


How Can Selected Dietary Ingredients Influence the Development and Progression of Endometriosis?
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
Search Strategy, Study Selection, and Data Extraction
3. The Role of Selected Dietary Components in the Course of Endometriosis
3.1. The Importance of Vitamins in Endometriosis
3.1.1. Vitamins C and E
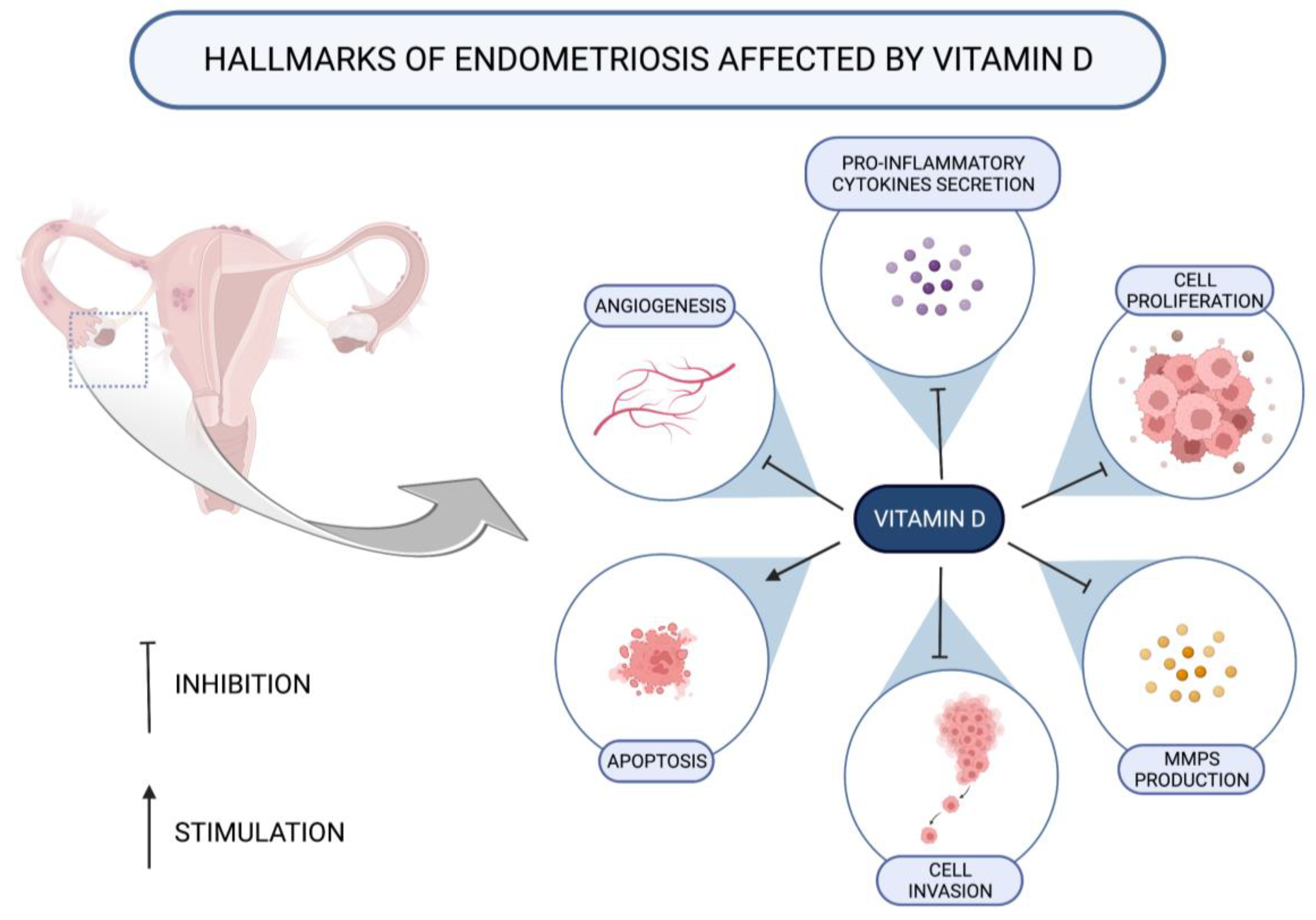
3.1.2. Vitamin D
3.1.3. Vitamin A
3.1.4. B Vitamins
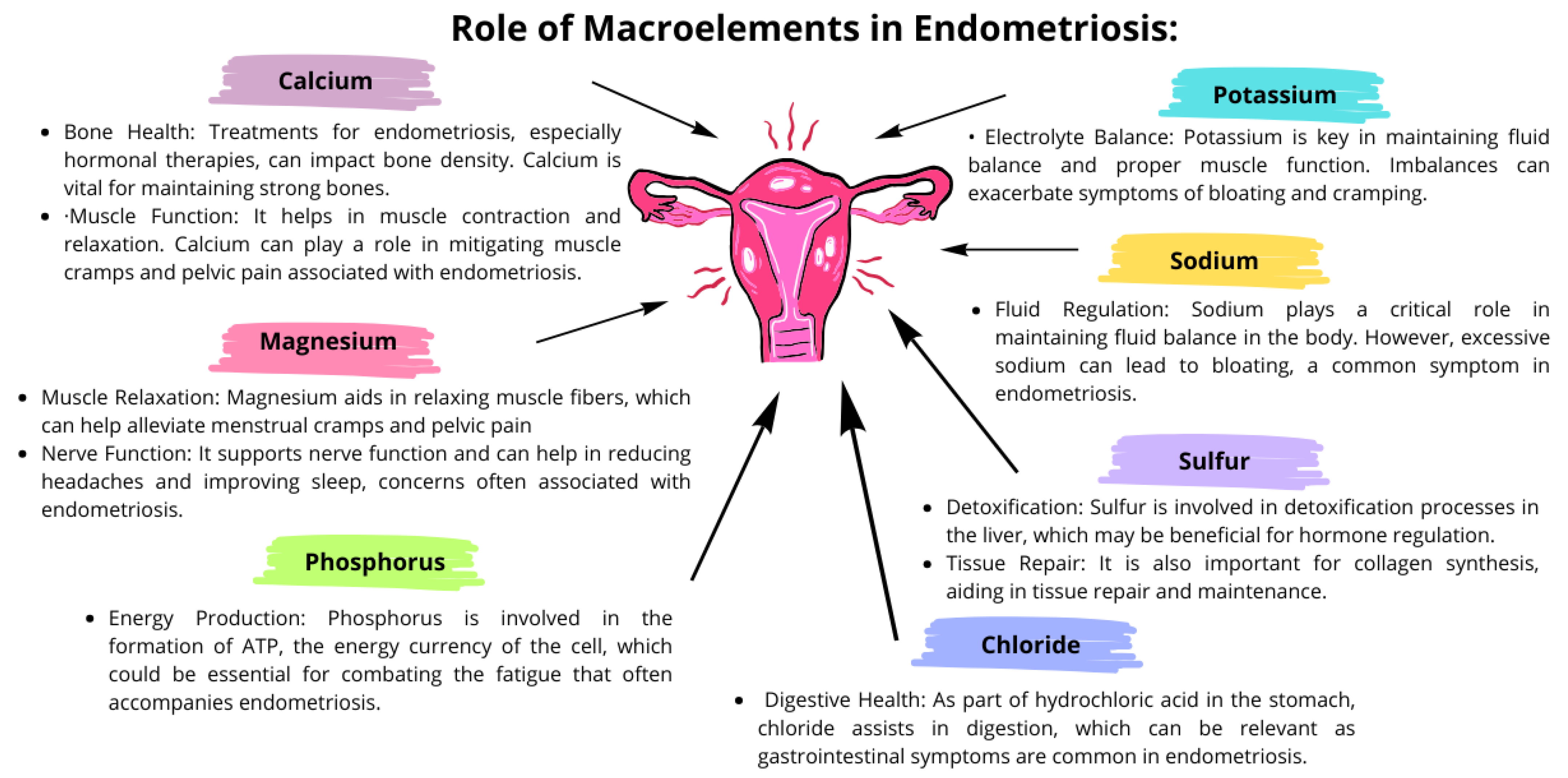
3.2. The Importance of Macroelements in the Course of Endometriosis
3.3. The Importance of Microelements in the Course of Endometriosis
3.3.1. The Importance of Zinc
3.3.2. The Importance of Copper in Endometriosis
3.3.3. The Role of Iron in Endometriosis
3.3.4. The Importance of Selenium in Endometriosis
3.3.5. The Importance of Manganese in Endometriosis
3.3.6. The Importance of Nickel in Endometriosis
3.3.7. The Importance of Chromium in the Course of Endometriosis
3.4. The Importance of Fatty Acids in Endometriosis
Omega-3-PUFA
3.5. The Importance of Carbohydrates
3.6. The Importance of Protein in Endometriosis
3.7. The Influence of Estrogen Derivatives on the Development and Progression of Endometriosis
3.7.1. Effect of Phytoestrogens
3.7.2. Effect of Xenoestrogens
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zondervan, K.T.; Becker, C.M.; Missmer, S.A. Endometriosis. N. Engl. J. Med. 2020, 382, 1244–1256. [Google Scholar] [CrossRef] [PubMed]
- Kalaitzopoulos, D.R.; Lempesis, I.G.; Samartzis, N.; Kolovos, G.; Dedes, I.; Daniilidis, A.; Nirgianakis, K.; Leeners, B.; Goulis, D.G.; Samartzis, E.P. Leptin Concentrations in Endometriosis: A Systematic Review and Meta-Analysis. J. Reprod. Immunol. 2021, 146, 103338. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Aaseth, J.; Doşa, M.D.; Pivina, L.; Dadar, M.; Pen, J.J.; Chirumbolo, S. Does Diet Play a Role in Reducing Nociception Related to Inflammation and Chronic Pain? Nutrition 2019, 66, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Alesi, S.; Villani, A.; Mantzioris, E.; Takele, W.W.; Cowan, S.; Moran, L.J.; Mousa, A. Anti-Inflammatory Diets in Fertility: An Evidence Review. Nutrients 2022, 14, 3914. [Google Scholar] [CrossRef] [PubMed]
- Fabozzi, G.; Verdone, G.; Allori, M.; Cimadomo, D.; Tatone, C.; Stuppia, L.; Franzago, M.; Ubaldi, N.; Vaiarelli, A.; Ubaldi, F.M.; et al. Personalized Nutrition in the Management of Female Infertility: New Insights on Chronic Low-Grade Inflammation. Nutrients 2022, 14, 1918. [Google Scholar] [CrossRef] [PubMed]
- Krabbenborg, I.; De Roos, N.; Van Der Grinten, P.; Nap, A. Diet Quality and Perceived Effects of Dietary Changes in Dutch Endometriosis Patients: An Observational Study. Reprod. BioMed. Online 2021, 43, 952–961. [Google Scholar] [CrossRef]
- Armour, M.; Sinclair, J.; Chalmers, K.J.; Smith, C.A. Self-Management Strategies amongst Australian Women with Endometriosis: A National Online Survey. BMC Complement. Altern. Med. 2019, 19, 17. [Google Scholar] [CrossRef]
- Armour, M.; Middleton, A.; Lim, S.; Sinclair, J.; Varjabedian, D.; Smith, C.A. Dietary Practices of Women with Endometriosis: A Cross-Sectional Survey. J. Altern. Complement. Med. 2021, 27, 771–777. [Google Scholar] [CrossRef]
- Becker, C.M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; et al. ESHRE Guideline: Endometriosis. Human. Reprod. Open 2022, 2022, hoac009. [Google Scholar] [CrossRef]
- Interdonato, L.; Siracusa, R.; Fusco, R.; Cuzzocrea, S.; Di Paola, R. Endocrine Disruptor Compounds in Environment: Focus on Women’s Reproductive Health and Endometriosis. Int. J. Mol. Sci. 2023, 24, 5682. [Google Scholar] [CrossRef]
- Ek, M.; Roth, B.; Ekström, P.; Valentin, L.; Bengtsson, M.; Ohlsson, B. Gastrointestinal Symptoms among Endometriosis Patients—A Case-Cohort Study. BMC Women’s Health 2015, 15, 59. [Google Scholar] [CrossRef] [PubMed]
- Smolarz, B.; Szyłło, K.; Romanowicz, H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). Int. J. Mol. Sci. 2021, 22, 10554. [Google Scholar] [CrossRef]
- Agostinis, C.; Balduit, A.; Mangogna, A.; Zito, G.; Romano, F.; Ricci, G.; Kishore, U.; Bulla, R. Immunological Basis of the Endometriosis: The Complement System as a Potential Therapeutic Target. Front. Immunol. 2021, 11, 599117. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.; Buzzaccarini, G.; Centini, G.; Moawad, G.; Ceccaldi, P.-F.; Gitas, G.; Alkatout, I.; Gullo, G.; Terzic, S.; Sleiman, Z. Impact of Lifestyle and Diet on Endometriosis: A Fresh Look to a Busy Corner. Menopause Rev. 2022, 21, 124–132. [Google Scholar] [CrossRef]
- Roshanzadeh, G.; Jahanian Sadatmahalleh, S.; Moini, A.; Mottaghi, A.; Rostami, F. The Relationship between Dietary Micronutrients and Endometriosis: A Case-Control Study. Int. J. Reprod. Biomed. 2023, 21, 333. [Google Scholar] [CrossRef] [PubMed]
- Yalçın Bahat, P.; Ayhan, I.; Üreyen Özdemir, E.; İnceboz, Ü.; Oral, E. Dietary Supplements for Treatment of Endometriosis: A Review. Acta Biomed. Atenei Parm. 2022, 93, e2022159. [Google Scholar] [CrossRef]
- Jurkiewicz-Przondziono, J.; Lemm, M.; Kwiatkowska-Pamuła, A.; Ziółko, E.; Wójtowicz, M.K. Influence of Diet on the Risk of Developing Endometriosis. Ginekol. Pol. 2017, 88, 96–102. [Google Scholar] [CrossRef]
