
Evidence and Perspectives for Choline Supplementation during Parenteral Nutrition—A Narrative Review

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
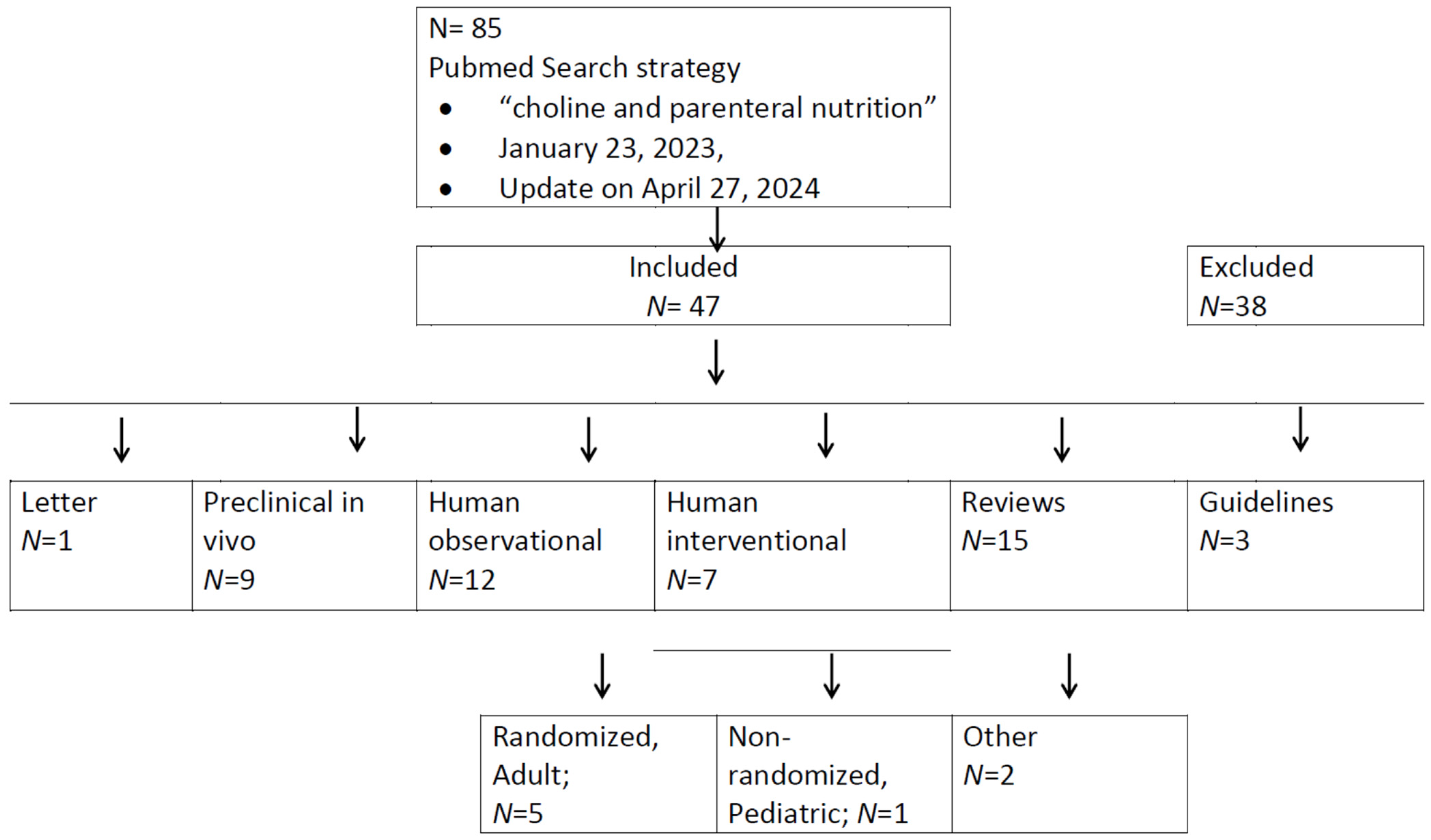
2. Materials and Methods
3. Results
3.1. A Letter to the Editor
3.2. Preclinical Studies
3.3. Observational Studies in Humans
3.4. Interventional Studies in Humans
3.5. Reviews
3.6. Guidelines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Beck, S.; Wojdyla, D.; Say, L.; Betran, A.P.; Merialdi, M.; Requejo, J.H.; Rubens, C.; Menon, R.; Van Look, P.F. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull. World Health Organ. 2010, 88, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Poets, C.F.; Wallwiener, D.; Vetter, K. Risks associated with delivering infants 2 to 6 weeks before term—A review of recent data. Dtsch. Ärzteblatt Int. 2012, 109, 721–726. [Google Scholar]
- Tsimis, M.E.; Abu Al-Hamayel, N.; Germaine, H.; Burd, I. Prematurity: Present and future. Minerva Ginecol. 2015, 67, 35–46. [Google Scholar] [PubMed]
- Tucker, J.; McGuire, W. Epidemiology of preterm birth. BMJ 2004, 329, 675–678. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922, Erratum in: Lancet 2019, 393, e44. [Google Scholar]
- Vaidya, R.; Yi, J.X.; O’Shea, T.M.; Jensen, E.T.; Joseph, R.M.; Shenberger, J.; Gogcu, S.; Wagner, K.; Msall, M.E.; Thompson, A.L.; et al. ELGAN-ECHO Study Investigators. Long-Term Outcome of Necrotizing Enterocolitis and Spontaneous Intestinal Perforation. Pediatrics 2022, 150, e2022056445. [Google Scholar] [CrossRef] [PubMed]
- Wendel, K.; Aas, M.; Gunnarsdottir, G.; Rossholt, M.; Bratlie, M.; Nordvik, T.; Landsend, E.; Fugelseth, D.; Domellöf, M.; Pripp, A.; et al. Effect of arachidonic and docosahexaenoic acid supplementation on respiratory outcomes and neonatal morbidities in preterm infants. Clin. Nutr. 2022, 42, 22–28. [Google Scholar] [CrossRef]
- Lockman, P.R.; Allen, D.D. The transport of choline. Drug Dev. Ind. Pharm. 2002, 28, 749–771. [Google Scholar] [CrossRef] [PubMed]
- Hollenbeck, C.B. An introduction to the nutrition and metabolism of choline. Cent. Nerv. Syst. Agents Med. Chem. 2012, 12, 100–113. [Google Scholar] [CrossRef]
- Bernhard, W.; Raith, M.; Shunova, A.; Lorenz, S.; Böckmann, K.; Minarski, M.; Poets, C.F.; Franz, A.R. Choline Kinetics in Neonatal Liver, Brain and Lung-Lessons from a Rodent Model for Neonatal Care. Nutrients 2022, 14, 720. [Google Scholar] [CrossRef]
- Grothe, J.; Riethmüller, J.; Tschürtz, S.M.; Raith, M.; Pynn, C.J.; Stoll, D.; Bernhard, W. Plasma phosphatidylcholine alterations in cystic fibrosis patients: Impaired metabolism and correlation with lung function and inflammation. Cell. Physiol. Biochem. 2015, 35, 1437–1453. