


Bioavailability of Lutein from Marigold Flowers (Free vs. Ester Forms): A Randomised Cross-Over Study to Assess Serum Response and Visual Contrast Threshold in Adults

 ,
,
Abstract

1. Introduction
2. Materials and Methods
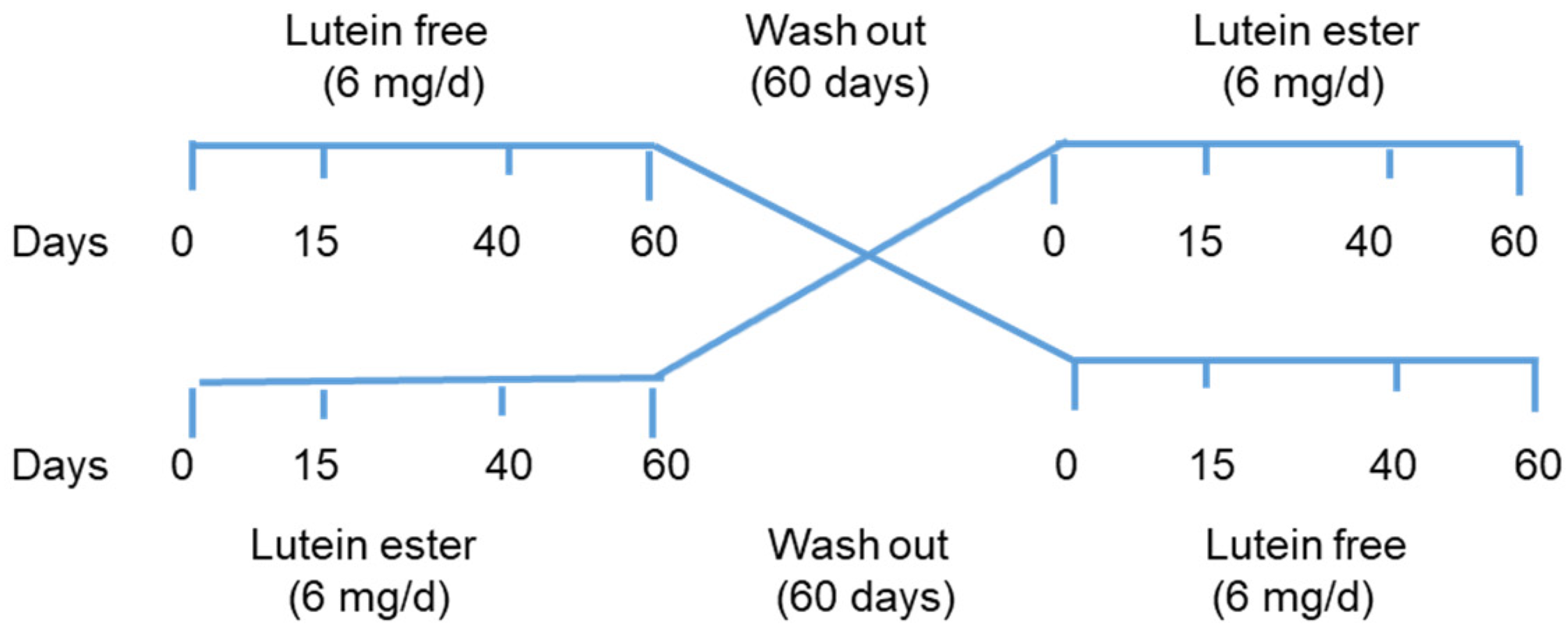
2.1. Subjects and Study Design
2.2. Lutein Supplements
2.3. Assessment of Dietary Intake of Lutein and Carotenoids
2.4. Analysis of Serum Concentrations of Lutein and Zeaxanthin
2.5. Visual Contrast Threshold
2.6. Statistical Analysis
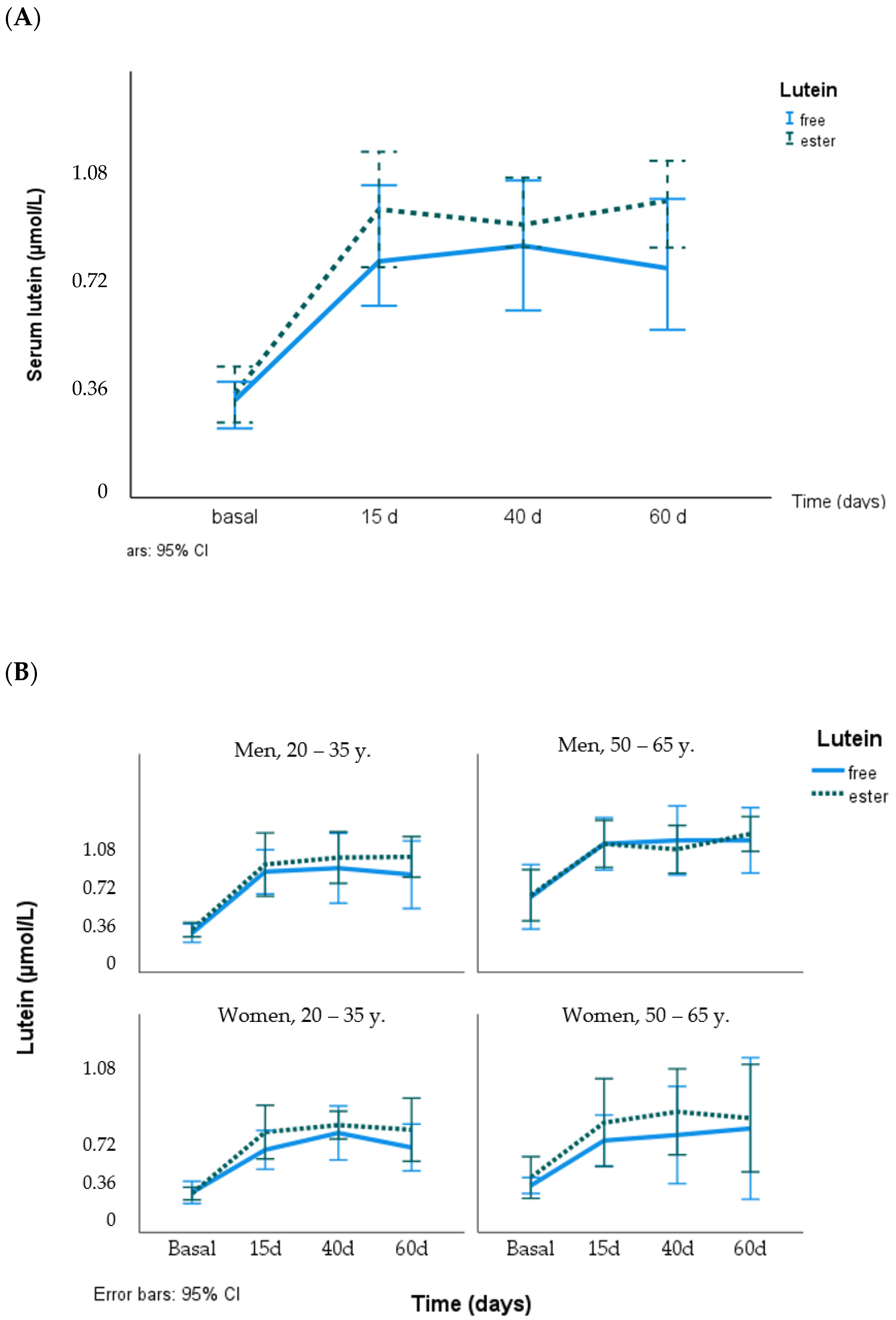
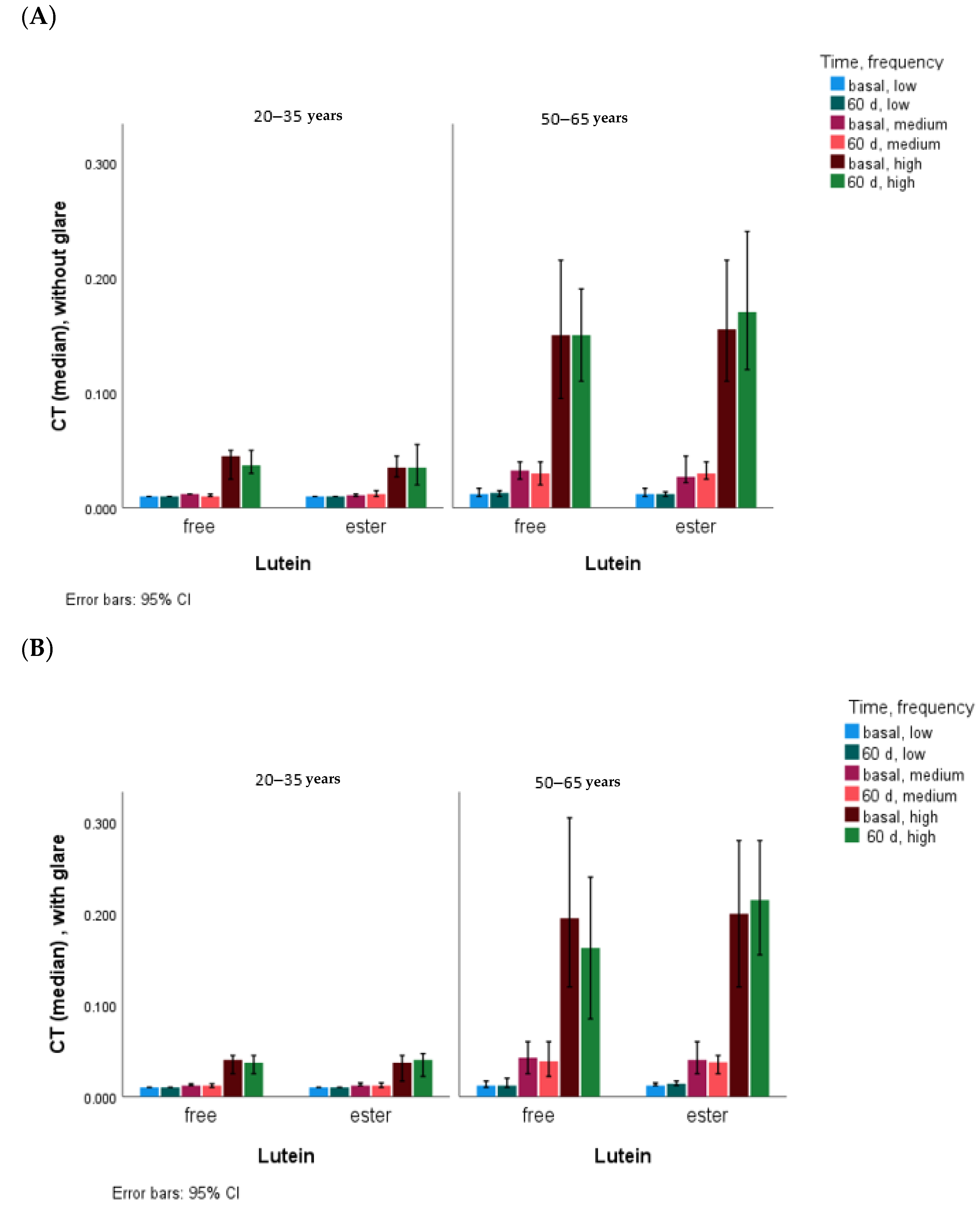
3. Results
4. Discussion
4.1. Serum Lutein and Zeaxanthin and Effect of Lutein Supplementation (Free vs. Ester)
4.2. CT and the Effect of Lutein Supplementation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rodríguez-Concepción, M.; Ávalos, F.J.; Bonet, M.L.; Boronat, A.; Gómez-Gómez, L.; Hornero-Méndez, D.; Limón, C.; Meléndez-Martinez, A.J.; Olmedilla-Alonso, B.; Palou, A.; et al. A global perspective on carotenoids: Metabolism, biotechnology, and benefits for nutrition and health. Prog. Lipid Res. 2018, 70, 62–93. [Google Scholar] [CrossRef] [PubMed]