- Barnard, N.D.; Holtz, D.N.; Schmidt, N.; Kolipaka, S.; Hata, E.; Sutton, M.; Znayenko-Miller, T.; Hazen, N.D.; Cobb, C.; Kahleova, H. Nutrition in the Prevention and Treatment of Endometriosis: A Review. Front. Nutr. 2023, 10, 1089891. [Google Scholar] [CrossRef]
- Monnin, N.; Fattet, A.J.; Koscinski, I. Endometriosis: Update of Pathophysiology, (Epi) Genetic and Environmental Involvement. Biomedicines 2023, 11, 978. [Google Scholar] [CrossRef]
- Cirillo, M.; Argento, F.R.; Becatti, M.; Fiorillo, C.; Coccia, M.E.; Fatini, C. Mediterranean Diet and Oxidative Stress: A Relationship with Pain Perception in Endometriosis. Int. J. Mol. Sci. 2023, 24, 14601. [Google Scholar] [CrossRef]
- Hondal, R.J. Selenium Vitaminology: The Connection between Selenium, Vitamin C, Vitamin E, and Ergothioneine. Curr. Opin. Chem. Biol. 2023, 75, 102328. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.; Levine, M. Vitamin C: The Known and the Unknown and Goldilocks. Oral. Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef] [PubMed]
- Spoelstra-de Man, A.M.E.; Elbers, P.W.G.; Oudemans-Van Straaten, H.M. Vitamin C: Should We Supplement? Curr. Opin. Crit. Care 2018, 24, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Han, S. The Role of Vitamin E in Immunity. Nutrients 2018, 10, 1614. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, T.; Burdeos, G.C.; Itaya, M.; Nakagawa, K.; Miyazawa, T. Vitamin E: Regulatory Redox Interactions: VITAMIN E: REGULATORY REDOX INTERACTIONS. IUBMB Life 2019, 71, 430–441. [Google Scholar] [CrossRef]
- Da Broi, M.G.; De Albuquerque, F.O.; De Andrade, A.Z.; Cardoso, R.L.; Jordão Junior, A.A.; Navarro, P.A. Increased Concentration of 8-Hydroxy-2′-Deoxyguanosine in Follicular Fluid of Infertile Women with Endometriosis. Cell Tissue Res. 2016, 366, 231–242. [Google Scholar] [CrossRef]
- Da Broi, M.G.; Jordão-Jr, A.A.; Ferriani, R.A.; Navarro, P.A. Oocyte Oxidative DNA Damage May Be Involved in Minimal/Mild Endometriosis-Related Infertility. Mol. Reprod. Dev. 2018, 85, 128–136. [Google Scholar] [CrossRef]
- Ferreira, E.M.; Giorgi, V.S.I.; Rodrigues, J.K.; De Andrade, A.Z.; Junior, A.A.J.; Navarro, P.A. Systemic Oxidative Stress as a Possible Mechanism Underlying the Pathogenesis of Mild Endometriosis-Related Infertility. Reprod. BioMed. Online 2019, 39, 785–794. [Google Scholar] [CrossRef]
- Liu, F.; He, L.; Liu, Y.; Shi, Y.; Du, H. The Expression and Role of Oxidative Stress Markers in the Serum and Follicular Fluid of Patients with Endometriosis. Clin. Exp. Obstet. Gynecol. 2013, 40, 372–376. [Google Scholar]
- Ekici, E.İ.; Güney, M.; Nazıroğlu, M. Protective Effect of Cabergoline on Mitochondrial Oxidative Stress-Induced Apoptosis Is Mediated by Modulations of TRPM2 in Neutrophils of Patients with Endometriosis. J. Bioenerg. Biomembr. 2020, 52, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Wu, Z.; Wang, M.; Cheng, W. Effects of Vitamin C on the Outcome of in Vitro Fertilization–Embryo Transfer in Endometriosis: A Randomized Controlled Study. J. Int. Med. Res. 2018, 46, 4624–4633. [Google Scholar] [CrossRef] [PubMed]
- Nishihara, T.; Matsumoto, K.; Hosoi, Y.; Morimoto, Y. Evaluation of Antioxidant Status and Oxidative Stress Markers in Follicular Fluid for Human in Vitro Fertilization Outcome. Reprod. Med. Biol. 2018, 17, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Hoorsan, H.; Simbar, M.; Tehrani, F.R.; Fathi, F.; Mosaffa, N.; Riazi, H.; Akradi, L.; Nasseri, S.; Bazrafkan, S. The Effectiveness of Antioxidant Therapy (Vitamin C) in an Experimentally Induced Mouse Model of Ovarian Endometriosis. Womens Health 2022, 18, 174550572210962. [Google Scholar] [CrossRef] [PubMed]
- Erten, O.U.; Ensari, T.A.; Dilbaz, B.; Cakiroglu, H.; Altinbas, S.K.; Çaydere, M.; Goktolga, U. Vitamin C Is Effective for the Prevention and Regression of Endometriotic Implants in an Experimentally Induced Rat Model of Endometriosis. Taiwan. J. Obstet. Gynecol. 2016, 55, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Durak, Y.; Kokcu, A.; Kefeli, M.; Bildircin, D.; Çelik, H.; Alper, T. Effect of Vitamin C on the Growth of Experimentally Induced Endometriotic Cysts: Vitamin C and Endometriosis Development. J. Obstet. Gynaecol. Res. 2013, 39, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Lin, X.; Xu, W.; Lin, X.; Huang, Q.; Shi, L.; Pan, Y.; Zhang, Y.; Zhu, Y.; Li, C.; et al. MiR-210-3p Protects Endometriotic Cells from Oxidative Stress-Induced Cell Cycle Arrest by Targeting BARD1. Cell Death Dis. 2019, 10, 144. [Google Scholar] [CrossRef]
- Amini, L.; Chekini, R.; Nateghi, M.R.; Haghani, H.; Jamialahmadi, T.; Sathyapalan, T.; Sahebkar, A. The Effect of Combined Vitamin C and Vitamin E Supplementation on Oxidative Stress Markers in Women with Endometriosis: A Randomized, Triple-Blind Placebo-Controlled Clinical Trial. Pain. Res. Manag. 2021, 2021, 5529741. [Google Scholar] [CrossRef]
- Santanam, N.; Kavtaradze, N.; Murphy, A.; Dominguez, C.; Parthasarathy, S. Antioxidant Supplementation Reduces Endometriosis-Related Pelvic Pain in Humans. Transl. Res. 2013, 161, 189–195. [Google Scholar] [CrossRef]
- Darling, A.M.; Chavarro, J.E.; Malspeis, S.; Harris, H.R.; Missmer, S.A. A Prospective Cohort Study of Vitamins B, C, E, and Multivitamin Intake and Endometriosis. J. Endometr. Pelvic Pain. Disord. 2013, 5, 17–26. [Google Scholar] [CrossRef]