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W.; Pynn, C.J.; Jaworski, A.; Rau, G.A.; Hohlfeld, J.M.; Freihorst, J.; Poets, C.F.; Stoll, D.; Postle, A.D. Mass spectrometric analysis of surfactant metabolism in human volunteers using deuteriated choline. Am. J. Respir. Crit. Care Med. 2004, 170, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W.; Poets, C.F.; Franz, A.R. Choline and choline-related nutrients in regular and preterm infant growth. Eur. J. Nutr. 2019, 58, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W.; Böckmann, K.; Maas, C.; Mathes, M.; Hövelmann, J.; Shunova, A.; Hund, V.; Schleicher, E.; Poets, C.F.; Franz, A.R. Combined choline and DHA supplementation: A randomized controlled trial. Eur. J. Nutr. 2020, 59, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S. Choline, Other Methyl-Donors and Epigenetics. Nutrients 2017, 9, 445. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S.H. Choline: Critical role during fetal development and dietary requirements in adults. Annu. Rev. Nutr. 2006, 26, 229–250. [Google Scholar] [CrossRef]
- Canty, D.J.; Zeisel, S.H. Lecithin and choline in human health and disease. Nutr. Rev. 1994, 52, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W.; Raith, M.; Kunze, R.; Koch, V.; Heni, M.; Maas, C.; Abele, H.; Poets, C.F.; Franz, A.R. Choline concentrations are lower in postnatal plasma of preterm infants than in cord plasma. Eur. J. Nutr. 2015, 54, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Wiechers, C.; Avellina, V.; Luger, B.; Böckmann, K.; Minarski, M.; Maas, C.; Bernhard, W.; Poets, C.F.; Franz, A.R. Body Composition of Preterm Infants following Rapid Transition to Enteral Feeding. Neonatology 2022, 119, 246–254. [Google Scholar] [CrossRef]
- National Academy of Sciences. Dietary Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and Its Panel on Folate, Other B Vitamins, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press: Washington, DC, USA, 1998. [Google Scholar] [PubMed]
- EFSA Panel on Dietetic Products; Nutrition and Allergies (NDA). Dietary Reference Values for choline. EFSA J. 2016, 14, 4484. [Google Scholar] [CrossRef]
- EFSA Panel on Nutrition; Novel Foods and Food allergens (NDA); Turck, D.; Bohn, T.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; et al. Choline and contribution to normal liver function of the foetus and exclusively breastfed infants: Evaluation of a health claim pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA J. 2023, 21, 8115. [Google Scholar]
- Hojsak, I.; Colomb, V.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hulst, J.M.; ESPGHAN Committee on Nutrition. ESPGHAN Committee on Nutrition Position Paper. Intravenous Lipid Emulsions and Risk of Hepatotoxicity in Infants and Children: A Systematic Review and Meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 776–792. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.J.; Lapillonne, A.; Bronsky, J.; Domellof, M.; Embleton, N.; Iacobelli, S.; Jochum, F.; Joosten, K.; Kolacek, S.; Mihatsch, W.A.; et al. Research priorities in pediatric parenteral nutrition: A consensus and perspective from ESPGHAN/ESPEN/ESPR/CSPEN. Pediatr. Res. 2022, 92, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, V.; Capozza, M.; Panza, R.; Laforgia, N.; Baldassarre, M.E. Macronutrients and Micronutrients in Parenteral Nutrition for Preterm Newborns: A Narrative Review. Nutrients 2022, 14, 1530. [Google Scholar] [CrossRef] [PubMed]
