

Associations of Flavonoid Intakes with Mortality among Populations with Hypertension: A Prospective Cohort Study


Abstract
1. Introduction
2. Materials and Methods
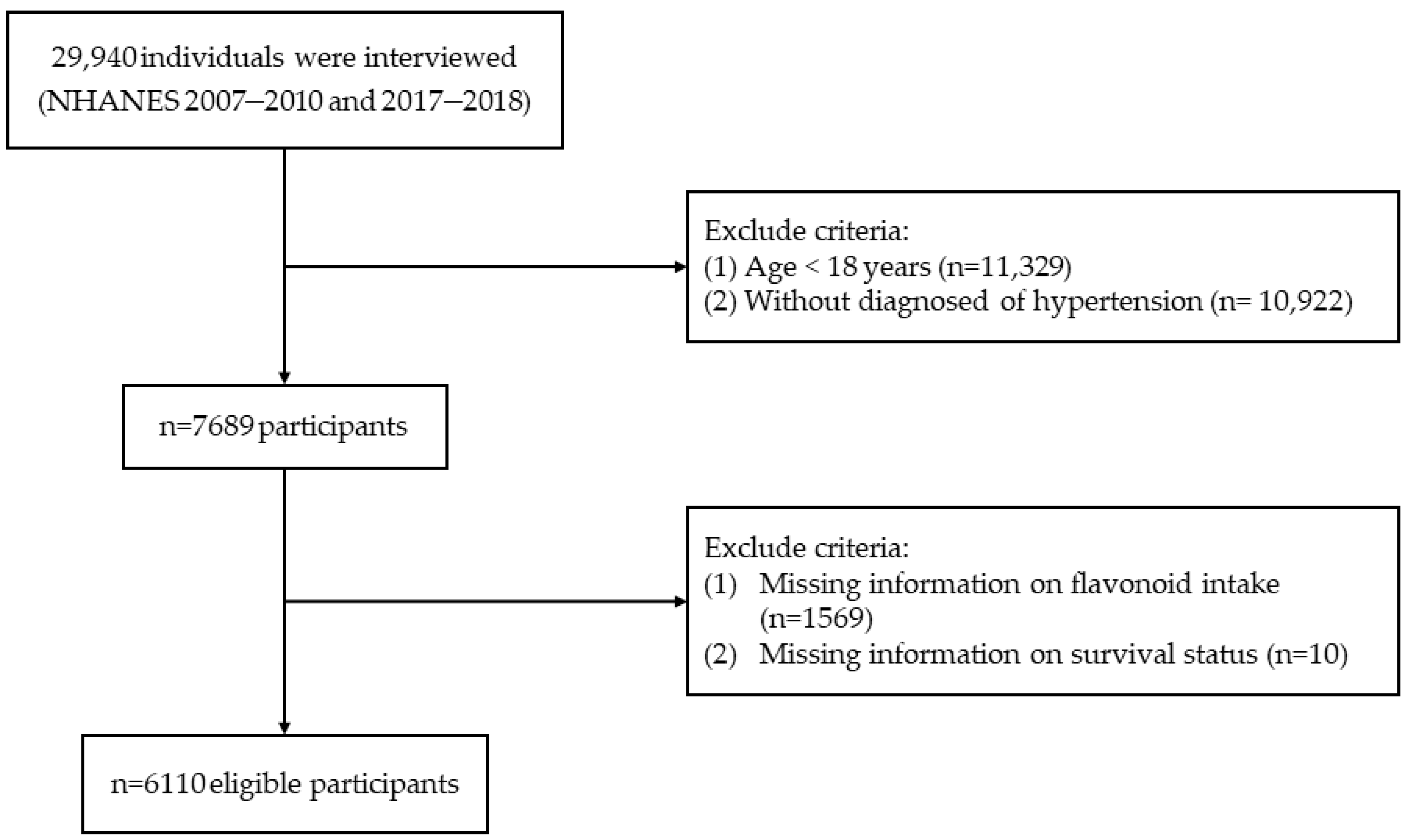
2.1. Study Population
2.2. Assessment of Flavonoid Intake
2.3. Mortality Confirmation
2.4. Covariates Assessment
2.5. Statistical Analysis
3. Results
3.1. Subsection
3.1.1. Baseline Characteristics
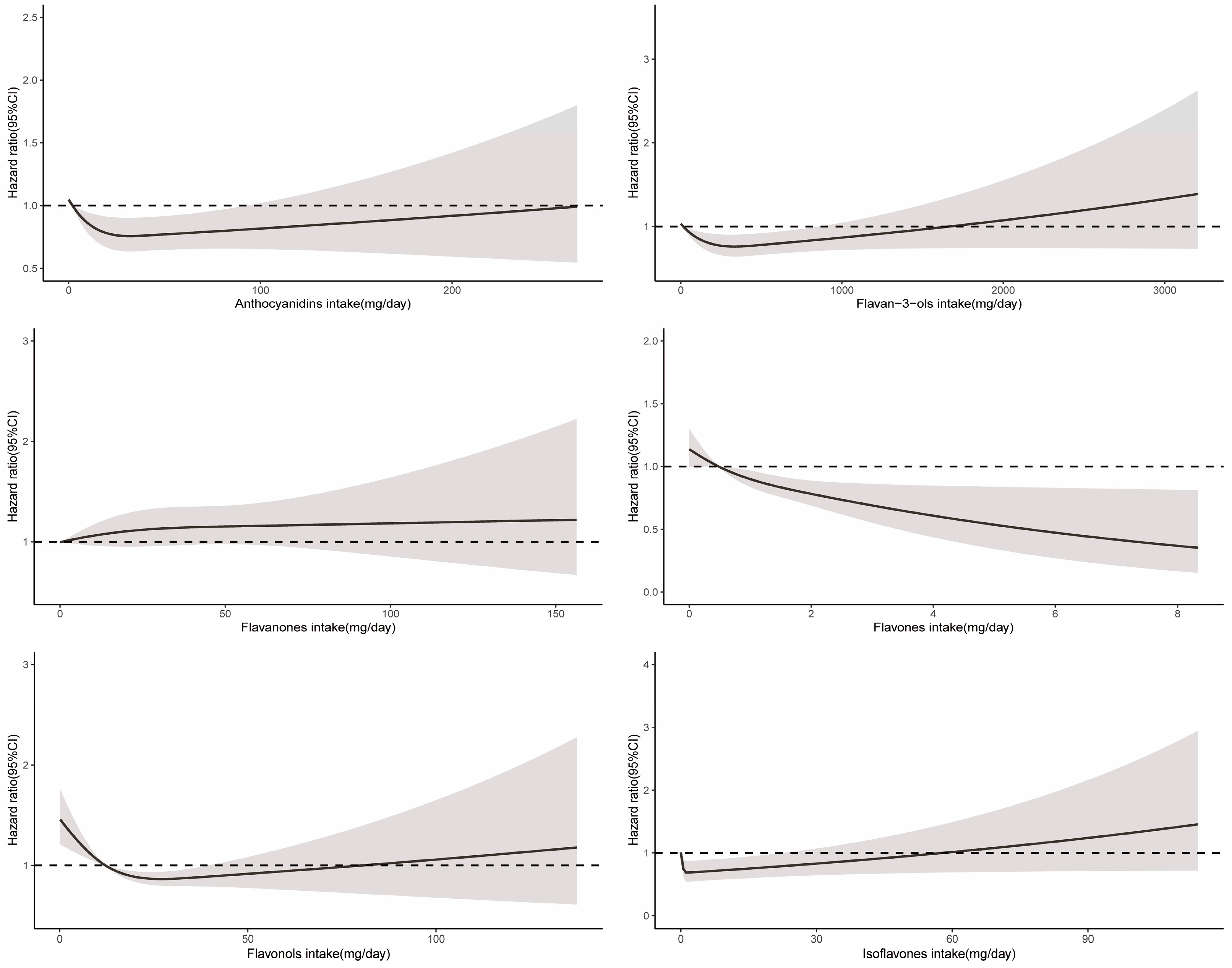
3.1.2. Total Flavonoid and Flavonoid Subclasses and All-Cause Mortality
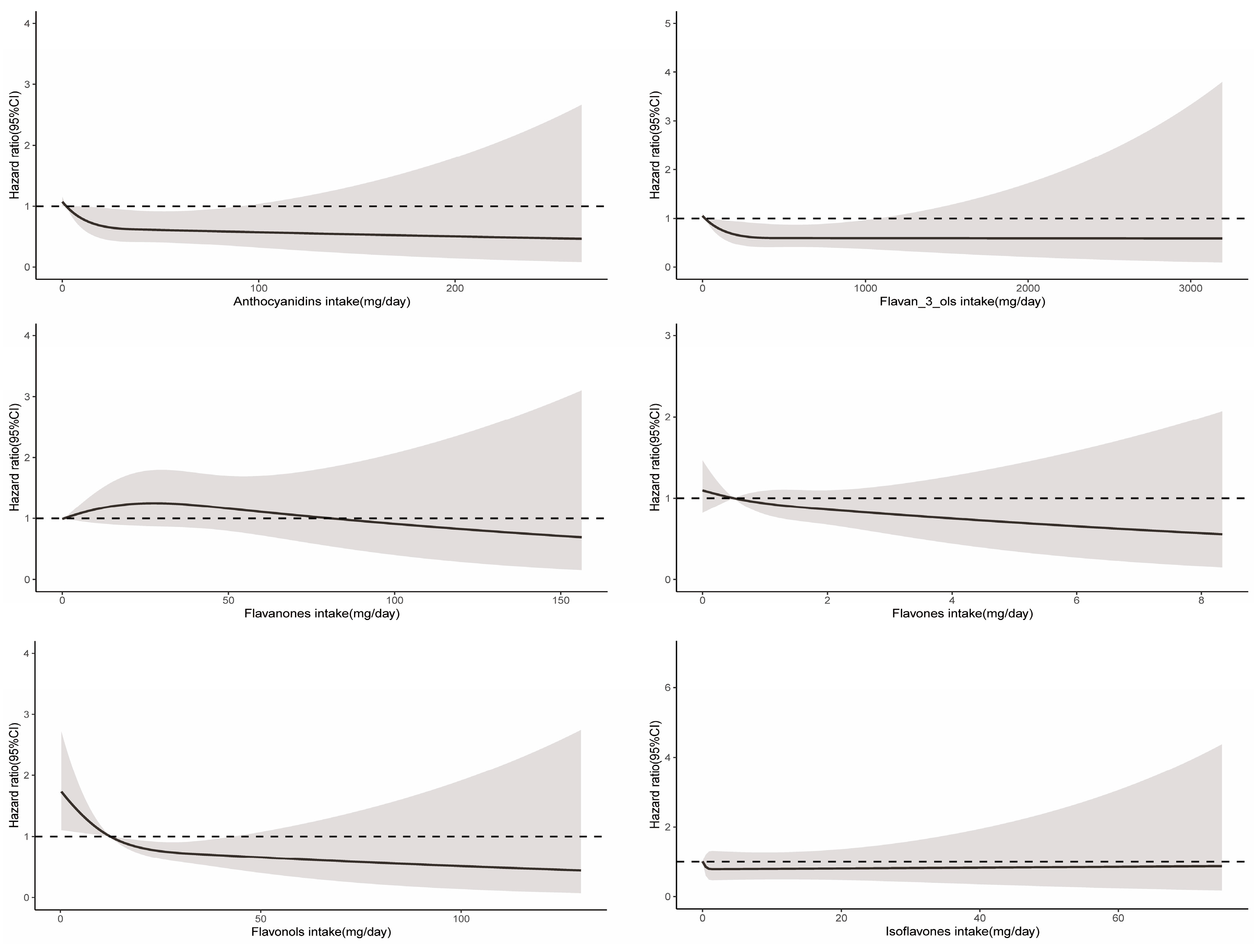
3.1.3. Total Flavonoid and Flavonoid Subclasses and Cause-Specific Mortality
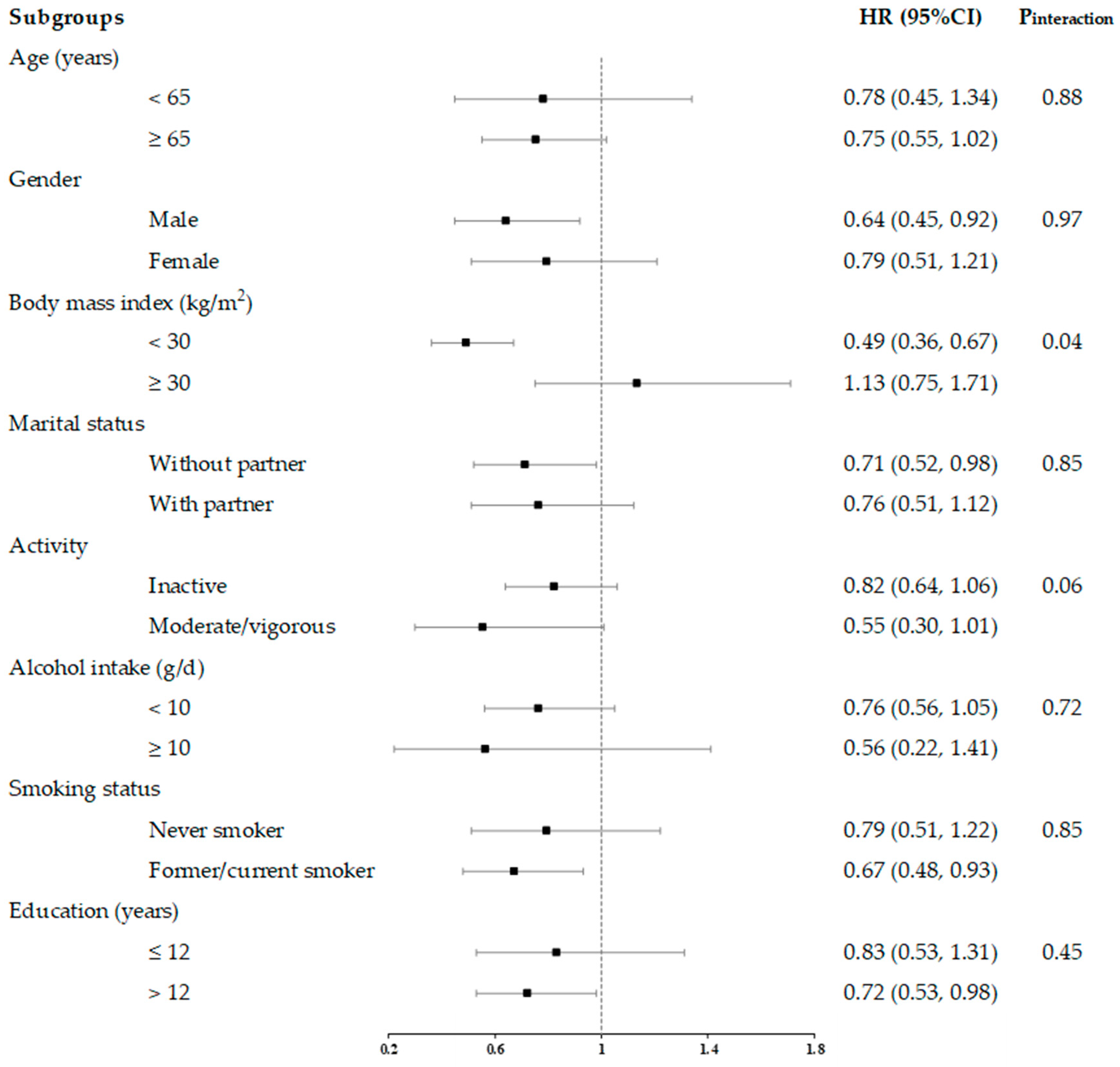
3.1.4. Stratified Analyses
3.1.5. Sensitivity Analyses
4. Discussion
4.1. Main Findings
4.2. Comparison with Previous Studies
4.3. Public Health and Clinical Implications
4.4. Mechanisms
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, L.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Grossman, E.; Messerli, F.H.; Boyko, V.; Goldbourt, U. Is there an association between hypertension and cancer mortality? Am. J. Med. 2002, 112, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global Disparities of Hypertension Prevalence and Control: A Systematic Analysis of Population-Based Studies From 90 Countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; MacLaughlin, E.J.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/N MA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, E127–E248. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Abate, K.H.