Manna, G.; et al. Diet and Physical Activity in Adult Dominant Polycystic Kidney Disease: A Review of the Literature. Nutrients 2023, 15, 2621. [Google Scholar] [CrossRef]
- Hemler, E.C.; Hu, F.B. Plant-Based Diets for Personal, Population, and Planetary Health. Adv. Nutr. 2019, 10, S275–S283. [Google Scholar] [CrossRef]
- Satija, A.; Hu, F.B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 2018, 28, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.S.; Candussi, C.J.; Tresserra-Rimbau, A.; Jennings, A.; Bondonno, N.P.; Hill, C.; Sowah, S.A.; Cassidy, A.; Kühn, T. A healthful plant-based diet is associated with lower type 2 diabetes risk via improved metabolic state and organ function: A prospective cohort study. Diabetes Metab. 2023, 50, 101499. [Google Scholar] [CrossRef]
- Samtiya, M.; Aluko, R.E.; Dhewa, T.; Moreno-Rojas, J.M. Potential Health Benefits of Plant Food-Derived Bioactive Components: An Overview. Foods 2021, 10, 839. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Grams, M.E.; Coresh, J.; Rebholz, C.M. Plant-Based Diets and Incident CKD and Kidney Function. Clin. J. Am. Soc. Nephrol. 2019, 14, 682–691. [Google Scholar] [CrossRef]
- Carrero, J.J.; González-Ortiz, A.; Avesani, C.M.; Bakker, S.J.; Bellizzi, V.; Chauveau, P.; Clase, C.M.; Cupisti, A.; Espinosa-Cuevas, A.; Molina, P.; et al. Plant-based diets to manage the risks and complications of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 525–542. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro III, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef] [PubMed]
- Moloudpour, B.; Jam, S.A.; Darbandi, M.; Janati, A.; Gholizadeh, M.; Najafi, F.; Pasdar, Y. Association Between Plant-based Diet and Kidney Function in Adults. J. Ren. Nutr. 2024, 34, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Heo, G.Y.; Koh, H.B.; Kim, H.J.; Kim, K.W.; Jung, C.Y.; Kim, H.W.; Chang, T.I.; Park, J.T.; Yoo, T.H.; Kang, S.W.; et al. Association of Plant Protein Intake with Risk of Incident CKD: A UK Biobank Study. Am. J. Kidney Dis. 2023, 82, 687–697.e1. [Google Scholar] [CrossRef]
- Li, P.; Xia, C.; Liu, P.; Peng, Z.; Huang, H.; Wu, J.; He, Z. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in evaluation of inflammation in non-dialysis patients with end-stage renal disease (ESRD). BMC Nephrol. 2020, 21, 511. [Google Scholar] [CrossRef] [PubMed]
- Ahbap, E.; Sakacı, T.; Kara, E.; Sahutoglu, T.; Koc, Y.; Basturk, T.; Sevınc, M.; Akgol, C.; Kayalar, A.; Ucar, Z.; et al. Neutrophil-to-lymphocyte ratio and platelet-tolymphocyte ratio in evaluation of inflammation in end-stage renal disease. Clin. Nephrol. 2016, 85, 199–208. [Google Scholar] [CrossRef]
