
Assessing Lifestyle Patterns and Their Influence on Weight Status in Students from a High School in Sibiu, Romania: An Adaptation of ISCOLE Questionnaires and the Child Feeding Questionnaire
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
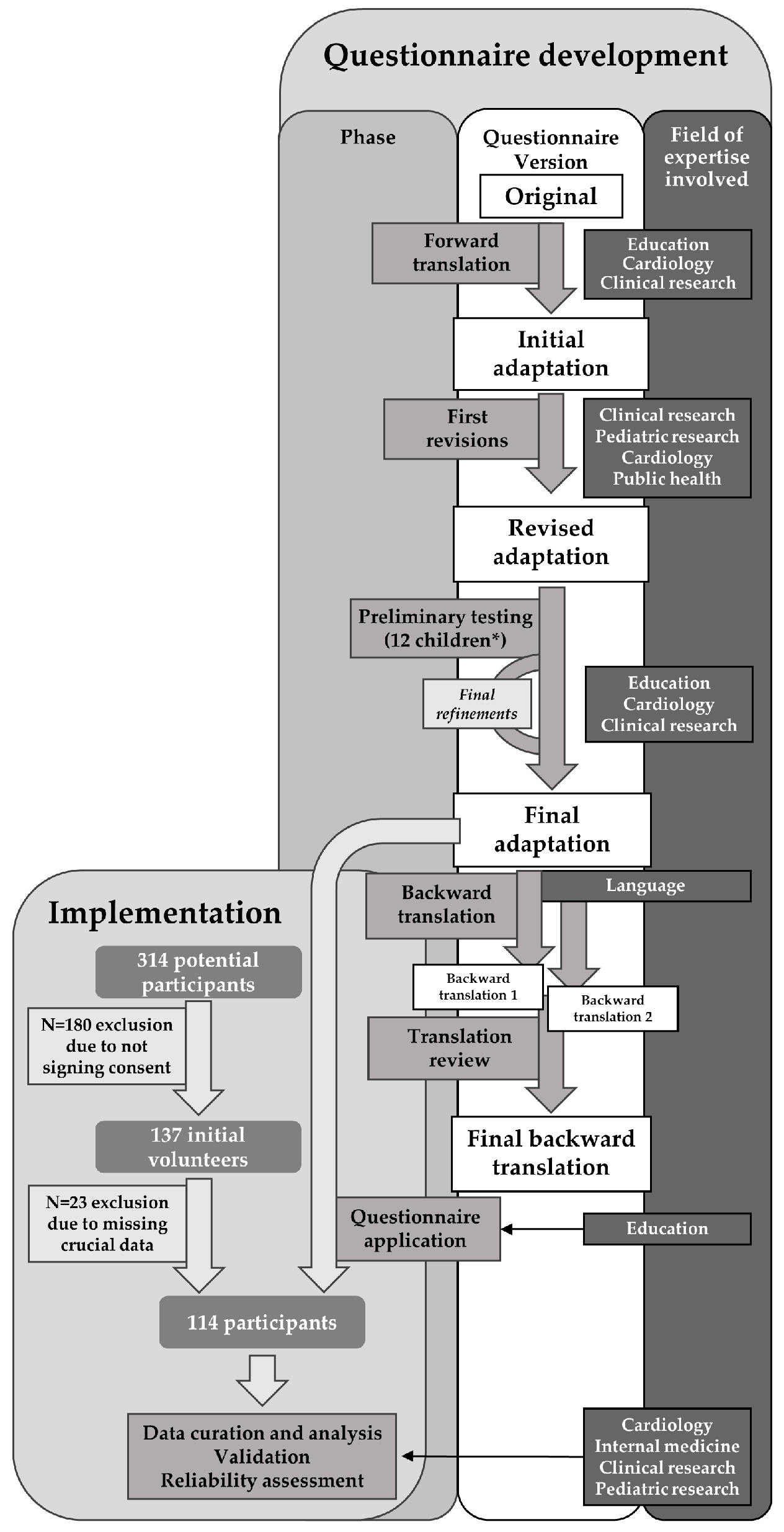
2.2. Adapting the Questionnaire
2.2.1. Assembling the Expert Committee
2.2.2. Adaptation and Translation
2.3. Data Collection and Structure
2.3.1. Child Demographics
2.3.2. Anthropometric Data
2.3.3. Family Demographics, Health, and History
2.3.4. Physical Activity, Sedentary Time, and Sleep Patterns
2.3.5. Dietary Patterns and Attitudes
2.3.6. School Performance
2.4. Preliminary Testing
2.5. Inclusion/Exclusion Criteria
2.6. Statistical Analysis
2.7. Questionnaire Validation
3. Results
3.1. Demographic Data
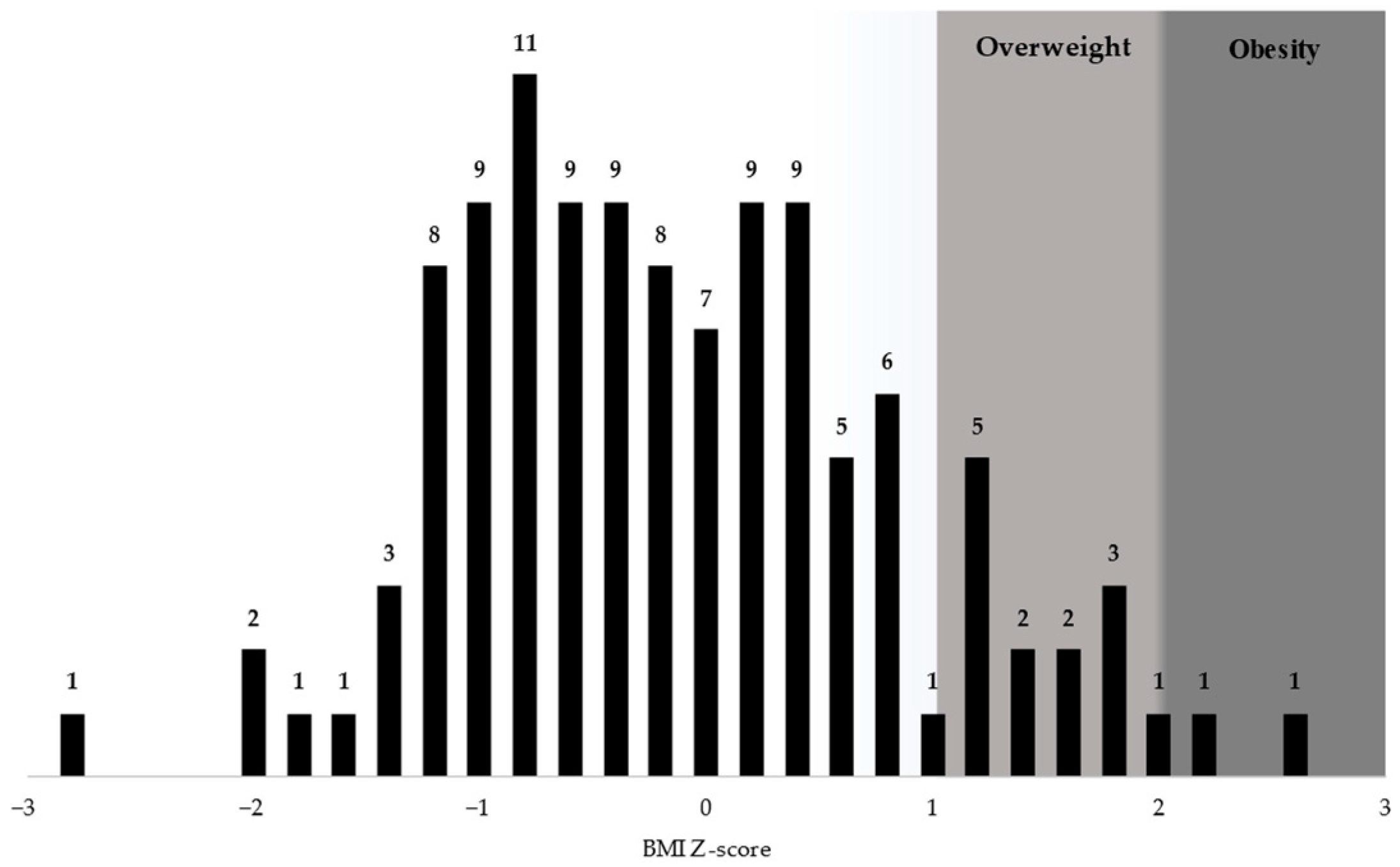
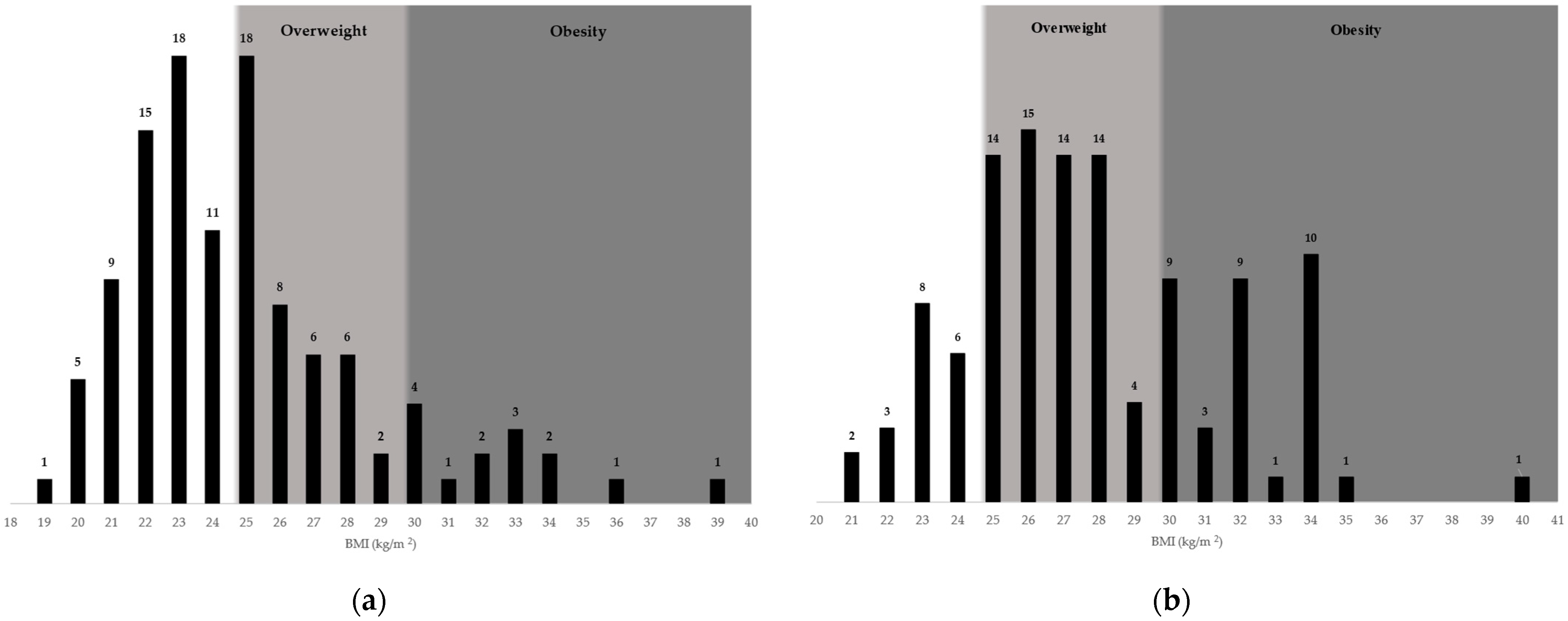
3.2. Anthropometric Data and Descriptive Statistics
3.3. Factors Associated with Adolescent Overweight and Obesity
3.3.1. Demographic and Socio-Economic Factors
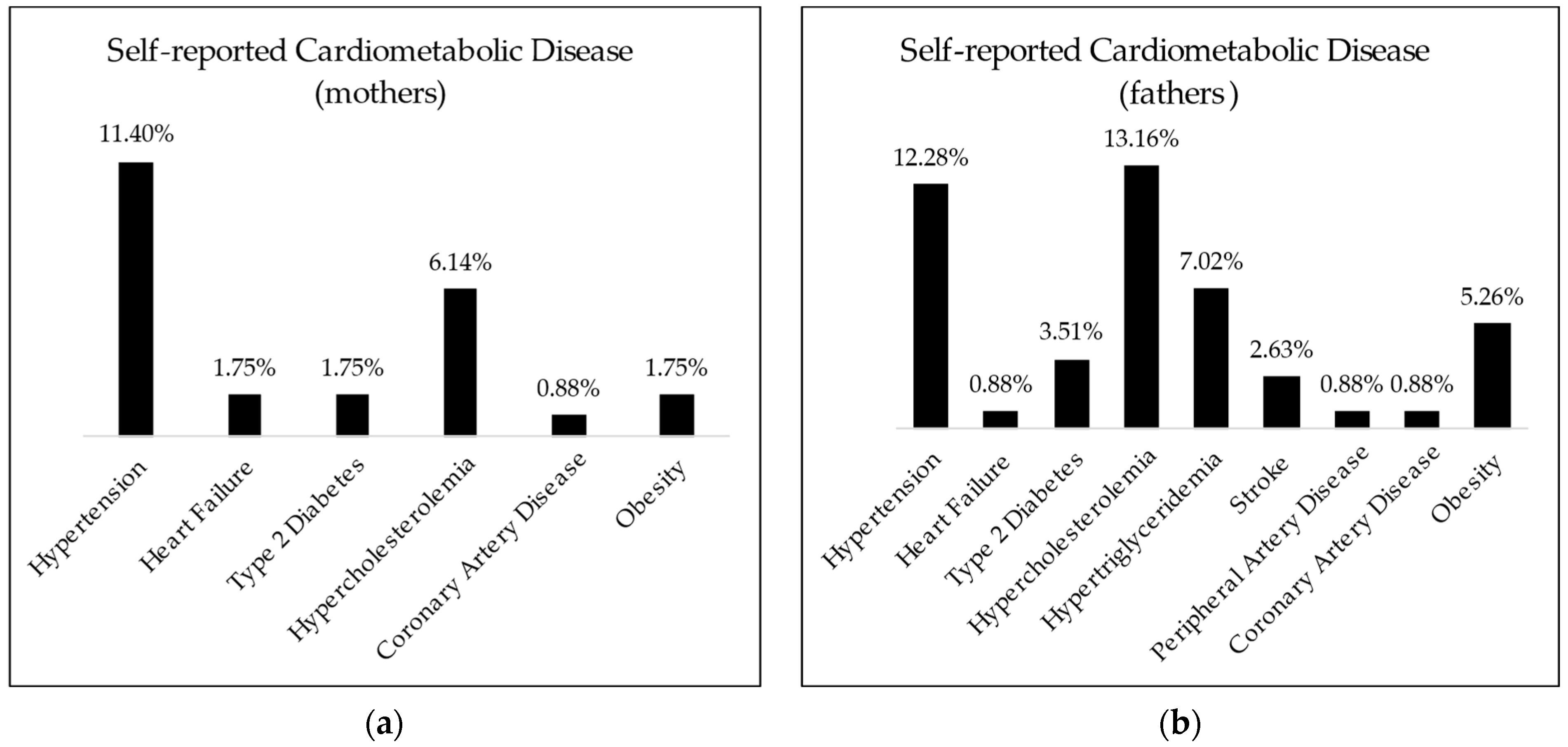
3.3.2. Child and Family Health History
3.3.3. Physical Activity, Sedentary Time, and Sleep Patterns
3.3.4. Dietary Patterns and Attitudes
3.4. Factors Associated with School Performance
3.5. Questionnaire Internal Consistency
4. Discussion
4.1. General Findings
4.2. Questionnaire Validation
4.3. Overall Achievement of Objectives
4.4. Strengths and Limitations