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990-2015. J. Am. Med. Assoc. 2017, 317, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Burnier, M.; Egan, B.M. Adherence in Hypertension. Circ. Res. 2019, 124, 1124–1140. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Danaei, G.; Stevens, G.A.; Bixby, H.; Taddei, C.; Carrillo-Larco, R.M.; Solomon, B.; Riley, L.M.; Di Cesare, M.; Iurilli, M.L.C.; et al. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: An analysis of 123 nationally representative surveys. Lancet 2019, 394, 639–651. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Maaliki, D.; Shaito, A.A.; Pintus, G.; El-Yazbi, A.; Eid, A.H. Flavonoids in hypertension: A brief review of the underlying mechanisms. Curr. Opin. Pharmacol. 2019, 45, 57–65. [Google Scholar] [CrossRef]
- Peluso, I.; Miglio, C.; Morabito, G.; Ioannone, F.; Serafini, M. Flavonoids and Immune Function in Human: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2015, 55, 383–395. [Google Scholar] [CrossRef]
- Harahap, U.; Syahputra, R.A.; Ahmed, A.; Nasution, A.; Wisely, W.; Sirait, M.L.; Dalimunthe, A.; Zainalabidin, S.; Taslim, N.A.; Nurkolis, F.; et al. Current insights and future perspectives of flavonoids: A promising antihypertensive approach. Phytother. Res. 2024. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Cassidy, A.; O’Reilly, E.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef]