- Khan, M.A.; Kassianos, A.J.; Hoy, W.E.; Alam, A.K.; Healy, H.G.; Gobe, G.C. Promoting Plant-Based Therapies for Chronic Kidney Disease. J. Evid.-Based Integr. Med. 2022, 27, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, N.; Anteyi, E. The Role of Dietary Fiber and Gut Microbiome Modulation in Progression of Chronic Kidney Disease. Toxins 2022, 14, 183. [Google Scholar] [CrossRef]
- Sirich, T.L.; Plummer, N.S.; Gardner, C.D.; Hostetter, T.H.; Meyer, T.W. Effect of increasing dietary fiber on plasma levels of colon-derived solutes in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1603–1610. [Google Scholar] [CrossRef]
- Xie, L.M.; Ge, Y.Y.; Huang, X.; Zhang, Y.Q.; Li, J.X. Effects of fermentable dietary fiber supplementation on oxidative and inflammatory status in hemodialysis patients. Int. J. Clin. Exp. Med. 2015, 8, 1363–1369. [Google Scholar]
- Krishnamurthy, V.M.; Wei, G.; Baird, B.C.; Murtaugh, M.; Chonchol, M.B.; Raphael, K.L.; Greene, T.; Beddhu, S. High dietary fiber intake is associated with decreased inflammation and all-cause mortality in patients with chronic kidney disease. Kidney Int. 2012, 81, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Kaimori, J.Y.; Isaka, Y. Plant-Dominant Low Protein Diet: A Potential Alternative Dietary Practice for Patients with Chronic Kidney Disease. Nutrients 2023, 15, 1002. [Google Scholar] [CrossRef] [PubMed]
- Kramers, B.J. Salt, but not protein intake, is associated with accelerated disease progression in autosomal dominant polycystic kidney disease. Kidney Int. 2020, 98, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Nowak, K.L.; Chonchol, M.B.; Bing, K.; Ghanem, A.; Rahbari-Oskoui, F.F.; Dahl, N.K.; Mrug, M. Polycystic Kidney Disease Diet: What is Known and What is Safe. Clin. J. Am. Soc. Nephrol. 2024, 19, 664–682. [Google Scholar] [CrossRef]
- Elmadfa, I.; Meyer, A.L. Animal Proteins as Important Contributors to a Healthy Human Diet. Annu. Rev. Anim. Biosci. 2017, 5, 111–131. [Google Scholar] [CrossRef]
- Alvirdizadeh, S.; Yuzbashian, E.; Mirmiran, P.; Eghtesadi, S.; Azizi, F. A prospective study on total protein, plant protein and animal protein in relation to the risk of incident chronic kidney disease. BMC Nephrol. 2020, 21, 489. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Plant Food Groups | PDI | hPDI | uPDI | |
|---|---|---|---|---|
| Healthy | ||||