4.5. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Controlling the Global Obesity Pandemic. Available online: https://www.who.int/activities/controlling-the-global-obesity-epidemic (accessed on 24 March 2024).
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 March 2024).
- World Health Organization. Noncommunicable Diseases: Childhood Overweight and Obesity. Available online: https://www.who.int/news-room/q-a-detail/noncommunicable-diseases-childhood-overweight-and-obesity (accessed on 25 March 2024).
- Dietz, W. Critical Periods in Childhood for the Development of Obesity. Am. J. Clin. Nutr. 1994, 59, 955–959. [Google Scholar] [CrossRef]
- Dietz, W.H. Overweight in Childhood and Adolescence. N. Engl. J. Med. 2004, 350, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumanyika, S.; Robinson, T.N.; Scott, B.J.; St. Jeor, S.; Williams, C.L. Overweight in Children and Adolescents. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef] [PubMed]
- Mueller, W.H. The Changes with Age of the Anatomical Distribution of Fat. Soc. Sci. Med. 1982, 16, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Llorente-Cantarero, F.J.; Aguilar-Gómez, F.J.; Anguita-Ruiz, A.; Rupérez, A.I.; Vázquez-Cobela, R.; Flores-Rojas, K.; Aguilera, C.M.; Gonzalez-Gil, E.M.; Gil-Campos, M.; Bueno-Lozano, G.; et al. Changes in Physical Activity Patterns from Childhood to Adolescence: Genobox Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 7227. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting Adult Obesity from Childhood Obesity: A Systematic Review and Meta-Analysis. Obes. Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory Factor Analysis of the Child Feeding Questionnaire: A Measure of Parental Attitudes, Beliefs and Practices about Child Feeding and Obesity Proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Kaur, H.; Li, C.; Nazir, N.; Choi, W.S.; Resnicow, K.; Birch, L.L.; Ahluwalia, J.S. Confirmatory Factor Analysis of the Child-Feeding Questionnaire among Parents of Adolescents. Appetite 2006, 47, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Design and Methods. BMC Public Health 2013, 13, 900. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Maher, C.; Maia, J.; Olds, T.; Sarmiento, O.L.; Standage, M.; Tremblay, M.S.; et al. International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): Contributions to Understanding the Global Obesity Epidemic. Nutrients 2019, 11, 848. [Google Scholar] [CrossRef]
- Hassapidou, M.; Tzotzas, T.; Makri, E.; Pagkalos, I.; Kaklamanos, I.; Kapantais, E.; Abrahamian, A.; Polymeris, A.; Tziomalos, K. Prevalence and Geographic Variation of Abdominal Obesity in 7- and 9-Year-Old Children in Greece; World Health Organization Childhood Obesity Surveillance Initiative 2010. BMC Public Health 2017, 17, 126. [Google Scholar] [CrossRef] [PubMed]
- European Childhood Obesity Group. Launch COSI Report. Available online: https://www.ecog-obesity.eu/cosi-report/ (accessed on 25 March 2024).