- Clark, J.L.; Zahradka, P.; Taylor, C.G. Efficacy of flavonoids in the management of high blood pressure. Nutr. Rev. 2015, 73, 799–822. [Google Scholar] [CrossRef]
- Lajous, M.; Rossignol, E.; Fagherazzi, G.; Perquier, F.; Scalbert, A.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C. Flavonoid intake and incident hypertension in women. Am. J. Clin. Nutr. 2016, 103, 1091–1098. [Google Scholar] [CrossRef]
- Mahdavi-Roshan, M.; Salari, A.; Ghorbani, Z.; Ashouri, A. The effects of regular consumption of green or black tea beverage on blood pressure in those with elevated blood pressure or hypertension: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 51, 102430. [Google Scholar] [CrossRef]
- Mazidi, M.; Katsiki, N.; Banach, M. A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies. Nutrients 2020, 12, 2350. [Google Scholar] [CrossRef]
- Wang, K.; Chen, Z.; Shen, M.; Chen, P.; Xiao, Y.; Fang, Z.; Hu, X.; Tang, J.; Liu, Q.; Zhou, S. Dietary fruits and vegetables and risk of cardiovascular diseases in elderly Chinese. Eur. J. Public Health 2023, 33, 1088–1094. [Google Scholar] [CrossRef]
- Bondonno, N.P.; Lewis, J.R.; Blekkenhorst, L.C.; Bondonno, C.P.; Shin, J.H.C.; Croft, K.D.; Woodman, R.J.; Wong, G.; Lim, W.H.; Gopinath, B.; et al. Association of flavonoids and flavonoid-rich foods with all-cause mortality: The Blue Mountains Eye Study. Clin. Nutr. 2020, 39, 141–150. [Google Scholar] [CrossRef]
