
Cognitive Function during and after Pregnancy and One-Year Postpartum in Type 1 Diabetes: A Longitudinal Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statements
2.2. Study Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Collection
2.3.1. Cognitive Test
2.3.2. Blood Sample Analyses
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lezak, M.D.; Howieson, D.B.; Bigler, E.D.; Tranel, D. Neuropsychological Assessment, 5th ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44 (Suppl. S1), S15–S33. [Google Scholar] [CrossRef]
- Brismar, T.; Cooray, G.; Sundgren, M.; Hyllienmark, L. On the physiology of cognitive decline in type 1 diabetes. Neurophysiol. Clin. 2021, 51, 59–265. [Google Scholar] [CrossRef]
- Dogra, V.; Mittal, B.; Senthil Kumaran, S.; Nehra, A.; Sagar, R.; Gupta, A.; Kalaivani, M.; Gupta, Y.; Tandon, N. Evaluation of Cognitive Deficits in Adults with Type 1 Diabetes Stratified by the Age of Diabetes Onset: A Cross-Sectional Study. Adv. Ther. 2022, 39, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Fang, C.; Li, X.; Cao, Y.J.; Zhang, Q.L.; Huang, Y.; Pan, J.; Zhang, X. Type 1 diabetes-associated cognitive impairment and diabetic peripheral neuropathy in Chinese adults: Results from a prospective cross-sectional study. BMC Endocr. Disord. 2019, 27, 1934. [Google Scholar] [CrossRef]
- Shalimova, A.; Graff, B.; Gasecki, D.; Wolf, J.; Sabisz, A.; Szurowska, E.; Jodzio, K.; Narkiewicz, K. Cognitive Dysfunction in Type 1 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2019, 104, 2239–2249. [Google Scholar] [CrossRef]