- Negrea, M.O.; Negrea, G.O.; Săndulescu, G.; Neamtu, B.; Costea, R.M.; Teodoru, M.; Cipăian, C.R.; Solomon, A.; Popa, M.L.; Domnariu, C.D. Assessing Obesogenic School Environments in Sibiu County, Romania: Adapting the ISCOLE School Environment Questionnaire. Children 2023, 10, 1746. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M. Recommendations for the Cross-Cultural Adaptation of the DASH and Quick DASH Outcome Measures; Institute for Work and Health: Toronto, ON, Canada, 2007. [Google Scholar]
- Tsang, S.; Royse, C.; Terkawi, A. Guidelines for Developing, Translating, and Validating a Questionnaire in Perioperative and Pain Medicine. Saudi J. Anaesth. 2017, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Castle, M.E.; Tak, C.R. Self-Reported vs RUCA Rural-Urban Classification among North Carolina Pharmacists. Pharm. Pract. 2021, 19, 2406. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.-Y.; Um, Y.-J. Factors Affecting Obesity in Urban and Rural Adolescents: Demographic, Socioeconomic Characteristics, Health Behavior and Health Education. Int. J. Environ. Res. Public Health 2021, 18, 2405. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. BMI-for-Age (5–19 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 25 March 2024).
- World Health Organization. Growth Reference Data for 5–19 Years. Application Tools. Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/application-tools (accessed on 25 March 2024).
- Söderberg, L.; Lind, T.; Karlsland Åkeson, P.; Sandström, A.-K.; Hernell, O.; Öhlund, I. A Validation Study of an Interviewer-Administered Short Food Frequency Questionnaire in Assessing Dietary Vitamin D and Calcium Intake in Swedish Children. Nutrients 2017, 9, 682. [Google Scholar] [CrossRef] [PubMed]
- Allison, C.; Colby, S.; Opoku-Acheampong, A.; Kidd, T.; Kattelmann, K.; Olfert, M.D.; Zhou, W. Accuracy of Self-Reported BMI Using Objective Measurement in High School Students. J. Nutr. Sci. 2020, 9, e35. [Google Scholar] [CrossRef] [PubMed]
- Muthuri, S.K.; Onywera, V.O.; Tremblay, M.S.; Broyles, S.T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Relationships between Parental Education and Overweight with Childhood Overweight and Physical Activity in 9–11 Year Old Children: Results from a 12-Country Study. PLoS ONE 2016, 11, e0147746. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Defining Adult Overweight & Obesity. Available online: https://www.cdc.gov/obesity/basics/adult-defining.html#:~:text=if%20your%20bmi%20is%2018.5,falls%20within%20the%20obesity%20range (accessed on 25 March 2024).
- Yeung, E.H.; Hu, F.B.; Solomon, C.G.; Chen, L.; Louis, G.M.; Schisterman, E.; Willett, W.C.; Zhang, C. Life-Course Weight Characteristics and the Risk of Gestational Diabetes. Diabetologia 2010, 53, 668–678. [Google Scholar] [CrossRef]
- Kassem, Z.; Burmeister, C.; Johnson, D.A.; Dakki, H.; Joseph, C.L.M.; Cassidy-Bushrow, A.E. Reliability of Birth Weight Recall by Parent or Guardian Respondents in a Study of Healthy Adolescents. BMC Res. Notes 2018, 11, 878. [Google Scholar] [CrossRef]
- Qiao, Y.; Ma, J.; Wang, Y.; Li, W.; Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Birth Weight and Childhood Obesity: A 12-Country Study. Int. J. Obes. Suppl. 2015, 5 (Suppl. S2), S74–S79. [Google Scholar] [CrossRef]
- Liu, J.; Tuvblad, C.; Li, L.; Raine, A.; Baker, L.A. Medical Record Validation of Maternal Recall of Pregnancy and Birth Events From a Twin Cohort. Twin Res. Hum. Genet. 2013, 16, 845–860. [Google Scholar] [CrossRef]
- Kidscreen. KIDSCREEN-10 Index. Available online: https://www.kidscreen.org/english/questionnaires/kidscreen-10-index/ (accessed on 25 March 2024).
- Kidscreen. Analysis. Available online: https://www.kidscreen.org/english/analysis/ (accessed on 25 March 2024).
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Relationship between Lifestyle Behaviors and Obesity in Children Ages 9–11: Results from a 12-country Study. Obesity 2015, 23, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Adolescent and School Health. YRBSS Questionnaires. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/questionnaires.htm (accessed on 25 March 2024).