- Vanek, V.W.; Borum, P.; Buchman, A.; Fessler, T.A.; Howard, L.; Jeejeebhoy, K.; Kochevar, M.; Shenkin, A.; Valentine, C.J.; Novel Nutrient Task Force, Parenteral Multi-Vitamin and Multi–Trace Element Working Group, American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors. A.S.P.E.N. position paper: Recommendations for changes in commercially available parenteral multivitamin and multi-trace element products. Nutr. Clin. Pract. 2012, 27, 440–491. [Google Scholar] [PubMed]
- Drenckpohl, D.C.; Christifano, D.N.; Carlson, S.E. Is choline deficiency an unrecognized factor in necrotizing enterocolitis of preterm infants? Pediatr. Res. 2024; published online ahead of print on April 24th 2024. [Google Scholar] [CrossRef] [PubMed]
- Burt, M.E.; Hanin, I.; Brennan, M.F. Choline deficiency associated with total parenteral nutrition. Lancet 1980, 2, 638–639. [Google Scholar] [CrossRef]
- Hall, R.I.; Ross, L.H.; Bozovic, M.G.; Grant, J.P. The effect of choline supplementation on hepatic steatosis in the parenterally fed rat. JPEN J. Parenter. Enter. Nutr. 1985, 9, 597–599. [Google Scholar] [CrossRef] [PubMed]
- Morán Penco, J.M.; Maciá Botejara, E.; Salas Martinez, J.; Mahedero Ruiz, G.; Climent Mata, V.; Saenz de Santamaria, J.; Vinagre Velasco, L.M. Liver lipid composition and intravenous.; intraperitoneal.; and enteral administration of intralipid. Nutrition 1994, 10, 26–31. [Google Scholar]
- Buchman, A.L.; Jenden, D.J.; Moukarzel, A.A.; Roch, M.; Rice, K.M.; Chang, A.S.; Ament, M.E. Choline pharmacokinetics during intermittent intravenous choline infusion in human subjects. Clin. Pharmacol. Ther. 1994, 55, 277–283. [Google Scholar] [CrossRef]
- Narkewicz, M.R.; Caldwell, S.; Jones, G. Cysteine supplementation and reduction of total parenteral nutrition-induced hepatic lipid accumulation in the weanling rat. J. Pediatr. Gastroenterol. Nutr. 1995, 21, 18–24. [Google Scholar] [PubMed]
- Oz, H.S.; Im, H.J.; Chen, T.S.; de Villiers, W.J.; McClain, C.J. Glutathione-enhancing agents protect against steatohepatitis in a dietary model. J. Biochem. Mol. Toxicol. 2006, 20, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wu, Y.; Guo, Y.; Tang, Q.; Lu, T.; Cai, W.; Huang, H. Choline Alleviates Parenteral Nutrition-Associated Duodenal Motility Disorder in Infant Rats. JPEN J. Parenter. Enter. Nutr. 2016, 40, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Lu, T.; Chen, F.; Yan, J.; Chen, F.; Zhang, Q.; Wang, J.; Yan, W.; Yu, T.; Tang, Q.; et al. Choline Protects Against Intestinal Failure-Associated Liver Disease in Parenteral Nutrition-Fed Immature Rats. JPEN J. Parenter. Enteral Nutr. 2018, 42, 436–445, Erratum in: JPEN J Parenter Enteral Nutr. 2018, 42, 490. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.K.; Zhu, J.; Gong, Z.Z.; Wen, J.; Xiao, Y.T.; Zhang, T.; Cai, W. Supplementary choline attenuates olive oil lipid emulsion-induced enterocyte apoptosis through suppression of CELF1/AIF pathway. J. Cell Mol. Med. 2018, 22, 1562–1573. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Yang, J.; Mamtawla, G.; Zhang, L.; Gao, X.; Wang, X. Differential Metabolomic Analysis of Liver Tissues from Rat Models of Parenteral Nutrition-Associated Liver Disease. Biomed. Res. Int. 2020, 2020, 9156359. [Google Scholar] [CrossRef] [PubMed]
- Chawla, R.K.; Berry, C.J.; Kutner, M.H.; Rudman, D. Plasma concentrations of transsulfuration pathway products during nasoenteral and intravenous hyperalimentation of malnourished patients. Am. J. Clin. Nutr. 1985, 42, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Sheard, N.F.; Tayek, J.A.; Bistrian, B.R.; Blackburn, G.L.; Zeisel, S.H. Plasma choline concentration in humans fed parenterally. Am. J. Clin. Nutr. 1986, 43, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L.; Moukarzel, A.; Jenden, D.J.; Roch, M.; Rice, K.; Ament, M.E. Low plasma free choline is prevalent in patients receiving long term parenteral nutrition and is associated with hepatic aminotransferase abnormalities. Clin. Nutr. 1993, 12, 33–37. [Google Scholar] [CrossRef]
- Maherzi, A.; Vatier, J.; Cezard, J.P.; Ferkdadji, L.; Duet, M.; Celice-Pinguaud, C.; Peuchmaur, M.; Navarro, J. Characteristics and consequences of duodenogastric reflux in children on total parenteral nutrition (TPN) for severe gastrointestinal disorders. Clin. Nutr. 1994, 13, 345–350. [Google Scholar] [CrossRef]
- Misra, S.; Ahn, C.; Ament, M.E.; Choi, H.J.; Jenden, D.J.; Roch, M.; Buchman, A.L. Plasma choline concentrations in children requiring long-term home parenteral nutrition: A case control study. JPEN J. Parenter. Enter. Nutr. 1999, 23, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L.; Sohel, M.; Moukarzel, A.; Bryant, D.; Schanler, R.; Awal, M.; Burns, P.; Dorman, K.; Belfort, M.; Jenden, D.J.; et al. Plasma choline in normal newborns, infants, toddlers, and in very-low-birth-weight neonates requiring total parenteral nutrition. Nutrition 2001, 17, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.W.; Kinosian, B.P.; Stoner, N.E.; Lentine, D.C.; Buzby, G.P. Choline and vitamin B12 deficiencies are interrelated in folate-replete long-term total parenteral nutrition patients. J. Parenter. Enter. Nutr. 2002, 26, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L.; Ament, M.E.; Jenden, D.J.; Ahn, C. Choline deficiency is associated with increased risk for venous catheter thrombosis. J. Parenter. Enter. Nutr. 2006, 30, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Sentongo, T.A.; Kumar, P.; Karza, K.; Keys, L.; Iyer, K.; Buchman, A.L. Whole-blood-free choline and choline metabolites in infants who require chronic parenteral nutrition therapy. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Goss, K.C.W.; Goss, V.M.; Townsend, J.P.; Koster, G.; Clark, H.W.; Postle, A.D. Postnatal adaptations of phosphatidylcholine metabolism in extremely preterm infants: Implications for choline and PUFA metabolism. Am. J. Clin. Nutr. 2020, 112, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.K.; Pedersen, A.; Malmodin, D.; Lund, A.M.; Hellgren, G.; Löfqvist, C.; Pupp, I.H.; Hellström, A. Serum choline in extremely preterm infants declines with increasing parenteral nutrition. Eur. J. Nutr. 2021, 60, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Tayek, J.A.; Bistrian, B.; Sheard, N.F.; Zeisel, S.H.; Blackburn, G.L. Abnormal liver function in malnourished patients receiving total parenteral nutrition: A prospective randomized study. J. Am. Coll. Nutr. 1990, 9, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L.; Dubin, M.; Jenden, D.; Moukarzel, A.; Roch, M.H.; Rice, K.; Gornbein, J.; Ament, M.E.; Eckhert, C.D. Lecithin increases plasma free choline and decreases hepatic steatosis in long-term total parenteral nutrition patients. Gastroenterology 1992, 102, 1363–1370. [Google Scholar] [CrossRef]
- Demetriou, A.A. Lecithin increases plasma free choline and decreases hepatic steatosis in long-term total parenteral nutrition patients. J. Parenter. Enter. Nutr. 1992, 16, 487–488. [Google Scholar] [CrossRef]
- Buchman, A.L.; Dubin, M.D.; Moukarzel, A.A.; Jenden, D.J.; Roch, M.; Rice, K.M.; Gornbein, J.; Ament, M.E. Choline deficiency: A cause of hepatic steatosis during parenteral nutrition that can be reversed with intravenous choline supplementation. Hepatology 1995, 22, 1399–1403. [Google Scholar] [PubMed]
- Buchman, A.L.; Ament, M.E.; Sohel, M.; Dubin, M.; Jenden, D.J.; Roch, M.; Pownall, H.; Farley, W.; Awal, M.; Ahn, C. Choline deficiency causes reversible hepatic abnormalities in patients receiving parenteral nutrition: Proof of a human choline requirement: A placebo-controlled trial. J. Parenter. Enter. Nutr. 2001, 25, 260–268. [Google Scholar] [CrossRef]
- Buchman, A.L.; Sohel, M.; Brown, M.; Jenden, D.J.; Ahn, C.; Roch, M.; Brawley, T.L. Verbal and visual memory improve after choline supplementation in long-term total parenteral nutrition: A pilot study. J. Parenter. Enter. Nutr. 2001, 25, 30–35. [Google Scholar] [CrossRef] [PubMed]
- da Costa, K.A.; Niculescu, M.D.; Craciunescu, C.N.; Fischer, L.M.; Zeisel, S.H. Choline deficiency increases lymphocyte apoptosis and DNA damage in humans. Am. J. Clin. Nutr. 2006, 84, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Guerrerio, A.L.; Mattis, L.; Conner, K.G.; Hampsey, J.; Stasinopoulos, D.M.; DeJong, R.; Boctor, E.M.; Sheth, S.; Hamper, U.M.; Scheimann, A.O. Oral choline supplementation in children with intestinal failure. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Rudman, D.; Williams, P.J. Nutrient deficiencies during total parenteral nutrition. Nutr. Rev. 1985, 43, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Shronts, E.P. Essential nature of choline with implications for total parenteral nutrition. J. Am. Diet. Assoc. 1997, 97, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L. Choline deficiency during parenteral nutrition in humans. Nutr. Clin. Pract. 2003, 18, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Kitchen, P.; Forbes, A. Parenteral nutrition. Curr. Opin. Gastroenterol. 2003, 19, 144–147. [Google Scholar] [CrossRef]
