

Patterns of Dietary Supplement Use among GBT2Q Men and Non-Binary Individuals in Canada

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Questionnaire Development and Design
2.4. Statistical Analysis
3. Results
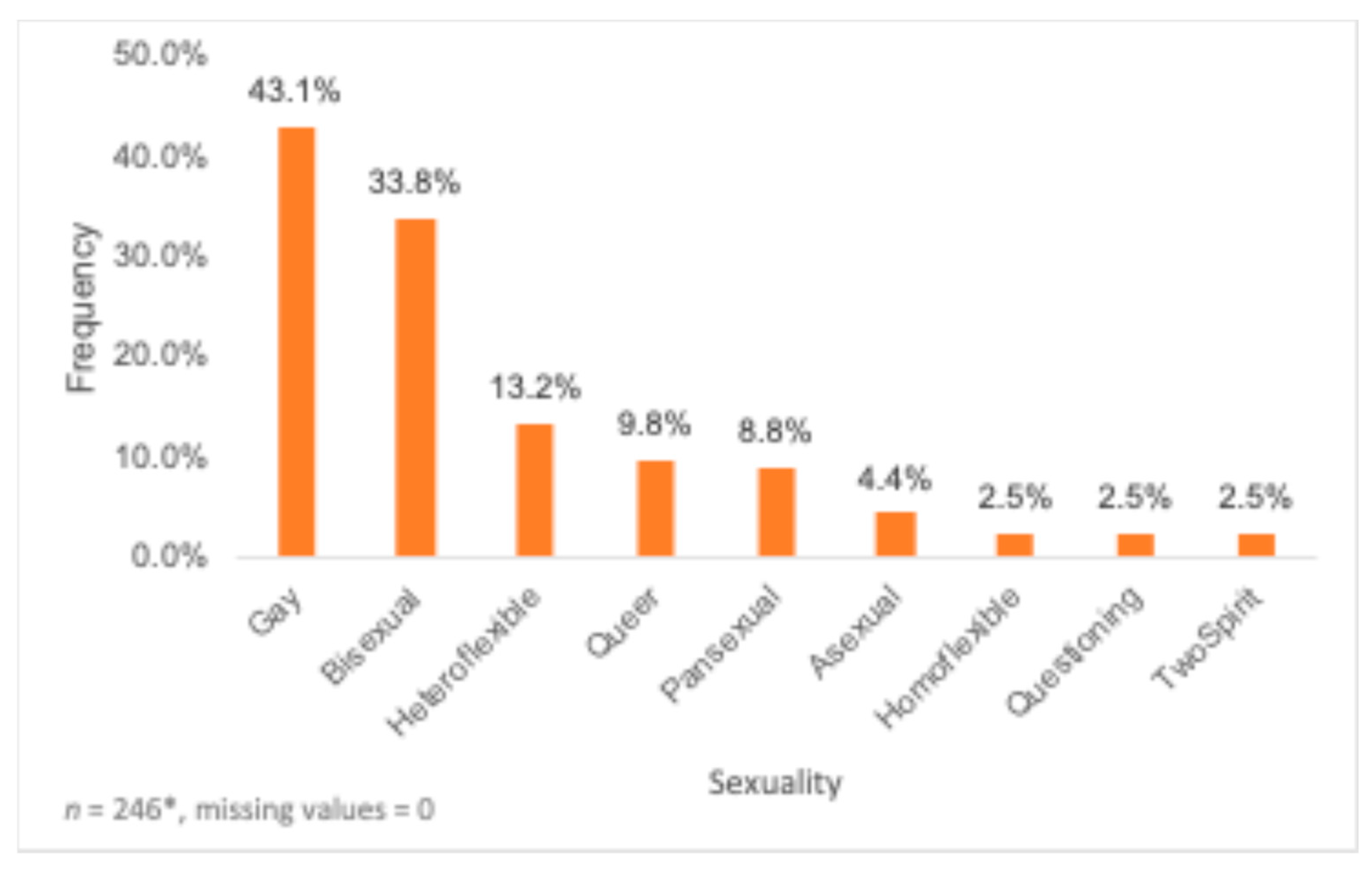
3.1. Characteristics of Participants
3.2. Types of Used Dietary Supplements
3.3. Reasons for Dietary Supplement Use
3.4. Source of Information
3.5. Predictors of Use of Dietary Supplements
3.6. Nutritional Labels and Negative Side Effects
3.7. Use of Non-Dietary Supplements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Health Canada, Government of Canada. About Natural Health Products. 2016. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/natural-non-prescription.html (accessed on 13 February 2023).