- Zhou, N.; Xie, Z.-P.; Liu, Q.; Xu, Y.; Dai, S.-C.; Lu, J.; Weng, J.-Y.; Wu, L.-D. The dietary inflammatory index and its association with the prevalence of hypertension: A cross-sectional study. Front. Immunol. 2023, 13, 1097228. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention [CDC]. NCHS Research Ethics Review Board Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 2 March 2024).
- U.S. Department of Agriculture [USDA]. Food and Nutrient Database for Dietary Studies. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-flavonoid-database/ (accessed on 2 March 2024).
- Centers for Disease Control and Prevention [CDC]. National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm#intro (accessed on 2 March 2024).
- Harnly, J.M.; Doherty, R.F.; Beecher, G.R.; Holden, J.M.; Haytowitz, D.B.; Bhagwat, S.; Gebhardt, S. Flavonoid content of US fruits, vegetables, and nuts. J. Agric. Food Chem. 2006, 54, 9966–9977. [Google Scholar] [CrossRef]
- Zhou, Y.; Gu, K.; Zhou, F. Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study. Nutrients 2023, 15, 976. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention [CDC]. 2019 Public-Use Linked Mortality Files. Available online: https://www.cdc.gov/nchs/data-linkage/mortality-public.htm (accessed on 2 March 2024).
- Mahemuti, N.; Jing, X.; Zhang, N.; Liu, C.; Li, C.; Cui, Z.; Liu, Y.; Chen, J. Association between Systemic Immunity-Inflammation Index and Hyperlipidemia: A Population-Based Study from the NHANES (2015–2020). Nutrients 2023, 15, 1177. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention [CDC]. NHANES Tutorials. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx (accessed on 2 March 2024).
