
Prevention, Assessment, and Management of Malnutrition in Older Adults with Early Stages of Cognitive Disorders


Abstract
1. Introduction
2. Mechanisms of Malnutrition in Old Age
3. Risk Factors for Malnutrition in Early Cognitive Disorders
3.1. Cognitive, Psychological, and Social Factors
3.2. Pathophysiological Factors
3.3. Medication-Related Factors
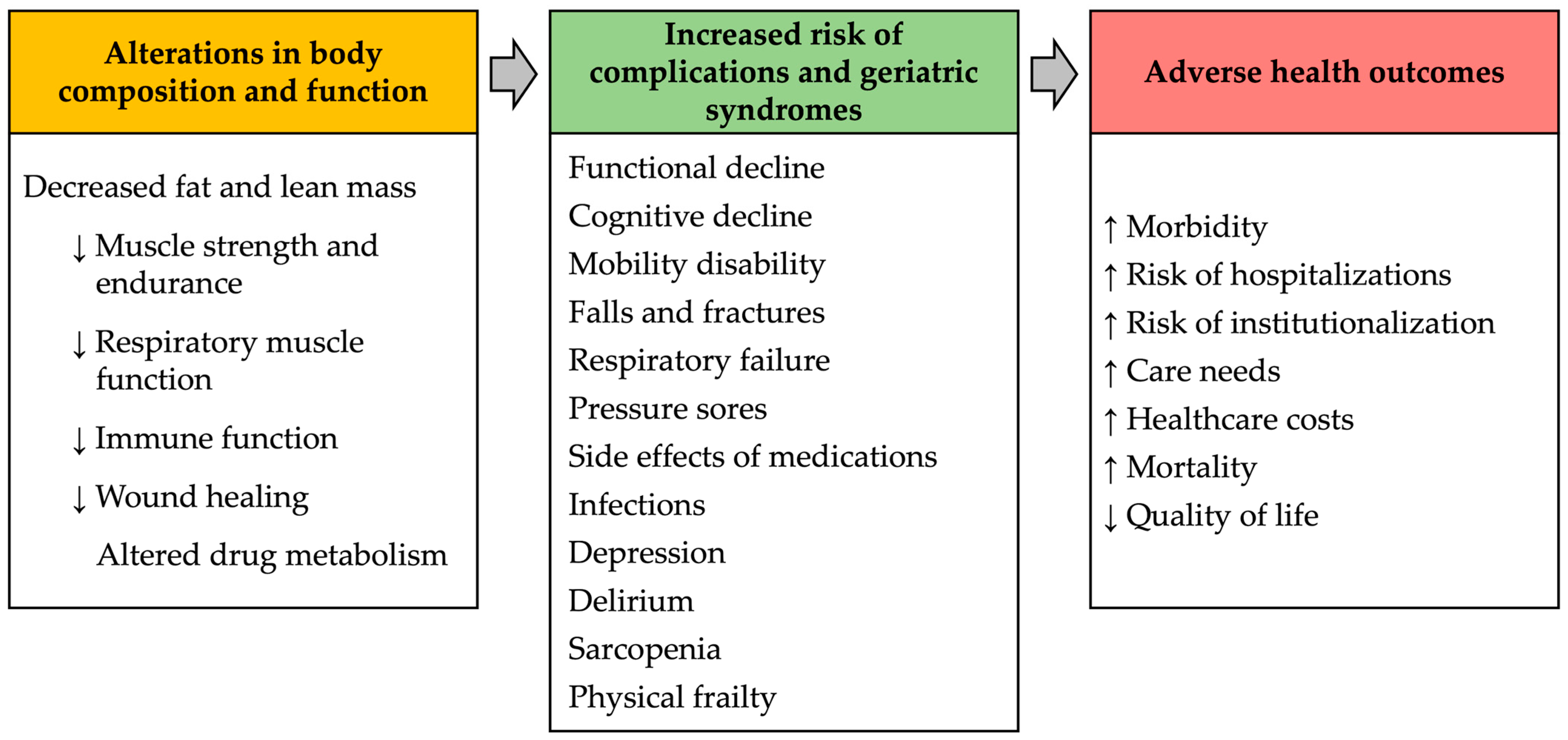
4. Consequences of Malnutrition
4.1. Adverse Health Outcomes of Energy-Protein Malnutrition
4.2. Micronutrient Deficiencies
4.2.1. B-Complex Vitamins
4.2.2. Vitamin D
5. Prevention and Management of Malnutrition
5.1. Screening and Assessment of Malnutrition
5.2. Management of Malnutrition
5.2.1. Individualized Management of Malnutrition
5.2.2. Strategies to Ensure Adequate Food Intake
5.2.3. Prevention of Dehydration
5.2.4. Replacement Therapy for Vitamin Deficiency and Cognition
6. Evidence on Nutritional Strategies Aimed at Preventing Cognitive Decline
6.1. Vitamin Supplements
6.2. Healthy Dietary Patterns for Neuroprotection
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Leij-Halfwerk, S.; Verwijs, M.H.; van Houdt, S.; Borkent, J.W.; Guaitoli, P.R.; Pelgrim, T.; Heymans, M.W.; Power, L.; Visser, M.; Corish, C.A.; et al. Prevalence of protein-energy malnutrition risk in european older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults ≥65 years: A systematic review and meta-analysis. Maturitas 2019, 126, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Wright, O.R.L.; Woo, J.; Hoogendijk, E.O. Malnutrition in older adults. Lancet 2023, 401, 951–966. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I.T. Limitations of nutrient intake. The effect of stressors: Trauma, sepsis and multiple organ failure. Eur. J. Clin. Nutr. 1999, 53 (Suppl. S1), S143–S147. [Google Scholar] [CrossRef]
- Ligthart-Melis, G.C.; Luiking, Y.C.; Kakourou, A.; Cederholm, T.; Maier, A.B.; de van der Schueren, M.A.E. Frailty, sarcopenia, and malnutrition frequently (co-)occur in hospitalized older adults: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1216–1228. [Google Scholar] [CrossRef] [PubMed]
- Arifin, H.; Chen, R.; Banda, K.J.; Kustanti, C.Y.; Chang, C.Y.; Lin, H.C.; Liu, D.; Lee, T.Y.; Chou, K.R. Meta-analysis and moderator analysis of the prevalence of malnutrition and malnutrition risk among older adults with dementia. Int. J. Nurs. Stud. 2024, 150, 104648. [Google Scholar] [CrossRef]
- World Health Organization, Geneva. International Classification of Diseases Eleventh Revision (ICD-11). Available online: https://icd.who.int/en (accessed on 10 May 2024).
