1. Introduction
Type 1 diabetes mellitus (DMT-1) is a metabolic disorder, mainly of autoimmune origin, characterized by hyperglycemia caused by a complete lack of insulin secretion. Chronic hyperglycemia in DMT-1 can lead to long-term damage and dysfunction in multiple organs, especially the eyes, kidneys, nerves, heart, and blood vessels [
1]. As a result of chronic hyperglycemia, oxidative stress deteriorates further the damage to the aforementioned organs [
2]. Although optimal control of plasma glucose and lipid concentrations reduces the incidence of diabetes mellitus (DM) complications [
3], optimal glycemic control is quite difficult to achieve and maintain over time, especially in patients with DMT-1 due to hypoglycemia induced by incorrect insulin delivery [
4].
Moreover, the increasing cost of treating DM and its complications consists of a financial burden for many economies, whereas the quality of life of people with DM-related complications deteriorates, and life expectancy also decreases [
5,
6]. The total estimated cost of diagnosed diabetes in the USA in 2022 was
$412.9 billion [
7]. The high cost of DM therapies and their side effects have led to research into contemporary alternative treatments.
Several studies [
8,
9,
10] demonstrate the protective effect of a variety of antioxidant plant products against cell and tissue damage, such as the extract of saffron or
Crocus sativus L.
Crocus sativus L. is a bulbous and perennial plant with red stigmas and attached yellowish style [
10]. Its red stigmas, in dried form, is the spice commonly known as saffron or crocus which is produced mainly in Greece, Iran, and India [
11]. Saffron is characterized by its peculiar features, including its aromatic smell, bitter taste, and intense red color, and contains potential pharmacological active ingredients. Its bitter taste originates from picrocrocin, a,b-D-glucoside of hydroxyl-safranal. The chief components of stigma are crocetin, its glucosidic derivatives, safranal, picrocrocin, crocins and flavonoids like kaempferol and quercetin [
10]. The primary active ingredients are crocins (approximately 10% of the total content). High-quality saffron consists of approximately 30% crocins, 5–15% picrocrocin, and often 2.5% volatile compounds, one of which is safranal. Greek saffron, known as Greek red saffron, has the highest concentration of the above ingredients [
11].
Studies have shown that the saffron has antidiabetic and antioxidant effects [
12,
13,
14,
15,
16,
17,
18,
19]. Also, the possibilities of saffron in the treatment of hyperlipidemia, hypertension, atherosclerosis, and myocardial damage have been highlighted in experimental studies [
20,
21,
22,
23] and in systematic reviews [
11] and meta-analyses [
24,
25]. Previous systematic reviews on the impact of
Crocus sativus L. on metabolic profile in patients with DM or metabolic syndrome (MS) demonstrated implausible findings due to the low-quality clinical trials assessed. The available limited evidence (five studies with saffron 15–100 mg daily for 2–3 months, five studies with crocin 5–100 mg for 2–3 months) showed a potentially favorable effect of saffron in fasting blood glucose levels. Fourteen studies were included in the review, and individuals with DMT-1 were included in only one study [
11]. A more recent meta-analysis demonstrated improvements in fasting blood glucose (FBG) in the DMT-2 and prediabetes individuals and HbA1c only in the prediabetes individuals [
25]. Another meta-analysis in herbs and spices effectiveness in glycemic control in DMT-2 has shown that
Crocus sativus L. (five studies with saffron 15–400 mg daily (tablet or powder) for 2–3 months and two studies with crocin with 15 mg for 3 months) has significantly reduced fasting blood glucose in individuals with DMT-2 [
24].
Probiotics have shown promising results in improving metabolic health, especially in reducing body weight, fasting blood glucose, HbA1c, and insulin in people with DMT-2 [
26]. Although a recent randomized controlled trial (RCT) in children with DMT-1 has shown no effect in glycemic control when administering
L. rhamnosus and
B. lactis for 6 months [
27], evidence from a meta-analysis of RCTs shows that administration of two species of probiotics and more have a significant effect in reducing body weight and HbA1c in people with DMT-2 [
26]. Specifically,
B. lactis,
B. longum, and
L. rhamnosus can favor weight loss in people with DMT-2, whereas
B. breve,
B. longum, and
L. rhamnosus have shown a reduction in FBG and
B. breve,
B. lactis, and
B. longum reduce HbA1c significantly [
26].