- Schink, M.; Konturek, P.C.; Herbert, S.L.; Renner, S.P.; Burghaus, S.; Blum, S.; Fasching, P.A.; Neurath, M.F.; Zopf, Y. Different Nutrient Intake and Prevalence of Gastrointestinal Comorbidities in Women with Endometriosis. J. Physiol. Pharmacol. 2019, 70, 255–268. [Google Scholar] [CrossRef]
- Delrue, C.; Speeckaert, M.M. Vitamin D and Vitamin D-Binding Protein in Health and Disease. Int. J. Mol. Sci. 2023, 24, 4642. [Google Scholar] [CrossRef] [PubMed]
- Ghanavatinejad, A.; Rashidi, N.; Mirahmadian, M.; Rezania, S.; Mosalaei, M.; Ghasemi, J.; Zarnani, A.-H. Vitamin D3 Controls TLR4- and TLR2-Mediated Inflammatory Responses of Endometrial Cells. Gynecol. Obstet. Investig. 2021, 86, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Burjiah, A.; Adi, A.; Widjiati, W. Vitamin D Inhibited Endometriosis Development in Mice Model through Interleukin 17 Modulation. Open Vet. J. 2022, 12, 956. [Google Scholar] [CrossRef] [PubMed]
- Abbas, M.A.; Taha, M.O.; Disi, A.M.; Shomaf, M. Regression of Endometrial Implants Treated with Vitamin D3 in a Rat Model of Endometriosis. Eur. J. Pharmacol. 2013, 715, 72–75. [Google Scholar] [CrossRef]
- Yildirim, B.; Guler, T.; Akbulut, M.; Oztekin, O.; Sariiz, G. 1–Alpha, 25–Dihydroxyvitamin D3 Regresses Endometriotic Implants in Rats by Inhibiting Neovascularization and Altering Regulation of Matrix Metalloproteinase. Postgrad. Med. 2014, 126, 104–110. [Google Scholar] [CrossRef]
- Akyol, A.; Şimşek, M.; İlhan, R.; Can, B.; Baspinar, M.; Akyol, H.; Gül, H.F.; Gürsu, F.; Kavak, B.; Akın, M. Efficacies of Vitamin D and Omega-3 Polyunsaturated Fatty Acids on Experimental Endometriosis. Taiwan J. Obstet. Gynecol. 2016, 55, 835–839. [Google Scholar] [CrossRef]
- Miyashita, M.; Koga, K.; Izumi, G.; Sue, F.; Makabe, T.; Taguchi, A.; Nagai, M.; Urata, Y.; Takamura, M.; Harada, M.; et al. Effects of 1,25-Dihydroxy Vitamin D3 on Endometriosis. J. Clin. Endocrinol. Metab. 2016, 101, 2371–2379. [Google Scholar] [CrossRef]
- Ingles, S.A.; Wu, L.; Liu, B.T.; Chen, Y.; Wang, C.-Y.; Templeman, C.; Brueggmann, D. Differential Gene Expression by 1,25(OH) 2D3 in an Endometriosis Stromal Cell Line. J. Steroid Biochem. Mol. Biol. 2017, 173, 223–227. [Google Scholar] [CrossRef]
- Delbandi, A.-A.; Mahmoudi, M.; Shervin, A.; Zarnani, A.-H. 1,25-Dihydroxy Vitamin D3 Modulates Endometriosis-Related Features of Human Endometriotic Stromal Cells. Am. J. Reprod. Immunol. 2016, 75, 461–473. [Google Scholar] [CrossRef]
- Pazhohan, A.; Amidi, F.; Akbari-Asbagh, F.; Seyedrezazadeh, E.; Aftabi, Y.; Abdolalizadeh, J.; Khodarahmian, M.; Khanlarkhani, N.; Sobhani, A. Expression and Shedding of CD44 in the Endometrium of Women with Endometriosis and Modulating Effects of Vitamin D: A Randomized Exploratory Trial. J. Steroid Biochem. Mol. Biol. 2018, 178, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, N.; Arefi, S.; Sadri, M.; Delbandi, A.-A. Effect of Active Vitamin D on Proliferation, Cell Cycle and Apoptosis in Endometriotic Stromal Cells. Reprod. BioMed. Online 2023, 46, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Ke, J.; Ye, J.; Li, M.; Zhu, Z. The Role of Matrix Metalloproteinases in Endometriosis: A Potential Target. Biomolecules 2021, 11, 1739. [Google Scholar] [CrossRef] [PubMed]
- Pazhohan, A.; Danaei-Mehrabad, S.; Mohamad-Rezaeii, Z.; Amidi, F.; Khodarahmian, M.; Shabani Nashtaei, M.; Sobhani, A.; Farajzadeh, M.A. The Modulating Effects of Vitamin D on the Activity of β-Catenin in the Endometrium of Women with Endometriosis: A Randomized Exploratory Trial. Gynecol. Endocrinol. 2021, 37, 278–282. [Google Scholar] [CrossRef]
- Ma, B.; Hottiger, M.O. Crosstalk between Wnt/β-Catenin and NF-κB Signaling Pathway during Inflammation. Front. Immunol. 2016, 7, 378. [Google Scholar] [CrossRef] [PubMed]
- Yarmolinskaya, M.; Denisova, A.; Tkachenko, N.; Ivashenko, T.; Bespalova, O.; Tolibova, G.; Tral, T. Vitamin D Significance in Pathogenesis of Endometriosis. Gynecol. Endocrinol. 2021, 37, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Delbandi, A.-A.; Torab, M.; Abdollahi, E.; Khodaverdi, S.; Rokhgireh, S.; Moradi, Z.; Heidari, S.; Mohammadi, T. Vitamin D Deficiency as a Risk Factor for Endometriosis in Iranian Women. J. Reprod. Immunol. 2021, 143, 103266. [Google Scholar] [CrossRef]
- Anastasi, E.; Fuggetta, E.; De Vito, C.; Migliara, G.; Viggiani, V.; Manganaro, L.; Granato, T.; Benedetti Panici, P.; Angeloni, A.; Porpora, M.G. Low Levels of 25-OH Vitamin D in Women with Endometriosis and Associated Pelvic Pain. Clin. Chem. Lab. Med. (CCLM) 2017, 55, e282–e284. [Google Scholar] [CrossRef]
- Buggio, L.; Somigliana, E.; Pizzi, M.N.; Dridi, D.; Roncella, E.; Vercellini, P. 25-Hydroxyvitamin D Serum Levels and Endometriosis: Results of a Case–Control Study. Reprod. Sci. 2019, 26, 172–177. [Google Scholar] [CrossRef]
- Dressler, N.; Chandra, A.; Aguirre Dávila, L.; Spineli, L.M.; Schippert, C.; Von Versen-Höynck, F. BMI and Season Are Associated with Vitamin D Deficiency in Women with Impaired Fertility: A Two-Centre Analysis. Arch. Gynecol. Obstet. 2016, 293, 907–914. [Google Scholar] [CrossRef]