- Cavalli, A.; Lelli, D.; Pedone, C.; Boccardi, V.; Mecocci, P.; Incalzi, R.A. Attention, praxis, and reasoning are associated with risk of undernutrition in older people with cognitive impairment. J. Alzheimers Dis. 2022, 89, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; Sisto, A.; Marzetti, E. Anorexia of aging: Risk factors, consequences, and potential treatments. Nutrients 2016, 8, 69. [Google Scholar] [CrossRef]
- Landis, B.N.; Konnerth, C.G.; Hummel, T. A study on the frequency of olfactory dysfunction. Laryngoscope 2004, 114, 1764–1769. [Google Scholar] [CrossRef]
- Smoliner, C.; Fischedick, A.; Sieber, C.C.; Wirth, R. Olfactory function and malnutrition in geriatric patients. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 1582–1588. [Google Scholar] [CrossRef]
- Doty, R.L. Influence of Age and Age-related diseases on olfactory function. Ann. N. Y. Acad. Sci. 1989, 561, 76–86. [Google Scholar] [CrossRef] [PubMed]
- van der Lely, A.J.; Tschop, M.; Heiman, M.L.; Ghigo, E. Biological, physiological, pathophysiological, and pharmacological aspects of ghrelin. Endocr. Rev. 2004, 25, 426–457. [Google Scholar] [CrossRef]
- Gutzwiller, J.-P.; Göke, B.; Drewe, J.; Hildebrand, P.; Ketterer, S.; Handschin, D.; Winterhalder, R.; Conen, D.; Beglinger, C. Glucagon-like peptide-1: A potent regulator of food intake in humans. Gut 1999, 44, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Di Francesco, V.; Fantin, F.; Omizzolo, F.; Residori, L.; Bissoli, L.; Bosello, O.; Zamboni, M. The anorexia of aging. Dig. Dis. 2007, 25, 129–137. [Google Scholar] [CrossRef]
- Di Francesco, V.; Zamboni, M.; Zoico, E.; Mazzali, G.; Dioli, A.; Omizzolo, F.; Bissoli, L.; Fantin, F.; Rizzotti, P.; Solerte, S.B.; et al. Unbalanced serum leptin and ghrelin dynamics prolong postprandial satiety and inhibit hunger in healthy elderly: Another reason for the “anorexia of aging”. Am. J. Clin. Nutr. 2006, 83, 1149–1152. [Google Scholar] [CrossRef] [PubMed]
- Strader, A.D.; Woods, S.C. Gastrointestinal hormones and food intake. Gastroenterology 2005, 128, 175–191. [Google Scholar] [CrossRef]
- Zamboni, M.; Zoico, E.; Fantin, F.; Panourgia, M.P.; Di Francesco, V.; Tosoni, P.; Solerte, B.; Vettor, R.; Bosello, O. Relation between leptin and the metabolic syndrome in elderly women. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 396–400. [Google Scholar] [CrossRef]
- Vincenzo, D.F.; Mauro, Z.; Andrea, D.; Elena, Z.; Gloria, M.; Francesca, O.; Luisa, B.; Sebastiano, B.S.; Luigi, B.; Ottavio, B. Delayed postprandial gastric emptying and impaired gallbladder contraction together with elevated cholecystokinin and peptide YY serum levels sustain satiety and inhibit hunger in healthy elderly persons. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1581–1585. [Google Scholar] [CrossRef]
- MacIntosh, C.G.; Andrews, J.M.; Jones, K.L.; Wishart, J.M.; Morris, H.A.; Jansen, J.B.; Morley, J.E.; Horowitz, M.; Chapman, I.M. Effects of age on concentrations of plasma cholecystokinin, glucagon-like peptide 1, and peptide YY and their relation to appetite and pyloric motility. Am. J. Clin. Nutr. 1999, 69, 999–1006. [Google Scholar] [CrossRef]
- MacIntosh, C.G.; Morley, J.E.; Wishart, J.; Morris, H.; Jansen, J.B.M.J.; Horowitz, M.; Chapman, I.M. Effect of exogenous cholecystokinin (CCK)-8 on food intake and plasma CCK, leptin, and insulin concentrations in older and young adults: Evidence for increased CCK activity as a cause of the anorexia of aging. J. Clin. Endocrinol. Metab. 2001, 86, 5830–5837. [Google Scholar] [CrossRef]
- Sturm, K.; MacIntosh, C.G.; Parker, B.A.; Wishart, J.; Horowitz, M.; Chapman, I.M. Appetite, food intake, and plasma concentrations of cholecystokinin, ghrelin, and other gastrointestinal hormones in undernourished older women and well-nourished young and older women. J. Clin. Endocrinol. Metab. 2003, 88, 3747–3755. [Google Scholar] [CrossRef]
- Cummings, D.E.; Overduin, J. Gastrointestinal regulation of food intake. J. Clin. Investig. 2007, 117, 13–23. [Google Scholar] [CrossRef]
- Chapman, I.M.; MacIntosh, C.G.; Morley, J.E.; Horowitz, M. The anorexia of ageing. Biogerontology 2002, 3, 67–71. [Google Scholar] [CrossRef]
- Morton, G.J.; Cummings, D.E.; Baskin, D.G.; Barsh, G.S.; Schwartz, M.W. Central nervous system control of food intake and body weight. Nature 2006, 443, 289–295. [Google Scholar] [CrossRef]
- Baechle, J.J.; Chen, N.; Makhijani, P.; Winer, S.; Furman, D.; Winer, D.A. Chronic inflammation and the hallmarks of aging. Mol. Metab. 2023, 74, 101755. [Google Scholar] [CrossRef]
- Franceschi, C.; Campisi, J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69 (Suppl. S1), S4–S9. [Google Scholar] [CrossRef]
- La Cava, A. Leptin in inflammation and autoimmunity. Cytokine 2017, 98, 51–58. [Google Scholar] [CrossRef]
- Morley, J.E.; Thomas, D.R. Anorexia and aging: Pathophysiology. Nutrition 1999, 15, 499–503. [Google Scholar] [CrossRef]
- Yeh, S.-S.; Blackwood, K.; Schuster, M.W. The cytokine basis of cachexia and its treatment: Are they ready for prime time? J. Am. Med. Dir. Assoc. 2008, 9, 219–236. [Google Scholar] [CrossRef]
- Laviano, A.; Meguid, M.M.; Inui, A.; Muscaritoli, M.; Rossi-Fanelli, F. Therapy insight: Cancer anorexia-cachexia syndrome--when all you can eat is yourself. Nat. Clin. Pract. Oncol. 2005, 2, 158–165. [Google Scholar] [CrossRef]
- Yeh, S.S.; Schuster, M.W. Geriatric cachexia: The role of cytokines. Am. J. Clin. Nutr. 1999, 70, 183–197. [Google Scholar] [CrossRef]
- Idrizaj, E.; Traini, C.; Vannucchi, M.G.; Baccari, M.C. Nitric oxide: From gastric motility to gastric dysmotility. Int. J. Mol. Sci. 2021, 22, 9990. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Wu, N.W.; Parker, K.; Dudossat, E.; Linquest, L.; Flanagan, C.J.; Dharani, A.; Patel, H.; Willett, O.; Cornett, E.M.; et al. Proton pump inhibitors, kidney damage, and mortality: An updated narrative review. Adv. Ther. 2023, 40, 2693–2709. [Google Scholar] [CrossRef]
- Huang, H.; Tseng, Y.; Chen, Y.; Chen, P.; Chiu, H. Diagnostic accuracy of the clinical dementia rating scale for detecting mild cognitive impairment and dementia: A bivariate meta-analysis. Int. J. Geriatr. Psychiatry 2021, 36, 239–251. [Google Scholar] [CrossRef]
- Silveri, M.C.; Reali, G.; Jenner, C.; Puopolo, M. Attention and memory in the preclinical stage of dementia. J. Geriatr. Psych. Neur. 2007, 20, 67–75. [Google Scholar] [CrossRef]
- Grober, E.; Hall, C.B.; Lipton, R.B.; Zonderman, A.B.; Resnick, S.M.; Kawas, C. Memory impairment, executive dysfunction, and intellectual decline in preclinical Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2008, 14, 266–278. [Google Scholar] [CrossRef]
- Volkert, D.; Chourdakis, M.; Faxen-Irving, G.; Frühwald, T.; Landi, F.; Suominen, M.H.; Vandewoude, M.; Wirth, R.; Schneider, S.M. ESPEN guidelines on nutrition in dementia. Clin. Nutr. 2015, 34, 1052–1073. [Google Scholar] [CrossRef]
- Razani, J.; Casas, R.; Wong, J.T.; Lu, P.; Alessi, C.; Josephson, K. Relationship between executive functioning and activities of daily living in patients with relatively mild dementia. Appl. Neuropsychol. 2007, 14, 208–214. [Google Scholar] [CrossRef]
- Marshall, G.A.; Rentz, D.M.; Frey, M.T.; Locascio, J.J.; Johnson, K.A.; Sperling, R.A. Executive function and instrumental activities of daily living in MCI and AD. Alzheimers Dement. 2011, 7, 300–308. [Google Scholar] [CrossRef]