- Davies, S.J.; Lum, J.A.; Skouteris, H.; Byrne, L.K.; Hayden, M.J. Cognitive impairment during pregnancy: A meta-analysis. Med. J. Aust. 2018, 208, 35–40. [Google Scholar] [CrossRef]
- Nevo-Shenker, M.; Shalitin, S. The Impact of Hypo- and Hyperglycemia on Cognition and Brain Development in Young Children with Type 1 Diabetes. Horm. Res. Paediatr. 2021, 94, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Gonder-Frederick, L.A.; Zrebiec, J.F.; Bauchowitz, A.U.; Ritterband, L.M.; Magee, J.C.; Cox, D.J.; Clarke, W.L. Cognitive function is disrupted by both hypo- and hyperglycemia in school-aged children with type 1 diabetes: A field study. Diabetes Care 2009, 32, 1001–1006. [Google Scholar] [CrossRef]
- Wessels, A.M.; Scheltens, P.; Barkhof, F.; Heine, R.J. Hyperglycaemia as a determinant of cognitive decline in patients with type 1 diabetes. Eur. J. Pharmacol. 2008, 585, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.J.; Northam, E.A.; Ryan, C.M. The effect of type 1 diabetes on the developing brain. Lancet Child Adolesc. Health 2019, 3, 427–436. [Google Scholar] [CrossRef]
- Lacy, M.E.; Moran, C.; Gilsanz, P.; Beeri, M.S.; Karter, A.J.; Whitmer, R.A. Comparison of cognitive function in older adults with type 1 diabetes, type 2 diabetes, and no diabetes: Results from the Study of Longevity in Diabetes (SOLID). BMJ Open Diabetes Res. Care 2022, 10, e002557. [Google Scholar] [CrossRef]
- Musen, G.; Tinsley, L.J.; Marcinkowski, K.A.; Pober, D.; Sun, J.K.; Khatri, M.; Huynh, R.; Lu, A.; King, G.L.; Keenan, H.A. Cognitive Function Deficits Associated with Long-Duration Type 1 Diabetes and Vascular Complications. Diabetes Care 2018, 41, 1749–1756. [Google Scholar] [CrossRef]