- Ciavattini, A.; Serri, M.; Delli Carpini, G.; Morini, S.; Clemente, N. Ovarian Endometriosis and Vitamin D Serum Levels. Gynecol. Endocrinol. 2017, 33, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Mehdizadehkashi, A.; Rokhgireh, S.; Tahermanesh, K.; Eslahi, N.; Minaeian, S.; Samimi, M. The Effect of Vitamin D Supplementation on Clinical Symptoms and Metabolic Profiles in Patients with Endometriosis. Gynecol. Endocrinol. 2021, 37, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Nodler, J.L.; DiVasta, A.D.; Vitonis, A.F.; Karevicius, S.; Malsch, M.; Sarda, V.; Fadayomi, A.; Harris, H.R.; Missmer, S.A. Supplementation with Vitamin D or ω-3 Fatty Acids in Adolescent Girls and Young Women with Endometriosis (SAGE): A Double-Blind, Randomized, Placebo-Controlled Trial. Am. J. Clin. Nutr. 2020, 112, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Almassinokiani, F.; Khodaverdi, S.; Solaymani-dodaran, M.; Akbari, P.; Pazouki, A. Effects of Vitamin D on Endometriosis-Related Pain: A Double-Blind Clinical Trial. Med. Sci. Monit. 2016, 22, 4960–4966. [Google Scholar] [CrossRef]
- Shim, J.Y.; Laufer, M.R.; King, C.R.; Lee, T.T.M.; Einarsson, J.I.; Tyson, N. Evaluation and Management of Endometriosis in the Adolescent. Obstet. Gynecol. 2024, 143, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Pierzchalski, K.; Taylor, R.N.; Nezhat, C.; Jones, J.W.; Napoli, J.L.; Yang, G.; Kane, M.A.; Sidell, N. Retinoic Acid Biosynthesis Is Impaired in Human and Murine Endometriosis1. Biol. Reprod. 2014, 91, 84. [Google Scholar] [CrossRef]
- Yamagata, Y.; Takaki, E.; Shinagawa, M.; Okada, M.; Jozaki, K.; Lee, L.; Sato, S.; Maekawa, R.; Taketani, T.; Asada, H.; et al. Retinoic Acid Has the Potential to Suppress Endometriosis Development. J. Ovarian Res. 2015, 8, 49. [Google Scholar] [CrossRef]
- Samavat, H.; Kurzer, M.S. Estrogen Metabolism and Breast Cancer. Cancer Lett. 2015, 356, 231–243. [Google Scholar] [CrossRef]
- Li, S.; Fu, X.; Wu, T.; Yang, L.; Hu, C.; Wu, R. Role of Interleukin-6 and Its Receptor in Endometriosis. Med. Sci. Monit. 2017, 23, 3801–3807. [Google Scholar] [CrossRef]
- Li, L.; Gao, H.; Pan, L.; Zhao, Y.; Liang, Z.; Zhang, Q.; Wang, D. All-Trans Retinoic Acid Inhibits Epithelial-to-Mesenchymal Transition (EMT) through the down-Regulation of IL-6 in Endometriosis. Ann. Palliat. Med. 2021, 10, 11348–11361. [Google Scholar] [CrossRef]
- Czuba, L.C.; Zhong, G.; Yabut, K.C.; Isoherranen, N. Analysis of Vitamin A and Retinoids in Biological Matrices. In Methods in Enzymology; Elsevier: Amsterdam, The Netherlands, 2020; Volume 637, pp. 309–340. ISBN 978-0-12-820144-2. [Google Scholar]
- Hanna, M.; Jaqua, E.; Nguyen, V.; Clay, J. B Vitamins: Functions and Uses in Medicine. Perm. J. 2022, 26, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Gille, D.; Schmid, A. Vitamin B12 in Meat and Dairy Products. Nutr. Rev. 2015, 73, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.A.; Hafez, H.A.; Kamel, M.A.; Ghamry, H.I.; Shukry, M.; Farag, M.A. Dietary Vitamin B Complex: Orchestration in Human Nutrition throughout Life with Sex Differences. Nutrients 2022, 14, 3940. [Google Scholar] [CrossRef] [PubMed]
- Pattanittum, P.; Kunyanone, N.; Brown, J.; Sangkomkamhang, U.S.; Barnes, J.; Seyfoddin, V.; Marjoribanks, J. Dietary Supplements for Dysmenorrhoea. Cochrane Database Syst. Rev. 2016, 2016, CD002124. [Google Scholar] [CrossRef] [PubMed]
- Abdollahifard, S.; Rahmanian Koshkaki, A.; Moazamiyanfar, R. The Effects of Vitamin B1 on Ameliorating the Premenstrual Syndrome Symptoms. Glob. J. Health Sci. 2014, 6, p144. [Google Scholar] [CrossRef] [PubMed]
- Farag, M.A.; Abib, B.; Qin, Z.; Ze, X.; Ali, S.E. Dietary Macrominerals: Updated Review of Their Role and Orchestration in Human Nutrition throughout the Life Cycle with Sex Differences. Curr. Res. Food Sci. 2023, 6, 100450. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.A.H. Overview of the Vital Roles of Macro Minerals in the Human Body. J. Trace Elem. Miner. 2023, 4, 100076. [Google Scholar] [CrossRef]
- Weyh, C.; Krüger, K.; Peeling, P.; Castell, L. The Role of Minerals in the Optimal Functioning of the Immune System. Nutrients 2022, 14, 644. [Google Scholar] [CrossRef]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A. The Role of Selected Dietary Factors in the Development and Course of Endometriosis. Nutrients 2023, 15, 2773. [Google Scholar] [CrossRef]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of Minerals and Trace Elements in Diabetes and Insulin Resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef]
- Delsouc, M.B.; Ghersa, F.; Ramírez, D.; Della Vedova, M.C.; Gil, R.A.; Vallcaneras, S.S.; Casais, M. Endometriosis Progression in Tumor Necrosis Factor Receptor P55-Deficient Mice: Impact on Oxidative/Nitrosative Stress and Metallomic Profile. J. Trace Elem. Med. Biol. 2019, 52, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Dring, J.C.; Forma, A.; Chilimoniuk, Z.; Dobosz, M.; Teresiński, G.; Buszewicz, G.; Flieger, J.; Cywka, T.; Januszewski, J.; Baj, J. Essentiality of Trace Elements in Pregnancy, Fertility, and Gynecologic Cancers—A State-of-the-Art Review. Nutrients 2021, 14, 185. [Google Scholar] [CrossRef] [PubMed]