- Holm, B.; Söderhamn, O. Factors associated with nutritional status in a group of people in an early stage of dementia. Clin. Nutr. 2003, 22, 385–389. [Google Scholar] [CrossRef]
- Johansson, M.M.; Marcusson, J.; Wressle, E. Cognitive impairment and its consequences in everyday life: Experiences of people with mild cognitive impairment or mild dementia and their relatives. Int. Psychogeriatr. 2015, 27, 949–958. [Google Scholar] [CrossRef]
- Droogsma, E.; Van Asselt, D.Z.B.; Scholzel-Dorenbos, C.J.M.; Van Steijn, J.H.M.; Van Walderveen, P.E.; Van Der Hooft, C.S. Nutritional status of community-dwelling elderly with newly diagnosed Alzheimer’s disease: Prevalence of malnutrition and the relation of various factors to nutritional status. J. Nutr. Health Aging 2013, 17, 606–610. [Google Scholar] [CrossRef]
- Suma, S.; Watanabe, Y.; Hirano, H.; Kimura, A.; Edahiro, A.; Awata, S.; Yamashita, Y.; Matsushita, K.; Arai, H.; Sakurai, T. Factors affecting the appetites of persons with Alzheimer’s disease and mild cognitive impairment: Factors related to appetite and dementia. Geriatr. Gerontol. Int. 2018, 18, 1236–1243. [Google Scholar] [CrossRef]
- Di Iulio, F.; Palmer, K.; Blundo, C.; Casini, A.R.; Gianni, W.; Caltagirone, C.; Spalletta, G. Occurrence of neuropsychiatric symptoms and psychiatric disorders in mild Alzheimer’s disease and mild cognitive impairment subtypes. Int. Psychogeriatr. 2010, 22, 629–640. [Google Scholar] [CrossRef]
- Köhler, C.A.; Magalhães, T.F.; Oliveira, J.M.M.P.; Alves, G.S.; Knöchel, C.; Oertel-Knöchel, V.; Pantel, J.; Carvalho, A.F. Neuropsychiatric disturbances in mild cognitive impairment (MCI): A Systematic review of population-based studies. Curr. Alzheimer Res. 2016, 13, 1066–1082. [Google Scholar] [CrossRef]
- Kai, K.; Hashimoto, M.; Amano, K.; Tanaka, H.; Fukuhara, R.; Ikeda, M. Relationship between eating disturbance and dementia severity in patients with Alzheimer’s disease. PLoS ONE 2015, 10, e0133666. [Google Scholar] [CrossRef]
- Leung, D.K.Y.; Chan, W.C.; Spector, A.; Wong, G.H.Y. Prevalence of depression, anxiety, and apathy symptoms across dementia stages: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2021, 36, 1330–1344. [Google Scholar] [CrossRef]
- Simmons, W.K.; Burrows, K.; Avery, J.A.; Kerr, K.L.; Bodurka, J.; Savage, C.R.; Drevets, W.C. Depression-related increases and decreases in appetite: Dissociable patterns of aberrant activity in reward and interoceptive neurocircuitry. Am. J. Psychiatry 2016, 173, 418–428. [Google Scholar] [CrossRef]
- Kimura, A.; Sugimoto, T.; Kitamori, K.; Saji, N.; Niida, S.; Toba, K.; Sakurai, T. Malnutrition is associated with behavioral and psychiatric symptoms of dementia in older women with mild cognitive impairment and early-stage Alzheimer’s disease. Nutrients 2019, 11, 1951. [Google Scholar] [CrossRef]
- Zamboni, G.; Wilcock, G. Lack of awareness of symptoms in people with dementia: The structural and functional basis. Int. J. Geriatr. Psychiatry 2011, 26, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Pacyna, R.R.; Han, S.D.; Wroblewski, K.E.; McClintock, M.K.; Pinto, J.M. Rapid olfactory decline during aging predicts dementia and GMV loss in AD brain regions. Alzheimers Dement. 2023, 19, 1479–1490. [Google Scholar] [CrossRef]
- Bathini, P.; Brai, E.; Auber, L.A. Olfactory dysfunction in the pathophysiological continuum of dementia. Ageing Res. Rev. 2019, 55, 100956. [Google Scholar] [CrossRef]
- Yap, A.C.; Mahendran, R.; Kua, E.H.; Zhou, W.; Wang, D.Y. Olfactory dysfunction is associated with mild cognitive impairment in community-dwelling older adults. Front. Aging Neurosci. 2022, 14, 930686. [Google Scholar] [CrossRef] [PubMed]
- Steinbach, S.; Hundt, W.; Vaitl, A.; Heinrich, P.; Förster, S.; Bürger, K.; Zahnert, T. Taste in mild cognitive impairment and Alzheimer’s disease. J. Neurol. 2010, 257, 238–246. [Google Scholar] [CrossRef]
- Yoo, H.S.; Jeon, S.; Chung, S.J.; Yun, M.; Lee, P.H.; Sohn, Y.H.; Evans, A.C.; Ye, B.S. Olfactory dysfunction in Alzheimer’s disease-and Lewy body-related cognitive impairment. Alzheimers Dement. 2018, 14, 1243–1252. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.-Y.; Jeong, H.S.; Lee, J.W.; Kwon, K.R.; Rha, K.-S.; Kim, Y.M. Effects of nutritional status and cognitive ability on olfactory function in geriatric patients. Auris Nasus Larynx 2016, 43, 56–61. [Google Scholar] [CrossRef]
- Gunzer, W. Changes of olfactory performance during the process of aging—Psychophysical testing and its relevance in the fight against malnutrition. J. Nutr. Health Aging 2017, 21, 1010–1015. [Google Scholar] [CrossRef]
- Toussaint, N.; de Roon, M.; van Campen, J.P.C.M.; Kremer, S.; Boesveldt, S. Loss of olfactory function and nutritional status in vital older adults and geriatric patients. Chem. Senses 2015, 40, 197–203. [Google Scholar] [CrossRef]
- Kim, W.Y.; Hur, M.; Cho, M.S.; Lee, H.S. Effect of olfactory function on nutritional status of Korean elderly women. Nutr. Res. 2003, 23, 723–734. [Google Scholar] [CrossRef]
- Gao, S.; Nguyen, J.T.; Hendrie, H.C.; Unverzagt, F.W.; Hake, A.; Smith-Gamble, V.; Hall, K. accelerated weight loss and incident dementia in an elderly African-American cohort. J. Am. Geriatr. Soc. 2011, 59, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Ogunniyi, A.; Gao, S.; Unverzagt, F.W.; Baiyewu, O.; Gureje, O.; Nguyen, J.T.; Smith-Gamble, V.; Murrell, J.R.; Hake, A.M.; Hall, K.S.; et al. Weight loss and incident dementia in elderly Yoruba Nigerians: A 10-year follow-up study. Int. Psychogeriatr. 2011, 23, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.K.; Wilkins, C.H.; Morris, J.C. Accelerated weight loss may precede diagnosis in Alzheimer disease. Arch. Neurol. 2006, 63, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Fu, W.; Cao, S.; Jiang, H.; Guo, Y.; Xv, H.; Liu, J.; Gan, Y.; Lu, Z. Weight loss and the risk of dementia: A meta-analysis of cohort studies. Curr. Alzheimer Res. 2021, 18, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Doorduijn, A.S.; van de Rest, O.; van der Flier, W.M.; Visser, M.; de van der Schueren, M.A.E. Energy and protein intake of Alzheimer’s disease patients compared to cognitively normal controls: Systematic review. J. Am. Med. Dir. Assoc. 2019, 20, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Shatenstein, B.; Kergoat, M.-J.; Reid, I. Poor nutrient intakes during 1-year follow-up with community-dwelling older adults with early-stage Alzheimer dementia compared to cognitively intact matched controls. J. Am. Diet. Assoc. 2007, 107, 2091–2099. [Google Scholar] [CrossRef] [PubMed]
- Doorduijn, A.S.; De Van Der Schueren, M.A.E.; Van De Rest, O.; De Leeuw, F.A.; Hendriksen, H.M.A.; Teunissen, C.E.; Scheltens, P.; Van Der Flier, W.M.; Visser, M. Energy Intake and expenditure in patients with Alzheimer’s disease and mild cognitive impairment: The NUDAD project. Alzheimers Res. Ther. 2020, 12, 116. [Google Scholar] [CrossRef] [PubMed]
- Porter, J.; Thompson, H.; Tjahyo, A.S. Understanding total energy expenditure in people with dementia: A systematic review with directions for future research. Australas. J. Ageing 2021, 40, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, I.; Sorrentino, L.; Paoletti, A.; Marra, R.; Arbitrio, M. The state of the art on acetylcholinesterase inhibitors in the treatment of Alzheimer’s disease. J. Cent. Nerv. Syst. Dis. 2021, 13, 11795735211029113. [Google Scholar] [CrossRef]