- Gropp, K.; Janssen, I.; Pickett, W. Active Transportation to School in Canadian Youth: Should Injury Be a Concern? Inj. Prev. 2013, 19, 64–67. [Google Scholar] [CrossRef]
- Mullan, E.; Markland, D.; Ingledew, D.K. A Graded Conceptualisation of Self-Determination in the Regulation of Exercise Behaviour: Development of a Measure Using Confirmatory Factor Analytic Procedures. Personal. Individ. Differ. 1997, 23, 745–752. [Google Scholar] [CrossRef]
- Motl, R.W.; Dishman, R.K.; Trost, S.G.; Saunders, R.P.; Dowda, M.; Felton, G.; Ward, D.S.; Pate, R.R. Factorial Validity and Invariance of Questionnaires Measuring Social-Cognitive Determinants of Physical Activity among Adolescent Girls. Prev. Med. 2000, 31, 584–594. [Google Scholar] [CrossRef]
- Olaya-Contreras, P.; Bastidas, M.; Arvidsson, D. Colombian Children with Overweight and Obesity Need Additional Motivational Support at School to Perform Health-Enhancing Physical Activity. J. Phys. Act. Health 2015, 12, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.R.; Carskadon, M.A.; Acebo, C.; Seifer, R.; Fallone, G.; Labyak, S.E.; Martin, J.L. Evidence for the Validity of a Sleep Habits Survey for Adolescents. Sleep 2003, 26, 213–216. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC Healthy Schools. Sleep in Middle and High School Students. Available online: https://www.cdc.gov/healthyschools/features/students-sleep.htm#:~:text=Importance%20of%20Sleep&text=How%20much%20sleep%20someone%20needs,10%20hours%20per%2024%20hours (accessed on 25 March 2024).
- World Health Organization. Inequalities in Children’s Health: HBSC International Report from the 2005/2006 Survey; Currie, C., Gabhainn, S.N., Godeau, E., Roberts, C., Smith, R., Currie, D., Pickett, W., Richter, M., Morgan, A., Barnekow, V., Eds.; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Mikkilä, V.; Vepsäläinen, H.; Saloheimo, T.; Gonzalez, S.A.; Meisel, J.D.; Hu, G.; Champagne, C.M.; Chaput, J.-P.; Church, T.S.; Katzmarzyk, P.T.; et al. An International Comparison of Dietary Patterns in 9–11-Year-Old Children. Int. J. Obes. Suppl. 2015, 5 (Suppl. S2), S17–S21. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Morrison, J.A.; Schreiber, G.; Schumann, B.C.; Crawford, P.B.; Obarzanek, E. Emotion-Induced Eating and Sucrose Intake in Children: The NHLBI Growth and Health Study. Int. J. Eat. Disord. 1999, 25, 389–398. [Google Scholar] [CrossRef]
- Presser, S.; Couper, M.P.; Lessler, J.T.; Martin, E.; Martin, J.; Rothgeb, J.M.; Singer, E. Methods for Testing and Evaluating Survey Questions. Public Opin. Q 2004, 68, 109–130. [Google Scholar] [CrossRef]
- Edwards, J.E.; Thomas, M.D. The Organizational Survey Process. Am. Behav. Sci. 1993, 36, 419–442. [Google Scholar] [CrossRef]
- Sheatsley, P.B. Questionnaire Construction and Item Writing. In Handbook of Survey Research; Elsevier: Amsterdam, The Netherlands, 1983; pp. 195–230. [Google Scholar] [CrossRef]
- Sørensen, T.I.; Holst, C.; Stunkard, A.J.; Skovgaard, L.T. Correlations of Body Mass Index of Adult Adoptees and Their Biological and Adoptive Relatives. Int. J. Obes. Relat. Metab. Disord. 1992, 16, 227–236. [Google Scholar]
- Chaput, J.-P.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Mikkilä, V.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; et al. Outdoor Time and Dietary Patterns in Children around the World. J. Public Health 2018, 40, e493–e501. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.A.; Rodriguez, D.; Schmitz, K.H.; Audrain-McGovern, J. Sleep Duration and Adolescent Obesity. Pediatrics 2013, 131, e1428–e1434. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 8th ed.; Cengage: London, UK, 2018. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equalation Modeling, 4th ed.; Guliford Press: New York, NY, USA, 2016. [Google Scholar]
- Dzielska, A.; Michalska, A.; Kleszczewska, D.; Schönbach, D.M.I.; Marques, A.; Peralta, M.; Demetriou, Y. Translation, Cultural Adaptation and Validation of the Basic Psychological Needs Satisfaction in Active Commuting to and From School (BPNS-ACS) Scale in Polish Students. J. Mother Child 2021, 25, 228–235. [Google Scholar]
- Shah, B.; Tombeau Cost, K.; Fuller, A.; Birken, C.S.; Anderson, L.N. Sex and Gender Differences in Childhood Obesity: Contributing to the Research Agenda. BMJ Nutr. Prev. Health 2020, 3, 387–390. [Google Scholar] [CrossRef]
- Mannino, A.; Sarapis, K.; Moschonis, G. The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review. Nutrients 2022, 14, 5125. [Google Scholar] [CrossRef]
- Cawley, J.; Frisvold, D.; Meyerhoefer, C. The Impact of Physical Education on Obesity among Elementary School Children. J. Health Econ. 2013, 32, 743–755. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC Healthy Schools. Youth Physical Activity Guidelines Toolkit. Available online: https://www.cdc.gov/healthyschools/physicalactivity/guidelines_backup.htm#:~:text=Activity%20Guidelines%20Toolkit-,Introduction,of%20physical%20activity%20each%20day (accessed on 25 March 2024).