- Maret, W. Zinc Biochemistry: From a Single Zinc Enzyme to a Key Element of Life. Adv. Nutr. 2013, 4, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Garzon, S.; Götte, M.; Viganò, P.; Franchi, M.; Ghezzi, F.; Martin, D.C. The Pathogenesis of Endometriosis: Molecular and Cell Biology Insights. Int. J. Mol. Sci. 2019, 20, 5615. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-M.; Yang, W.-X. Epithelial-to-Mesenchymal Transition in the Development of Endometriosis. Oncotarget 2017, 8, 41679–41689. [Google Scholar] [CrossRef] [PubMed]
- Debnath, P.; Huirem, R.S.; Dutta, P.; Palchaudhuri, S. Epithelial–Mesenchymal Transition and Its Transcription Factors. Biosci. Rep. 2022, 42, BSR20211754. [Google Scholar] [CrossRef]
- Lamouille, S.; Xu, J.; Derynck, R. Molecular Mechanisms of Epithelial–Mesenchymal Transition. Nat. Rev. Mol. Cell Biol. 2014, 15, 178–196. [Google Scholar] [CrossRef]
- Kapoor, C.; Vaidya, S.; Wadhwan, V.; Hitesh; Kaur, G.; Pathak, A. Seesaw of Matrix Metalloproteinases (MMPs). J. Can. Res. Ther. 2016, 12, 28. [Google Scholar] [CrossRef]
- Huang, L.; Drake, V.J.; Ho, E. Zinc. Adv. Nutr. 2015, 6, 224–226. [Google Scholar] [CrossRef]
- Singh, A.K.; Chattopadhyay, R.; Chakravarty, B.; Chaudhury, K. Markers of Oxidative Stress in Follicular Fluid of Women with Endometriosis and Tubal Infertility Undergoing IVF. Reprod. Toxicol. 2013, 42, 116–124. [Google Scholar] [CrossRef]
- Di Carlo, C.; Bonifacio, M.; Tommaselli, G.A.; Bifulco, G.; Guerra, G.; Nappi, C. Metalloproteinases, Vascular Endothelial Growth Factor, and Angiopoietin 1 and 2 in Eutopic and Ectopic Endometrium. Fertil. Steril. 2009, 91, 2315–2323. [Google Scholar] [CrossRef] [PubMed]
- Malvezzi, H.; Aguiar, V.G.; de Paz, C.C.P.; Tanus-Santos, J.E.; Penna, I.A.d.A.; Navarro, P.A. Increased Circulating MMP-2 Levels in Infertile Patients With Moderate and Severe Pelvic Endometriosis. Reprod. Sci. 2013, 20, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Duan, S.; Zhang, H.; Chen, Y.; Guo, M. Zinc Deficiency Promoted Fibrosis via ROS and TIMP/MMPs in the Myocardium of Mice. Biol. Trace Elem. Res. 2020, 196, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Scrimgeour, A.G.; Carrigan, C.T.; Condlin, M.L.; Urso, M.L.; Van Den Berg, R.M.; Van Helden, H.P.M.; Montain, S.J.; Joosen, M.J.A. Dietary Zinc Modulates Matrix Metalloproteinases in Traumatic Brain Injury. J. Neurotrauma 2018, 35, 2495–2506. [Google Scholar] [CrossRef]
- Furuya, M.; Masuda, H.; Hara, K.; Uchida, H.; Sato, K.; Sato, S.; Asada, H.; Maruyama, T.; Yoshimura, Y.; Katabuchi, H.; et al. ZEB1 Expression Is a Potential Indicator of Invasive Endometriosis. Acta Obstet. Gynecol. Scand. 2017, 96, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Bartnik, P.; Kacperczyk-Bartnik, J.; Goławski, K.; Sierdziński, J.; Mańka, G.; Kiecka, M.; Lipa, M.; Warzecha, D.; Spaczyński, R.; Piekarski, P.; et al. Plasma and Peritoneal Fluid ZEB Levels in Patients with Endometriosis and Infertility. Biomedicines 2022, 10, 2460. [Google Scholar] [CrossRef] [PubMed]
- Messalli, E.M.; Schettino, M.T.; Mainini, G.; Ercolano, S.; Fuschillo, G.; Falcone, F.; Esposito, E.; Di Donna, M.C.; De Franciscis, P.; Torella, M. The Possible Role of Zinc in the Etiopathogenesis of Endometriosis. Clin. Exp. Obstet. Gynecol. 2014, 41, 541–546. [Google Scholar] [CrossRef]
- Lai, G.-L.; Yeh, C.-C.; Yeh, C.-Y.; Chen, R.-Y.; Fu, C.-L.; Chen, C.-H.; Tzeng, C.-R. Decreased Zinc and Increased Lead Blood Levels Are Associated with Endometriosis in Asian Women. Reprod. Toxicol. 2017, 74, 77–84. [Google Scholar] [CrossRef]
- Jeon, Y.; Yoon, J.D.; Cai, L.; Hwang, S.-U.; Kim, E.; Zheng, Z.; Lee, E.; Kim, D.Y.; Hyun, S.-H. Supplementation of Zinc on Oocyte in Vitro Maturation Improves Preimplatation Embryonic Development in Pigs. Theriogenology 2014, 82, 866–874. [Google Scholar] [CrossRef]
- Duncan, F.E.; Que, E.L.; Zhang, N.; Feinberg, E.C.; O’Halloran, T.V.; Woodruff, T.K. The Zinc Spark Is an Inorganic Signature of Human Egg Activation. Sci. Rep. 2016, 6, 24737. [Google Scholar] [CrossRef]
- Bost, M.; Houdart, S.; Oberli, M.; Kalonji, E.; Huneau, J.-F.; Margaritis, I. Dietary Copper and Human Health: Current Evidence and Unresolved Issues. J. Trace Elem. Med. Biol. 2016, 35, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Kaleler, İ.; Acikgoz, A.S.; Gezer, A.; Uslu, E. A Potential Role of Sirtuin3 and Its Target Enzyme Activities in Patients with Ovarian Endometrioma. Gynecol. Endocrinol. 2021, 37, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.; Divekar, S.D.; Storchan, G.B.; Parodi, D.A.; Martin, M.B. Metals and Breast Cancer. J. Mammary Gland. Biol. Neoplasia 2013, 18, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Thézénas, M.-L.; De Leo, B.; Laux-Biehlmann, A.; Bafligil, C.; Elger, B.; Tapmeier, T.; Morten, K.; Rahmioglu, N.; Dakin, S.G.; Charles, P.; et al. Amine Oxidase 3 Is a Novel Pro-Inflammatory Marker of Oxidative Stress in Peritoneal Endometriosis Lesions. Sci. Rep. 2020, 10, 1495. [Google Scholar] [CrossRef]
- Turgut, A.; Özler, A.; Görük, N.Y.; Tunc, S.Y.; Evliyaoglu, O.; Gül, T. Copper, Ceruloplasmin and Oxidative Stress in Patients with Advanced-Stage Endometriosis. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1472–1478. [Google Scholar]