- Zhao, X.; Han, Q.; Lv, Y.; Sun, L.; Gang, X.; Wang, G. Biomarkers for cognitive decline in patients with diabetes mellitus: Evidence from clinical studies. Oncotarget 2017, 9, 7710–7726. [Google Scholar] [CrossRef]
- Ryan, C.M.; Geckle, M.O.; Orchard, T.J. Cognitive efficiency declines over time in adults with Type 1 diabetes: Effects of micro- and macrovascular complications. Diabetologia 2003, 46, 940–948. [Google Scholar] [CrossRef]
- Sima, A.A.; Kamiya, H. Is C-peptide replacement the missing link for successful treatment of neurological complications in type 1 diabetes? Curr. Drug Targets 2008, 9, 37–46. [Google Scholar] [CrossRef]
- Barber, T.M.; Kyrou, I.; Randeva, H.S.; Weickert, M.O. Mechanisms of Insulin Resistance at the Crossroad of Obesity with Associated Metabolic Abnormalities and Cognitive Dysfunction. Int. J. Mol. Sci. 2021, 22, 546. [Google Scholar] [CrossRef] [PubMed]
- Jequier, E. Leptin signaling, adiposity, and energy balance. Ann. N. Y. Acad. Sci. 2022, 967, 379–388. [Google Scholar] [CrossRef]
- Leigh, S.J.; Morris, M.J. Diet, inflammation and the gut microbiome: Mechanisms for obesity-associated cognitive impairment. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165767. [Google Scholar] [CrossRef]
- Enebe, J.T.; Enebe, N.O.; Nwagha, T.U.; Meka, I.A.; Nwankwo, M.E.; Izuka, E.O.; Egede, J.O.; Ugwu, I.A.; Okoro, N.I.; Okoye, H.C.; et al. Serum leptin levels and relationship with maternal weight gain at term among obese and non-obese pregnant women in Enugu, Nigeria: A comparative cross-sectional study. J. Int. Med. Res. 2023, 51, 3000605231213265. [Google Scholar] [CrossRef] [PubMed]