| Whole grains | Whole-grain breakfast cereal, other cooked breakfast cereal, cooked oatmeal, dark bread, brown rice, other grains, bran, wheat germ, popcorn | Positive | Positive | Reverse |
| Fruits | Raisins or grapes, prunes, bananas, cantaloupe, watermelon, fresh apples or pears, oranges, grapefruit, strawberries, blueberries, peaches or apricots or plums | Positive | Positive | Reverse |
| Vegetables | Tomatoes, tomato juice, tomato sauce, broccoli, cabbage, cauliflower, Brussels sprouts, carrots, mixed vegetables, yellow or winter squash, eggplant or zucchini, yams or sweet potatoes, spinach cooked, spinach raw, kale or mustard or chard greens, iceberg or head lettuce, romaine or leaf lettuce, celery, mushrooms, beets, alfalfa sprouts, garlic, corn | Positive | Positive | Reverse |
| Nuts | Nuts, peanut butter | Positive | Positive | Reverse |
| Legumes | String beans, tofu or soybeans, beans or lentils, peas or lima beans | Positive | Positive | Reverse |
| Vegetable oils | Oil-based salad dressing, vegetable oil used for cooking | Positive | Positive | Reverse |
| Tea and coffee | Tea, coffee, decaffeinated coffee | Positive | Positive | Reverse |
| Less healthy | ||||
| Fruit juices | Apple cider (non-alcoholic) or juice, orange juice, grapefruit juice, other fruit juice | Positive | Reverse | Positive |
| Refined grains | Refined-grain breakfast cereal, white bread, English muffins or bagels or rolls, muffins or biscuits, white rice, pancakes or waffles, crackers, pasta | Positive | Reverse | Positive |
| Potatoes | French fries, baked or mashed potatoes, potato or corn chips | Positive | Reverse | Positive |
| Sugar-sweetened beverages | Colas with caffeine and sugar, colas without caffeine but with sugar, other carbonated beverages with sugar, non-carbonated fruit drinks with sugar | Positive | Reverse | Positive |
| Sweets and desserts | Chocolates, candy bars, candy without chocolate, cookies (home-baked and ready-made), brownies, doughnuts, cake (home-baked and ready-made), sweet rolls (home-baked and ready-made), pies (home-baked and ready-made), jams or jellies or preserves or syrup or honey | Positive | Reverse | Positive |
| Animal food groups | PDI | hPDI | uPDI | |
| Animal fat | Butter added to food, butter or lard used for cooking | Reverse | Reverse | Reverse |
| Dairy | Skimmed low-fat milk, whole milk, cream, sour cream, sherbet, ice cream, yogurt, cottage or ricotta cheese, cream cheese, other cheese | Reverse | Reverse | Reverse |
| Egg | Eggs | Reverse | Reverse | Reverse |