- Britton, G.; Khachik, F. Carotenoids in food. In Carotenoids—Nutrition and Health; Britton, G., Liaaen-Jensen, S., Pfander, H., Eds.; Birkhauser: Basel, Switzerland, 2009; Volume 5, pp. 45–66. [Google Scholar]
- Mercadante, A.Z.; Rodrigues, D.B.; Petry, F.C.; Mariutti, L.R.B. Carotenoid esters in foods—A review and practical directions on analysis and occurrence. Food Res. Int. 2017, 99, 830–850. [Google Scholar] [CrossRef] [PubMed]
- Hornero-Méndez, D. Ocurrence of carotenoid esters in foods. In Carotenoid Esters in Foods: Physical, Chemical and Biological Properties; Mercadante, A.Z., Ed.; The Royal Society of Chemistry: London, UK, 2019; pp. 182–284. [Google Scholar]
- Olmedilla-Alonso, B.; Estévez-Santiago, R. Dietary intake of carotenoids: Nutritional status assessment and the importance of considering free and esters forms in foods. In Carotenoid Esters in Foods: Physical, Chemical and Biological Properties; Mercadante, A.Z., Ed.; The Royal Society of Chemistry: London, UK, 2019; pp. 375–389. [Google Scholar]
- Seddon, J.M.; Ajani, U.A.; Sperduto, R.D.; Hiller, R.; Blair, N.; Burton, T.C.; Farber, M.D.; Gragoudas, E.S.; Haller, J.; Miller, D.T.; et al. Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye disease case-control study group. JAMA 1994, 272, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Prog. Retin Eye Res. 2016, 50, 34–66. [Google Scholar] [CrossRef] [PubMed]
- Chew, E.Y.; Clemons, T.E.; Agrón, E.; Domalpally, A.; Keenan, T.D.L.; Vitale, S.; Weber, C.; Smith, D.C.; Christen, W.; AREDS2 Research Group. Long-term Outcomes of Adding Lutein/Zeaxanthin and ω-3 Fatty Acids to the AREDS Supplements on Age-Related Macular Degeneration Progression: AREDS2 Report 28. JAMA Ophthalmol. 2022, 140, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Olmedilla, B.; Granado, F.; Blanco, I.; Vaquero, M.; Cajigal, C. Lutein in patients with cataracts and age-related macular degeneration: A long-term supplementation study. J. Sci. Food Agric. 2001, 81, 904–909. [Google Scholar] [CrossRef]
- Hammond, B.R. Dietary carotenoids and the nervous system. Foods 2015, 4, 698–701. [Google Scholar] [CrossRef] [PubMed]
- Mares, J. Lutein and zeaxanthin isomers in eye health and disease. Annu. Rev. Nutr. 2016, 36, 571–602. [Google Scholar] [CrossRef] [PubMed]