- Statistics Canada, Government of Canada. Health Fact Sheets: Use of Supplements, 2015. 2017. Available online: https://publications.gc.ca/collections/collection_2022/statcan/82-625-x/82-625-2017001-14831-eng.pdf (accessed on 14 January 2022).
- Temple, N.J. The Marketing of Dietary Supplements: A Canadian Perspective. Curr. Nutr. Rep. 2013, 2, 167–173. [Google Scholar] [CrossRef]
- Temple, N.J. The Regulation of Dietary Supplements in Canada: Many Promises but Little Progress. J. Diet. Suppl. 2017, 14, 117–120. [Google Scholar] [CrossRef]
- Calzo, J.P.; Sonneville, K.R.; Scherer, E.A.; Jackson, B.; Austin, S.B. Gender Conformity and Use of Laxatives and Muscle-Building Products in Adolescents and Young Adults. Pediatrics 2016, 138, e20154073. [Google Scholar] [CrossRef] [PubMed]
- Yager, Z.; O’Dea, J.A. Relationships between Body Image, Nutritional Supplement Use, and Attitudes towards Doping in Sport among Adolescent Boys: Implications for Prevention Programs. J. Int. Soc. Sports Nutr. 2014, 11, 13. [Google Scholar] [CrossRef]
- Strübel, J.; Petrie, T.A. Appearance and Performance Enhancing Drug Usage and Psychological Well-Being in Gay and Heterosexual Men. Psychol. Sex. 2019, 10, 132–148. [Google Scholar] [CrossRef]
- Maughan, R.J.; Shirreffs, S.M.; Vernec, A. Making Decisions About Supplement Use. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 212–219. [Google Scholar] [CrossRef]
- Foote, J.A.; Murphy, S.P.; Wilkens, L.R.; Hankin, J.H.; Henderson, B.E.; Kolonel, L.N. Factors Associated with Dietary Supplement Use among Healthy Adults of Five Ethnicities: The Multiethnic Cohort Study. Am. J. Epidemiol. 2003, 157, 888–897. [Google Scholar] [CrossRef]
- Li, J.; Li, X.; Gathirua-Mwangi, W.; Song, Y. Prevalence and Trends in Dietary Supplement Use among US Adults with Diabetes: The National Health and Nutrition Examination Surveys, 1999–2014. BMJ Open Diabetes Res. Care 2020, 8, e000925. [Google Scholar] [CrossRef]
- Roy, K.-A.; El Khoury, D.; Dwyer, J.J.M.; Mountjoy, M. Dietary Supplementation Practices among Varsity Athletes at a Canadian University. J. Diet. Suppl. 2021, 18, 614–629. [Google Scholar] [CrossRef]
- Griffiths, S.; Murray, S.B.; Touyz, S. Disordered Eating and the Muscular Ideal. J. Eat. Disord. 2013, 1, 15. [Google Scholar] [CrossRef]
- Brennan, D.J.; Asakura, K.; George, C.; Newman, P.A.; Giwa, S.; Hart, T.A.; Souleymanov, R.; Betancourt, G. “Never Reflected Anywhere”: Body Image among Ethnoracialized Gay and Bisexual Men. Body Image 2013, 10, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Calzo, J.P.; Blashill, A.J.; Brown, T.A.; Argenal, R.L. Eating Disorders and Disordered Weight and Shape Control Behaviors in Sexual Minority Populations. Curr. Psychiatry Rep. 2017, 19, 49. [Google Scholar] [CrossRef] [PubMed]