| Fish or seafood | Canned tuna, dark meat fish, other fish, shrimp or lobster or scallops | Reverse | Reverse | Reverse |
| Meat | Chicken or turkey with skin, chicken or turkey without skin, bacon, hot dogs, processed meats, liver, hamburger, beef or pork or lamb mixed dish, beef or pork or lamb main dish | Reverse | Reverse | Reverse |
| Miscellaneous animal-based foods | Pizza, chowder or cream soup, mayonnaise or other creamy salad dressing | Reverse | Reverse | Reverse |
| Early CKD (eGFR ≥ 60 mL/min/1.73 m2; n = 69) | Advanced CKD (eGFR < 60 mL/min/1.73 m2; n = 37) | p | |
|---|---|---|---|
| Age (y) | 49.80 ± 12.39 | 60.00 ± 9.10 | <0.001 |
| Sex (M/F) | 33/36 | 20/17 | 0.541 |
| Height (cm) | 164.37 ± 8.70 | 165.23 ± 8.02 | 0.618 |
| Body weight (kg) | 63.08 ± 11.49 | 62.51 ± 10.91 | 0.805 |
| BMI (kg/m2) | 23.25 ± 3.06 | 22.76 ± 2.81 | 0.428 |
| Anemia, n (%) | 5 (7.2) | 12 (32.4) | 0.001 |
| Diabetes, n (%) | 2 (2.9) | 3 (8.1) | 0.340 |
| Dyslipidemia, n (%) | 20 (29.0) | 20 (54.1) | 0.011 |
| Gout, n (%) | 1 (1.4) | 2 (5.4) | 0.278 |
| Hypertension, n (%) | 43 (62.3) | 35 (94.6) | <0.001 |
| Hyperuricemia, n (%) | 2 (2.9) | 4 (10.8) | 0.180 |
| SBP (mmHg) | 127.34 ± 13.72 | 126.91 ± 11.35 | 0.876 |
| DBP (mmHg) | 82.10 ± 10.30 | 81.15 ± 9.67 | 0.653 |
| ESR (mm/h) | 16.92 ± 18.73 | 21.94 ± 18.04 | 0.359 |
| Neutrophil–lymphocyte ratio | 1.80 ± 0.90 | 1.88 ± 0.72 | 0.662 |
| Platelet–lymphocyte ratio | 126.29 ± 43.00 | 128.67 ± 42.91 | 0.789 |
| Serum albumin (g/dL) | 4.33 ± 0.32 | 4.21 ± 0.22 | 0.039 |
| Hemoglobin (g/dL) | 13.43 ± 1.55 | 12.05 ± 1.48 | <0.001 |
| Hematocrit (%) | 40.57 ± 4.13 | 37.26 ± 3.97 | <0.001 |
| eGFR (mL/min/1.73 m2) | 89.48 ± 16.18 | 33.80 ± 13.57 | <0.001 |
| BUN (mg/dL) | 14.12 ± 3.40 | 30.54 ± 14.20 | <0.001 |
| Serum creatinine (mg/dL) | 0.88 ± 0.19 | 2.13 ± 0.81 | <0.001 |
| Serum calcium (mg/dL) | 9.25 ± 0.33 | 9.20 ± 0.34 | 0.454 |
| Serum phosphorus (mg/dL) | 3.51 ± 0.51 | 3.60 ± 0.53 | 0.395 |
| Serum potassium (mmol/L) | 4.25 ± 0.28 | 4.59 ± 0.41 | <0.001 |
| Serum sodium (mmol/L) | 140.67 ± 1.66 | 141.27 ± 2.28 | 0.122 |
| PDI | hPDI | uPDI | |
|---|---|---|---|
| SBP (mmHg) | 0.0003 | −0.088 | 0.015 |
| DBP (mmHg) | 0.134 | −0.039 | −0.030 |
| ESR (mm/h) | −0.182 | −0.237 | −0.061 |
| Neutrophil–lymphocyte ratio | −0.130 | −0.202 * | 0.123 |
| Platelet–lymphocyte ratio | 0.035 | −0.223 * | 0.083 |
| Serum albumin (g/dL) | −0.050 | 0.007 | −0.004 |
| Hemoglobin (g/dL) | −0.054 | 0.034 | −0.058 |
| Hematocrit (%) | −0.066 | 0.022 | −0.008 |