To our knowledge, there is no study in the current literature to investigate the impact of saffron extract on the metabolic profile of individuals with DMT-1. However, because saffron is not marketed in our country as a stand-alone supplement but only in combination with probiotics and prebiotics, we decided to use this combination in our study. The aim of this randomized, double-blind placebo-controlled study was to evaluate the effectiveness of extract of Crocus sativus L. on the metabolic control in people with DMT-1 using glucose monitoring systems.
2. Materials and Methods
2.1. Protocol Registration
The study was registered in
clinicaltrials.gov with registration number NCT05933460. The study protocol was submitted and approved by the Bioethics Committee of the School of Medicine of the Aristotle University of Thessaloniki (protocol number 1.46-21/11/2018). The study follows the CONSORT statement for reporting and presenting the results of clinical trials (
Supplementary Materials). The study was conducted according to the principles of the Declaration of Helsinki [
28].
2.2. Sample Size Calculation
The sample size was calculated based on the assumption that the HbA1c at the end of the study will differ by 0.5% between groups with a statistical power of 80% and a statistical significance level of 0.05, 28 patients are required to be included in the study (14 patients in each group).
So far, clinical studies examining the effect of saffron and its components on patients [
29,
30,
31,
32] or healthy volunteers [
33,
34] had a varying sample size from 10 to 80 subjects.
2.3. Patients Recruitment
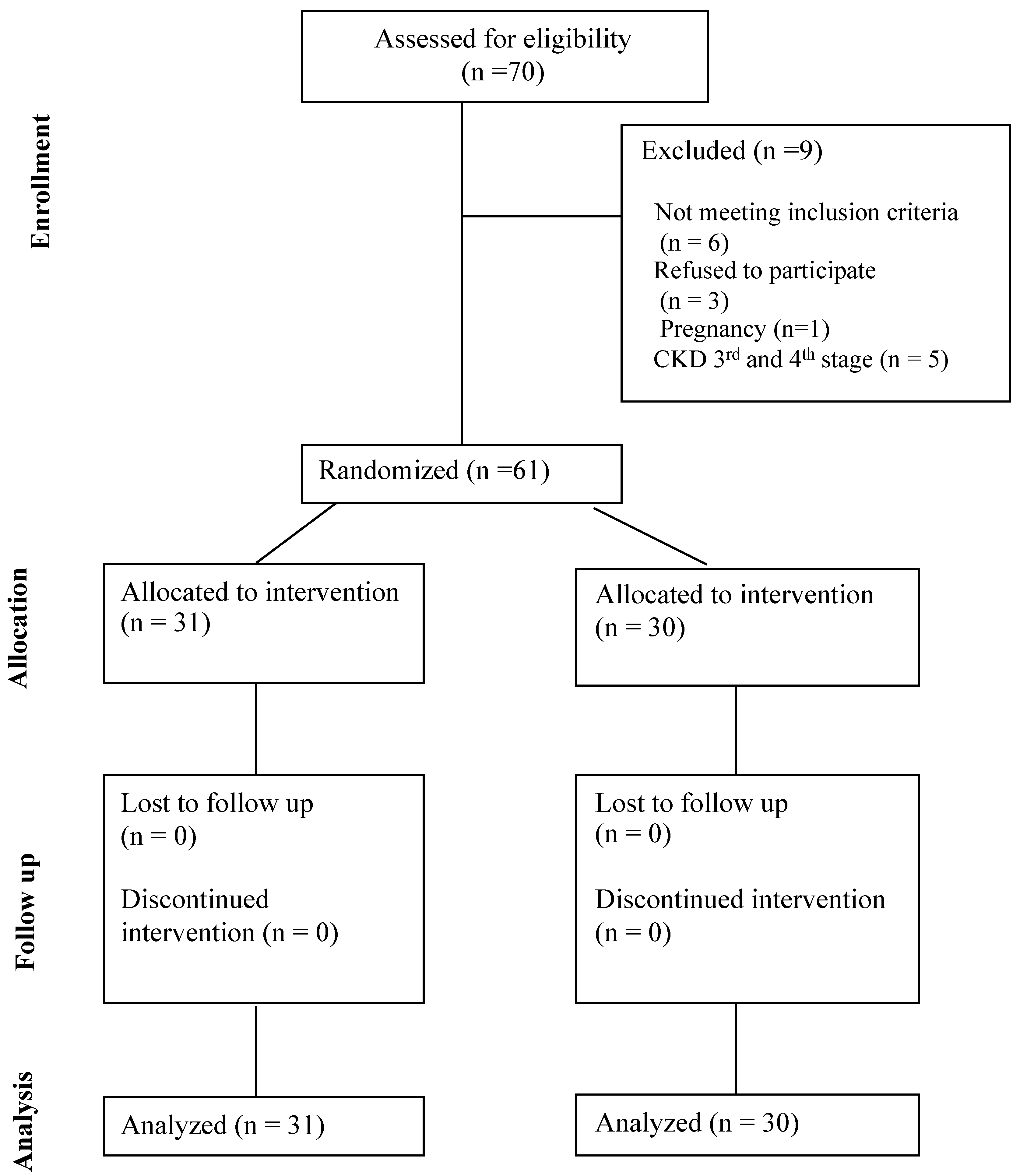
The study was conducted at the Diabetes outpatient clinic of the 1st Propaedeutic Department of Internal Medicine of the University General Hospital of Thessaloniki AHEPA from April 2022 to March 2023. Sixty-one adults with DMT-1, fulfilling the inclusion criteria, were enrolled according to the following inclusion and exclusion criteria.