- Wan, Y.; Ma, D.; Shang, Q.; Xu, H. Association between dietary flavonoid intake and hypertension among US adults. Front. Immunol. 2024, 15, 1380493. [Google Scholar] [CrossRef]
- Zhou, F.; Gu, K.; Zhou, Y. Flavonoid intake is associated with lower all-cause and disease-specific mortality: The National Health and Nutrition Examination Survey 2007–2010 and 2017–2018. Front. Nutr. 2023, 10, 1046998. [Google Scholar] [CrossRef]
- Zong, Z.; Cheng, X.; Yang, Y.; Qiao, J.; Hao, J.; Li, F. Association between dietary flavonol intake and mortality risk in the U.S. adults from NHANES database. Sci. Rep. 2024, 14, 4572. [Google Scholar] [CrossRef]
- Liu, X.; Liu, Y.; Huang, Y.; Yu, H.; Yuan, S.; Tang, B.; Wang, P.; He, Q. Dietary total flavonoids intake and risk of mortality from all causes and cardiovascular disease in the general population: A systematic review and meta-analysis of cohort studies. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Panche, A.N.; Diwan, A.D.; Chandra, S.R. Flavonoids: An overview. J. Nutr. Sci. 2016, 5, e47. [Google Scholar] [CrossRef]
- Bondonno, N.P.; Dalgaard, F.; Kyrø, C.; Murray, K.; Bondonno, C.P.; Lewis, J.R.; Croft, K.D.; Gislason, G.; Scalbert, A.; Cassidy, A.; et al. Flavonoid intake is associated with lower mortality in the Danish Diet Cancer and Health Cohort. Nat. Commun. 2019, 10, 3651. [Google Scholar] [CrossRef]
- Al-Makki, A.; DiPette, D.; Whelton, P.K.; Murad, M.H.; Mustafa, R.A.; Acharya, S.; Beheiry, H.M.; Champagne, B.; Connell, K.; Cooney, M.T.; et al. Hypertension Pharmacological Treatment in Adults: A World Health Organization Guideline Executive Summary. Hypertension 2022, 79, 293–301. [Google Scholar] [CrossRef]
- Mancia Chairperson, G.; Kreutz Co-Chair, R.; Brunstrom, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Jimenez, C.; Cleries, R.; Agudo, A.; Sanchez, M.-J.; Sanchez-Cantalejo, E.; Molina-Montes, E.; Navarro, C.; Chirlaque, M.-D.; Maria Huerta, J.; et al. Dietary Flavonoid and Lignan Intake and Mortality in a Spanish Cohort. Epidemiology 2013, 24, 726–733. [Google Scholar] [CrossRef]
- Hayek, T.; Fuhrman, B.; Vaya, J.; Rosenblat, M.; Belinky, P.; Coleman, R.; Elis, A.; Aviram, M. Reduced progression of atherosclerosis in apolipoprotein E-deficient mice following consumption of red wine, or its polyphenols quercetin or catechin, is associated with reduced susceptibility of LDL to oxidation and aggregation. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 2744–2752. [Google Scholar] [CrossRef]
- Fuhrman, B.; Volkova, N.; Coleman, R.; Aviram, M. Grape powder polyphenols attenuate atherosclerosis development in apolipoprotein E deficient (E-O) mice and reduce macrophage atherogenicity. J. Nutr. 2005, 135, 722–728. [Google Scholar] [CrossRef]
- Baumann, J.; von Bruchhausen, F.; Wurm, G. Flavonoids and related compounds as inhibition of arachidonic acid peroxidation. Prostaglandins 1980, 20, 627–639. [Google Scholar] [CrossRef]
- López-Posadas, R.; Ballester, I.; Mascaraque, C.; Suárez, M.D.; Zarzuelo, A.; Martínez-Augustin, O.; Sánchez de Medina, F. Flavonoids exert distinct modulatory actions on cyclooxygenase 2 and NF-κB in an intestinal epithelial cell line (IEC18). Br. J. Pharmacol. 2010, 160, 1714–1726. [Google Scholar] [CrossRef]
- Sharifi-Rad, J.; Quispe, C.; Shaheen, S.; El Haouari, M.; Azzini, E.; Butnariu, M.; Sarac, I.; Pentea, M.; Ramirez-Alarcon, K.; Martorell, M.; et al. Flavonoids as potential anti-platelet aggregation agents: From biochemistry to health promoting abilities. Crit. Rev. Food Sci. Nutr. 2022, 62, 8045–8058. [Google Scholar] [CrossRef]
- Faggio, C.; Sureda, A.; Morabito, S.; Sanches-Silva, A.; Mocan, A.; Nabavi, S.F.; Nabavi, S.M. Flavonoids and platelet aggregation: A brief review. Eur. J. Pharmacol. 2017, 807, 91–101. [Google Scholar] [CrossRef]
- Xiong, H.-H.; Lin, S.-Y.; Chen, L.-L.; Ouyang, K.-H.; Wang, W.-J. The Interaction between Flavonoids and Intestinal Microbes: A Review. Foods 2023, 12, 320. [Google Scholar] [CrossRef]