- McCreary, D.R.; Hildebrandt, T.B.; Heinberg, L.J.; Boroughs, M.; Thompson, J.K. A Review of Body Image Influences on Men’s Fitness Goals and Supplement Use. Am. J. Mens. Health 2007, 1, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; McGuire, F.H.; Lavender, J.M.; Brown, T.A.; Murray, S.B.; Compte, E.J.; Cattle, C.J.; Flentje, A.; Lubensky, M.E.; Obedin-Maliver, J.; et al. Appearance and Performance-Enhancing Drugs and Supplements (APEDS): Lifetime Use and Associations with Eating Disorder and Muscle Dysmorphia Symptoms among Cisgender Sexual Minority People. Eat. Behav. 2022, 44, 101595. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, M.C.; Moradi, B. Body Image and Eating Disorder Symptoms in Sexual Minority Men: A Test and Extension of Objectification Theory. J. Couns. Psychol. 2010, 57, 154–166. [Google Scholar] [CrossRef]
- Blashill, A.J.; Tomassilli, J.; Biello, K.; O’Cleirigh, C.; Safren, S.A.; Mayer, K.H. Body Dissatisfaction Among Sexual Minority Men: Psychological and Sexual Health Outcomes. Arch. Sex. Behav. 2016, 45, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Hadland, S.E.; Austin, S.B.; Goodenow, C.S.; Calzo, J.P. Weight Misperception and Unhealthy Weight Control Behaviors among Sexual Minorities in the General Adolescent Population. J. Adolesc. Health 2014, 54, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Badenes-Ribera, L.; Fabris, M.A.; Longobardi, C. The Relationship between Internalized Homonegativity and Body Image Concerns in Sexual Minority Men: A Meta-Analysis. Psychol. Sex 2018, 9, 251–268. [Google Scholar] [CrossRef]
- Filice, E.; Raffoul, A.; Meyer, S.B.; Neiterman, E. The Influence of Grindr, a Geosocial Networking Application, on Body Image in Gay, Bisexual and Other Men Who Have Sex with Men: An Exploratory Study. Body Image 2019, 31, 59–70. [Google Scholar] [CrossRef]
- Brennan, D.J.; Craig, S.L.; Thompson, D.E.A. Factors Associated with a Drive for Muscularity among Gay and Bisexual Men. Cult Health Sex 2012, 14, 1–15. [Google Scholar] [CrossRef]
- Ghaderi, A.; Welch, E. Appearance and Performance-Enhancing Drugs and Supplements, Eating Disorders Symptoms, Drive for Muscularity, and Sexual Orientation in a Sample of Young Men. Nutrients 2022, 14, 4920. [Google Scholar] [CrossRef]
- Grieve, F.G. A Conceptual Model of Factors Contributing to the Development of Muscle Dysmorphia. Eat. Disord. 2007, 15, 63–80. [Google Scholar] [CrossRef]
- Nhean, S.; Tseng, A.; Sheehan, N.L.; Bogoch, I.I. Use and Safety of Appearance and Performance Enhancing Supplements in Gay, Bisexual, and Other Men Who Have Sex with Men Receiving Daily Tenofovir Disoproxil Fumarate/Emtricitabine as HIV Pre-Exposure Prophylaxis. AIDS Care 2023, 35, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, S.; Murray, S.B.; Krug, I.; McLean, S.A. The Contribution of Social Media to Body Dissatisfaction, Eating Disorder Symptoms, and Anabolic Steroid Use among Sexual Minority Men. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 149–156. [Google Scholar] [CrossRef]