- Ergaz, Z.; Weinstein-Fudim, L.; Ornoy, A. High Sucrose Low Copper Diet in Pregnant Diabetic Rats Induces Transient Oxidative Stress, Hypoxia, and Apoptosis in the Offspring’s Liver. Birth Defects Res. 2018, 110, 1001–1015. [Google Scholar] [CrossRef]
- Pollack, A.Z.; Louis, G.M.B.; Chen, Z.; Peterson, C.M.; Sundaram, R.; Croughan, M.S.; Sun, L.; Hediger, M.L.; Stanford, J.B.; Varner, M.W.; et al. Trace Elements and Endometriosis: The ENDO Study. Reprod. Toxicol. 2013, 42, 41–48. [Google Scholar] [CrossRef]
- Singh, A.; Ghosh, P.; Mukherjee, S.; Ojha, A.K.; Hansda, A.; Choudhury, P.; Halder, S.; Sharma, S.; Mukherjee, G.; Dasgupta, S.; et al. Transition Metallo-Curcumin Complexes: A New Hope for Endometriosis? J. Mater. Chem. B 2022, 10, 9682–9698. [Google Scholar] [CrossRef]
- Ni, S.; Yuan, Y.; Kuang, Y.; Li, X. Iron Metabolism and Immune Regulation. Front. Immunol. 2022, 13, 816282. [Google Scholar] [CrossRef]
- Ansariniya, H.; Yavari, A.; Javaheri, A.; Zare, F. Oxidative Stress-related Effects on Various Aspects of Endometriosis. Am. J. Rep. Immunol. 2022, 88, e13593. [Google Scholar] [CrossRef]
- Scutiero, G.; Iannone, P.; Bernardi, G.; Bonaccorsi, G.; Spadaro, S.; Volta, C.A.; Greco, P.; Nappi, L. Oxidative Stress and Endometriosis: A Systematic Review of the Literature. Oxidative Med. Cell. Longev. 2017, 2017, 7265238. [Google Scholar] [CrossRef] [PubMed]
- Pascolo, L.; Pachetti, M.; Camillo, A.; Cernogoraz, A.; Rizzardi, C.; Mikus, K.V.; Zanconati, F.; Salomé, M.; Suárez, V.T.; Romano, F.; et al. Detention and Mapping of Iron and Toxic Environmental Elements in Human Ovarian Endometriosis: A Suggested Combined Role. Sci. Total Environ. 2023, 864, 161028. [Google Scholar] [CrossRef] [PubMed]
- Imanaka, S.; Yamada, Y.; Kawahara, N.; Kobayashi, H. A Delicate Redox Balance between Iron and Heme Oxygenase-1 as an Essential Biological Feature of Endometriosis. Arch. Med. Res. 2021, 52, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Polak, G.; Barczyński, B.; Wertel, I.; Kwaśniewski, W.; Bednarek, W.; Derewianka-Polak, M.; Frąszczak, K.; Olajossy, M.; Kotarski, J. Disrupted Iron Metabolism in Peritoneal Fluid May Induce Oxidative Stress in the Peritoneal Cavity of Women with Endometriosis. Ann. Agric. Environ. Med. 2018, 25, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yang, R.; Lan, J.; Wu, Y.; Huang, J.; Fan, Q.; You, Y.; Lin, H.; Jiao, X.; Chen, H.; et al. Iron Overload Modulates Follicular Microenvironment via ROS/HIF-1α/FSHR Signaling. Free Radic. Biol. Med. 2023, 196, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.M.; Papaleo, E.; Corti, L.; Santambrogio, P.; Levi, S.; Vigano, P.; Candiani, M.; Panina-Bordignon, P. Iron Availability Is Increased in Individual Human Ovarian Follicles in Close Proximity to an Endometrioma Compared with Distal Ones. Human. Reprod. 2014, 29, 577–583. [Google Scholar] [CrossRef]
- Alizadeh, M.; Mahjoub, S.; Esmaelzadeh, S.; Hajian, K.; Basirat, Z.; Ghasemi, M. Evaluation of Oxidative Stress in Endometriosis: A Case-Control Study. Casp. J. Intern. Med. 2015, 6, 25–29. [Google Scholar]
- Atiya, H.I.; Frisbie, L.; Goldfeld, E.; Orellana, T.; Donnellan, N.; Modugno, F.; Calderon, M.; Watkins, S.; Zhang, R.; Elishaev, E.; et al. Endometriosis-Associated Mesenchymal Stem Cells Support Ovarian Clear Cell Carcinoma through Iron Regulation. Cancer Res. 2022, 82, 4680–4693. [Google Scholar] [CrossRef]
- Imanaka, S.; Maruyama, S.; Kimura, M.; Nagayasu, M.; Kawahara, N.; Kobayashi, H. Relationship between Cyst Fluid Concentrations of Iron and Severity of Dysmenorrhea in Patients with Ovarian Endometrioma. Gynecol. Obstet. Investig. 2021, 86, 185–192. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Deng, M.; Xu, C.; Zhang, Y.; Wu, D.; Tang, F.; Yang, R.; Miao, J. Ferroptosis Induced by Iron Overload Promotes Fibrosis in Ovarian Endometriosis and Is Related to Subpopulations of Endometrial Stromal Cells. Front. Pharmacol. 2022, 13, 930614. [Google Scholar] [CrossRef]
- Kieliszek, M. Selenium–Fascinating Microelement, Properties and Sources in Food. Molecules 2019, 24, 1298. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Zhao, C.; Hu, H.; Yin, S. Food Sources of Selenium and Its Relationship with Chronic Diseases. Nutrients 2021, 13, 1739. [Google Scholar] [CrossRef] [PubMed]
- Avery, J.; Hoffmann, P. Selenium, Selenoproteins, and Immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Dharmaraj, S. Selenium and Selenoproteins: It’s Role in Regulation of Inflammation. Inflammopharmacol 2020, 28, 667–695. [Google Scholar] [CrossRef] [PubMed]
- Candas, D.; Li, J.J. MnSOD in Oxidative Stress Response-Potential Regulation via Mitochondrial Protein Influx. Antioxid. Redox Signal. 2014, 20, 1599–1617. [Google Scholar] [CrossRef]
- Winarto, H.; Tan, M.; Sadikin, M.; Wanandi, S. Expression Is Down-Regulated by Oxidative Stress in Endometriosis and Endometriosis-Associated Ovarian Cancer. Transl. Oncogenom. 2017, 9, 1177272716689818. [Google Scholar] [CrossRef]
- De Graaf, N.P.J.; Roffel, S.; Gibbs, S.; Kleverlaan, C.J.; Lopez Gonzalez, M.; Rustemeyer, T.; Feilzer, A.J.; Bontkes, H.J. Nickel Allergy Is Associated with a Broad Spectrum Cytokine Response. Contact Dermat. 2023, 88, 10–17. [Google Scholar] [CrossRef]