Inclusion criteria included: (i) adults with DMT-1, (ii) diabetes duration > 12 months, (iii) their diabetes management treatment included Continuous Glucose Monitoring (CGM) or Intermittent Glucose Monitoring (either on Multiple Daily injections or continuous subcutaneous insulin infusion), and (iv) did not intend to change their diabetes therapy. Exclusion criteria were: (i) adults with DMT-2, (ii) adults with liver disease or impaired liver function, (iii) women with DMT-1 planning for pregnancy, pregnant or breastfeeding, (iv) adults with Chronic Kidney Disease with GFR < 60 mL/min/1.73 m2, (v) adults on antiplatelet treatment for non-preventive purposes, (vi) people on advanced hybrid closed loop treatment, (vii) adults with history of allergic reaction to Crocus sativus, (viii) adults with daily herbal consumption or taking daily multivitamin or probiotic and prebiotic supplements, (ix) adults that were unable to understand the study framework and consent to the trial.
2.4. Randomization and Allocation
The allocation and randomization sequences were performed using a table of random numbers that was produced by a computer-generated sequence in blocks of two. The randomization order and treatment allocation were concealed from the responsible researcher and statistician. All tests and measurements were performed by a physician and a dietitian blinded to the allocation of the participants. Supplement containers were administered by a third independent researcher who was unaware of the randomization sequence. Supplement containers were sequentially numbered, packed identically, and dispensed according to the allocation sequence. There were no dropouts, and all patients completed the study.
2.5. Intervention Details
People were informed about the trial procedures and signed an informed consent form. Individuals were randomized to receive a new oral supplement in sachets containing probiotics, prebiotics, Magnesium, and
Crocus sativus L. extract (LactoLevure ProbioMood; UNI-PHARMA S.A., Kifisia, Greece) or placebo daily for 6 months. The exact formulation of the product is presented in
Table 1.
Individuals were advised to take 3 sachets per day diluted in 200 mL water each, consisting of a total daily 84 mg Crocus sativus extract (3.5% bioactive ingredients such as crocin and safranal). Placebos were provided by the company in identical containers containing all ingredients without the Crocus sativus extract. Participants were obliged to return empty containers back for compliance purposes.
2.6. Antidiabetic and Concomitant Medication
All participants were using a continuous glucose monitoring system (Guardian™ Sensor 3, Medtronic, Dublin, Ireland) or intermittent glucose monitoring system (FreeStyle Libre, Abbott, Chicago, IL, USA) either on multiple daily injections (MDI) or continuous subcutaneous insulin infusion (CSII). Other comorbidities, diabetes complications, and concomitant medication were recorded as part of the participant’s medical history. Participants were stable throughout the study period and no change was required to their overall treatment regimen.
2.7. Data Collection—Measurements and Tests
All laboratory analyses were performed in the Biochemistry Laboratory of the University General Hospital of AHEPA. Primary outcomes were analyzed with the high-performance liquid chromatography (HPLC) method (for HbA1c) and enzymatic colorimetry (total cholesterol, HDL cholesterol, triglycerides, and fasting blood glucose). LDL cholesterol was calculated with the Friedewald equation [
35]. Primary outcomes are given in mg/dL. Blood pressure was measured in two consecutive measurements according to current guidelines [
36] and then averaged by an experienced physician.