- Bissels, G.J.; Whitmer, R.A. Cognitive dysfunction in diabetes: How to implement emerging guidelines. Diabetologia 2020, 63, 3–9. [Google Scholar] [CrossRef]
- Henry, J.F.; Sherwin, B.B. Hormones and cognitive functioning during late pregnancy and postpartum: A longitudinal study. Behav. Neurosci. 2012, 6, 3–85. [Google Scholar] [CrossRef]
- Tulchinsk, D.; Hobel, C.J.; Yeager, E.; Marshall, J.R. Plasma estrone, estradiol, estriol, progesterone, and 17-hydroxyprogesterone in human pregnancy. I. Normal pregnancy. Am. J. Obstet. Gynecol. 1972, 112, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.; Schaffir, J. “Pregnancy Brain”: A Review of Cognitive Changes in Pregnancy and Postpartum. Obstet. Gynecol. Surv. 2019, 74, 178–185. [Google Scholar] [CrossRef]
- Barda, G.; Mizrachi, Y.; Borokchovich, I.; Yair, L.; Kertesz, D.P.; Dabby, R. The effect of pregnancy on maternal cognition. Sci. Rep. 2021, 11, 12187. [Google Scholar] [CrossRef] [PubMed]
- Cato, A.; Hershey, T. Cognition and Type 1 Diabetes in Children and Adolescents. Diabetes Spectr. 2016, 29, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Amidei, C.B.; Fayosse, A.; Dumurgier, J.; Machado-Fragua, M.D.; Tabak, A.G.; van Sloten, T.; Kivimäki, M.; Dugravot, A.; Sabia, S.; Singh-Manoux, A. Association between Age at Diabetes Onset and Subsequent Risk of Dementia. JAMA 2021, 325, 1640–1649. [Google Scholar] [CrossRef]