- Di Gioacchino, M.; Ricciardi, L.; De Pità, O.; Minelli, M.; Patella, V.; Voltolini, S.; Di Rienzo, V.; Braga, M.; Ballone, E.; Mangifesta, R.; et al. Nickel Oral Hyposensitization in Patients with Systemic Nickel Allergy Syndrome. Ann. Med. 2014, 46, 31–37. [Google Scholar] [CrossRef]
- Ricciardi, L.; Arena, A.; Arena, E.; Zambito, M.; Ingrassia, A.; Valenti, G.; Loschiavo, G.; D’Angelo, A.; Saitta, S. Systemic Nickel Allergy Syndrome: Epidemiological Data from Four Italian Allergy Units. Int. J. Immunopathol. Pharmacol. 2014, 27, 131–136. [Google Scholar] [CrossRef]
- Yuk, J.-S.; Kim, Y.J.; Yi, K.-W.; Tak, K.; Hur, J.-Y.; Shin, J.-H. High Rate of Nickel Allergy in Women with Endometriosis: A 3-Year Population-Based Study: Nickel Allergy in Endometriosis. J. Obstet. Gynaecol. Res. 2015, 41, 1255–1259. [Google Scholar] [CrossRef]
- Yuk, J.-S.; Shin, J.S.; Shin, J.-Y.; Oh, E.; Kim, H.; Park, W.I. Nickel Allergy Is a Risk Factor for Endometriosis: An 11-Year Population-Based Nested Case-Control Study. PLoS ONE 2015, 10, e0139388. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Senanayake, H.; Waduge, V. Elevated Levels of Whole Blood Nickel in a Group of Sri Lankan Women with Endometriosis: A Case Control Study. BMC Res. Notes 2013, 6, 13. [Google Scholar] [CrossRef]
- Borghini, R.; Porpora, M.G.; Casale, R.; Marino, M.; Palmieri, E.; Greco, N.; Donato, G.; Picarelli, A. Irritable Bowel Syndrome-Like Disorders in Endometriosis: Prevalence of Nickel Sensitivity and Effects of a Low-Nickel Diet. An Open-Label Pilot Study. Nutrients 2020, 12, 341. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.B. New Evidence against Chromium as an Essential Trace Element. J. Nutr. 2017, 147, 2212–2219. [Google Scholar] [CrossRef]
- Yin, R.V.; Phung, O.J. Effect of Chromium Supplementation on Glycated Hemoglobin and Fasting Plasma Glucose in Patients with Diabetes Mellitus. Nutr. J. 2015, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.B.; Lukaski, H.C. Chromium. Adv. Nutr. 2018, 9, 505–506. [Google Scholar] [CrossRef]
- Field, C.J.; Robinson, L. Dietary Fats. Adv. Nutr. 2019, 10, 722–724. [Google Scholar] [CrossRef]
- Djuricic, I.; Calder, P.C. Beneficial Outcomes of Omega-6 and Omega-3 Polyunsaturated Fatty Acids on Human Health: An Update for 2021. Nutrients 2021, 13, 2421. [Google Scholar] [CrossRef]
- Ishihara, T.; Yoshida, M.; Arita, M. Omega-3 Fatty Acid-Derived Mediators That Control Inflammation and Tissue Homeostasis. Int. Immunol. 2019, 31, 559–567. [Google Scholar] [CrossRef]
- Tomio, K.; Kawana, K.; Taguchi, A.; Isobe, Y.; Iwamoto, R.; Yamashita, A.; Kojima, S.; Mori, M.; Nagamatsu, T.; Arimoto, T.; et al. Omega-3 Polyunsaturated Fatty Acids Suppress the Cystic Lesion Formation of Peritoneal Endometriosis in Transgenic Mouse Models. PLoS ONE 2013, 8, e73085. [Google Scholar] [CrossRef]
- Attaman, J.A.; Stanic, A.K.; Kim, M.; Lynch, M.P.; Rueda, B.R.; Styer, A.K. The Anti-Inflammatory Impact of Omega-3 Polyunsaturated Fatty Acids During the Establishment of Endometriosis-Like Lesions. Am. J. Reprod. Immunol. 2014, 72, 392–402. [Google Scholar] [CrossRef] [PubMed]
- Herington, J.L.; Glore, D.R.; Lucas, J.A.; Osteen, K.G.; Bruner-Tran, K.L. Dietary Fish Oil Supplementation Inhibits Formation of Endometriosis-Associated Adhesions in a Chimeric Mouse Model. Fertil. Steril. 2013, 99, 543–550.e1. [Google Scholar] [CrossRef] [PubMed]
- Stepanow, K.; Ogłuszka, M.; Lepczyński, A.; Poławska, E.; Pierzchała, M. Transgeniczne Myszy Jako Model w Badaniach Wpływu Wielonienasyconych Kwasów Tłuszczowych Na Organizm. Postep. Biochem. 2018, 64, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Kader, A.I.; Gonied, A.S.; Lotfy Mohamed, M.; Mohamed, S.L. Impact of Endometriosis-Related Adhesions on Quality of Life among Infertile Women. Int. J. Fertil Steril. 2019, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Hopeman, M.M.; Riley, J.K.; Frolova, A.I.; Jiang, H.; Jungheim, E.S. Serum Polyunsaturated Fatty Acids and Endometriosis. Reprod. Sci. 2015, 22, 1083–1087. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-H.; Jo, S.; Park, Y.; Lee, H.-H.; Chung, S.-H.; Lee, W.-S. Differences in Omega-3 and Fatty Acid Profiles between Patients with Endometriosis and Those with a Functional Ovarian Cyst. J. Obstet. Gynaecol. 2013, 33, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Youseflu, S.; Sadatmahalleh, S.J.; Mottaghi, A.; Kazemnejad, A. The Association of Food Consumption and Nutrient Intake with Endometriosis Risk in Iranian Women: A Case-Control Study. Int. J. Reprod. Biomed. 2019, 17, 661. [Google Scholar] [CrossRef]
- Schwartz, N.R.M.; Afeiche, M.C.; Terry, K.L.; Farland, L.V.; Chavarro, J.E.; Missmer, S.A.; Harris, H.R. Glycemic Index, Glycemic Load, Fiber, and Gluten Intake and Risk of Laparoscopically Confirmed Endometriosis in Premenopausal Women. J. Nutr. 2022, 152, 2088–2096. [Google Scholar] [CrossRef]
- Markova, M.; Koelman, L.; Hornemann, S.; Pivovarova, O.; Sucher, S.; Machann, J.; Rudovich, N.; Thomann, R.; Schneeweiss, R.; Rohn, S.; et al. Effects of Plant and Animal High Protein Diets on Immune-Inflammatory Biomarkers: A 6-Week Intervention Trial. Clin. Nutr. 2020, 39, 862–869. [Google Scholar] [CrossRef]