- Dorobantu, M.; Tautu, O.-F.; Dimulescu, D.; Sinescu, C.; Gusbeth-Tatomir, P.; Arsenescu-Georgescu, C.; Mitu, F.; Lighezan, D.; Pop, C.; Babes, K.; et al. Perspectives on Hypertension’s Prevalence, Treatment and Control in a High Cardiovascular Risk East European Country. J. Hypertens. 2018, 36, 690–700. [Google Scholar] [CrossRef] [PubMed]
- Kanter, R.; Caballero, B. Global Gender Disparities in Obesity: A Review. Adv. Nutr. 2012, 3, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Negrea, M.O.; Neamtu, B.; Dobrotă, I.; Sofariu, C.R.; Crisan, R.M.; Ciprian, B.I.; Domnariu, C.D.; Teodoru, M. Causative Mechanisms of Childhood and Adolescent Obesity Leading to Adult Cardiometabolic Disease: A Literature Review. Appl. Sci. 2021, 11, 11565. [Google Scholar] [CrossRef]
- Dalrymple, K.V.; Martyni-Orenowicz, J.; Flynn, A.C.; Poston, L.; O’Keeffe, M. Can Antenatal Diet and Lifestyle Interventions Influence Childhood Obesity? A Systematic Review. Matern. Child Nutr. 2018, 14, e12628. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.; Noetel, M.; Parker, P.; Del Pozo Cruz, B.; Biddle, S.; Ronto, R.; Hulteen, R.; Parker, R.; Thomas, G.; De Cocker, K.; et al. An Umbrella Review of the Benefits and Risks Associated with Youths’ Interactions with Electronic Screens. Nat. Hum. Behav. 2023, 8, 82–99. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski, J.K.; Gillison, F.B.; Cumming, S.; Church, T.S.; Katzmarzyk, P.T.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Denstel, K.D.; Fogelholm, M.; et al. Associations between Breakfast Frequency and Adiposity Indicators in Children from 12 Countries. Int. J. Obes. Suppl. 2015, 5 (Suppl. S2), S80–S88. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Skogen, I.B.; Båtevik, F.O.; Krumsvik, R.J.; Høydal, K.L. Weight-Based Victimization and Physical Activity among Adolescents with Overweight or Obesity: A Scoping Review of Quantitative and Qualitative Evidence. Front. Sports Act. Living 2022, 4, 732737. [Google Scholar] [CrossRef] [PubMed]
- Aydi, B.; Selmi, O.; Marsigliante, S.; Souissi, M.A.; Souissi, N.; Muscella, A. Integration of Obese Children in Physical Education Sessions: An Exploratory Study. Children 2023, 10, 133. [Google Scholar] [CrossRef]
- Rozga, M.; Handu, D. Nutrition Interventions for Pediatric Obesity Prevention: An Umbrella Review of Systematic Reviews. Nutrients 2023, 15, 5097. [Google Scholar] [CrossRef]
- Aguirre, M.d.J.X.; Drumond Andrade, F.C.; Aguirre, M.A.C.; Justino, J.R.; Maciel, B.L.L. Social Network, Food Patterns, Physical Activity and Associations with Overweight and Obesity in Adolescents from a School in Rural Brazil. Nutrients 2023, 15, 3305. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Categories | Overweight or Obese | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| Gender | Female | 63 (94%) | 4 (6%) | <0.01 |
| Male | 36 (76.6%) | 11 (23.4%) | ||
| Living environment (real) | Rural | 15 (88.2%) | 2 (11.8%) | 0.606 |
| Urban | 84 (86.6%) | 13 (13.4%) | ||
| Estimated family income (missing = 2) | Below average | 5 (100%) | 0 (0%) | 1 |
| Average | 65 (86.7%) | 10 (13.3%) | ||
| Above average | 28 (87.5%) | 4 (12.5%) | ||
| Maternal higher education | No (ISCED ≤ 4) | 32 (78%) | 9 (22%) | 0.037 |
| Yes (ISCED > 4) | 67 (91.8%) | 6 (8.2%) | ||
| Paternal higher education | No (ISCED ≤ 4) | 40 (85.1%) | 7 (14.9%) | 0.646 |
| Yes (ISCED > 4) | 59 (88.1%) | 8 (11.9%) | ||
| Variable | Categories | Overweight or Obese | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| Term birth (missing = 1) | Pre-term | 7 (87.5%) | 1 (12.5%) | 0.588 |
| On term | 85 (87.6%) | 12 (12.4%) | ||
| Post-term | 6 (75%) | 2 (25%) | ||
| Birth weight (missing = 5) | >4000 g | 5 (55.6%) | 4 (44.4%) | <0.01 |
| ≤4000 g | 90 (90%) | 10 (10%) | ||
| Maternal age at conception | <30 years | 68 (87.2%) | 10 (12.8%) | 1 |
| ≥30 years | 31 (86.1%) | 5 (13.9%) | ||
| Paternal age at conception | <30 years | 46 (86.8%) | 7 (13.2%) | 0.988 |
| ≥30 years | 53 (86.9%) | 8 (13.1%) | ||
| Feeding during first 6 months (missing = 1) | Breastfed (no formula) | 60 (89.6%) | 7 (10.4%) | 0.241 |
| Formula (no breastfeeding) | 7 (70%) | 3 (30%) | ||
| Combined | 31 (86.1%) | 5 (13.9%) | ||
| Maternal obesity | No | 94 (91.3%) | 9 (8.7%) | <0.01 |
| Yes | 5 (45.5%) | 6 (54.5%) | ||
| Paternal obesity | No | 79 (88.8%) | 10 (11.2%) | 0.314 |
| Yes | 20 (80%) | 5 (20%) | ||
| Variable | Weight Status | p-Value | |
|---|---|---|---|
| Normal Weight | Overweight or Obese | ||
| Mean (95% CI) ± StdDev/Median; MIN–MAX (IQR) | |||