- Lindbergh, C.A.; Renzi-Hammond, L.M.; Hammond, B.R.; Terry, D.P.; Mewborn, C.M.; Puente, A.N.; Miller, L.S. Lutein and Zeaxanthin influence brain function in older adults: A randomized controlled trial. J. Int. Neuropsychol. Soc. 2018, 24, 77–90. [Google Scholar] [CrossRef]
- Hammond, B.R.; Renzi-Hammond, L. The influence of the macular carotenoids on women’s eye and brain health. Nutr. Neurosci. 2023, 26, 720–726. [Google Scholar] [CrossRef]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, N.R. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: The Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optometry 2004, 75, 216–229. [Google Scholar] [CrossRef]
- Bartlett, H.E.; Eperjesi, F. Effect of lutein and antioxidant dietary supplementation on contrast sensitivity in age-related macular disease: A randomized controlled trial. Eur. J. Clin. Nutr. 2007, 61, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Allied Market Research©. Lutein and Zeaxanthin Market by Type (Lutein, Zeaxanthin), by Application (Supplements, Cosmetics, Pharmaceuticals, Others): Global Opportunity Analysis and Industry Forecast, 2021–2031. November 2022. Available online: https://www.alliedmarketresearch.com/lutein-and-zeaxanthin-market (accessed on 7 January 2024).