| eGFR (mL/min/1.73 m2) | 0.179 | 0.193 * | −0.418 * |
| BUN (mg/dL) | −0.106 | −0.192 * | 0.316 * |
| Serum creatinine (mg/dL) | −0.215 * | −0.273 * | 0.413 * |
| Serum calcium (mg/dL) | −0.024 | −0.037 | 0.020 |
| Serum phosphorus (mg/dL) | −0.0002 | −0.040 | 0.063 |
| Serum potassium (mmol/L) | 0.008 | −0.014 | 0.200 * |
| Serum sodium (mmol/L) | 0.085 | 0.122 | 0.197 * |
| PDI (Median Score = 54) | hPDI (Median Score = 57) | uPDI (Median Score = 54) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Low PDI (n = 50) | High PDI (n = 56) | p | Low hPDI (n = 52) | High hPDI (n = 54) | p | Low uPDI (n = 48) | High uPDI (n = 58) | p | |
| SBP (mmHg) | 124.94 ± 8.84 | 129.13 ± 15.41 | 0.103 | 129.08 ± 12.20 | 125.45 ± 13.43 | 0.157 | 125.31 ± 11.66 | 128.87 ± 13.84 | 0.166 |
| DBP (mmHg) | 80.30 ± 8.12 | 83.05 ± 11.38 | 0.169 | 81.24 ± 9.48 | 82.28 ± 10.63 | 0.605 | 80.65 ± 8.84 | 82.80 ± 11.01 | 0.283 |
| ESR (mm/h) | 19.83 ± 11.27 | 17.52 ± 22.55 | 0.654 | 21.00 ± 19.92 | 16.65 ± 17.46 | 0.397 | 16.41 ± 17.97 | 20.92 ± 19.16 | 0.377 |
| NLR | 1.90 ± 0.88 | 1.77 ± 0.78 | 0.411 | 2.08 ± 0.93 | 1.60 ± 0.65 | 0.003 | 1.78 ± 0.90 | 1.87 ± 0.78 | 0.576 |
| PLR | 121.98 ± 38.23 | 132.12 ± 46.55 | 0.233 | 137.92 ± 44.67 | 116.38 ± 38.25 | 0.010 | 124.33 ± 46.39 | 129.47 ± 39.83 | 0.548 |
| Serum albumin (g/dL) | 4.31 ± 0.27 | 4.27 ± 0.31 | 0.492 | 4.28 ± 0.31 | 4.30 ± 0.27 | 0.820 | 4.27 ± 0.27 | 4.31 ± 0.31 | 0.494 |
| Hemoglobin (g/dL) | 12.94 ± 1.74 | 12.94 ± 1.59 | 0.991 | 13.02 ± 1.46 | 12.86 ± 1.84 | 0.629 | 13.08 ± 1.60 | 12.83 ± 1.70 | 0.435 |
| Hematocrit (%) | 39.44 ± 4.57 | 39.37 ± 4.19 | 0.931 | 39.66 ± 3.90 | 39.15 ± 4.78 | 0.555 | 39.62 ± 4.17 | 39.23 ± 4.52 | 0.646 |
| eGFR (mL/min/1.73 m2) | 65.22 ± 30.47 | 74.35 ± 30.57 | 0.127 | 62.94 ± 33.20 | 76.89 ± 26.68 | 0.019 | 84.09 ± 25.00 | 58.42 ± 30.33 | <0.001 |
| BUN (mg/dL) | 21.26 ± 12.49 | 18.59 ± 11.05 | 0.245 | 22.88 ± 14.21 | 16.93 ± 7.89 | 0.009 | 15.60 ± 6.45 | 23.36 ± 13.90 | 0.001 |
| Serum creatinine (mg/dL) | 1.45 ± 0.83 | 1.20 ± 0.72 | 0.104 | 1.57 ± 0.91 | 1.07 ± 0.53 | 0.001 | 0.97 ± 0.37 | 1.61 ± 0.90 | <0.001 |
| Serum calcium (mg/dL) | 9.24 ± 0.35 | 9.22 ± 0.31 | 0.819 | 9.24 ± 0.35 | 9.22 ± 0.31 | 0.847 | 9.19 ± 0.29 | 9.27 ± 0.36 | 0.226 |
| Serum phosphorus (mg/dL) | 3.56 ± 0.54 | 3.53 ± 0.49 | 0.797 | 3.54 ± 0.54 | 3.55 ± 0.49 | 0.968 | 3.49 ± 0.45 | 3.59 ± 0.56 | 0.285 |
| Serum potassium (mmol/L) | 4.36 ± 0.38 | 4.37 ± 0.36 | 0.834 | 4.34 ± 0.38 | 4.39 ± 0.36 | 0.555 | 4.27 ± 0.33 | 4.45 ± 0.39 | 0.011 |