- Kaminski, P.L.; Chapman, B.P.; Haynes, S.D.; Own, L. Body Image, Eating Behaviors, and Attitudes toward Exercise among Gay and Straight Men. Eat. Behav. 2005, 6, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Tran, A.; Darboe, M.; Goyal, A.; Birk, N. Association between Dating App Use and Unhealthy Weight Control Behaviors and Muscle Enhancing Behaviors in Sexual Minority Men: A Cross-Sectional Study. BMC Public Health 2023, 23, 838. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, D.; Dwyer, J.J.M.; Fein, L.; Brauer, P.; Brennan, S.; Alfaro, I. Understanding the Use of Dietary Supplements among Athlete and Non-Athlete University Students: Development and Validation of a Questionnaire. Sports 2019, 7, 166. [Google Scholar] [CrossRef]
- El Khoury, D.; Hansen, J.; Tabakos, M.; Spriet, L.L.; Brauer, P. Dietary Supplement Use among Non-Athlete Students at a Canadian University: A Pilot-Survey. Nutrients 2020, 12, 2284. [Google Scholar] [CrossRef]
- Community-Based Research Centre (CBRC). Sex Now 2021, Online Survey—Full Questionnaire. Available online: https://www.cbrc.net/sex_now_2021_online_survey_full_questionnaire (accessed on 28 April 2023).
- Statistics Canada, Government of Canada. Use of Nutritional Supplements, Health Fact Sheets. 2017. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2017001/article/14831-eng.htm (accessed on 19 July 2023).
- Statistics Canada, Government of Canada. Vitamin B12 Status of Canadians, 2009 to 2011. 2012. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2012001/article/11731-eng.htm#:~:text=Vitamin%20B12%20sufficiency%20in%20Canadians,olds%20had%20sufficient%20vitamin%20B12 (accessed on 29 August 2023).
- Statistics Canada, Government of Canada. Vitamin C Status of Canadian Adults: Findings from the 2012/2013 Canadian Health Measures Survey. 2017. Available online: https://www150.statcan.gc.ca/n1/pub/82-003-x/2016005/article/14612-eng.htm#archived (accessed on 29 August 2023).
- Rodriguez, N.R.; DiMarco, N.M.; Langley, S. Position of the American Dietetic Association, dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Am. Diet. Assoc. 2009, 109, 509–527. [Google Scholar] [CrossRef]
- Kårlund, A.; Gómez-Gallego, C.; Turpeinen, A.M.; Palo-oja, O.-M.; El-Nezami, H.; Kolehmainen, M. Protein Supplements and Their Relation with Nutrition, Microbiota Composition and Health: Is More Protein Always Better for Sportspeople? Nutrients 2019, 11, 829. [Google Scholar] [CrossRef]
- Dascombe, B.J.; Karunaratna, M.; Cartoon, J.; Fergie, B.; Goodman, C. Nutritional Supplementation Habits and Perceptions of Elite Athletes within a State-Based Sporting Institute. J. Sci. Med. Sport 2010, 13, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Perkin, J.E.; Wilson, W.J.; Schuster, K.; Rodriguez, J.; Allen-Chabot, A. Prevalence of Nonvitamin, Nonmineral Supplement Usage among University Students. J. Am. Diet. Assoc. 