- Dye, L.; Boyle, N.B.; Champ, C.; Lawton, C. The relationship between obesity and cognitive health and decline. Proc. Nutr. Soc. 2017, 76, 443–454. [Google Scholar] [CrossRef]
- Ivanisevic, M.; Marcinko, D.; Vuckovic-Rebrina, S.; Delmis, J. Positive Association between Preserved C-Peptide and Cognitive Function in Pregnant Women with TyDiabetes. Biomedicines 2022, 10, 2785. [Google Scholar] [CrossRef]
- Warren, M.W.; Hynan, L.S.; Weiner, M.F. Leptin and cognition. Dement. Geriatr. Cogn. Disord. 2012, 33, 410–415. [Google Scholar] [CrossRef]
- Scarpace, P.J.; Zhang, Y. Elevated leptin: Consequence or cause of obesity? Front. Biosci. 2007, 12, 3531–3544. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | Minimum | Maximum | Mean ± SD |
|---|---|---|---|---|
| Age (years) | 64 | 19 | 40 | 30.9 ± 5.2 |
| <30 years | 25 | 19 | 29 | 25.6 ± 3.0 |
| ≥30 years | 39 | 30 | 38 | 34.3 ± 2.9 |
| Duration of T1DM (y) | 64 | 2 | 37 | 14.9 ± 9.2 |
| ≤8 years | 19 | 2 | 8 | 3.5 ± 2.0 |
| >8 years | 45 | 9 | 37 | 19.8 ± 6.3 |
| Age of T1DM onset (y) | 64 | 2 | 36 | 16.0 ± 9.3 |
| ≤10 years | 25 | 2 | 10 | 7.3 ± 2.8 |
| >10 years | 39 | 11 | 36 | 21.6 ± 7.5 |
| Height (cm) | 64 | 156 | 183 | 166.3 ± 5.7 |
| Gestational weight gain (kg) | 64 | 0 | 22 | 13.0 ± 4.4 |
| BMI (kg/m2) before pregnancy | 64 | 18.1 | 37.4 | 23.6 ± 4.7 |
| ≤24.9 (kg/m2) | 44 | 18.1 | 24.6 | 21.4 ± 1.6 |
| 25–29.9 (kg/m2) | 12 | 25 | 29.9 | 27.1 ± 3.7 |
| ≥30.0 (kg/m2) | 8 | 31 | 37.4 | 32.3 ± 1.3 |
| BMI (kg/m2) at the time of delivery | 64 | 18.9 | 43.0 | 28.0 ± 4.7 |
| ≤24.9 (kg/m2) | 18 | 18.9 | 24.8 | 23.1 ± 1.7 |