- Soysal, P.; Isik, A.T.; Stubbs, B.; Solmi, M.; Volpe, M.; Luchini, C.; D’Onofrio, G.; Pilotto, A.; Manzato, E.; Sergi, G.; et al. Acetylcholinesterase inhibitors are associated with weight loss in older people with dementia: A systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 1368–1374. [Google Scholar] [CrossRef]
- Beaudart, C.; Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.Y.; Lengelé, L.; Bruyère, O. Malnutrition as a strong predictor of the onset of sarcopenia. Nutrients 2019, 11, 2883. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hsu, T.-H.; Wu, W.-T.; Huang, K.-C.; Han, D.-S. Association between sarcopenia and cognitive impairment: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1164.e7–1164.e15. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Chu, Z.; Quan, X.; Zhang, Y.; Yuan, W.; Yao, Y.; Zhao, Y.; Fu, S. Malnutrition is positively associated with cognitive decline in centenarians and oldest-old adults: A cross-sectional study. EClinicalMedicine 2022, 47, 101336. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.W.; Kim, Y.; Choi, Y.H.; Lee, J.M.; Yoon, B.; Park, K.W.; Kim, S.E.; Kim, H.J.; Yoon, S.J.; Jeong, J.H.; et al. Association of nutritional status with cognitive stage in the elderly Korean population: The Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer’s Disease. J. Clin. Neurol. 2019, 15, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Borda, M.G.; Ayala Copete, A.M.; Tovar-Rios, D.A.; Jaramillo-Jimenez, A.; Giil, L.M.; Soennesyn, H.; Gómez-Arteaga, C.; Venegas-Sanabria, L.C.; Kristiansen, I.; Chavarro-Carvajal, D.A.; et al. Association of malnutrition with functional and cognitive trajectories in people living with dementia: A five-year follow-up study. J. Alzheimers Dis. 2021, 79, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Sanders, C.; Behrens, S.; Schwartz, S.; Wengreen, H.; Corcoran, C.D.; Lyketsos, C.G.; Tschanz, J.T. Nutritional status is associated with faster cognitive decline and worse functional impairment in the progression of dementia. J. Alzheimers Dis. 2016, 52, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Kishino, Y.; Sugimoto, T.; Kimura, A.; Kuroda, Y.; Uchida, K.; Matsumoto, N.; Saji, N.; Niida, S.; Sakurai, T. Longitudinal association between nutritional status and BPSD in older women with mild cognitive impairment and early-stage Alzheimer’s disease. Clin. Nutr. 2022, 41, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O. B Vitamins and the brain: Mechanisms, dose and efficacy—A review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.; Jaqua, E.; Nguyen, V.; Clay, J. B Vitamins: Functions and uses in medicine. Perm. J. 2022, 26, 89–97. [Google Scholar] [CrossRef]
- Temova Rakuša, Ž.; Roškar, R.; Hickey, N.; Geremia, S. Vitamin B12 in foods, food supplements, and medicines—A review of its role and properties with a focus on its stability. Molecules 2022, 28, 240. [Google Scholar] [CrossRef]
- Gillies, N.; Cameron-Smith, D.; Pundir, S.; Wall, C.R.; Milan, A.M. Exploring trajectories in dietary adequacy of the B vitamins folate, riboflavin, vitamins B6 and B12, with advancing older age: A systematic review. Br. J. Nutr. 2021, 126, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.M. Factors in aging that effect the bioavailability of nutrients. J. Nutr. 2001, 131, 1359S–1361S. [Google Scholar] [CrossRef]
- Basu, T.K.; Donaldson, D. Intestinal absorption in health and disease: Micronutrients. Best Pract. Res. Clin. Gastroenterol. 2003, 17, 957–979. [Google Scholar] [CrossRef]
- Porter, K.M.; Ward, M.; Hughes, C.F.; O’Kane, M.; Hoey, L.; McCann, A.; Molloy, A.M.; Cunningham, C.; Casey, M.C.; Tracey, F.; et al. Hyperglycemia and metformin use are associated with B vitamin deficiency and cognitive dysfunction in older adults. J. Clin. Endocr. Metab. 2019, 104, 4837–4847. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.E.; Hirsch, J.A.; Fonzetti, P.; Jordan, B.D.; Cirio, R.T.; Elder, J. Vitamin B1 (thiamine) and dementia. Ann. N. Y. Acad. Sci. 2016, 1367, 21–30. [Google Scholar] [CrossRef]
- Briani, C.; Torre, C.D.; Citton, V.; Manara, R.; Pompanin, S.; Binotto, G.; Adami, F. Cobalamin deficiency: Clinical picture and radiological findings. Nutrients 2013, 5, 4521. [Google Scholar] [CrossRef]
- Pacei, F.; Tesone, A.; Laudi, N.; Laudi, E.; Cretti, A.; Pnini, S.; Varesco, F.; Colombo, C. The relevance of thiamine evaluation in a practical setting. Nutrients 2020, 12, 2810. [Google Scholar] [CrossRef]
- Mosegaard, S.; Dipace, G.; Bross, P.; Carlsen, J.; Gregersen, N.; Olsen, R.K.J. Riboflavin deficiency—Implications for general human health and inborn errors of metabolism. Int. J. Mol. Sci. 2020, 21, 3847. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.; Hoey, L.; Hughes, C.F.; Ward, M.; McNulty, H. Causes, consequences and public health implications of low B-vitamin status in ageing. Nutrients 2016, 8, 725. [Google Scholar] [CrossRef]
- Gasperi, V.; Sibilano, M.; Savini, I.; Catani, M.V. Niacin in the central nervous system: An update of biological aspects and clinical applications. Int. J. Mol. Sci. 2019, 20, 974. [Google Scholar] [CrossRef]
- Xu, J.; Patassini, S.; Begley, P.; Church, S.; Waldvogel, H.J.; Faull, R.L.M.; Unwin, R.D.; Cooper, G.J.S. Cerebral deficiency of vitamin B5 (d-pantothenic acid; pantothenate) as a potentially-reversible cause of neurodegeneration and dementia in sporadic Alzheimer’s disease. Biochem. Biophys. Res. Commun. 2020, 527, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.E.; Abrams, S.A.; Aloia, J.; Bergeron, G.; Bourassa, M.W.; Brown, K.H.; Calvo, M.S.; Cashman, K.D.; Combs, G.; De-Regil, L.M.; et al. Global prevalence and disease burden of vitamin D deficiency: A roadmap for action in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2018, 1430, 44–79. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Antonio, L.; Olarte, O.R. Calcifediol (25OH vitamin D3) deficiency: A risk factor from early to old age. Nutrients 2022, 14, 1168. [Google Scholar] [CrossRef] [PubMed]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Armas, L.A.G.; French, C. All-source basal vitamin D inputs are greater than previously thought and cutaneous inputs are smaller. J. Nutr. 2013, 143, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Steur, M.; Allen, N.E.; Appleby, P.N.; Travis, R.C.; Key, T.J. Plasma concentrations of 25-hydroxyvitamin D in meat eaters, fish eaters, vegetarians and vegans: Results from the EPIC-Oxford study. Public Health Nutr. 2011, 14, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Sunlight and vitamin D: A global perspective for health. Dermatoendocrinol. 2013, 5, 51–108. [Google Scholar] [CrossRef]
- Holick, M.F. Biological effects of sunlight, ultraviolet radiation, visible light, infrared radiation and vitamin D for health. Anticancer Res. 2016, 36, 1345–1356. [Google Scholar]
- Wang, T.J.; Zhang, F.; Richards, J.B.; Kestenbaum, B.; van Meurs, J.B.; Berry, D.; Kiel, D.P.; Streeten, E.A.; Ohlsson, C.; Koller, D.L.; et al. Common genetic determinants of vitamin D insufficiency: A genome-wide association study. Lancet 2010, 376, 180–188. [Google Scholar] [CrossRef]
- Clements, M.R.; Johnson, L.; Fraser, D.R. A New mechanism for induced vitamin D deficiency in calcium deprivation. Nature 1987, 325, 62–65. [Google Scholar] [CrossRef]