- Kelly, D.A. Intestinal failure-associated liver disease: What do we know today? Gastroenterology 2006, 130, S70–S77. [Google Scholar] [CrossRef]
- Kumpf, V.J. Parenteral nutrition-associated liver disease in adult and pediatric patients. Nutr. Clin. Pract. 2006, 21, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.L. The addition of choline to parenteral nutrition. Gastroenterology 2009, 137, S119–S128. [Google Scholar] [CrossRef] [PubMed]
- Corbin, K.D.; Zeisel, S.H. Choline metabolism provides novel insights into nonalcoholic fatty liver disease and its progression. Curr. Opin. Gastroenterol. 2012, 28, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.W.; Li, Y.S. Pathogenesis and treatment of parenteral nutrition-associated liver disease. Hepatobiliary Pancreat. Dis. Int. 2012, 11, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Reid, D.T.; Eksteen, B. Murine models provide insight to the development of non-alcoholic fatty liver disease. Nutr. Res. Rev. 2015, 28, 133–142. [Google Scholar] [CrossRef]
- Cahova, M.; Bratova, M.; Wohl, P. Parenteral Nutrition-Associated Liver Disease: The Role of the Gut Microbiota. Nutrients 2017, 9, 987. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, S.B.; Mayr, J.A. Choline-related-inherited metabolic diseases-A mini review. J. Inherit. Metab. Dis. 2019, 42, 237–242, Erratum in: J. Inherit. Metab. Dis. 2020, 43, 156. [Google Scholar] [CrossRef] [PubMed]
- Vanek, V.W.; Borum, P.; Buchman, A.; Fessler, T.A.; Howard, L.; Shenkin, A.; Novel Nutrient Task Force, Parenteral Vitamin and Trace Element Working Group; The American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.); Novel Nutrient Task Force Parenteral Vitamin and Trace Element Working Group; The American Society for Parenteral and Enteral Nutrition A S P E N. A Call to Action to Bring Safer Parenteral Micronutrient Products to the U.S. Market. Nutr. Clin. Pract. 2015, 30, 559–569. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef]
- Cohen, C.; Olsen, M.M. Pediatric total parenteral nutrition. Liver histopathology. Arch. Pathol. Lab. Med. 1981, 105, 152–156. [Google Scholar]
- Janosík, M.; Kery, V.; Gaustadnes, M.; Maclean, K.N.; Kraus, J.P. Regulation of human cystathionine beta-synthase by S-adenosyl-L-methionine: Evidence for two catalytically active conformations involving an autoinhibitory domain in the C-terminal region. Biochemistry 2001, 40, 10625–10633. [Google Scholar] [CrossRef] [PubMed]