- Ochoa Becerra, M.; Mojica Contreras, L.; Hsieh Lo, M.; Mateos Díaz, J.; Castillo Herrera, G. Lutein as a functional food ingredient: Stability and bioavailability. J. Funct. Foods 2020, 66, 103771. [Google Scholar] [CrossRef]
- Bunea, A.; Socaciu, C.; Pintea, A. Xanthophyll esters in fruits and vegetables. Not. Bot. Horti Agrobot. 2014, 42, 310–324. [Google Scholar] [CrossRef]
- Granado, F.; Olmedilla, B.; Gil-Martínez, E.; Blanco, I. Lutein ester in serum after lutein supplementation in human subjects. Brit. J. Nutr. 1998, 80, 445–449. [Google Scholar] [CrossRef]
- Bowen, P.E.; Herbst-Espinosa, S.M.; Hussain, E.A.; Stacewicz-Sapuntzakis, M. Esterification does not impair lutein bioavailability in humans. J. Nutr. 2002, 132, 3668–3673. [Google Scholar] [CrossRef]
- Landrum, J.; Bone, R.; Mendez, V.; Valenciaga, A.; Babino, D. Comparison of dietary supplementation with lutein diacetate and lutein: A pilot study of the effects on serum and macular pigment. Acta Biochim. Pol. 2012, 59, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Norkus, E.P.; Norkus, K.L.; Dharmarajan, T.S.; Schierle, J.; Schalch, W. Serum lutein response is greater from free lutein than from esterified lutein during 4 weeks of supplementation in healthy adults. J. Am. Coll. Nutr. 2010, 29, 575–585. [Google Scholar] [CrossRef]
- Wu, L.; Huang, X.; Shi, K.; Tan, R. Bioavailability comparison of free and esterified lutein for layer hens. Braz. J. Poult. Sci. 2009, 11, 95–98. [Google Scholar] [CrossRef]
- Yoshizako, H.; Hara, K.; Takai, Y.; Kaidzu, S.; Obana, A.; Ohira, A. Comparison of macular pigment and serum lutein concentration changes between free lutein and lutein esters supplements in Japanese subjects. Acta Ophthalmol. 2016, 94, e411–e416. [Google Scholar] [CrossRef]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 16th ed.; Ediciones Pirámide: Madrid, Spain, 2013. [Google Scholar]
- Estévez Santiago, R.; Beltrán de Miguel, B.; Cuadrado Vives, C.; Olmedilla Alonso, B. Software application for the calculation of dietary intake of individual carotenoids and of its contribution to vitamin A intake. Nutr. Hosp. 2013, 28, 823–829. [Google Scholar] [PubMed]
- Granado, F.; Olmedilla-Alonso, B.; Blanco, I.; Rojas-Hidalgo, E. Carotenoid composition in raw and cooked Spanish vegetables. J. Agric. Food Chem. 1992, 40, 2135–2140. [Google Scholar] [CrossRef]
- Olmedilla, B.; Granado, F.; Blanco, I.; Rojas-Hidalgo, E. Quantitation of Provitamin-A and Non-Provitamin-A Carotenoids in the Fruits Most Commonly Consumed in Spain. In Food and Cancer Prevention: Chemical and Biological Aspects; Waldron, K.W., Johnson, I.T., Fenwick, G.R., Eds.; Royal Society of Chemistry: Cambridge, UK, 1993; pp. 141–145. [Google Scholar]
- Beltrán, B.; Estévez, R.; Cuadrado, C.; Jiménez, S.; Olmedilla Alonso, B. Base de datos de carotenoides para valoración de la ingesta dietética de carotenos, xantofilas y de vitamina A: Utilización en un estudio comparativo del estado nutricional en vitamina A de adultos jóvenes. Nutr. Hosp. 2012, 27, 1334–1343. [Google Scholar] [PubMed]
- Olmedilla, B.; Granado, F.; Gil-Martínez, E.; Blanco, I.; Rojas-Hidalgo, E. Reference levels of retinol, a-tocopherol and main carotenoids in serum of control and insulin-dependent diabetic Spanish subjects. Clin. Chem. 1997, 43, 1066–1071. [Google Scholar] [CrossRef]