| Serum sodium (mmol/L) | 140.78 ± 2.15 | 140.96 ± 1.68 | 0.622 | 140.58 ± 1.96 | 141.17 ± 1.83 | 0.113 | 140.65 ± 1.87 | 141.07 ± 1.94 | 0.258 |
| PDI (Median Score = 54) | hPDI (Median Score = 57) | uPDI (Median Score = 54) | ||||
|---|---|---|---|---|---|---|
| Low PDI (n = 50) | High PDI (n = 56) | Low hPDI (n = 52) | High hPDI (n = 54) | Low uPDI (n = 48) | High uPDI (n = 58) | |
| Model 1 Odds ratio (95% CI) | 1.00 (Ref) | 0.654 (0.293–1.459) p = 0.300 | 1.00 (Ref) | 0.256 (0.109–0.603) p = 0.002 | 1.00 (Ref) | 6.276 (2.420–16.271) p < 0.001 |
| Model 2 Odds ratio (95% CI) | 1.00 (Ref) | 0.462 (0.185–1.153) p = 0.098 | 1.00 (Ref) | 0.117 (0.039–0.351) p < 0.001 | 1.00 (Ref) | 8.450 (2.810–25.409) p < 0.001 |
| PDI (Median Score = 54) | hPDI (Median Score = 57) | uPDI (Median Score = 54) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Low PDI (n = 50) | High PDI (n = 56) | p | Low hPDI (n = 52) | High hPDI (n = 54) | p | Low uPDI (n = 48) | High uPDI (n = 58) | p | |
| Energy (kcal) | 1791.74 ± 435.05 | 1883.89 ± 494.47 | 0.313 | 1912.23 ± 490.23 | 1771.28 ± 437.90 | 0.121 | 1888.69 ± 543.46 | 1800.48 ± 394.27 | 0.336 |
| Carbohydrate (g) | 255.91 ± 56.79 | 285.50 ± 78.82 | 0.030 | 276.62 ± 70.29 | 266.66 ± 71.15 | 0.470 | 267.29 ± 77.51 | 275.06 ± 64.74 | 0.575 |
| Fiber (g) | 21.60 ± 8.52 | 25.51 ± 9.80 | 0.032 | 20.60 ± 8.89 | 26.62 ± 8.96 | 0.001 | 25.69 ± 8.61 | 21.99 ± 9.73 | 0.042 |
| Protein (g) | 70.13 ± 21.29 | 71.47 ± 21.17 | 0.747 | 73.39 ± 23.35 | 68.38 ± 18.65 | 0.224 | 75.97 ± 22.95 | 66.59 ± 18.66 | 0.022 |
| Animal protein (g) | 36.13 ± 17.10 | 34.31 ± 15.94 | 0.572 | 38.70 ± 18.22 | 31.77 ± 13.86 | 0.029 | 40.07 ± 17.44 | 31.11 ± 14.50 | 0.005 |
| Plant protein (g) | 32.50 ± 9.09 | 35.38 ± 10.06 | 0.126 | 32.85 ± 9.19 | 35.15 ± 10.08 | 0.222 | 34.58 ± 10.58 | 33.56 ± 8.93 | 0.590 |
| Fat (g) | 50.13 ± 20.12 | 47.99 ± 20.08 | 0.584 | 52.36 ± 21.35 | 45.76 ± 18.29 | 0.090 | 54.18 ± 22.99 | 44.71 ± 16.20 | 0.015 |
| Cholesterol (mg) | 293.67 ± 151.40 | 294.44 ± 220.81 | 0.983 | 295.27 ± 128.13 | 292.93 ± 236.62 | 0.950 | 309.90 ± 140.30 | 280.98 ± 223.91 | 0.439 |
| SFAs (g) | 10.48 ± 5.69 | 10.87 ± 7.74 | 0.770 | 11.38 ± 6.65 | 10.01 ± 6.97 | 0.301 | 10.65 ± 5.03 | 10.71 ± 8.05 | 0.968 |
| MUFAs (g) | 12.41 ± 7.09 | 12.98 ± 9.52 | 0.728 | 13.01 ± 7.84 | 12.43 ± 9.02 | 0.724 | 12.83 ± 5.05 | 12.62 ± 10.47 | 0.900 |
| PUFAs (g) | 12.31 ± 5.89 | 13.75 ± 7.08 | 0.261 | 12.12 ± 6.44 | 13.99 ± 6.59 | 0.143 | 14.61 ± 7.00 | 11.79 ± 5.92 | 0.027 |