- Steegborn, C.; Clausen, T.; Sondermann, P.; Jacob, U.; Worbs, M.; Marinkovic, S.; Huber, R.; Wahl, M.C. Kinetics and inhibition of recombinant human cystathionine gamma-lyase. Toward the rational control of transsulfuration. J. Biol. Chem. 1999, 274, 12675–12684. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.H.; Innis, S.M.; Davidson, A.G.; James, S.J. Phosphatidylcholine and lysophosphatidylcholine excretion is increased in children with cystic fibrosis and is associated with plasma homocysteine, S-adenosylhomocysteine, and S-adenosylmethionine. Am. J. Clin. Nutr. 2005, 81, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Innis, S.M.; Davidson, A.G.; Bay, B.N.; Slack, P.J.; Hasman, D. Plasma choline depletion is associated with decreased peripheral blood leukocyte acetylcholine in children with cystic fibrosis. Am. J. Clin. Nutr. 2011, 93, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, W. Choline in cystic fibrosis: Relations to pancreas insufficiency, enterohepatic cycle, PEMT and intestinal microbiota. Eur. J. Nutr. 2021, 60, 1737–1759. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Agellon, L.B.; Vance, D.E. Phosphatidylcholine homeostasis and liver failure. J. Biol. Chem. 2005, 280, 37798–37802. [Google Scholar] [CrossRef]
- da Costa, K.A.; Kozyreva, O.G.; Song, J.; Galanko, J.A.; Fischer, L.M.; Zeisel, S.H. Common genetic polymorphisms affect the human requirement for the nutrient choline. FASEB J. 2006, 20, 1336–1344. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E.; Li, Z.; Jacobs, R.L. Hepatic phosphatidylethanolamine N-methyltransferase.; unexpected roles in animal biochemistry and physiology. J. Biol. Chem. 2007, 282, 33237–33241. [Google Scholar] [CrossRef]
- Zeisel, S.H. The supply of choline is important for fetal progenitor cells. Semin. Cell Dev. Biol. 2011, 22, 624–628. [Google Scholar] [CrossRef]
- Maas, C.; Franz, A.R.; Shunova, A.; Mathes, M.; Bleeker, C.; Poets, C.F.; Schleicher, E.; Bernhard, W. Choline and polyunsaturated fatty acids in preterm infants’ maternal milk. Eur. J. Nutr. 2017, 56, 1733–1742. [Google Scholar] [CrossRef]
- Shunova, A.; Böckmann, K.A.; Minarski, M.; Franz, A.R.; Wiechers, C.; Poets, C.F.; Bernhard, W. Choline Content of Term and Preterm Infant Formulae Compared to Expressed Breast Milk-How Do We Justify the Discrepancies? Nutrients 2020, 12, 3815. [Google Scholar] [CrossRef] [PubMed]
- Böckmann, K.A.; Bernhard, W.; Minarski, M.; Shunova, A.; Wiechers, C.; Poets, C.F.; Franz, A.R. Choline supplementation for preterm infants: Metabolism of four Deuterium-labeled choline compounds. Eur. J. Nutr. 2023, 62, 1195–1205. [Google Scholar] [CrossRef] [PubMed]
- Tessitore, L.; Cui, Z.; Vance, D.E. Transient inactivation of phosphatidylethanolamine N-methyltransferase-2 and activation of cytidine triphosphate: Phosphocholine cytidylyltransferase during non-neoplastic liver growth. Biochem. J. 1997, 322, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Northfield, T.C.; Hofmann, A.F. Biliary lipid output during three meals and an overnight fast. I. Relationship to bile acid pool size and cholesterol saturation of bile in gallstone and control subjects. Gut 1975, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Böckmann, K.A.; Franz, A.R.; Shunova, A.; Minarski, M.; Wiechers, C.; Poets, C.F.; Bernhard, W. Different choline supplement metabolism in adults using deuterium labelling. Eur. J. Nutr. 2023, 62, 1795–1807. [Google Scholar] [CrossRef]