- Rodrigues, D.B.; Mercadante, A.Z.; Mariutti, L.R.B. Marigold carotenoids: Much more than lutein esters. Food Res. Internat. 2019, 119, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Eye Disease Case-Control Study Group. Antioxidant status and neovascular age-related macular degeneration. Arch. Ophthalmol. 1993, 111, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Granado, F.; Olmedilla, B.; Blanco, I. Nutritional and clinical relevance of lutein in human health. Br. J. Nutr. 2003, 90, 487–502. [Google Scholar] [CrossRef] [PubMed]
- Ranard, K.M.; Jeon, S.; Mohn, E.S.; Griffiths, J.; Johnson, E.J.; Erdman, J.W., Jr. Dietary guidance for lutein: Consideration for intake recommendations is scientifically supported. Eur. J. Nutr. 2017, 56 (Suppl. S3), 37–42. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, B.; Natoli, S.; Liewx, G.; Flood, M. Lutein and zeaxanthin- food sources, bioavailability and dietary variety in age-related macular degeneration protection. Nutrients 2017, 9, 120. [Google Scholar] [CrossRef]
- Böhm, V.; Lietz, G.; Olmedilla-Alonso, B.; Phelan, D.; Reboul, E.; Bánati, D.; Borel, P.; Corte-Real, J.; de Lera, A.R.; Desmarchelier, C.; et al. From carotenoid intake to carotenoid blood and tissue concentrations—Implications for dietary intake recommendations. Nutr. Rev. 2021, 79, 544–573. [Google Scholar] [CrossRef]
- Olmedilla-Alonso, B.; Beltran-de-Miguel, B.; Estevez-Santiago, R.; Cuadrado-Vives, C. Markers of lutein and zeaxanthin status in two age groups of men and women: Dietary intake, serum concentrations, lipid profile and macular pigment optical density. Nutr. J. 2014, 13, 52. [Google Scholar] [CrossRef]
- Estévez-Santiago, R.; Beltrán-de-Miguel, B.; Olmedilla-Alonso, B. Assessment of dietary lutein, zeaxanthin and lycopene intakes and sources in the Spanish Survey of Dietary Intake (2009–2010). Int. J. Food Sci. Nutr. 2016, 67, 305–313. [Google Scholar] [CrossRef]
- Bone, R.A.; Landrum, J.T. Dose-dependent response of serum lutein and macular pigment optical density to supplementation with lutein esters. Arch. Biochem. Biophys. 2010, 504, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Juturu, V.; Bowman, J.P.; Stringham, N.T.; Stringham, J.M. Bioavailability of lutein/zeaxanthin isomers and macular pigment optical density response to macular carotenoid supplementation: A randomized double blind placebo controlled study. New Front. Ophtahlmol. 2016, 2, 140–145. [Google Scholar] [CrossRef]
- Machida, N.; Kosehira, M.; Kitaichi, N. Clinical effects of dietary supplementation of lutein with high bio-accessibility on macular pigment optical density and contrast sensitivity: A randomized double-blind placebo-controlled parallel-group comparison trial. Nutrients 2020, 12, 2966. [Google Scholar] [CrossRef] [PubMed]
- Olmedilla, B.; Granado, F.; Southon, S.; Wright, A.J.A.; Blanco, I.; Gil-Martínez, E.; Van den Berg, H.; Corridan, B.; Hininger, I.; Thurnham, D.I.; et al. A European multicenter, placebo-controlled intervention trial with a-tocopherol, carotene rich palm-oil, lutein or lycopene at dietary achievable levels. Clin. Sci. 2002, 102, 447–456. [Google Scholar] [CrossRef]
- Breithaupt, D.E.; Weller, P.; Wolters, M.; Hahn, A. Comparison of plasma responses in human subjects after the ingestion of 3R,3R’-zeaxanthin dipalmitate from wolfberry (Lycium barbarum) and non-esterified 3R,3R’-zeaxanthin using chiral high-performance liquid chromatography. Br. J. Nutr. 2004, 91, 707–713. [Google Scholar] [CrossRef]
- Stringham, J.M.; Hammond, B.R., Jr. The glare hypothesis of macular pigment function. Optom. Vis. Sci. 2007, 84, 859–864. [Google Scholar] [CrossRef]