| ω-6 PUFAs (g) | 4.77 ± 4.39 | 5.08 ± 4.53 | 0.727 | 4.43 ± 4.52 | 5.42 ± 4.36 | 0.252 | 5.54 ± 4.71 | 4.43 ± 4.19 | 0.201 |
| ω-3 PUFAs (g) | 1.04 ± 1.17 | 1.25 ± 2.14 | 0.534 | 0.92 ± 1.19 | 1.37 ± 2.14 | 0.185 | 1.55 ± 2.28 | 0.82 ± 1.05 | 0.031 |
| Vit A (µg RAE) | 418.40 ± 216.31 | 499.70 ± 405.25 | 0.208 | 430.39 ± 321.43 | 491.16 ± 340.17 | 0.347 | 530.11 ± 354.74 | 404.44 ± 301.18 | 0.051 |
| Vit D (µg) | 3.91 ± 3.64 | 5.30 ± 9.79 | 0.343 | 4.89 ± 9.35 | 4.41 ± 5.33 | 0.746 | 5.65 ± 5.50 | 3.81 ± 8.85 | 0.212 |
| Vit E (mg α-TE) | 14.98 ± 4.96 | 18.60 ± 7.51 | 0.005 | 15.66 ± 5.30 | 18.08 ± 7.61 | 0.061 | 18.87 ± 7.85 | 15.25 ± 4.98 | 0.005 |
| Vit K (µg) | 151.54 ± 122.15 | 162.10 ± 108.17 | 0.638 | 141.76 ± 116.22 | 171.91 ± 111.99 | 0.177 | 158.71 ± 112.81 | 155.80 ± 116.92 | 0.897 |
| Vit B1 (mg) | 1.54 ± 0.50 | 1.67 ± 0.59 | 0.206 | 1.59 ± 0.51 | 1.63 ± 0.59 | 0.670 | 1.74 ± 0.62 | 1.50 ± 0.47 | 0.024 |
| Vit B2 (mg) | 1.35 ± 0.45 | 1.33 ± 0.39 | 0.781 | 1.36 ± 0.45 | 1.32 ± 0.39 | 0.671 | 1.51 ± 0.45 | 1.20 ± 0.33 | <0.001 |
| Niacin (mg NE) | 12.30 ± 4.42 | 13.57 ± 5.39 | 0.193 | 12.68 ± 4.99 | 13.25 ± 4.99 | 0.556 | 14.55 ± 5.38 | 11.66 ± 4.22 | 0.003 |
| Vit B6 (mg) | 1.78 ± 1.13 | 1.90 ± 1.20 | 0.605 | 1.68 ± 0.91 | 1.99 ± 1.35 | 0.174 | 2.13 ± 1.36 | 1.60 ± 0.91 | 0.020 |
| Folate (µg DFE) | 417.99 ± 127.67 | 451.09 ± 155.11 | 0.236 | 409.39 ± 141.37 | 460.60 ± 141.56 | 0.065 | 474.61 ± 145.80 | 403.09 ± 133.60 | 0.010 |
| Vit B12 (µg) | 8.48 ± 5.81 | 8.19 ± 5.27 | 0.788 | 8.29 ± 6.26 | 8.36 ± 4.72 | 0.946 | 9.33 ± 5.03 | 7.49 ± 5.78 | 0.086 |
| Vit C (mg) | 96.98 ± 63.33 | 115.45 ± 72.17 | 0.167 | 92.82 ± 64.72 | 120.15 ± 69.85 | 0.039 | 116.27 ± 71.83 | 98.86 ± 65.10 | 0.194 |
| Calcium (mg) | 461.22 ± 226.49 | 520.54 ± 219.48 | 0.174 | 481.35 ± 245.21 | 503.35 ± 202.66 | 0.615 | 535.82 ± 206.30 | 456.76 ± 232.89 | 0.070 |
| Phosphorus (mg) | 1006.38 ± 300.32 | 1063.32 ± 327.60 | 0.355 | 1027.47 ± 324.48 | 1045.13 ± 308.06 | 0.774 | 1134.14 ± 320.80 | 955.63 ± 288.18 | 0.003 |
| Sodium (mg) | 2925.43 ± 941.94 | 3308.05 ± 1174.16 | 0.069 | 3058.52 ± 1178.10 | 3194.06 ± 989.55 | 0.522 | 3440.21 ± 989.24 | 2868.83 ± 1097.04 | 0.006 |
| Potassium (mg) | 2518.73 ± 930.76 | 2906.80 ± 1081.18 | 0.052 | 2530.87 ± 1059.40 | 2909.49 ± 968.21 | 0.057 | 2974.40 ± 950.56 | 2516.31 ± 1049.15 | 0.022 |
| PDI (Median Score = 54) | hPDI (Median Score = 57) | uPDI (Median Score = 54) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Low PDI (n = 50) | High PDI (n = 56) | p | Low hPDI (n = 52) | High hPDI (n = 54) | p | Low uPDI (n = 48) | High uPDI (n = 58) | p | |