- Steingrimsdottir, L.; Gunnarsson, O.; Indridason, O.S.; Franzson, L.; Sigurdsson, G. Relationship between serum parathyroid hormone levels, vitamin D sufficiency, and calcium intake. JAMA 2005, 294, 2336–2341. [Google Scholar] [CrossRef] [PubMed]
- Chai, B.; Gao, F.; Wu, R.; Dong, T.; Gu, C.; Lin, Q.; Zhang, Y. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: An updated meta-analysis. BMC Neurol. 2019, 19, 284. [Google Scholar] [CrossRef]
- Goodwill, A.M.; Szoeke, C. A systematic review and meta-analysis of the effect of low vitamin D on cognition. J. Am. Geriatr. Soc. 2017, 65, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- van der Schaft, J.; Koek, H.L.; Dijkstra, E.; Verhaar, H.J.J.; van der Schouw, Y.T.; Emmelot-Vonk, M.H. The association between vitamin D and cognition: A systematic review. Ageing Res. Rev. 2013, 12, 1013–1023. [Google Scholar] [CrossRef]
- Sommer, I.; Griebler, U.; Kien, C.; Auer, S.; Klerings, I.; Hammer, R.; Holzer, P.; Gartlehner, G. Vitamin D deficiency as a risk factor for dementia: A systematic review and meta-analysis. BMC Geriatr. 2017, 17, 16. [Google Scholar] [CrossRef]
- Shen, L.; Ji, H.F. Vitamin D deficiency is associated with increased risk of Alzheimer’s disease and dementia: Evidence from meta-analysis. Nutr. J. 2015, 14, 76. [Google Scholar] [CrossRef]
- Serón-Arbeloa, C.; Labarta-Monzón, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-López, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition screening and assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the Global Clinical Nutrition Community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment Short-Form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef]
- Guigoz, Y.; Vellas, B.; Garry, P.J. Assessing the nutritional status of the elderly: The Mini Nutritional Assessment as part of the geriatric evaluation. Nutr. Rev. 1996, 54, S59–S65. [Google Scholar] [CrossRef]
- Alibhai, S.M.H.; Greenwood, C.; Payette, H. An approach to the management of unintentional weight loss in elderly people. Can. Med. Assoc. J. 2005, 172, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.E. Undernutrition in Older Adults. Fam Pract 2012, 29, i89–i93. [Google Scholar] [CrossRef] [PubMed]
- Morilla-Herrera, J.C.; Martín-Santos, F.J.; Caro-Bautista, J.; Saucedo-Figueredo, C.; García-Mayor, S.; Morales-Asencio, J.M. Effectiveness of food-based fortification in older people. A systematic review and meta-analysis. J. Nutr. Health Aging 2016, 20, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Trabal, J.; Farran-Codina, A. Effects of dietary enrichment with conventional foods on energy and protein intake in older adults: A systematic review. Nutr. Rev. 2015, 73, 624–633. [Google Scholar] [CrossRef]
- Lam, I.T.Y.; Keller, H.H.; Pfisterer, K.; Duizer, L.; Stark, K.; Duncan, A.M. Micronutrient food fortification for residential care: A scoping review of current interventions. J. Am. Med. Dir. Assoc. 2016, 17, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Lochs, H.; Dejong, C.; Hammarqvist, F.; Hebuterne, X.; Leon-Sanz, M.; Schütz, T.; van Gemert, W.; van Gossum, A.; Valentini, L.; Lübke, H.; et al. ESPEN guidelines on enteral nutrition: Gastroenterology. Clin. Nutr. 2006, 25, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Allen, V.J.; Methven, L.; Gosney, M.A. Use of nutritional complete supplements in older adults with dementia: Systematic review and meta-analysis of clinical outcomes. Clin. Nutr. 2013, 32, 950–957. [Google Scholar] [CrossRef]
- Lauque, S.; Arnaud-Battandier, F.; Gillette, S.; Plaze, J.-M.; Andrieu, S.; Cantet, C.; Vellas, B. Improvement of weight and fat-free mass with oral nutritional supplementation in patients with Alzheimer’s disease at risk of malnutrition: A prospective randomized study. J. Am. Geriatr. Soc. 2004, 52, 1702–1707. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Lauretani, F.; Ticinesi, A.; Gionti, L.; Nouvenne, A.; Prati, B.; Meschi, T.; Maggio, M. Impact of nutritional status on caregiver burden of elderly outpatients. A cross-sectional study. Nutrients 2019, 11, 281. [Google Scholar] [CrossRef]
- Fjellström, C.; Starkenberg, Å.; Wesslén, A.; Licentiate, M.S.; Tysén Bäckström, A.-C.; Faxén-Irving, G. To be a good food provider: An exploratory study among spouses of persons with Alzheimer’s disease. Am. J. Alzheimers Dis. 2010, 25, 521–526. [Google Scholar] [CrossRef]
- Bunn, D.K.; Abdelhamid, A.; Copley, M.; Cowap, V.; Dickinson, A.; Howe, A.; Killett, A.; Poland, F.; Potter, J.F.; Richardson, K.; et al. Effectiveness of interventions to indirectly support food and drink intake in people with dementia: Eating and Drinking Well in dementiA (EDWINA) systematic review. BMC Geriatr. 2016, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Young, K.; Bunn, F.; Trivedi, D.; Dickinson, A. Nutritional education for community dwelling older people: A systematic review of randomised controlled trials. Int. J. Nurs. Stud. 2011, 48, 751–780. [Google Scholar] [CrossRef] [PubMed]
- Stroebele, N.; De Castro, J.M. Effect of ambience on food intake and food choice. Nutrition 2004, 20, 821–838. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuizen, W.F.; Weenen, H.; Rigby, P.; Hetherington, M.M. Older adults and patients in need of nutritional support: Review of current treatment options and factors influencing nutritional intake. Clin. Nutr. 2010, 29, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Nijs, K.A.N.D.; de Graaf, C.; Kok, F.J.; van Staveren, W.A. Effect of family style mealtimes on quality of life, physical performance, and body weight of nursing home residents: Cluster randomised controlled trial. BMJ 2006, 332, 1180–1183. [Google Scholar] [CrossRef]
- e Castro, J.M.; Brewer, E.M. The amount eaten in meals by humans is a power function of the number of people present. Physiol. Behav. 1992, 51, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Locher, J.L.; Robinson, C.O.; Roth, D.L.; Ritchie, C.S.; Burgio, K.L. The effect of the presence of others on caloric intake in homebound older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1475–1478. [Google Scholar] [CrossRef] [PubMed]
- Volicer, L.; Stelly, M.; Morris, J.; McLaughlin, J.; Volicer, B.J. Effects of dronabinol on anorexia and disturbed behavior in patients with Alzheimer’s disease. Int. J. Geriatr. Psych. 1997, 12, 913–919. [Google Scholar] [CrossRef]
- Thomas, D.R. Guidelines for the use of orexigenic drugs in long-term care. Nutr. Clin. Pract. 2006, 21, 82–87. [Google Scholar] [CrossRef]
- Duning, T.; Kloska, S.; Steinsträter, O.; Kugel, H.; Heindel, W.; Knecht, S. Dehydration confounds the assessment of brain atrophy. Neurology 2005, 64, 548–550. [Google Scholar] [CrossRef]
- Cowen, L.E.; Hodak, S.P.; Verbalis, J.G. Age-associated abnormalities of water homeostasis. Endocrinol. Metab. Clin. N. Am. 2013, 42, 349–370. [Google Scholar] [CrossRef]
- Schliess, F.; Häussinger, D. Cell volume and insulin signaling. In International Review of Cytology; Elsevier Science & Technology: Cambridge, MA, USA, 2003; Volume 225, pp. 187–228. ISBN 0074-7696. [Google Scholar]