In terms of secondary outcomes, fourteen days’ reports from continuous and intermittent glucose monitoring systems were downloaded both at baseline and at the end of the intervention. Anthropometric measurements (body weight, height, waist circumference) and body composition analysis with bioelectrical impedance (Bodystat 1500, Bodystat Ltd., Douglas, Isle of Man) were performed by an experienced dietitian at all-time points. Furthermore, a scored questionnaire regarding diabetes distress [
37,
38] was also employed to assess the feeling of disease distress at baseline and after six months of intervention, and a Subjective Satiety and Hunger Rating questionnaire [
39] was also used at the end of the intervention.
To neutralize diet and physical activity as the main confounders of the outcomes and ensure the reliability of our results, a weighted food diary of 2 weeks was documented to assess the nutritional intake, both at baseline and at the end of the intervention and analyzed. The food diary was crosschecked with the participant each time with a one-hour session by an experienced dietitian to validate the accuracy of the reporting. Dietary data analysis was performed with Genesis R&D (Version 9.10-2012, ESHA Research Inc., Salem, OR, USA), adapted for Greek food items. The energy and macronutrient intake were averaged and are presented as daily intake in the results. Along with the dietary data, the level of physical activity was assessed with the International Physical Activity Questionnaire (IPAQ) [
40] at baseline and after six months of intervention.
2.8. Statistical Analysis
Statistical analysis was performed using SPSS v.23 software (IBM Corp., Armonk, NY, USA, Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY, USA: IBM Corp.). Data were collected via a standardized form in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA, 2018. Microsoft Excel, Available at:
https://office.microsoft.com/excel (accessed on 25 April 2024)). Data were tested for normal distribution using Shapiro Wilk’s Shapiro test with a significance level of
p < 0.05. Data are presented with mean and standard deviation if normally distributed and with median and interquartile range if not normally distributed. Categorical data are presented as % frequencies. To test the difference between the 2 groups at baseline, the independent samples
t-test was used, while the paired samples
t-test was used to test the difference from baseline to the end of the intervention in each group. The independent samples
t-test was used to test the difference of the change from baseline to end of the intervention between the 2 groups, and Cohen’s d for effect size is also reported. The significance level for all statistical tests was set at 0.05.
4. Discussion
Our main findings show that at the end of the intervention, the two groups differed significantly only in serum triglycerides. In the active group, after 6 months of treatment, glycated hemoglobin was significantly reduced, as well as serum triglycerides.
The other primary outcomes did not differ significantly between and within the groups from baseline to the end of the intervention. No changes were observed in anthropometric measurements, physical activity, diet, and other biomarkers that could affect the results. Diabetes distress score improved significantly only in the active group (
p = 0.044), suggesting an overall improvement in diabetes disease burden in these individuals, but that was not significantly different enough between the two groups. Thus, from the above, we can consider that the improvement in glycated hemoglobin, serum triglycerides, and diabetes distress score observed in the intervention group is mainly due to the intake of the supplement. Glycemia, reported by CGM data, did not demonstrate any difference within or between the two groups at baseline and at the end of the intervention. However, CGM data represent only two weeks’ glycemic control at baseline and end of intervention and may not fully reflect HbA1c values. This is supported in a recent study by Tozzo et al., where it is shown that longer periods of CGM data correspond more accurately to the average glycemia from HbA1c values since longer periods of CGM data (>26 days) and missing data <10% reduce sensor bias and enhance CGM data accuracy [
41].
Our findings are partially in agreement with evidence from recent meta-analyses that saffron has a favorable effect on the glycemic control of individuals with DM. Saffron has shown effectiveness in reducing FBG in individuals with DMT-2 and prediabetes [
24,
25,
42] and in reducing HbA1c only in prediabetes individuals [
25], whereas in a meta-analysis by Asbaghi et al. [
43] did not show any significant effect in FBG. The same meta-analysis (6 studies) that took into consideration individuals with and without DMT-2 showed that saffron supplementation produced a significant reduction in triglycerides and total cholesterol and increased HDL levels but had a non-significant effect on LDL cholesterol [
43]. In individuals with DMT-2, 100 mg/day of saffron for 8 weeks significantly reduced triglycerides, atherogenic index, FBG, and insulin but not HbA1c and other lipid parameters [
42]. In this present study, saffron improved HbA1c and decreased serum triglycerides in the active group after 6 months but did not have any improvement in the FBG. It is worth mentioning that the difference in serum triglycerides was also significant between groups and not only within the active group. Of note, the present study is conducted in individuals with DMT-1 whereas all other available studies in the literature are conducted in individuals with DMT-2 or prediabetes [
11,
24,
25,
43].