- Cassidy, A.; Minihane, A.-M. The role of metabolism (and the microbiome) in defining the clinical efficacy of dietary flavonoids. Am. J. Clin. Nutr. 2017, 105, 10–22. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M. Reactive oxygen species, vascular oxidative stress, and redox signaling in hypertension—What is the clinical significance? Hypertension 2004, 44, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, M.; Cel, K.; Sroka, Z. The mechanistic insights into the role of pH and solvent on antiradical and prooxidant properties of polyphenols—Nine compounds case study. Food Chem. 2023, 407, 134677. [Google Scholar] [CrossRef]
- Yen, G.C.; Duh, P.D.; Tsai, H.L.; Huang, S.L. Pro-oxidative properties of flavonoids in human lymphocytes. Biosci. Biotechnol. Biochem. 2003, 67, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Wu, Q.; Chen, S.; Gao, J.; Li, X.; Zhang, X.; Zhou, Y.; He, D.; Cheng, Z.; Zhu, Y.; et al. The Associations of Two Novel Inflammation Indexes, SII and SIRI with the Risks for Cardiovascular Diseases and All-Cause Mortality: A Ten-Year Follow-Up Study in 85,154 Individuals. J. Inflamm. Res. 2021, 14, 131–140. [Google Scholar] [CrossRef]
- Dias, P.; Pourová, J.; Vopršalová, M.; Nejmanová, I.; Mladěnka, P. 3-Hydroxyphenylacetic Acid: A Blood Pressure-Reducing Flavonoid Metabolite. Nutrients 2022, 14, 328. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Flavonoid Intake (mg/d) | |||||
|---|---|---|---|---|---|
| Overall | Q1 <23.9 | Q2 23.9–63.1 | Q3 63.1–212.5 | Q4 >212.5 | |
| No. of participants | 6110 | 1528 | 1527 | 1527 | 1528 |
| Age (years) | 57.7 (0.4) | 54.7 (0.7) | 57.6 (0.7) | 60.2 (0.5) | 58.2 (0.6) |
| BMI (kg/m2) | 31.3 (0.2) | 32.0 (0.3) | 31.4 (0.3) | 30.9 (0.3) | 31.2 (0.3) |
| Daily energy intake (kcal/d) | 2013 (17) | 1765 (25) | 2027 (27) | 2148 (32) | 2090 (38) |
| Alcohol consumption (g/d) | 8.9 (0.5) | 4.9 (0.7) | 11.7 (1.0) | 10.4 (1.0) | 8.3 (1.0) |
| Fruit intake (cup/d) | 1.0 (0.0) | 0.3 (0.0) | 0.9 (0.0) | 1.5 (0.1) | 1.2 (0.1) |
| Vegetable intake (cup/d) | 1.5 (0.0) | 1.1 (0.0) | 1.6 (0.1) | 1.7 (0.1) | 1.7 (0.0) |
| Whole grains intake (oz/d) | 0.8 (0.0) | 0.6 (0.0) | 0.9 (0.0) | 1.0 (0.0) | 0.9 (0.1) |
| Red meat intake (oz/d) | 1.7 (0.1) | 1.5 (0.1) | 1.6 (0.1) | 1.7 (0.1) | 1.8 (0.1) |
| Sex, % | |||||
| Female | 3117 (50.9) | 756 (49.9) | 769 (47.5) | 796 (51.4) | 796 (54.3) |
| Male | 2993 (49.1) | 772 (50.1) | 758 (52.5) | 731 (48.6) | 732 (45.7) |
| Race, % | |||||
| White | 2870 (69.2) | 681 (66.0) | 704 (68.2) | 692 (68.0) | 793 (73.9) |
| Black | 1571 (14.0) | 447 (17.3) | 371 (13.8) | 385 (14.0) | 368 (11.5) |
| Hispanic | 529 (4.7) | 138 (4.6) | 160 (5.9) | 148 (5.9) | 83 (2.7) |
| Mexican American | 729 (5.8) | 181 (6.9) | 213 (6.9) | 193 (5.6) | 142 (4.1) |
| Others | 411 (6.3) | 81 (5.3) | 79 (5.3) | 109 (6.4) | 142 (7.8) |
| Education, % | |||||
| <9 years | 711 (6.4) | 233 (8.9) | 191 (6.8) | 179 (6.3) | 109 (4.1) |
| 9–12 years | 952 (11.3) | 295 (16.0) | 242 (11.4) | 204 (8.9) | 211 (9.5) |
| >12 years | 4434 (82.1) | 998 (75.1) | 1093 (81.9) | 1136 (84.8) | 1207 (86.3) |
| Activity, % | |||||
| Inactive | 3738 (55.3) | 963 (55.9) | 954 (60.7) | 923 (53.1) | 898 (52.1) |
| Moderate | 1287 (24.6) | 279 (21.6) | 299 (20.5) | 356 (27.9) | 353 (27.8) |
| Vigorous | 1085 (20.0) | 286 (22.4) | 274 (18.8) | 248 (18.9) | 277 (20.1) |
| Marital status, % | |||||
| Without partner | 2500 (34.9) | 678 (38.8) | 646 (37.6) | 617 (33.3) | 559 (31.6) |
| With partner | 3570 (64.5) | 837 (61.2) | 873 (62.4) | 902 (66.7) | 958 (68.4) |
| Smoke, % | |||||
| Never | 3057 (51.1) | 655 (43.5) | 761 (51.2) | 840 (56.2) | 801 (53.7) |
| Former | 1946 (31.3) | 476 (31.2) | 488 (31.5) | 506 (32.9) | 476 (30.2) |
| Current | 1079 (17.2) | 391 (25.3) | 271 (17.3) | 173 (10.9) | 244 (16.2) |
| Diabetes, % | |||||
| No | 4122 (73.0) | 974 (70.3) | 1019 (71.9) | 1069 (75.6) | 1060 (74.9) |
| Yes | 1974 (26.7) | 549 (29.7) | 507 (28.1) | 454 (24.4) | 465 (25.1) |
| Hyperlipidemia, % | |||||
| No | 1160 (18.2) | 321 (21.3) | 285 (18.6) | 284 (18.4) | 270 (15.2) |
| Yes | 4949 (81.8) | 1207 (78.7) | 1242 (81.4) | 1242 (81.6) | 1258 (84.8) |
| Total Flavonoid Intake | ||||