2002, 102, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Lun, V.; Erdman, K.A.; Fung, T.S.; Reimer, R.A. Dietary Supplementation Practices in Canadian High-Performance Athletes. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, H.R.; Marriott, B.P.; Williams, C.; Judelson, D.A.; Glickman, E.L.; Geiselman, P.J.; Dotson, L.; Mahoney, C.R. Patterns of Dietary Supplement Use among College Students. Clin. Nutr. ESPEN 2015, 34, 976–985. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.R. Patients’ Perceptions and Use of Natural Health Products. Can. Pharm. J. 2018, 151, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Wiens, K.; Erdman, K.A.; Stadnyk, M.; Parnell, J.A. Dietary Supplement Usage, Motivation, and Education in Young, Canadian Athletes. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Joy, P.; Numer, M. Queering Educational Practices in Dietetics Training: A Critical Review of LGBTQ Inclusion Strategies. Can. J. Diet. Pract. Res. 2018, 79, 80–85. [Google Scholar] [CrossRef]
- Storozuk, A.; Ashley, M.; Delage, V.; Maloney, E.A. Got bots? practical recommendations to protect online survey data from BOT attacks. Quant. Methods Psychol. 2020, 16, 472–481. [Google Scholar] [CrossRef]
- El Khoury, D.; Tabakos, M.; Dwyer, J.J.M.; Mountjoy, M. Determinants of Supplementation among Canadian University Students: A Theory of Planned Behavior Perspective. J. Am. Coll. Health 2023, 71, 1957–1965. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Percentage | |
|---|---|---|
| Ethnicity | Arab (Saudi Arabian, Palestinian, Iraqi, etc.) | 1.5% |
| Black/African/Caribbean | 5.9% | |
| East/Southeast Asian (e.g., Chinese, Japanese, Korean, Vietnamese, Cambodian, Filipino, etc.) | 4.4% | |
| Indigenous (First Nations/Métis/Inuk) | 8.4% | |
| Latin American, Latina, Latino, Latinx, Latine (Costa Rican, Guatemalan, Brazilian, Columbian, etc.) | 1.5% | |
| Middle Eastern | 1.0% | |
| South Asian (East Indian, Sri Lankan, etc.) | 2.5% | |
| West Asian (Iranian, Afghani, etc.) | 0.5% | |
| White/European | 65.7% | |
| Mixed Ethnicity | 7.8% | |
| Dietitian visit in the last 6 months | Currently visits a dietitian | 53.4% |
| Has visited a dietitian in the past 6 months | 24.5% | |
| Has not visited a dietitian in the past 6 months | 21.1% | |
| Highest level of education | Did not finish high school | 2.0% |
| Apprenticeship training/trades | 5.4% | |
| Professional degree | 11.3% | |
| Highschool diploma | 20.6% | |
| Bachelor’s degree | 45.6% | |
| Master’s or doctorate degree | 13.7% | |
| Parent’s/guardian’s highest level of education | Did not finish high school | 3.9% |
| Apprenticeship training/trades | 7.4% | |
| Professional degree | 13.7% | |
| Highschool diploma | 29.4% | |
| Bachelor’s degree | 34.8% | |
| Master’s or doctorate degree | 9.3% | |
| Vitamins/Minerals | Proteins | Amino Acids | Carbohydrates | Stimulants/Energy Boosters | Non-Vitamin/Mineral Antioxidants | Fatty Acids | Herbs and Botanicals | Fat Burners/Weight Loss | |