Available evidence suggests that the concentration and combination of the components of saffron inhibit mechanistic pathways more synergistically than its individual bioactive compounds, suggesting the use of the saffron as a combination and not as sole compounds (e.g., crocin or safranal). Rahmani et al. [
44] showed that there is a linear dose-dependent relationship between the dose of saffron (mg/d), triglycerides, and cholesterol. Saffron has been proposed for acting hypotensive, hypolipidemic, and antidiabetic through several pathways. Saffron is considered to decrease systolic blood pressure through its vasomodulating effects and anti-inflammatory effects. Hypotensive effects also can be attributed to the blocking of calcium channels and possible interaction with endothelial nitric oxide (NO) [
45]. One possible lipid-lowering mechanism is through the reduction of lipid peroxidation factors such as malondialdehyde (MDA) by increasing the action and expression of antioxidant enzymes (such as glutathione reductase activity, superoxide of dismutase and others), preventing phosphorylation of certain protein kinases (e.g., I kappa B kinase-a (IKK) and AMP-activated protein kinase (AMPK)) and reducing the production of reactive oxygen species (ROS) [
46]. Another possible mechanism is regulating the expression of growth factors such as tumor necrosis factor-α, adiponectin, and leptin in adipose tissue or fat mass [
47]. Potential mechanisms of the effect on the lipid profile may be a potential inhibitory action of saffron and its bioactive ingredients on pancreatic lipase, antioxidant action, increase in the levels of adiponectin, activation of peroxisome proliferator-activated receptor alpha (PPAR-α) and modulation of heat shock proteins [
48]. One of the possible mechanisms of the beneficial action of saffron in metabolic control is the antioxidant aspect. Evidence in experimental studies shows that crocin can reduce oxidative stress by decreasing MDA and increasing glutathione [
49]. DM is a metabolic disorder that presents with increased oxidative stress due to chronic hyperglycemia [
50]. Therefore, we consider that saffron exerts an antioxidant beneficial action in the DM pathway. Also, its antidiabetic action is through the reduction of blood glucose by amplifying glucose uptake into cells, improving insulin signaling in insulin-sensitive tissues (adipose tissue and muscle) and increasing glucose transporter type 4 (GLUT-4) into the cell membranes. These hypoglycemic effects are shown by enhancing GLUT4 translocation into the plasma membrane via the AMPK/ACC pathway [
17,
51]. Saffron increases antioxidant enzymes (function) reduces ROS production by interfering with ROS-related pathways, thus reduces oxidative stress [
46].
Our study has several strengths. To our knowledge, this is the first double-blind, randomized clinical trial investigating the impact of Crocus sativus L. extract in people with DMT-1. It is of high importance that the supplement used was a standardized formulation and that the titration of saffron extract was known. It is also worth mentioning that the supplement used was well accepted and tolerated by our study participants. Of note, our glycemic findings are more robust due to continuous glucose monitoring both at baseline and end of intervention. Study duration was one of the major strengths, as all other similar studies have shorter intervention times. The study design was rigorous to ensure compliance and avoid confounding parameters during the intervention through close monitoring of patients and diligent dietary intake capture. Physical activity level assessment at both time points also provided credibility to our findings to ensure that any arising changes are not attributed to physical activity changes.
Our study also has limitations. Glucose monitoring data reflected only two weeks’ glycemic control at baseline and end of intervention. Presumably, collecting data for a longer period of time would be more efficient in understanding and confirming the improvement in glycemic control demonstrated with the HbA1c. Of note, the quantity of saffron extract used, may be insufficient to demonstrate efficacy to other biomarkers. However, we aimed to use a commercial supplement with a standardized formulation to ensure the bioactive ingredients’ proper delivery (bioavailability). Lastly, some differences in dietary intake may have resulted from reporting bias, and we should have aimed to have dietary intake documentation throughout the 6 month period. However, we decided to avoid burdening our participants with more reporting tasks for the study to ensure compliance with the protocol.
Future research should focus on evolving delivery of the saffron bioactives through supplements and developing supplements with a higher proportion of these bioactives. Also, more randomized controlled studies with a more extended period of time need to be conducted in individuals with either DMT-1 or DMT-2 to explore the full potential and safety of saffron supplementation in DM. Should discuss the results and how they can be interpreted from the perspective of previous studies and the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.


 ,
, 



{kind=link}