- Lauriola, M.; Mangiacotti, A.; D’Onofrio, G.; Cascavilla, L.; Paris, F.; Paroni, G.; Seripa, D.; Greco, A.; Sancarlo, D. Neurocognitive disorders and dehydration in older patients: Clinical experience supports the hydromolecular hypothesis of dementia. Nutrients 2018, 10, 562. [Google Scholar] [CrossRef] [PubMed]
- Nishi, S.K.; Babio, N.; Paz-Graniel, I.; Serra-Majem, L.; Vioque, J.; Fitó, M.; Corella, D.; Pintó, X.; Bueno-Cavanillas, A.; Tur, J.A.; et al. Water intake, hydration status and 2-year changes in cognitive performance: A prospective cohort study. BMC Med. 2023, 21, 82. [Google Scholar] [CrossRef] [PubMed]
- Mantantzis, K.; Drewelies, J.; Duezel, S.; Steinhagen-Thiessen, E.; Demuth, I.; Wagner, G.G.; Lindenberger, U.; Gerstorf, D. Dehydration predicts longitudinal decline in cognitive functioning and well-being among older adults. Psychol. Aging 2020, 35, 517–528. [Google Scholar] [CrossRef]
- Eastley, R.; Wilcock, G.K.; Bucks, R.S. Vitamin B12 deficiency in dementia and cognitive impairment: The effects of treatment on neuropsychological function. Int. J. Geriatr. Psychiatry 2000, 15, 226–233. [Google Scholar] [CrossRef]
- Ueno, A.; Hamano, T.; Enomoto, S.; Shirafuji, N.; Nagata, M.; Kimura, H.; Ikawa, M.; Yamamura, O.; Yamanaka, D.; Ito, T.; et al. Influences of vitamin B 12 supplementation on cognition and homocysteine in patients with vitamin B 12 deficiency and cognitive impairment. Nutrients 2022, 14, 1494. [Google Scholar] [CrossRef]
- Kwok, T.; Lee, J.; Ma, R.C.; Wong, S.Y.; Kung, K.; Lam, A.; Ho, C.S.; Lee, V.; Harrison, J.; Lam, L. A Randomized placebo controlled trial of vitamin B12 supplementation to prevent cognitive decline in older diabetic people with borderline low serum vitamin B12. Clin. Nutr. 2017, 36, 1509–1515. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.J.; de Groot, L.C.; Joosten, L.W.; Bloo, R.J.; Clarke, R.; Ueland, P.M.; Schneede, J.; Blom, H.J.; Hoefnagels, W.H.; Staveren, W.A. van Effect of oral vitamin B-12 with or without folic acid on cognitive function in older people with mild vitamin B-12 deficiency: A randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 84, 361–370. [Google Scholar] [CrossRef]
- Fioravanti, M.; Ferrario, E.; Massaia, M.; Cappa, G.; Rivolta, G.; Grossi, E.; Buckley, A.E. Low Folate levels in the cognitive decline of elderly patients and the efficacy of folate as a treatment for improving memory deficits. Arch. Gerontol. Geriatr. 1998, 26, 1–13. [Google Scholar] [CrossRef]
- Beauchet, O.; Launay, C.P.; Galery, K.; Vilcocq, C.; Dontot-Payen, F.; Rousseau, B.; Benoit, V.; Allali, G. Effects of vitamin D and calcium fortified yogurts on gait, cognitive performances, and serum 25-hydroxyvitamin D concentrations in older community-dwelling females: Results from the GAit, MEmory, DiEtary and vitamin D (GAME-D2) randomized controlled trial. Nutrients 2019, 11, 2880. [Google Scholar] [CrossRef]
- Hu, J.; Jia, J.; Zhang, Y.; Miao, R.; Huo, X.; Ma, F. Effects of vitamin D3 supplementation on cognition and blood lipids: A 12-month randomised, double-blind, placebo-controlled trial. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Hu, J.; Huo, X.; Miao, R.; Zhang, Y.; Ma, F. Effects of vitamin D supplementation on cognitive function and blood Aβ-related biomarkers in older adults with Alzheimer’s disease: A randomised, double-blind, placebo-controlled trial. J. Neurol. Neurosurg. Psychiatry 2019, 90, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Castle, M.; Fiedler, N.; Pop, L.C.; Schneider, S.J.; Schlussel, Y.; Sukumar, D.; Hao, L.; Shapses, S.A. Three doses of vitamin D and cognitive outcomes in older women: A double-blind randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Kubiak, J.; Svartberg, J.; Fuskevåg, O.M.; Figenschau, Y.; Martinaityte, I.; Grimnes, G. Vitamin D supplementation has no effect on cognitive performance after four months in mid-aged and older subjects. J. Neurol. Sci. 2019, 396, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Ginde, A.A.; Brown, S.M.; Baughman, A.; Collar, E.M.; Ely, E.W.; Gong, M.N.; Hope, A.A.; Hou, P.C.; Hough, C.L.; et al. Effect of early high-dose vitamin D3 repletion on cognitive outcomes in critically ill adults. Chest 2021, 160, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Owusu, J.E.; Islam, S.; Katumuluwa, S.S.; Stolberg, A.R.; Usera, G.L.; Anwarullah, A.A.; Shieh, A.; Dhaliwal, R.; Ragolia, L.; Mikhail, M.B.; et al. Cognition and vitamin D in older African-American women—Physical performance and osteoporosis prevention with vitamin D in older African Americans trial and dementia. J. Am. Geriatr. Soc. 2019, 67, 81–86. [Google Scholar] [CrossRef]
- Balk, E.M.; Raman, G.; Tatsioni, A.; Chung, M.; Lau, J.; Rosenberg, I.H. Vitamin B6, B12, and folic acid supplementation and cognitive function: A systematic review of randomized trials. Arch. Intern. Med. 2007, 167, 21–30. [Google Scholar] [CrossRef]
- Ford, A.H.; Almeida, O.P. Effect of vitamin B supplementation on cognitive function in the elderly: A systematic review and meta-analysis. Drugs Aging 2019, 36, 419–434. [Google Scholar] [CrossRef]
- McCleery, J.; Abraham, R.P.; Denton, D.A.; Rutjes, A.W.S.; Chong, L.-Y.; Al-Assaf, A.S.; Griffith, D.J.; Rafeeq, S.; Yaman, H.; Malik, M.A.; et al. Vitamin and mineral supplementation for preventing dementia or delaying cognitive decline in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2018, 11, CD011905. [Google Scholar] [CrossRef]
- Rutjes, A.W.; Denton, D.A.; Di Nisio, M.; Chong, L.; Abraham, R.P.; Al-Assaf, A.S.; Anderson, J.L.; Malik, M.A.; Vernooij, R.W.; Martínez, G.; et al. Vitamin and mineral supplementation for maintaining cognitive function in cognitively healthy people in mid and late life. Cochrane Database Syst. Rev. 2018, 2019, CD011906. [Google Scholar] [CrossRef]
- Behrens, A.; Graessel, E.; Pendergrass, A.; Donath, C. Vitamin B-can it prevent cognitive decline? A systematic review and meta-analysis. Syst. Rev. 2020, 9, 111. [Google Scholar] [CrossRef] [PubMed]
- Malouf, R.; Grimley Evans, J.; Malouf, R. Vitamin B6 for cognition. Cochrane Database Syst. Rev. 2003, 2010, CD004393. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Guo, Y.; Men, J.; Fu, H.; Xu, T. The preventive efficacy of vitamin B supplements on the cognitive decline of elderly adults: A systematic review and meta-analysis. BMC Geriatr. 2021, 21, 367. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Liang, F.; Zhang, L.; Liu, J.; Dou, H. Vitamin D supplement for prevention of Alzheimer’s disease: A systematic review and meta-analysis. Am. J. Ther. 2021, 28, E638–E648. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Y.; Cheng, Y.C.; Chiu, C.C.; Liu, H.C.; Huang, M.C.; Tu, Y.K.; Kuo, P.H. Effects of Vitamin D Supplementation on cognitive outcomes: A systematic review and meta-analysis. Neuropsychol. Rev. 2023; online ahead of print. [Google Scholar] [CrossRef]
- da Silva, A.B.J.; Barros, W.M.A.; da Silva, M.L.; Silva, J.M.L.; Souza, A.P.d.S.; da Silva, K.G.; de Sousa Fernandes, M.S.; Carneiro, A.C.B.d.F.; Souza, V.d.O.N.; Lagranha, C.J. Impact of vitamin D on cognitive functions in healthy individuals: A systematic review in randomized controlled clinical trials. Front. Psychol. 2022, 13, 987203. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Kasturiratne, A.; Simmonds, M. Effect of folic acid, with or without other B vitamins, on cognitive decline: Meta-analysis of randomized trials. Am. J. Med. 2010, 123, 522–527.e2. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Cooper-Brown, L.A.; Allali, G. Vitamin D Supplementation and cognition in adults: A systematic review of randomized controlled trials. CNS Drugs 2021, 35, 1249–1264. [Google Scholar] [CrossRef] [PubMed]