|---|---|---|---|---|---|---|---|---|---|
| Yes | 92.2% (188) * | 84.3% (172) * | 69.1% (141) * | 77.5% (158) * | 62.3% (127) * | 52.0% (107) * | 65.2% (133) * | 66.7% (136) * | 64.7% (132) * |
| No | 7.8% (16) * | 15.7% (32) * | 30.9% (36) * | 22.6% (46) * | 37.3% (76) * | 46.1% (94) * | 32.8% (67) * | 33.3% (68) * | 34.8% (71) * |
| >1 week | 14.5% (27) * | 21.0% (36) * | 31.2% (44) * | 17.3% (27) * | 26.8% (34) * | 27.6% (29) * | 29.3% (39) * | 31.8% (43) * | 22.7% (30) * |
| 2–3 times/week | 41.4% (77) * | 49.7% (85) * | 52.5% (74) * | 55.1% (86) * | 46.5% (59) * | 47.6% (50) * | 47.3% (63) * | 48.1% (65) * | 48.5% (64) * |
| 4–5 times/weeks | 25.30 (47) * | 25.4% (36) * | 14.2% (20) * | 21.1% (33) * | 18.1% (23) * | 19.0% (20) * | 15.8% (21) * | 15.5% (21) * | 19.7% (26) * |
| <6 times/week | 18.8% (35) * | 8.20% (14) * | 2.1% (3) * | 6.4% (10) * | 8.7% (11) * | 5.7% (6) * | 7.5% (10) * | 4.4% (6) * | 9.1% (12) * |
| >1 month | 9.5% (18) * | 12.8% (22) * | 19.7% (28) * | 13.4% (21) * | 13.4% (17) * | 15.2% (16) * | 21.9% (29) * | 14.2% (19) * | 15.3% (20) * |
| 1–2 months | 33.3% (63) * | 35.5% (61) * | 45.1% (64) * | 31.2% (49) * | 37.8% (48) * | 43.8% (46) * | 31.1% (41) * | 40.3% (54) * | 41.2% (54) * |
| 3–5 months | 25.4% (48) * | 23.2% (40) * | 25.3% (36) * | 27.4% (43) * | 26.8% (34) * | 32.4% (34) * | 29.5% (39) * | 25.2% (34) * | 27.5% (36) * |
| <6 months | 31.7% (60) * | 28.5% (49) * | 9.9% (14) * | 28.0% (44) * | 22.0% (28) * | 8.6% (9) * | 17.4% (23) * | 20.1% (27) * | 16.0% (21) * |
| Non-Binary | Transman | Genderfluid | Man | Genderqueer | Cisgender | |
|---|---|---|---|---|---|---|
| Vitamin | 97.9% (0.118) | 100.0% (0.211) | 86.7% (0.357) | 94.4% (0.316) | 93.8% (0.795) | 85.7% (0.199) |
| Proteins | 83.0% (0.774) | 83.3% (0.905) | 86.7% (0.795) | 86.9% (0.283) | 90.6% (0.285) | 81.0% (0.655) |
| Amino acids | 63.8% (0.371) | 50.0% (0.066) | 86.7% (0.126) | 75.7% (0.033) * | 68.8% (0.961) | 57.10% (0.210) |
| Carbohydrates | 83.0% (0.082) | 66.7% (0.465) | 66.7% (0.534) | 79.4% (0.485) | 78.1% (0.091) | 52.4% (0.011) * |
| Stimulants/energy boosters | 68.1% (0.101) | 61.1% (0.944) | 20.0% (0.002) * | 66.4% (0.287) | 56.3% (0.658) | 23.8% (<0.001) * |
| Non-Vitamin/Mineral Antioxidants | 40.4% (0.167) | 44.4% (0.632) | 60.0% (0.762) | 62.6% (0.006) * | 50.0% (0.695) | 38.1% (0.281) |
| Fatty acids | 68.1% (0.878) | 61.1% (0.720) | 73.3% (0.715) | 71.0% (0.080) * | 62.5% (0.595) | 52.4% (0.272) |
| Herbs and botanicals | 57.4% (0.126) | 55.6% (0.295) | 73.3% (0.569) | 72.9% (0.047) * | 75.0% (0.276) | 61.9% (0.625) |
| Fat burners/weight loss | 61.7% (0.741) | 55.6% (0.644) | 73.3% (0.751) | 71.0% (0.072) | 71.9% (0.614) | 38.1% (0.022) * |
| Gay | Bisexual | Pansexual | Heteroflexible | Homoflexible | Queer | |
|---|---|---|---|---|---|---|