- Hammond, B.R.; Fletcher, L.M.; Roos, F.; Wittwer, J.; Schalch, W. A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8583–8589. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Wang, T.; Zhang, B.; Qin, L.; Wu, C.; Li, Q.; Ma, L. Lutein and zeaxanthin supplementation and association with visual function in age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2014, 56, 252–258. [Google Scholar] [CrossRef]
- Estévez-Santiago, R.; Olmedilla-Alonso, B.; Beltrán-de-Miguel, B. Assessment of lutein and zeaxanthin status and dietary markers as predictors of the contrast threshold in 2 age groups of men and women. Nutr. Res. 2016, 36, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Lawler, T.; Liu, Z.; Nalbandyan, M.; Liu, Y.; Hammond, B.; Wallace, R.B.; Mares, J.A. Lutein and zeaxanthin supplement use is associated with increased macular pigment density over 15 years and greater contrast sensitivity in the Carotenoids in Age-Related Eye Disease Study of older-adult women. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2950. [Google Scholar]
- Yao, Y.; Qiu, A.-H.; Wu, S.-W.; Cai, Z.-Y.; Xu, S.; Liang, X.-Q. Lutein supplementation improves visual performance in Chinese drivers: 1-year randomized, double-blind, placebo-controlled study. Nutrition 2013, 29, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Lin, X.-M.; Zou, A.-Y.; Xu, X.-R.; Li, Y.; Xu, R. A 12-week lutein supplementation improves visual function in Chinese people with long-term computer display light exposure. Br. J. Nutr. 2009, 102, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Yan, S.-F.; Huang, Y.-H.; Lu, X.-R.; Qian, F.; Pan, H.-L.; Xu, X.R.; Zou, Z.Y.; Dong, P.C.; Xiao, X.; et al. Effect of lutein and zeaxanthin on mcular pigment and visual function in patients with early age-related macular degeneration. Ophthalmology 2012, 119, 2290–2297. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Wu, M.; Fu, D.; Yang, S.; Chen, J.; Wilson, K.; Lyons, T.J. Effects of modified LDL and HDL on retinal pigment epithelial cells: A role in diabetic retinopathy? Diabetologia 2013, 56, 2318–2328. [Google Scholar] [CrossRef]
- Fernandez-Garcia, E.; Carvajal-Lerida, I.; Jaren-Galan, M.; Garrido-Fernandez, J.; Perez-Galvez, A.; Hornero-Mendez, D. Carotenoids bioavailability from foods: From plant pigments to efficient biological activities. Food. Res. Int. 2012, 46, 438–450. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Free Lutein Group (n = 24) | Lutein Ester Group (n = 24) | Total Group (n = 48) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Lutein | Lutein/Cholesterol | Zeaxanthin | Lutein | Lutein/Cholesterol | Zeaxanthin | Lutein | Zeaxanthin | Lutein + Zeaxanthin | |
| Basal | 0.35 a (0.03) [0.29, 0.42] | 0.11 a (0.01) (0.09, 0.13] | 0.09 a (0.01) [0.07, 0.11] | 0.38 a (0.03) [0.32, 0.44] | 0.12 a (0.47) [0.10, 0.14] | 0.10 a (0.01) [0.08, 0.12] | 0.37 a (0.03) [0.31, 0.42] | 0.10 a (0.01) [0.08, 0.11] | 0.51 a (0.04) [0.43, 0.59] |
| 15 d | 0.81 b (0.04) [0.72, 0.89] | 0.26 b (0.02) [0.22, 0.29] | 0.14 b (0.01) [0.12, 0.16] | 0.90 b (0.06) [0.79, 1.01] | 0.29 b (0.02) [0.25, 0.33] | 0.14 b (0.01) [0.13, 0.16] | 0.85 b (0.04) [0.78, 0.93] | 0.14 b (0.01) [0.13, 0.15] | 1.02 b (0.05) [0.92, 1.12] |
| 40 d | 0.87 b (0.06) [0.74, 1.00] | 0.29 b (0.02) [0.24, 0.34] | 0.16 bc (0.01) [0.13, 0.18] | 0.94 b (0.05) [0.84, 1.04] | 0.31 b (0.02) [0.27, 0.36] | 0.16 bc (0.01) [0.14, 0.18] | 0.91 b (0.04) [0.83, 0.99] | 0.16 c (0.01) [0.14, 0.17] | 1.10 c (0.05) [1.03, 1.20] |