|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |
| Total flavonoids (mg/day) | 12.6 (0.2) | 40.9 (0.4) | 118.0 (1.8) | 665.8 (27.5) |
| Case/Person-years | 1528/10,707 | 1527/11,071 | 1527/10,706 | 1528/11,494 |
| All-cause mortality | ||||
| No. events (n) | 318 | 286 | 294 | 257 |
| Model 1 | ref | 0.75 (0.63, 0.89) | 0.59 (0.49, 0.73) | 0.60 (0.47, 0.76) |
| Model 2 | ref | 0.86 (0.71, 1.04) | 0.75 (0.59, 0.96) | 0.75 (0.59, 0.97) |
| Model 3 | ref | 0.85 (0.69, 1.04) | 0.72 (0.55, 0.96) | 0.74 (0.56, 0.97) |
| CVD-related mortality | ||||
| No. events (n) | 65 | 76 | 79 | 62 |
| Model 1 | ref | 0.64 (0.41, 0.99) | 0.63 (0.42, 0.94) | 0.60 (0.35, 1.02) |
| Model 2 | ref | 0.71 (0.45, 1.12) | 0.75 (0.48, 1.17) | 0.75 (0.42, 1.33) |
| Model 3 | ref | 0.73 (0.45, 1.17) | 0.78 (0.46, 1.33) | 0.77 (0.40, 1.46) |
| Cancer-related mortality | ||||
| No. events (n) | 80 | 64 | 62 | 59 |
| Model 1 | ref | 0.92 (0.55, 1.53) | 0.54 (0.33, 0.88) | 0.51 (0.31, 0.84) |
| Model 2 | ref | 1.07 (0.65, 1.78) | 0.68 (0.40, 1.16) | 0.60 (0.35, 1.01) |
| Model 3 | ref | 1.10 (0.65, 1.86) | 0.68 (0.37, 1.24) | 0.62 (0.35, 1.08) |
| Total Flavonoid Subclass Intake | ||||
|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |
| Anthocyanidins (mg/day) | ≤0.12 | 0.12–1.99 | 1.99–10.40 | >10.40 |
| Case/Person-years | 1528/10,445 | 1528/11,135 | 1526/11,425 | 1528/10,973 |
| All-cause mortality | ||||
| No. events (n) | 295 | 309 | 290 | 261 |
| Model 1 | ref | 0.86 (0.69, 1.07) | 0.69 (0.54, 0.87) | 0.57 (0.46, 0.71) |
| Model 2 | ref | 1.01 (0.81, 1.25) | 0.84 (0.67, 1.07) | 0.73 (0.59, 0.92) |
| Model 3 | ref | 1.00 (0.80, 1.25) | 0.82 (0.63, 1.06) | 0.70 (0.55, 0.89) |
| CVD-related mortality | ||||
| No. events (n) | 70 | 72 | 70 | 70 |
| Model 1 | ref | 0.91 (0.54, 1.52) | 0.67 (0.41, 1.10) | 0.53 (0.32, 0.90) |
| Model 2 | ref | 1.09 (0.67, 1.78) | 0.85 (0.50, 1.46) | 0.66 (0.38, 1.16) |
| Model 3 | ref | 1.10 (0.65, 1.84) | 0.84 (0.47, 1.52) | 0.65 (0.33, 1.25) |
| Cancer-related mortality | ||||
| No. events (n) | 75 | 76 | 57 | 57 |
| Model 1 | ref | 0.76 (0.48, 1.21) | 0.57 (0.36, 0.91) | 0.42 (0.26, 0.68) |
| Model 2 | ref | 0.89 (0.56, 1.40) | 0.75 (0.48, 1.18) | 0.56 (0.34, 0.93) |
| Model 3 | ref | 0.90 (0.58, 1.41) | 0.74 (0.46, 1.18) | 0.55 (0.32, 0.93) |
| Flavan-3-ols (mg/day) | ≤4.90 | 4.90–15.18 | 15.18–153.29 | >153.29 |
| Case/Person-years | 1528/10,645 | 1527/11,038 | 1527/10,750 | 1528/11,545 |
| All-cause mortality | ||||
| No. events (n) | 315 | 309 | 268 | 263 |
| Model 1 | ref | 0.80 (0.67, 0.96) | 0.66 (0.53, 0.81) | 0.63 (0.50, 0.79) |
| Model 2 | ref | 0.93 (0.78, 1.11) | 0.81 (0.68, 0.96) | 0.77 (0.61, 0.98) |
| Model 3 | ref | 0.91 (0.76, 1.08) | 0.77 (0.63, 0.93) | 0.76 (0.59, 0.96) |
| CVD-related mortality | ||||
| No. events (n) | 66 | 75 | 68 | 73 |
| Model 1 | ref | 1.09 (0.73, 1.64) | 0.81 (0.52, 1.28) | 0.86 (0.53, 1.39) |
| Model 2 | ref | 1.30 (0.88, 1.94) | 0.98 (0.66, 1.47) | 1.08 (0.68, 1.70) |
| Model 3 | ref | 1.34 (0.88, 2.03) | 1.08 (0.66, 1.75) | 1.12 (0.67, 1.86) |
| Cancer-related mortality | ||||
| No. events (n) | 85 | 65 | 59 | 56 |
| Model 1 | ref | 0.56 (0.38, 0.83) | 0.65 (0.41, 1.05) | 0.43 (0.27, 0.69) |
| Model 2 | ref | 0.72 (0.46, 1.12) | 0.85 (0.52, 1.39) | 0.51 (0.32, 0.83) |
| Model 3 | ref | 0.71 (0.48, 1.06) | 0.82 (0.49, 1.38) | 0.51 (0.31, 0.82) |
| Flavanones (mg/day) | ≤0.05 | 0.05–0.58 | 0.58–19.35 | >19.35 |
| Case/Person-years | 1539/10,239 | 1526/10,994 | 1517/11,472 | 1528/11,273 |
| All-cause mortality | ||||
| No. events (n) | 293 | 272 | 265 | 325 |
| Model 1 | ref | 0.81 (0.65, 1.02) | 0.73 (0.57, 0.94) | 0.81 (0.66, 1.00) |
| Model 2 | ref | 0.89 (0.70, 1.12) | 0.89 (0.69, 1.14) | 1.01 (0.82, 1.24) |
| Model 3 | ref | 0.92 (0.72, 1.16) | 0.93 (0.73, 1.18) | 1.04 (0.86, 1.27) |
| CVD-related mortality | ||||
| No. events (n) | 91 | 58 | 63 | 70 |
| Model 1 | ref | 0.62 (0.40, 0.97) | 0.62 (0.37, 1.06) | 0.58 (0.40, 0.85) |
| Model 2 | ref | 0.67 (0.41, 1.09) | 0.75 (0.45, 1.26) | 0.72 (0.49, 1.06) |
| Model 3 | ref | 0.67 (0.40, 1.13) | 0.77 (0.48, 1.25) | 0.76 (0.51, 1.14) |