| Protein intake (g/kg BW) | |||||||||
| Normal (≥0.8 g/kg BW) | 39 (78.0%) | 52 (92.9%) | 0.048 | 40 (76.9%) | 51 (94.4%) | 0.012 | 45 (93.75%) | 46 (79.3%) | 0.049 |
| Reduced (<0.8 g/kg BW) | 11 (22.0%) | 4 (7.1%) | 12 (23.1%) | 3 (5.6%) | 3 (6.25%) | 12 (20.7%) | |||
| Dietary Fiber | Dietary Protein | Dietary Animal Protein | Dietary Plant Protein | |
|---|---|---|---|---|
| SBP (mmHg) | −0.095 | −0.021 | 0.041 | −0.105 |
| DBP (mmHg) | 0.066 | 0.017 | 0.021 | 0.005 |
| ESR (mm/h) | −0.115 | −0.057 | 0.021 | −0.192 |
| Neutrophil–lymphocyte ratio | −0.208 * | −0.101 | 0.003 | −0.197 * |
| Platelet–lymphocyte ratio | −0.135 | −0.140 | −0.046 | −0.236 * |
| Serum albumin (g/dL) | 0.078 | 0.121 | 0.111 | 0.041 |
| Hemoglobin (g/dL) | 0.132 | 0.165 | 0.092 | 0.202 * |
| Hematocrit (%) | 0.126 | 0.148 | 0.076 | 0.191 |
| eGFR (mL/min/1.73 m2) | 0.200 * | 0.246 * | 0.216 * | 0.118 |
| BUN (mg/dL) | −0.317 * | −0.196 * | −0.104 | −0.214 * |
| Serum creatinine (mg/dL) | −0.336 * | −0.228 * | −0.180 | −0.158 |
| Serum calcium (mg/dL) | 0.055 | −0.043 | −0.059 | 0.023 |
| Serum phosphorus (mg/dL) | −0.029 | −0.015 | 0.003 | −0.073 |
| Serum potassium (mmol/L) | −0.047 | −0.013 | −0.018 | −0.001 |
| Serum sodium (mmol/L) | 0.046 | −0.154 | −0.143 | −0.067 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, S.; Han, M.; Ryu, H.; Kang, E.; Kim, M.; Ahn, C.; Yang, S.J.; Oh, K.-H. Compliance with a Healthful Plant-Based Diet Is Associated with Kidney Function in Patients with Autosomal Dominant Polycystic Kidney Disease. Nutrients 2024, 16, 2749. https://doi.org/10.3390/nu16162749
Heo S, Han M, Ryu H, Kang E, Kim M, Ahn C, Yang SJ, Oh K-H. Compliance with a Healthful Plant-Based Diet Is Associated with Kidney Function in Patients with Autosomal Dominant Polycystic Kidney Disease. Nutrients. 2024; 16(16):2749. https://doi.org/10.3390/nu16162749
Chicago/Turabian StyleHeo, Sumin, Miyeun Han, Hyunjin Ryu, Eunjeong Kang, Minsang Kim, Curie Ahn, Soo Jin Yang, and Kook-Hwan Oh. 2024. "Compliance with a Healthful Plant-Based Diet Is Associated with Kidney Function in Patients with Autosomal Dominant Polycystic Kidney Disease" Nutrients 16, no. 16: 2749. https://doi.org/10.3390/nu16162749
APA StyleHeo, S., Han, M., Ryu, H., Kang, E., Kim, M., Ahn, C., Yang, S. J., & Oh, K.-H. (2024). Compliance with a Healthful Plant-Based Diet Is Associated with Kidney Function in Patients with Autosomal Dominant Polycystic Kidney Disease. Nutrients, 16(16), 2749. https://doi.org/10.3390/nu16162749