| 60 d | 0.84 b (0.07) [0.69, 0.99] | 0.27 b (0.03) [0.22, 0.33] | 0.16 b (0.01) [0.13, 0.18] | 0.96 b (0.06) [0.84, 1.07] | 0.31 b (0.02) [0.27, 0.04] | 0.17 b (0.01) [0.15, 0.19] | 0.90 b (0.05) [0.80, 1.00] | 0.16 c (0.01) [0.15, 0.18] | 1.08 c (0.06) [0.96, 1.20] |
| Contrast Threshold | |||
|---|---|---|---|
| Visual Angle of the Estimulus (°) | without Glare | with Glare | |
| Baseline | Baseline | p-value | |
| 6.3° and 4.0° (mean) | 0.013 ± 0.013 [0.010] | 0.013 ± 0.008 [0.010] a | 0.145 |
| 2.5° and 1.6 (mean) | 0.026 ± 0.038 [0.029] | 0.037 ± 0.056 [0.017] | <0.001 |
| 1.0° and 0.7° (mean) | 0.108 ± 0.108 [0.050] | 0.118 ± 0.109 [0.060] | 0.009 |
| 60 days | 60 days | ||
| 6.3° and 4.0° (mean) | 0.016 ± 0.038 [0.010] | 0.014 ± 0.011 [0.010] b | 0.050 |
| 2.5° and 1.6 (mean) | 0.027 ± 0.044 [0.016] | 0.033 ± 0.046 [0.020] | <0.001 |
| 1.0° and 0.7° (mean) | 0.105 ± 0.010 [0.055] | 0.112 ± 0.105 [0.070] | 0.040 |
| Visual Angle of the Estimulus (°) | Lutein | Lutein + Zeaxanthin | Lutein/Cholesterol | Lutein | Lutein + Zeaxanthin | Lutein/Cholesterol |
|---|---|---|---|---|---|---|
| Baseline—without glare | Baseline—with glare | |||||
| 6.3° and 4.0° | 0.345 [0.001] | 0.329 [0.002] | 0.059 [0.591] | 0.263 [0.010] | 0.220 [0.031] | −0.001 [0.989] |
| 2.5° and 1.6 | 0.376 [<0.001] | 0.293 [0.007] | 0.063 [0.569] | 0.428 [<0.001] | 0.376 [<0.001] | 0.120 [0.245] |
| 1.0° and 0.7° | 0.364 [<0.001] | 0.264 [0.015] | 0.086 [0.434] | 0.359 [<0.001] | 0.325 [0.001] | 0.110 [0.284] |
| 60 days—without glare | 60 days–with glare | |||||
| 6.3° and 4.0° | 0.239 [0.026] | 0.231 [0.032] | 0.019 [0.862] | 0.188 [0.067] | 0.210 [0.040] | −0.031 [0.762] |
| 2.5° and 1.6 | 0.262 [0.015] | 0.276 [0.010] | −0.039 [0.720] | 0.213 [0.037] | 0.254 [0.013] | −0.061 [0.554] |
| 1.0° and 0.7° | 0.170 [0.117] | 0.232 [0.032] | −0.095 [0.386] | 0.322 [0.001] | 0.340 [<0.001] | 0.062 [0.547] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olmedilla-Alonso, B.; Granado-Lorencio, F.; Castro-Feito, J.; Herrero-Barbudo, C.; Blanco-Navarro, I.; Estévez-Santiago, R. Bioavailability of Lutein from Marigold Flowers (Free vs. Ester Forms): A Randomised Cross-Over Study to Assess Serum Response and Visual Contrast Threshold in Adults. Nutrients 2024, 16, 1415. https://doi.org/10.3390/nu16101415
Olmedilla-Alonso B, Granado-Lorencio F, Castro-Feito J, Herrero-Barbudo C, Blanco-Navarro I, Estévez-Santiago R. Bioavailability of Lutein from Marigold Flowers (Free vs. Ester Forms): A Randomised Cross-Over Study to Assess Serum Response and Visual Contrast Threshold in Adults. Nutrients. 2024; 16(10):1415. https://doi.org/10.3390/nu16101415
Chicago/Turabian StyleOlmedilla-Alonso, Begoña, Fernando Granado-Lorencio, Julio Castro-Feito, Carmen Herrero-Barbudo, Inmaculada Blanco-Navarro, and Rocío Estévez-Santiago. 2024. "Bioavailability of Lutein from Marigold Flowers (Free vs. Ester Forms): A Randomised Cross-Over Study to Assess Serum Response and Visual Contrast Threshold in Adults" Nutrients 16, no. 10: 1415. https://doi.org/10.3390/nu16101415
APA StyleOlmedilla-Alonso, B., Granado-Lorencio, F., Castro-Feito, J., Herrero-Barbudo, C., Blanco-Navarro, I., & Estévez-Santiago, R. (2024). Bioavailability of Lutein from Marigold Flowers (Free vs. Ester Forms): A Randomised Cross-Over Study to Assess Serum Response and Visual Contrast Threshold in Adults. Nutrients, 16(10), 1415. https://doi.org/10.3390/nu16101415