| 25–29.9 (kg/m2) | 28 | 25.3 | 29.9 | 27.6 ± 1.6 |
| ≥30.0 (kg/m2) | 17 | 30 | 43 | 34.1 ± 3.2 |
| Education | 64 | |||
| High school and university | 30 | |||
| Graduate school | 34 | |||
| HbA1c (%) 1st trimester | 64 | 5.4 | 8.0 | 7.2 ± 0.7 |
| HbA1c (%) 2nd trimester | 64 | 4.6 | 11.6 | 6.2 ± 1.1 |
| HbA1c (%) 3rd trimester | 64 | 4.2 | 7.8 | 5.9 ± 0.8 |
| Leptin 1st trimester (ng/L) | 60 | 3.7 | 234.9 | 22.8 (14.9–39.1) |
| Cognitive Function in Pregnancy | ||||
|---|---|---|---|---|
| Domain | N | Minimum | Maximum | Mean ± SD |
| Reasoning a | 64 | 277 | 717 | 479.8 ± 96.1 |
| Memory | 64 | 153 | 619 | 385.6 ± 115.9 |
| Attention c | 64 | 290 | 745 | 567.4 ± 102.2 |
| Coordination | 64 | 10 | 584 | 285.0 ± 128.0 |
| Perception | 64 | 249 | 672 | 480.6 ± 91.8 |
| Total cognitive function | 64 | 228 | 614 | 446.4 ± 82.1 |
| Cognitive function postpartum | ||||
| Reasoning b | 64 | 110 | 698 | 451.8 ± 134.7 |
| Memory | 64 | 159 | 672 | 421.0 ± 110.3 |
| Attention d | 64 | 124 | 738 | 538.6 ± 128.9 |
| Coordination | 64 | 31 | 626 | 299.4 ± 142.3 |
| Perception | 64 | 153 | 663 | 485.4 ± 101.7 |
| Total cognitive function | 64 | 157 | 645 | 454.4 ± 95.7 |
| Cognitive function one year after delivery | ||||
| Reasoning a,b | 52 | 107 | 674 | 437.5 ± 120.7 |
| Memory | 52 | 115 | 710 | 437.4 ± 128.3 |
| Attention c,d | 52 | 125 | 736 | 482.0 ± 141.4 |
| Coordination | 52 | 104 | 653 | 299.2 ± 134.8 |
| Perception | 52 | 186 | 645 | 450.8 ± 114.0 |
| Total cognitive function | 52 | 159 | 611 | 432.7 ± 99.1 |
| The First Trimester, n = 64 | ||||
|---|---|---|---|---|