| Maternal age (years) | 44.62 (43.78–45.46) ± 4.22 | 44.27 (42.18–46.35) ± 3.77 | 0.762 |
| 44; 34–53 (6) | 43; 37–51 (5) | ||
| Paternal age (years) | 47.34 (46.39–48.29) ± 4.76 | 48 (44.92–51.08) ± 5.57 | 0.171 |
| 47; 38–66 (6) | 47; 8–56 (10) | ||
| Quality of life score | 35.78 (34.58–36.95) ± 5.93 | 37.67 (34.51–40.82) ± 5.69 | 0.248 |
| 36; 20–50 (8) | 38; 30–50 (10) | ||
| Variable | Categories | Overweight or Obese | p-Value | |
|---|---|---|---|---|
| No | Yes | |||
| Active transport category | 1 | 76 (87.4%) | 11 (12.6%) | 0.454 |
| 2 | 10 (76.9%) | 3 (23.1%) | ||
| 3 | 13 (92.9%) | 1 (7.1%) | ||
| Weekday sleep duration | <8 h | 73 (89%) | 9 (11%) | 0.355 |
| ≥8 h | 26 (81.3%) | 6 (18.8%) | ||
| Days participating in PE during school week | 0 | 7 (58.3%) | 5 (41.7%) | <0.01 |
| ≥1 | 92 (90.2%) | 10 (9.8%) | ||
| Walking distance from home to public spaces with sports equipment (missing = 30) | >10 min | 50 (79.4%) | 13 (15.5%) | 0.017 |
| ≤10 min | 21 (100%) | 0 (0%) | ||
| Variable | Weight Status | p-Value | |
|---|---|---|---|
| Normal Weight | Overweight or Obese | ||
| Mean (95% CI) ± StdDev/Median; MIN–MAX (IQR) | |||
| Hours spent outside (daily average in a week) | 3.38 (3.14–3.61) ± 1.19 | 3.08 (2.28–3.88) ± 1.44 | 0.364 |
| 3.21; 0.86–6.14 (1.64) | 3.36; 1–6.43 (1.86) | ||
| Average daily non-academic screen time in a week (hours) | 2.57 (2.24–2.89) ± 1.62 | 2.65 (1.88–3.42) ± 1.39 | 0.75 |
| 2.5; 0–7 (2.28) | 2.57; 0.57–4.86 (2.29) | ||
| Average non-academic screen time during weekends (hours) | 2.96 (2.6–3.3) ± 1.84 | 4.1 (3.1–5.1) ± 1.8 | 0.031 |
| 3; 0–8 (2.5) | 4; 1–7 (3) | ||
| Average time spent watching television during weekends (hours) | 1.14 (0.91–1.37) ± 1.15 | 1.9 (1.09–2.71) ± 1.45 | 0.03 |
| 0.5; 0–5 (2) | 2; 0–5 (2.5) | ||
| Average time spent using the computer during weekends (hours) | 1.83 (1.51–2.13) ± 1.51 | 2.2 (1.29–3.11) ± 1.65 | 0.422 |
| 2; 0–5 (2.5) | 2; 0–5 (2.5) | ||
| Number of days a week of at least 60 min MVPA | 3.34 (2.94–3.74) ± 2.01 | 3.6 (2.67–4.53) ± 1.68 | 0.568 |
| 3; 0–7 (3) | 4; 0–7 (3) | ||
| Intrinsic Motivation for PA Score | 19.32 (18.65–20) ± 3.4 | 19.73 (18.13–21.33) ± 2.89 | 0.923 |
| 20; 11–25 (4) | 21; 14–24 (5) | ||
| Self-Efficacy for PA Score | 27.39 (26.13–28.66) ± 6.34 | 28.47 (25.23–31.71) ± 5.85 | 0.382 |
| 28; 10–40 (9) | 29; 18–40 (8) | ||
| Variable | Weight Status | p-Value | |
|---|---|---|---|
| Normal Weight | Overweight or Obese | ||
| Mean (95%CI) ± StdDev/Median; MIN–MAX (IQR) | |||
| Total weekly unhealthy food portions | 16.22 (13.62–18.82) ± 13.04 | 12.97 (8.51–17.42) ± 8.05 | 0.644 |
| 13; 0–100 (12.5) | 12; 0–27.5 (12.5) | ||
| Total weekly healthy food portions) | 30.97 (27.37–34.58) ± 18.06 | 29.93 (21.89–37.98) ± 14.53 | 0.957 |
| 27; 0–100 (24) | 27.5; 11–70.5 (14) | ||
| Weekly portions of chips | 1.09 (0.76–1.42) ± 1.66 | 0.2 (0–0.43) ± 0.41 | 0.026 |
| 1; 0–10 (1) | 0; 0–1 (<0.01) | ||
| Weekly portions of fruit juice | 2.71 (2.2–3.22) ± 2.56 | 1.23 (0.32–2.15) ± 1.66 | 0.049 |
| 1; 0–10 (4.5) | 1; 0–5.5 (3) | ||
| Total weekly food portions consumed in front of screens | 9.51 (7.88–11.14) ± 8.17 | 8.87 (3.95–13.78) ± 8.89 | 0.930 |
| 7; 0–41.5 (11) | 7.5; 0–37 (9) | ||
| Weekly portions of chips consumed in front of screens | 0.91 (0.68–1.15) ± 1.17 | 0.37 (0–0.8) ± 0.79 | 0.032 |
| 0.5; 0–5.5 (1) | 0; 0–3 (0.5) | ||
| Emotion-induced eating score | 11.31 (10.73–11.89) ± 2.9 | 12.4 (10.85–13.95) ± 2.8 | 0.387 |
| 11; 7–18 (5) | 11; 9–20 (4) | ||
| Variable | Weight Status | p-Value | |
|---|---|---|---|
| Normal Weight | Overweight or Obese | ||
| Mean (95%CI) ± StdDev/Median; MIN–MAX (IQR) | |||
| Monitoring high-fat foods | 3.55 (3.32–3.79) ± 1.15 | 4.27 (3.78–4.76) ± 0.88 | 0.019 |
| 4; 1–5 (1) | 4; 2–5 (1) | ||
| Perceived parent weight in the present | 2.24 (2.15–2.34) ± 0.48 | 2.67 (2.32–3.01) ± 0.62 | <0.01 |
| 2; 1–4 (<0.01) | 3; 2–4 (1) | ||
| Perceived child weight during first year of life | 1.93 (1.86–1.99) ± 0.336 | 2.13 (1.85–2.42) ± 0.516 | 0.049 |
| 2; 1–3 (<0.01) | 2; 1–3 (<0.01) | ||
| Perceived child weight during age 2 to 3 | 1.95 (1.88–2.01) ± 0.31 | 2.2 (1.97–2.43) ± 0.41 | <0.01 |
| 2; 1–3 (<0.01) | 2; 2–3 (<0.01) | ||
| Perceived child weight during preschool | 1.86 (1.79–1.93) ± 0.35 | 2.2 (1.97–2.43) ± 0.41 | <0.01 |
| 2; 1–2 (<0.01) | 2; 2–3 (<0.01) | ||
| Perceived child weight during primary classes | 1.93 (1.86–1.99) ± 0.34 | 2.27 (2.01–2.52) ± 0.46 | <0.01 |
| 2; 1–3 (<0.01) | 2; 2–3 (1) | ||
| Perceived child weight during Middle School | 2.01 (1.93–2.09) ± 0.37 | 2.47 (2.11–2.82) ± 0.64 | <0.01 |