- Markun, S.; Gravestock, I.; Jäger, L.; Rosemann, T.; Pichierri, G.; Burgstaller, J.M. Effects of vitamin B12 supplementation on cognitive function, depressive symptoms, and fatigue: A systematic review, meta-analysis, and meta-regression. Nutrients 2021, 13, 923. [Google Scholar] [CrossRef]
- Grodstein, F. Gaps and novel approaches in nutrition epidemiology for dementia prevention. Alzheimers Dement. 2021, 17, e049652. [Google Scholar] [CrossRef]
- Yassine, H.N.; Samieri, C.; Livingston, G.; Glass, K.; Wagner, M.; Tangney, C.; Plassman, B.L.; Ikram, M.A.; Voigt, R.M.; Gu, Y.; et al. Nutrition state of science and dementia prevention: Recommendations of the nutrition for dementia prevention working group. Lancet Healthy Longev. 2022, 3, e501–e512. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.H.; Gao, X.; Na, M.; Kris-Etherton, P.M.; Mitchell, D.C.; Jensen, G.L. Dietary pattern, diet quality, and dementia: A systematic review and meta-analysis of prospective cohort studies. J. Alzheimers Dis. 2020, 78, 151–168. [Google Scholar] [CrossRef] [PubMed]
- van de Rest, O.; Berendsen, A.A.; Haveman-Nies, A.; de Groot, L.C. Dietary patterns, cognitive decline, and dementia: A systematic review. Adv. Nutr. 2015, 6, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean diet and cardiovascular disease: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2019, 58, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean diet and age-related cognitive decline: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Trichopoulou, A.; Panza, F. Cross-sectional and longitudinal associations between adherence to Mediterranean diet with physical performance and cognitive function in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 70, 101395. [Google Scholar] [CrossRef] [PubMed]
- Limongi, F.; Siviero, P.; Bozanic, A.; Noale, M.; Veronese, N.; Maggi, S. The effect of adherence to the Mediterranean diet on late-life cognitive disorders: A systematic review. J. Am. Med. Dir. Assoc. 2020, 21, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Petersson, S.D.; Philippou, E. Mediterranean diet, cognitive function, and dementia: A systematic review of the evidence. Adv. Nutr. 2016, 7, 889–904. [Google Scholar] [CrossRef]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean diet, cognitive function, and dementia: A systematic review. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef]
- Singh, B.; Parsaik, A.K.; Mielke, M.M.; Erwin, P.J.; Knopman, D.S.; Petersen, R.C.; Roberts, R.O. Association of Mediterranean diet with mild cognitive impairment and Alzheimer’s disease: A systematic review and meta-analysis. J. Alzheimers Dis. 2014, 39, 271–282. [Google Scholar] [CrossRef]
- Radd-Vagenas, S.; Duffy, S.L.; Naismith, S.L.; Brew, B.J.; Flood, V.M.; Fiatarone Singh, M.A. Effect of the Mediterranean diet on cognition and brain morphology and function: A systematic review of randomized controlled trials. Am. J. Clin. Nutr. 2018, 107, 389–404. [Google Scholar] [CrossRef] [PubMed]
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diets are associated with less cognitive decline and a lower risk of Alzheimer’s disease—A review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Custodero, C.; Lozupone, M.; Imbimbo, B.P.; Valiani, V.; Agosti, P.; Schilardi, A.; D’Introno, A.; La Montagna, M.; Calvani, M.; et al. Relationships of dietary patterns, foods, and micro- and macronutrients with Alzheimer’s disease and late-life cognitive disorders: A systematic review. J. Alzheimers Dis. 2017, 59, 815–849. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Vitamin | Source | Risk Factors for Deficiency | Cognitive and Neuropsychiatric Syndromes of Deficiency | Ref. | |
|---|---|---|---|---|---|
| B1 | Thiamin | Plant and animal products | Poor intake (alcohol abuse, prolonged fasting, malnutrition), malabsorption (gastrointestinal malignancies, upper gastrointestinal or pancreatic surgery), increased utilization (hyperthyroidism), increased loss (diarrhea, advanced kidney disease, dialysis), drug-nutrient interaction (diuretics) | Wernicke–Korsakoff syndrome, cognitive decline, depression | [79,80,86,88] |
| B2 | Riboflavin | Poor intake (alcohol abuse, malnutrition, vegan diet), malabsorption (diabetes, liver disease, thyroid, and renal insufficiency), increased loss (diarrhea, dialysis) | Brain dysfunction, personality change | [79,80,89,90] | |
| B3 | Niacin | Poor intake (alcohol abuse, malnutrition), malabsorption (Crohn’s disease), drug-nutrient interaction (azathioprine, 6-mercaptopurine, 5-fluorouracil) | Depression, anxiety, cognitive decline, psychotic symptoms | [79,80,91] | |
| B5 | Pantothenic acid | Poor intake (alcohol abuse), malabsorption (diabetes, inflammatory bowel diseases), drug-nutrient interaction (cholinesterase inhibitors, memantine) | Cognitive impairment, depression | [79,80,92] | |
| B6 | Pyridoxine | Poor intake (alcohol abuse, malnutrition), malabsorption (advanced kidney disease), drug-nutrient interaction (steroids, valproic acid, carbamazepine, phenytoin, metformin) | Irritability, impaired alertness, depression, cognitive decline, dementia | [79,80,85,90] | |
| B7 | Biotin | Poor intake (alcohol abuse), malabsorption (genetic disorders), drug-nutrient interaction (anticonvulsants) | Depression | [79,80,84] | |
| B9 | Folic acid/folate | Plant products | Poor intake (alcohol abuse, malnutrition); malabsorption (intestinal diseases); others (low B2 and B12 levels); drug-nutrient interaction (methotrexate, metformin, cholestyramine, anticonvulsants) | Affective disorders, behavior changes, psychosis, cognitive decline, dementia | [79,80,87,90] |
| B12 | Cobalamin | Animal products | Poor intake (alcohol abuse, vegetarian diet, malnutrition), malabsorption (intestinal diseases, gastric/intestinal resection, atrophic gastritis, bacterial overgrowth, Helicobacter pylori, pancreatic insufficiency), drug-nutrient interaction (proton-pump inhibitors, H2-receptor antagonists, metformin) | ||
| Vitamin | Study Design and Population | Intervention | Results | Ref. |
|---|---|---|---|---|
| B12 | Longitudinal case-control study: 88 patients with B12 vitamin deficiency; n = 66 with dementia; n = 22 with cognitive impairment | Oral B12 vitamin supplementation was administered to all participants. A neuropsychological test battery was performed at baseline and after 8 months. | B12 supplementation improved cognition in patients with cognitive impairment, but there was no effect in those with dementia or on the deterioration rate of cognition compared with matched controls. | Eastley et al. [137] |
| Longitudinal study: n = 39 patients with B12 vitamin deficiency and cognitive impairment | Oral B12 vitamin supplementation was administered to all participants. MMSE was performed at baseline and at follow-up visits (21–133 days). | The mean MMSE score of patients improved significantly from a score of 20.5 (SD 6.4) to 22.9 (SD 5.5). | Ueno et al. [138] | |