| Domain/Score | 600–800 n (%) | 400–600 n (%) | 200–400 n (%) | 0–200 n (%) |
| Reasoning a | 5 (5.4) | 46 (71.9) | 13 (20.3) | |
| Memory | 1 (1.6) | 30 (46.9) | 32 (50.0) | 1 (1.6%) |
| Attention c | 25 (40.6) | 34 (53.1) | 4 (6.3) | |
| Coordination | 13 (20.3) | 31 (48.4) | 20 (31.3) | |
| Perception | 7 (10.8) | 43 (67.2) | 14 (21.9) | |
| Total cognitive function | 3 (4.7) | 46 (71.9) | 15 (23.4) | |
| Postpartum (after delivery), n = 64 | ||||
| Reasoning b | 7 (10.9) | 40 (62.5) | 14 (21.9) | 3 (4.7) |
| Memory | 3 (4.7) | 34 (53.1) | 26 (40.6) | 1 (1.6) |
| Attention c,d | 23 (35.9) | 33 (51.6) | 7 (10.9) | 1 (1.6) |
| Coordination | 3 (4.7) | 12 (18.8) | 35 (54.7) | 14 (21.9) |
| Perception | 9 (14.1) | 45 (70.3) | 9 (14.1) | 1 (1.6) |
| Total cognitive function | 4 (6.3%) | 41 (64.1%) | 18 (28.1%) | 1 (1.6%) |
| One year after delivery, n = 52 | ||||
| Reasoning a,b | 1 (1.9) | 36 (69.2) | 13 (25.0) | 2 (3.8) |
| Memory | 7 (13.5) | 28 (53.8) | 15 (28.8) | 2 (3.1) |
| Attention c,d | 13 (25.0) | 26 (50.0) | 11 (21.2) | 2 (3.8) |
| Coordination | 2 (3.8) | 11 (21.2) | 24 (45.2) | 15 (28.8) |
| Perception | 4 (7.7) | 31 (59.6) | 16 (30.8) | 1 (1.9) |
| Total cognitive function | 1 (1.9) | 37 (71.2) | 13 (25.0) | 1 (1.9) |
| Model | β (95% CI) | p | |
|---|---|---|---|
| Reasoning | Leptin | −0.309 (−0.146; −0.015) | 0.017 |
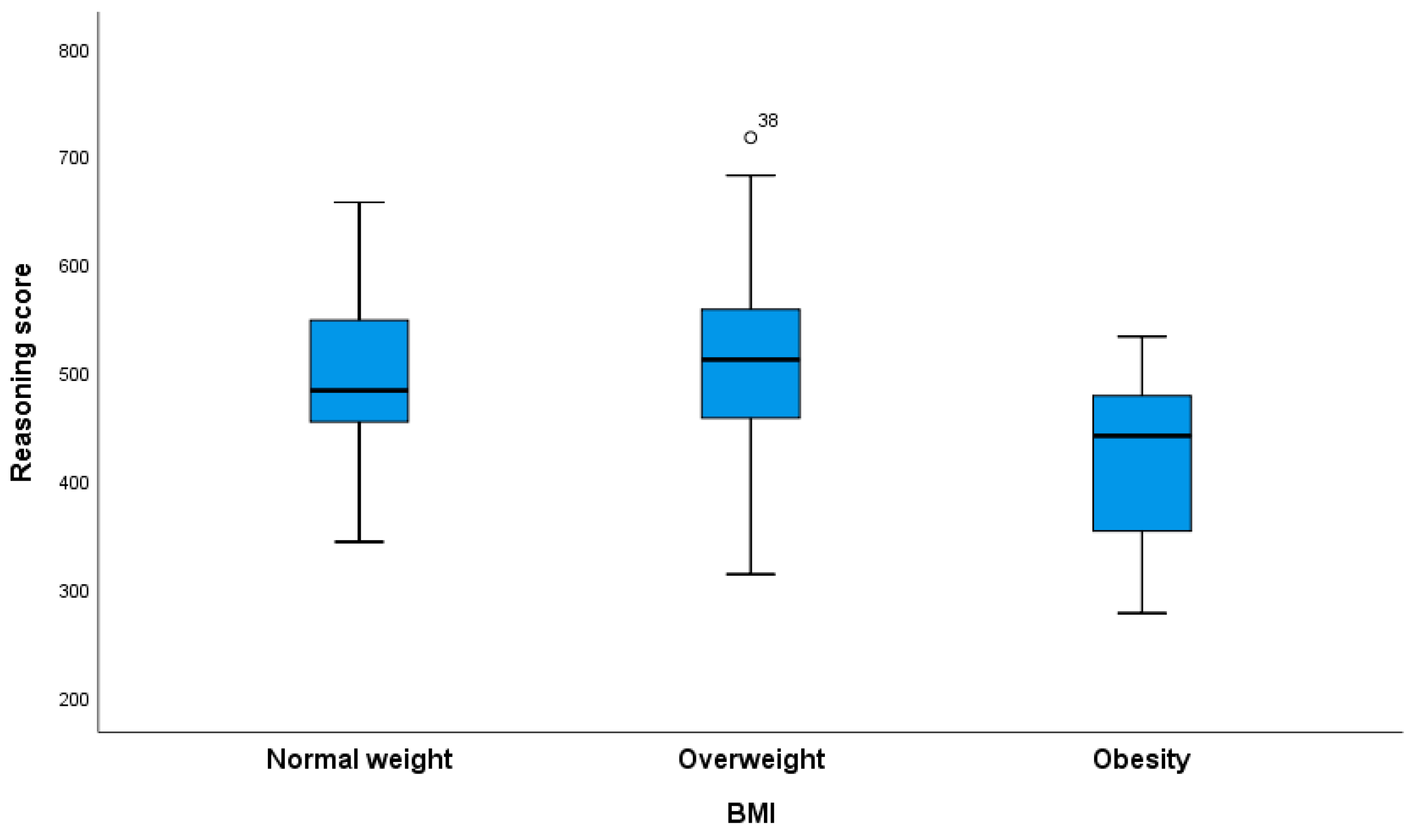
| Reasoning | BMI | −0.251 (−0.044; −0.024) | 0.044 |
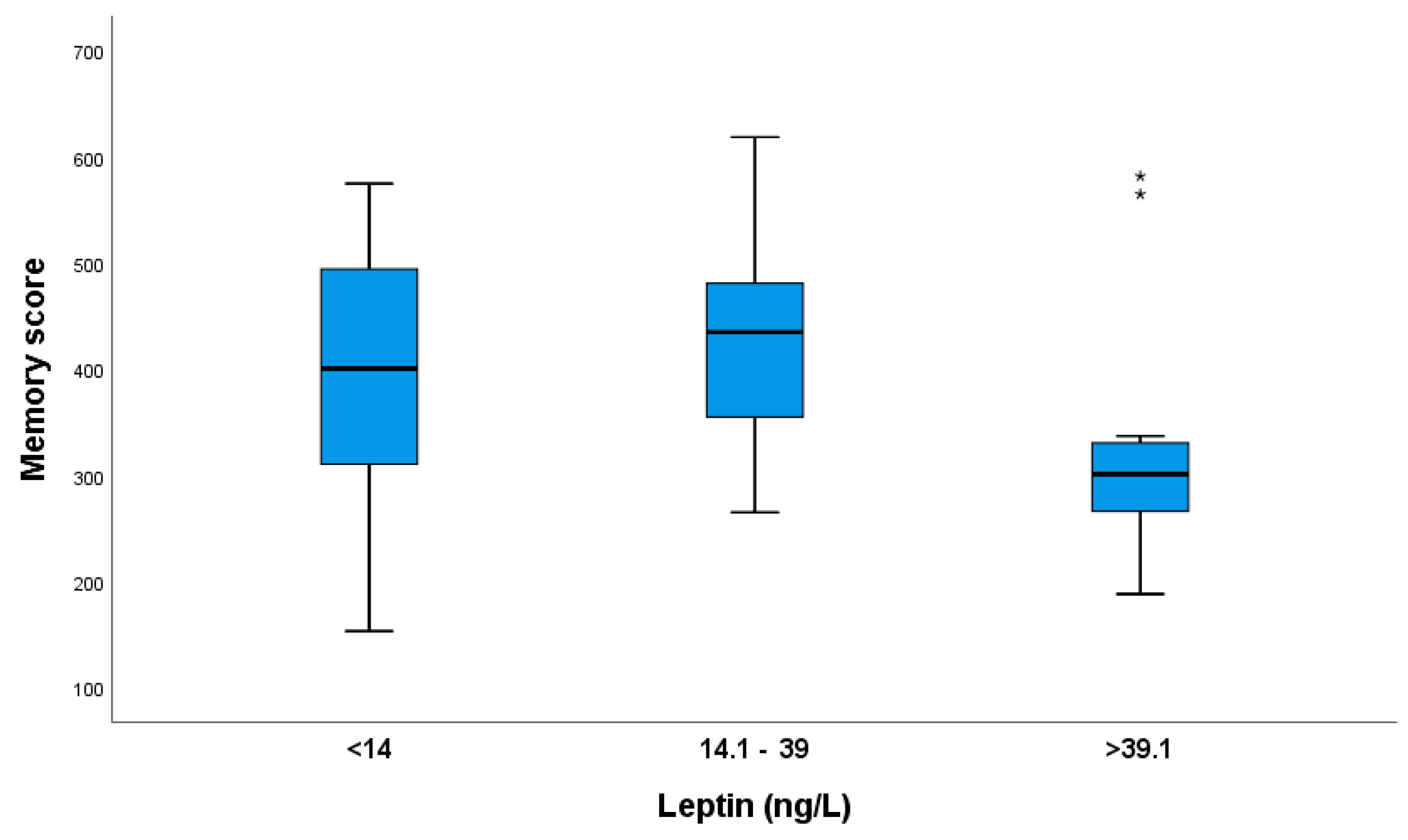
| Memory | Leptin | −0.386 (−0.146; −0.031) | 0.002 |
| Memory | BMI | −0.244 (−0.020; −0.000) | 0.046 |