| 2; 1–3 (<0.01) | 2; 2–4 (1) | ||
| Perceived child weight during High School | 1.94 (1.89–1.99) ± 0.25 | 2.53 (2.18–2.89) ± 0.64 | <0.01 |
| 2; 1–2 (<0.01) | 2; 2–4 (1) | ||
| Concern regarding child weight | 1.78 (1.57–1.98) ± 1 | 3 (2.25–3.75) ± 1.36 | <0.01 |
| 1; 1–5 (2) | 3; 1–5 (2) | ||
| Restriction of sweets | 3.88 (3.66–4.11) ± 1.1 | 4.47 (4.11–4.82) ± 0.64 | 0.041 |
| 4; 1–5 (1) | 5; 3–5 (1) | ||
| Questionnaire | Question Interval | No. of Items after Adaptation | Cronbach’s Alpha (Adapted Items) |
|---|---|---|---|
| ISCOLE-LDQ | 13–20 (Self-Efficacy for PA) | 8 | 0.849 |
| 21–25 (Intrinsic Motivation for PA) | 5 (RC: 21, 23) | 0.52 | |
| 33 (23-FFQ) | 23 | 0.877 | |
| 34 (Screen FFQ) | 9 | 0.753 | |
| 39–45 (Emotional eating) | 7 | 0.723 | |
| 46–56 (Kidscreen-10) | 11 (RC according to official instructions) | 0.798 | |
| CFQ | 1–3 (Perceived Responsibility) | 3 | 0.703 |
| 4, 5, 7 | |||
| (Perceived Parent Weight) | 3 | 0.438 | |
| 8–13 (Perceived Child Weight) | |||
| 6 | 0.734 | ||
| 14, 16 (Concern) | 2 | 0.671 | |
| 17–23 + new question (Restriction) | 8 | 0.726 | |
| 25–28 (Pressure to Eat) | 4 | 0.677 | |
| 29–31 (Monitor) | 3 | 0.869 | |
| ISCOLE-NHEQ | Section D, 1–17 | 16 | 0.7 |
| (Foods in the Home) | |||
| Section E, 1–5 | 6 | 0.585 | |
| (Where you Shop) | |||
| Section G, 1–5 (Food Shopping) | 5 | 0.275 | |
| Section H, 1–5 (Child’s Play Equipment) | 8 | 0.597 | |
| Section J, 1–13 (Child’s Places for Physical Activity) | 12 | 0.729 | |
| Section L, 1–13 | 9 | 0.795 | |
| (Distance to Locations) | |||
| Section M, 1–4 | 4 | 0.488 | |
| (Family) |
| Investigated Variables | Weight Status Correlation | Interpretation/Previous Findings |
|---|---|---|
| Gender | Higher values in males | Previously described by Shah et al. [54] |
| Maternal higher education | Inverse | Previously described variable correlation associated with country socio-economical status (Katzmarzyk et al.) [13] |
| Maternal obesity | Positive | Similar results by Mannino et al. [55] |
| Birth weight | Positive | Similar results by Qiao et al. [29] |
| Participation in PE classes | Inverse | Similar results by Cawley et al. [56] |
| Walking distance from home to public spaces with sports equipment | Positive | May offer future research directions regarding the impact of publicly available physical activity resources |
| Non-academic screen time during weekends (mostly due to television watching) | Positive | Integral part of previously described effects of sedentary time on childhood weight balance [13] |
| Consumption of potato chips | Inverse | Possibly due to social desirability bias |
| Parental monitoring of high-fat foods | Positive | Similar findings by Birch et al. [10], and Kaur et al. [11] |
| Parental concern regarding child weight | ||
| Parental restriction of sweets | ||
| Parental self-perceived weight (present) | ||
| Parental perceived weight of child (all periods) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negrea, M.O.; Negrea, G.O.; Săndulescu, G.; Neamtu, B.; Solomon, A.; Popa, M.L.; Stoia, O.; Domnariu, C.D.; Teodoru, M. Assessing Lifestyle Patterns and Their Influence on Weight Status in Students from a High School in Sibiu, Romania: An Adaptation of ISCOLE Questionnaires and the Child Feeding Questionnaire. Nutrients 2024, 16, 1532. https://doi.org/10.3390/nu16101532
Negrea MO, Negrea GO, Săndulescu G, Neamtu B, Solomon A, Popa ML, Stoia O, Domnariu CD, Teodoru M. Assessing Lifestyle Patterns and Their Influence on Weight Status in Students from a High School in Sibiu, Romania: An Adaptation of ISCOLE Questionnaires and the Child Feeding Questionnaire. Nutrients. 2024; 16(10):1532. https://doi.org/10.3390/nu16101532
Chicago/Turabian StyleNegrea, Mihai Octavian, Gabriel Octavian Negrea, Gabriela Săndulescu, Bogdan Neamtu, Adelaida Solomon, Mirela Livia Popa, Oana Stoia, Carmen Daniela Domnariu, and Minodora Teodoru. 2024. "Assessing Lifestyle Patterns and Their Influence on Weight Status in Students from a High School in Sibiu, Romania: An Adaptation of ISCOLE Questionnaires and the Child Feeding Questionnaire" Nutrients 16, no. 10: 1532. https://doi.org/10.3390/nu16101532
APA StyleNegrea, M. O., Negrea, G. O., Săndulescu, G., Neamtu, B., Solomon, A., Popa, M. L., Stoia, O., Domnariu, C. D., & Teodoru, M. (2024). Assessing Lifestyle Patterns and Their Influence on Weight Status in Students from a High School in Sibiu, Romania: An Adaptation of ISCOLE Questionnaires and the Child Feeding Questionnaire. Nutrients, 16(10), 1532. https://doi.org/10.3390/nu16101532