| RCT: n = 271 patients with borderline low serum vitamin B12 levels and diabetes without cognitive impairment | Patients were assigned to oral B12 vitamin supplementation or placebo for 27 months. MMSE and CDR were performed at baseline and at 9-month intervals up to 27 months. | Vitamin B12 supplementation did not prevent cognitive decline. | Kwok et al. [139] | |
| B12 and B9 | RCT: n = 193 patients with mild vitamin B12 deficiency; n = 110 without cognitive impairment; n = 51 with MCI; n = 23 with dementia | Patients were assigned to receive oral vitamin B12 supplementation with or without vitamin B9; or a placebo for 24 weeks. A neuropsychological test battery was performed at baseline and at week 24. | There was no beneficial effect of vitamin B12 supplementation alone or in combination with vitamin B9 on cognitive functions (no stratification based on levels of cognitive function impairment was performed). | Eussen et al. [140] |
| B9 | RCT: n = 30 patients with vitamin B9 deficiency and MCI | Patients were assigned to receive oral vitamin B9 supplementation or placebo for 60 days. The Randt Memory Test was performed at baseline and at 60 days. | Patients treated with vitamin B9 showed a significant improvement in memory and attention efficiency when compared with the placebo group. The degree of memory improvement was positively correlated with the initial severity of B9 deficiency. | Fioravanti et al. [141] |
| D3 | RCT: n = 40 older women with D vitamin deficiency | Participants were assigned to D3 and calcium-fortified yogurts or placebo for 3 months. A cognitive test battery was performed at baseline and at 3 months. | The intervention group performed better on the MMSE, but there were no differences in other cognitive test results (TMT, FAB, digit span, and Stroop test). | Beauchet et al. [142] |
| RCT: n = 210 patients with low serum 25OHD and AD | Patients were assigned to receive oral vitamin D3 treatment or a placebo for 12 months. A neuropsychological test battery was performed at baseline, 6 months, and 12 months. | Both patients with AD and MCI who were treated with vitamin D3 showed a significant improvement in several cognitive tests compared with controls. | Jia et al. [144] | |
| RCT: n = 163 patients with low serum 25OHD and MCI | Hu et al. [143] | |||
| RCT: n = 374 patients with vitamin D deficiency | Patients were assigned to receive vitamin D3 treatment or a placebo. The Digit Symbol-Coding Test was performed at baseline and at 4 months. | At the end of the study, there were no statistically significant differences between the two groups in changes in cognitive test scores. | Jorde et al. [146] | |
| RCT: n = 95 critically ill patients with vitamin D deficiency | Patients were assigned to receive enteral vitamin D3 treatment or placebo at baseline. Cognition was assessed using the RBANS 1 to 1.5 years later. | No evidence was found that early administration of high-dose (540,000 IU) enteral vitamin D3 improved long-term cognition or executive function in critically ill patients with vitamin D deficiency. | Han et al. [147] | |
| RCT: n = 42 postmenopausal women with slightly low serum 25OHD | Participants were assigned to receive 600 (control group), 2000, or 4000 IU per day of total vitamin D3 supplementation for 1 year. Cognition was assessed using the CANTAB only at the end of the trial. | Participants taking vitamin D at 2000 IU per day performed better on learning and memory tests than the other groups. | Castle et al. [145] | |
| RCT: n = 260 postmenopausal women with low serum 25OHD | Participants were assigned to receive vitamin D combined with calcium or a placebo with calcium. MMSE was administered every 6 months. | There was no difference in cognition over time between women taking vitamin D3 supplementation and those taking placebo. | Owusu et al. [148] |
| Vitamin | No. of RCTs | Participants | Results | Ref. |
|---|---|---|---|---|
| B6, B12, and B9 | 16 | Adults with and without dementia; n = 6276 | No effects of B12 vitamin supplementation alone or in combination with B6 and/or B9 vitamins were found on any subdomain of cognitive function. | Markun et al. [161] |
| 14 | Adults with and without dementia; n = 866 | No evidence of the effect of vitamin B6, B12, and B9 supplementations, alone or in combinations, on cognitive functions. | Balk et al. [149] | |
| 31 | Adults with and without dementia; n = 17,029 | Vitamin B6, B12, and B9 supplementation did not show an improvement in cognitive functions. | Ford et al. [150] | |
| 5 | Adults with MCI; n = 879 | The evidence on overall cognitive function was of very low quality. There was little or no effect of B vitamins taken for 6 to 24 months on cognitive functions. | McCleery et al. [151] | |
| 14 | Healthy adults; n = 27,882 | Vitamin B6, B12, and B9 supplementation had little or no effect on global cognition at any time point up to 5 years. | Rutjes et al. [152] | |
| 20 | Healthy adults; n = 12,697 | There was no overall evidence that oral vitamin B supplementation prevented cognitive decline. | Behrens et al. [153] | |
| B9 | 9 | Healthy older adults; n = 2358 | There was no effect of vitamin B9 supplementation on cognitive decline. | Wald et al. [159] |
| B6 | 2 | Healthy older adults; n = 117 | There was no benefit from vitamin B6 supplementation on cognitive functions. | Malouf et al. [154] |
| B vitamins | 21 | Adults with and without MCI; n = 7571 | There was a significant effect of B vitamin supplementation on global cognitive function but not on information processing speed, episodic memory, or executive function. | Li et al. [155] |
| D3 | 20 | Healthy adults; n = 6700 | The review yielded mixed findings and concluded that there was no effect of vitamin D supplementation on cognitive functions. | Beauchet et al. [160] |
| 24 | Adults with and without dementia; n = 7557 | Vitamin D supplementation had a small but significant positive effect on cognition. A subgroup analysis indicated that the effect size of vitamin D was stronger in participants with baseline vitamin D deficiency. | Chen et al. [157] | |
| 9 | Adults without AD; n = 2345 | There was no significant difference in cognitive functions between participants supplemented with vitamin D and the comparison groups. | Du et al. [156] | |
| 9 | Healthy older adults; n = 5588 | There were positive changes in verbal memory, learning memory, attention, executive function, and global cognitive function. | Silva et al. [158] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loda, I.; D’Angelo, E.; Marzetti, E.; Kerminen, H. Prevention, Assessment, and Management of Malnutrition in Older Adults with Early Stages of Cognitive Disorders. Nutrients 2024, 16, 1566. https://doi.org/10.3390/nu16111566
Loda I, D’Angelo E, Marzetti E, Kerminen H. Prevention, Assessment, and Management of Malnutrition in Older Adults with Early Stages of Cognitive Disorders. Nutrients. 2024; 16(11):1566. https://doi.org/10.3390/nu16111566
Chicago/Turabian StyleLoda, Irene, Emanuela D’Angelo, Emanuele Marzetti, and Hanna Kerminen. 2024. "Prevention, Assessment, and Management of Malnutrition in Older Adults with Early Stages of Cognitive Disorders" Nutrients 16, no. 11: 1566. https://doi.org/10.3390/nu16111566
APA StyleLoda, I., D’Angelo, E., Marzetti, E., & Kerminen, H. (2024). Prevention, Assessment, and Management of Malnutrition in Older Adults with Early Stages of Cognitive Disorders. Nutrients, 16(11), 1566. https://doi.org/10.3390/nu16111566