| Cancer-related mortality | ||||
| No. events (n) | 62 | 69 | 65 | 69 |
| Model 1 | ref | 1.18 (0.76, 1.82) | 0.80 (0.52, 1.25) | 0.88 (0.54, 1.42) |
| Model 2 | ref | 1.31 (0.85, 2.01) | 1.01 (0.64, 1.62) | 1.20 (0.72, 2.00) |
| Model 3 | ref | 1.36 (0.88, 2.10) | 1.06 (0.67, 1.69) | 1.31 (0.75, 2.28) |
| Flavones(mg/day) | ≤0.18 | 0.18–0.48 | 0.48–1.06 | >1.06 |
| Case/Person-years | 1556/10,423 | 1499/10,907 | 1531/11,507 | 1524/11,140 |
| All-cause mortality | ||||
| No. events (n) | 329 | 303 | 295 | 228 |
| Model 1 | ref | 0.84 (0.64, 1.10) | 0.66 (0.51, 0.85) | 0.54 (0.40, 0.74) |
| Model 2 | ref | 0.96 (0.74, 1.25) | 0.80 (0.64, 1.01) | 0.70 (0.51, 0.97) |
| Model 3 | ref | 0.96 (0.74, 1.26) | 0.81 (0.65, 1.03) | 0.72 (0.51, 1.03) |
| CVD-related mortality | ||||
| No. events (n) | 77 | 79 | 72 | 54 |
| Model 1 | ref | 0.93 (0.56, 1.53) | 0.66 (0.39, 1.11) | 0.46 (0.24, 0.90) |
| Model 2 | ref | 1.07 (0.64, 1.80) | 0.82 (0.48, 1.40) | 0.60 (0.30, 1.20) |
| Model 3 | ref | 1.09 (0.62, 1.92) | 0.83 (0.49, 1.42) | 0.61 (0.29, 1.29) |
| Cancer-related mortality | ||||
| No. events (n) | 71 | 62 | 70 | 62 |
| Model 1 | ref | 0.66 (0.38, 1.14) | 0.65 (0.40, 1.04) | 0.62 (0.34, 1.14) |
| Model 2 | ref | 0.73 (0.41, 1.29) | 0.77 (0.46, 1.29) | 0.79 (0.41, 1.53) |
| Model 3 | ref | 0.74 (0.42, 1.30) | 0.82 (0.49, 1.38) | 0.91 (0.45, 1.83) |
| Flavonols (mg/day) | ≤6.58 | 6.58–12.17 | 12.17–21.55 | >21.55 |
| Case/Person-years | 1528/10,420 | 1528/11,087 | 1526/10,964 | 1528/11,506 |
| All-cause mortality | ||||
| No. events (n) | 336 | 312 | 290 | 217 |
| Model 1 | ref | 0.74 (0.60, 0.90) | 0.73 (0.59, 0.89) | 0.53 (0.39, 0.71) |
| Model 2 | ref | 0.80 (0.64, 1.00) | 0.86 (0.69, 1.06) | 0.63 (0.46, 0.86) |
| Model 3 | ref | 0.82 (0.64, 1.05) | 0.87 (0.68, 1.12) | 0.66 (0.46, 0.94) |
| CVD-related mortality | ||||
| No. events (n) | 70 | 82 | 78 | 52 |
| Model 1 | ref | 0.81 (0.49, 1.34) | 0.78 (0.49, 1.24) | 0.57 (0.29, 1.14) |
| Model 2 | ref | 0.88 (0.50, 1.53) | 0.90 (0.52, 1.55) | 0.72 (0.32, 1.58) |
| Model 3 | ref | 0.91 (0.51, 1.64) | 0.94 (0.51, 1.73) | 0.76 (0.33, 1.77) |
| Cancer-related mortality | ||||
| No. events (n) | 78 | 74 | 61 | 52 |
| Model 1 | ref | 0.81 (0.54, 1.20) | 0.73 (0.44, 1.20) | 0.46 (0.28, 0.77) |
| Model 2 | ref | 0.92 (0.63, 1.35) | 0.86 (0.52, 1.42) | 0.49 (0.28, 0.87) |
| Model 3 | ref | 0.93 (0.61, 1.42) | 0.89 (0.52, 1.52) | 0.52 (0.28, 0.96) |
| Total Isoflavones (mg/day) | ≤0.01 | >0.01 |
|---|---|---|
| Case/Person-years | 3291/23,505 | 2819/20,473 |
| All-cause mortality | ||
| No. events (n) | 699 | 456 |
| HR (95% Cl) | ||
| Model 1 | ref | 0.72 (0.61, 0.84) |
| Model 2 | ref | 0.77 (0.65, 0.92) |
| Model 3 | ref | 0.79 (0.67, 0.93) |
| CVD-related mortality | ||
| No. events (n) | 171 | 111 |
| HR (95% Cl) | ||
| Model 1 | ref | 0.67 (0.48, 0.94) |
| Model 2 | ref | 0.72 (0.51, 1.01) |
| Model 3 | ref | 0.73 (0.52, 1.03) |
| Cancer-related mortality | ||
| No. events (n) | 164 | 101 |
| HR (95% Cl) | ||
| Model 1 | ref | 0.75 (0.56, 0.99) |
| Model 2 | ref | 0.81 (0.59, 1.11) |
| Model 3 | ref | 0.82 (0.59, 1.13) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.; Lu, T.; Yang, R.; Zhou, S. Associations of Flavonoid Intakes with Mortality among Populations with Hypertension: A Prospective Cohort Study. Nutrients 2024, 16, 1534. https://doi.org/10.3390/nu16101534
Wang K, Lu T, Yang R, Zhou S. Associations of Flavonoid Intakes with Mortality among Populations with Hypertension: A Prospective Cohort Study. Nutrients. 2024; 16(10):1534. https://doi.org/10.3390/nu16101534
Chicago/Turabian StyleWang, Kang, Taotao Lu, Rukai Yang, and Shenghua Zhou. 2024. "Associations of Flavonoid Intakes with Mortality among Populations with Hypertension: A Prospective Cohort Study" Nutrients 16, no. 10: 1534. https://doi.org/10.3390/nu16101534
APA StyleWang, K., Lu, T., Yang, R., & Zhou, S. (2024). Associations of Flavonoid Intakes with Mortality among Populations with Hypertension: A Prospective Cohort Study. Nutrients, 16(10), 1534. https://doi.org/10.3390/nu16101534