| Attention | Leptin | −0.292 (−0.137; −0.009) | 0.027 |
| Attention | BMI | −0250 (−0.052; −0.001) | 0.052 |
| Coordination | Leptin | −0.214 (−0.092; −0.009) | 0.109 |
| Coordination | BMI | −0.173 (−0.015; −0.003) | 0.169 |
| Perception | Leptin | −0.203 (−0.121; 0.016) | 0.127 |
| Perception | BMI | −0.059 (−0.016; 0.010) | 0.641 |
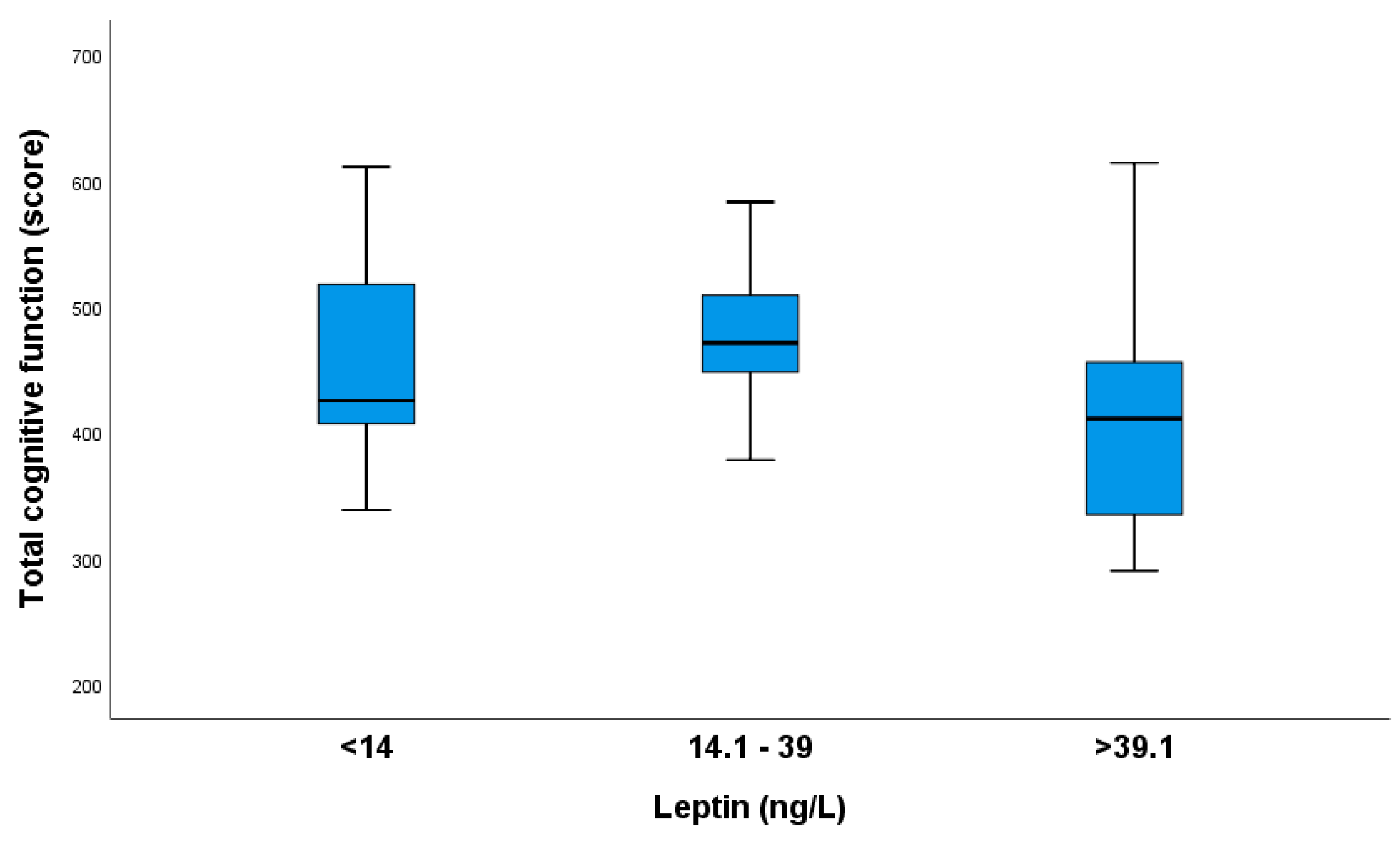
| Total CogniFit | Leptin | −0.382 (−0.190; −0.040) | 0.003 |
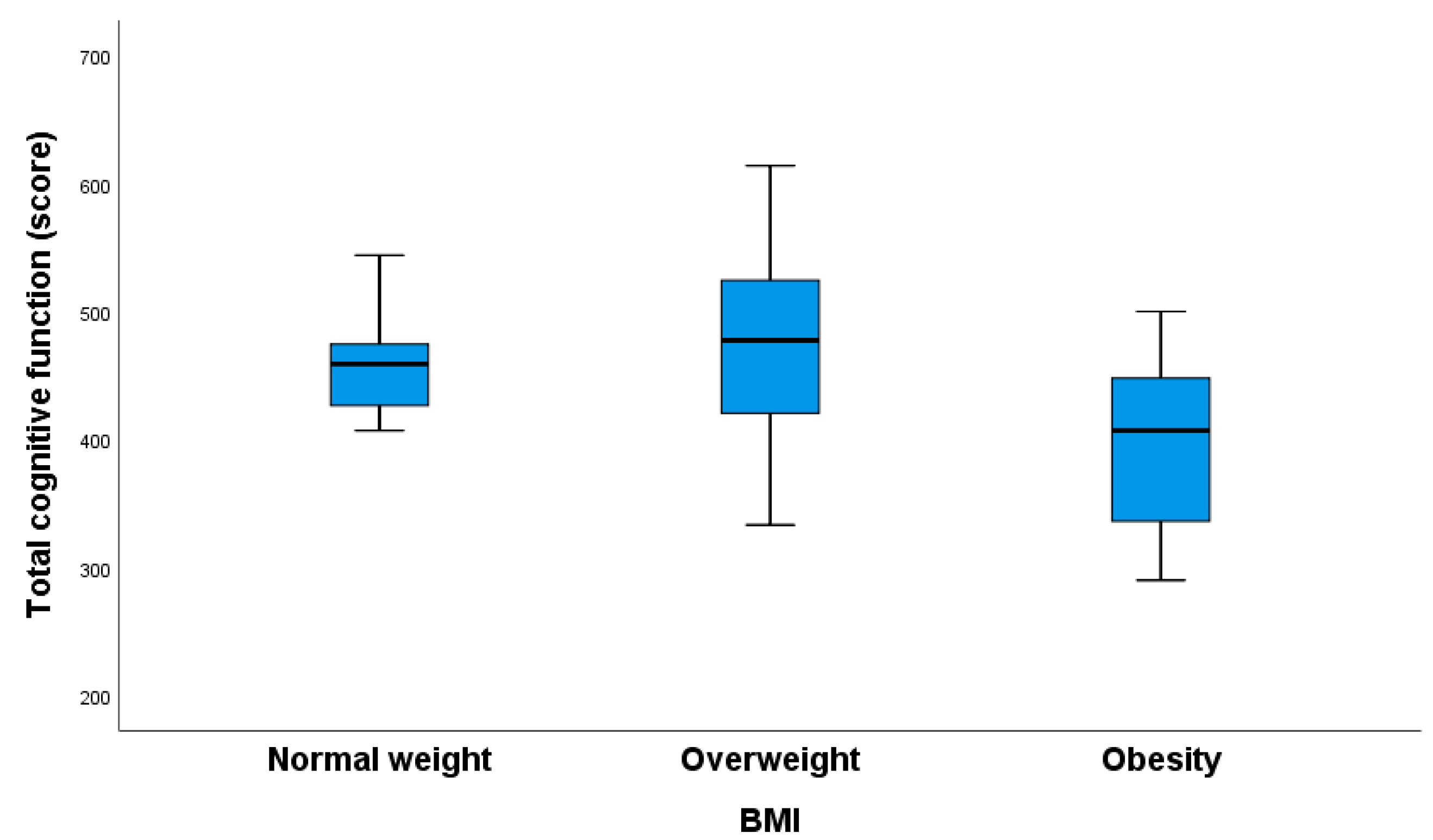
| Total CogniFit | BMI | −0.218 (−0.027; −0.001) | 0.078 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivanisevic, M.; Gasparovic, V.E.; Herman, M.; Delmis, J. Cognitive Function during and after Pregnancy and One-Year Postpartum in Type 1 Diabetes: A Longitudinal Study. Nutrients 2024, 16, 2751. https://doi.org/10.3390/nu16162751
Ivanisevic M, Gasparovic VE, Herman M, Delmis J. Cognitive Function during and after Pregnancy and One-Year Postpartum in Type 1 Diabetes: A Longitudinal Study. Nutrients. 2024; 16(16):2751. https://doi.org/10.3390/nu16162751
Chicago/Turabian StyleIvanisevic, Marina, Vesna Elvedji Gasparovic, Mislav Herman, and Josip Delmis. 2024. "Cognitive Function during and after Pregnancy and One-Year Postpartum in Type 1 Diabetes: A Longitudinal Study" Nutrients 16, no. 16: 2751. https://doi.org/10.3390/nu16162751
APA StyleIvanisevic, M., Gasparovic, V. E., Herman, M., & Delmis, J. (2024). Cognitive Function during and after Pregnancy and One-Year Postpartum in Type 1 Diabetes: A Longitudinal Study. Nutrients, 16(16), 2751. https://doi.org/10.3390/nu16162751