| Vitamin | 95.5% (0.181) | 95.7% (0.240) | 88.9% (0.522) | 92.6% (0.991) | 60.0% (0.005) * | 90.9% (0.633) |
| Proteins | 89.8% (0.062) | 87.0% (0.458) | 77.8% (0.425) | 85.2% (0.894) | 40.0% (0.006) * | 75.0% (0.228) |
| Amino acids | 70.5% (0.719) | 78.3% (0.043) * | 38.9% (0.004) * | 77.8% (0.296) | 100.0% (0.13) | 30.0% (<0.001) * |
| Carbohydrates | 75.0% (0.435) | 88.4% (0.026) * | 72.2% (0.795) | 77.8% (0.926) | 20.0% (0.007) * | 60.0% (0.121) |
| Stimulants/energy boosters | 61.4% (0.512) | 72.5% (0.086) | 44.4% (0.237) | 48.1% (0.231) | 0.0% (0.013) * | 35.0% (0.026) * |
| Non-Vitamin/Mineral Antioxidants | 53.4% (0.119) | 65.2% (0.022) * | 22.2% (0.018) * | 44.4% (0.486) | 40.0% (0.802) | 25.0% (0.023) * |
| Fatty acids | 58.0% (0.023) | 79.7% (0.005) * | 27.8% (<0.001) * | 74.1% (0.487) | 80.0% (0.767) | 40.0% (0.023) * |
| Herbs and botanicals | 68.2% (0.689) | 76.8% (0.028) * | 44.4% (0.036) * | 81.5% (0.080) | 40.0% (0.200) | 40.0% (0.008) * |
| Fat burners/weight loss | 69.3% (0.217) | 75.2% (0.216) | 33.3% (0.012) * | 70.4% (0.761) | 20.0% (0.099) | 40.0% (0.044) * |
| Model | B | S.E. * | Significance * | Exp(B) * | 95% CI for Exp(B) * | |
|---|---|---|---|---|---|---|
| Age vs. protein supplement use | 1.334 | 0.607 | 0.028 | 3.796 | 1.156 | 12.469 |
| Dietitian visit vs. vitamins use | −1.852 | 0.559 | <0.001 | 0.157 | 0.052 | 0.469 |
| Dietitian visit vs. carbohydrates use | −2.106 | 0.381 | <0.001 | 0.122 | 0.058 | 0.257 |
| Ethnicity vs. frequency of vitamin use | −0.625 | 0.278 | 0.024 | 0.535 | −1.170 | −0.081 |
| Dietitian visit vs. frequency of carbohydrate use | −1.830 | 0.334 | <0.001 | 0.160 | −2.485 | −1.175 |
| Ethnicity vs. length of vitamin use | −0.788 | 0.278 | 0.005 | 0.455 | −1.332 | −0.244 |
| Ethnicity vs. length of protein use | −0.681 | 0.275 | 0.013 | 0.506 | −1.219 | −0.143 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghazitabatabai, S.Y.; Zaid, M.; Forbes, L.; Davies, A.; Klassen, B.; Lachowsky, N.J.; El Khoury, D. Patterns of Dietary Supplement Use among GBT2Q Men and Non-Binary Individuals in Canada. Nutrients 2024, 16, 2678. https://doi.org/10.3390/nu16162678
Ghazitabatabai SY, Zaid M, Forbes L, Davies A, Klassen B, Lachowsky NJ, El Khoury D. Patterns of Dietary Supplement Use among GBT2Q Men and Non-Binary Individuals in Canada. Nutrients. 2024; 16(16):2678. https://doi.org/10.3390/nu16162678
Chicago/Turabian StyleGhazitabatabai, Seyedeh Yasaman, Manahil Zaid, Laura Forbes, Adam Davies, Ben Klassen, Nathan J. Lachowsky, and Dalia El Khoury. 2024. "Patterns of Dietary Supplement Use among GBT2Q Men and Non-Binary Individuals in Canada" Nutrients 16, no. 16: 2678. https://doi.org/10.3390/nu16162678
APA StyleGhazitabatabai, S. Y., Zaid, M., Forbes, L., Davies, A., Klassen, B., Lachowsky, N. J., & El Khoury, D. (2024). Patterns of Dietary Supplement Use among GBT2Q Men and Non-Binary Individuals in Canada. Nutrients, 16(16), 2678. https://doi.org/10.3390/nu16162678