- Feuer, G.; Di Fonzo, C.J. Intrahepatic cholestasis: A review of biochemical-pathological mechanisms. Drug Metabol. Drug Interact. 1992, 10, 1–161. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.L.; Mohamed, R.; Mohamed, Z.; Zain, S.M. Phosphatidylethanolamine N-methyltransferase gene rs7946 polymorphism plays a role in risk of nonalcoholic fatty liver disease: Evidence from meta-analysis. Pharmacogenet Genom. 2016, 26, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Resseguie, M.E.; da Costa, K.A.; Galanko, J.A.; Patel, M.; Davis, I.J.; Zeisel, S.H. Aberrant estrogen regulation of PEMT results in choline deficiency-associated liver dysfunction. J. Biol. Chem. 2011, 286, 1649–1658. [Google Scholar] [CrossRef] [PubMed]
- Zeisel, S.H. The fetal origins of memory: The role of dietary choline in optimal brain development. J. Pediatr. 2006, 149, S131–S136. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.M.; da Costa, K.A.; Kwock, L.; Stewart, P.W.; Lu, T.S.; Stabler, S.P.; Allen, R.H.; Zeisel, S.H. Sex and menopausal status influence human dietary requirements for the nutrient choline. Am. J. Clin. Nutr. 2007, 85, 1275–1285. [Google Scholar] [CrossRef]
- Bernhard, W.; Raith, M.; Koch, V.; Kunze, R.; Maas, C.; Abele, H.; Poets, C.F.; Franz, A.R. Plasma phospholipids indicate impaired fatty acid homeostasis in preterm infants. Eur. J. Nutr. 2014, 53, 1533–1547. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernhard, W.; Böckmann, K.A.; Minarski, M.; Wiechers, C.; Busch, A.; Bach, D.; Poets, C.F.; Franz, A.R. Evidence and Perspectives for Choline Supplementation during Parenteral Nutrition—A Narrative Review. Nutrients 2024, 16, 1873. https://doi.org/10.3390/nu16121873
Bernhard W, Böckmann KA, Minarski M, Wiechers C, Busch A, Bach D, Poets CF, Franz AR. Evidence and Perspectives for Choline Supplementation during Parenteral Nutrition—A Narrative Review. Nutrients. 2024; 16(12):1873. https://doi.org/10.3390/nu16121873
Chicago/Turabian StyleBernhard, Wolfgang, Katrin A. Böckmann, Michaela Minarski, Cornelia Wiechers, Annegret Busch, Daniela Bach, Christian F. Poets, and Axel R. Franz. 2024. "Evidence and Perspectives for Choline Supplementation during Parenteral Nutrition—A Narrative Review" Nutrients 16, no. 12: 1873. https://doi.org/10.3390/nu16121873
APA StyleBernhard, W., Böckmann, K. A., Minarski, M., Wiechers, C., Busch, A., Bach, D., Poets, C. F., & Franz, A. R. (2024). Evidence and Perspectives for Choline Supplementation during Parenteral Nutrition—A Narrative Review. Nutrients, 16(12), 1873. https://doi.org/10.3390/nu16121873