- Nieman, K.M.; Anderson, B.D.; Cifelli, C.J. The Effects of Dairy Product and Dairy Protein Intake on Inflammation: A Systematic Review of the Literature. J. Am. Coll. Nutr. 2021, 40, 571–582. [Google Scholar] [CrossRef]
- Ulven, S.M.; Holven, K.B.; Gil, A.; Rangel-Huerta, O.D. Milk and Dairy Product Consumption and Inflammatory Biomarkers: An Updated Systematic Review of Randomized Clinical Trials. Adv. Nutr. 2019, 10, S239–S250. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Zhang, W.; Ge, M.; Sun, Q.; Peng, L.; Cheng, W.; Li, X. Relationship Between Dairy Products Intake and Risk of Endometriosis: A Systematic Review and Dose-Response Meta-Analysis. Front. Nutr. 2021, 8, 701860. [Google Scholar] [CrossRef] [PubMed]
- Steiner, B.M.; Berry, D.C. The Regulation of Adipose Tissue Health by Estrogens. Front. Endocrinol. 2022, 13, 889923. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Mahmoud Abdelshafy, A.; Luo, Z.; Belwal, T.; Lin, X.; Xu, Y.; Wang, L.; Yang, M.; Qi, M.; Dong, Y.; et al. Occurrence, Detection, and Dissipation of Pesticide Residue in Plant-Derived Foodstuff: A State-of-the-Art Review. Food Chem. 2022, 384, 132494. [Google Scholar] [CrossRef] [PubMed]
- Wieczorek, K.; Szczęsna, D.; Jurewicz, J. Environmental Exposure to Non-Persistent Endocrine Disrupting Chemicals and Endometriosis: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5608. [Google Scholar] [CrossRef]
- Youseflu, S.; Jahanian Sadatmahalleh, S.; Roshanzadeh, G.; Mottaghi, A.; Kazemnejad, A.; Moini, A. Effects of Endometriosis on Sleep Quality of Women: Does Life Style Factor Make a Difference? BMC Women’s Health 2020, 20, 168. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Harris, H.R.; Vitonis, A.F.; Chavarro, J.E.; Missmer, S.A. A Prospective Cohort Study of Meat and Fish Consumption and Endometriosis Risk. Am. J. Obstet. Gynecol. 2018, 219, 178.e1–178.e10. [Google Scholar] [CrossRef]
- Canivenc-Lavier, M.-C.; Bennetau-Pelissero, C. Phytoestrogens and Health Effects. Nutrients 2023, 15, 317. [Google Scholar] [CrossRef]
- Bartiromo, L.; Schimberni, M.; Villanacci, R.; Ottolina, J.; Dolci, C.; Salmeri, N.; Viganò, P.; Candiani, M. Endometriosis and Phytoestrogens: Friends or Foes? A Systematic Review. Nutrients 2021, 13, 2532. [Google Scholar] [CrossRef]
- Szukiewicz, D. Insight into the Potential Mechanisms of Endocrine Disruption by Dietary Phytoestrogens in the Context of the Etiopathogenesis of Endometriosis. Int. J. Mol. Sci. 2023, 24, 12195. [Google Scholar] [CrossRef]
- Desmawati, D.; Sulastri, D. Phytoestrogens and Their Health Effect. Open Access Maced. J. Med. Sci. 2019, 7, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Patra, S.; Gorai, S.; Pal, S.; Ghosh, K.; Pradhan, S.; Chakrabarti, S. A Review on Phytoestrogens: Current Status and Future Direction. Phytother. Res. 2023, 37, 3097–3120. [Google Scholar] [CrossRef] [PubMed]
- Petrine, J.C.P.; Del Bianco-Borges, B. The Influence of Phytoestrogens on Different Physiological and Pathological Processes: An Overview. Phytother. Res. 2021, 35, 180–197. [Google Scholar] [CrossRef] [PubMed]
- Lecomte, S.; Demay, F.; Ferrière, F.; Pakdel, F. Phytochemicals Targeting Estrogen Receptors: Beneficial Rather Than Adverse Effects? Int. J. Mol. Sci. 2017, 18, 1381. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Liu, M.; Zhang, B.; Zhao, S.-J.; Jiang, S.-W. Phytoestrogens for the Management of Endometriosis: Findings and Issues. Pharmaceuticals 2021, 14, 569. [Google Scholar] [CrossRef]
- Wang, X.; Ha, D.; Yoshitake, R.; Chan, Y.S.; Sadava, D.; Chen, S. Exploring the Biological Activity and Mechanism of Xenoestrogens and Phytoestrogens in Cancers: Emerging Methods and Concepts. Int. J. Mol. Sci. 2021, 22, 8798. [Google Scholar] [CrossRef]
- Paterni, I.; Granchi, C.; Minutolo, F. Risks and Benefits Related to Alimentary Exposure to Xenoestrogens. Crit. Rev. Food Sci. Nutr. 2017, 57, 3384–3404. [Google Scholar] [CrossRef]
- Wang, L.-H.; Chen, L.-R.; Chen, K.-H. In Vitro and Vivo Identification, Metabolism and Action of Xenoestrogens: An Overview. Int. J. Mol. Sci. 2021, 22, 4013. [Google Scholar] [CrossRef]
- Reddy, V.; McCarthy, M.; Raval, A.P. Xenoestrogens Impact Brain Estrogen Receptor Signaling during the Female Lifespan: A Precursor to Neurological Disease? Neurobiol. Dis. 2022, 163, 105596. [Google Scholar] [CrossRef]
- Bustamante-Barrientos, F.A.; Méndez-Ruette, M.; Ortloff, A.; Luz-Crawford, P.; Rivera, F.J.; Figueroa, C.D.; Molina, L.; Bátiz, L.F. The Impact of Estrogen and Estrogen-Like Molecules in Neurogenesis and Neurodegeneration: Beneficial or Harmful? Front. Cell. Neurosci. 2021, 15, 636176. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Proposed Targets of Vitamin D Action | Authors and Year of the Study | Study Groups | Supplementation Dose of Vitamin D | Detailed Observed Changes | Possible Mechanisms of Vitamin D Action |
|---|---|---|---|---|---|
| Size of the endometriotic lesions | Burjiah et al., 2022 [44] | 24 mice divided into four equal groups | supplementation with 8, 16, or 24 IU of vitamin D for 3 weeks | decreased size of the lesion | mechanism of action was not indicated |
| Abbas et al., 2013 [45] | 21 rats divided into three equal groups | supplementation with 42 μg/kg of cholecalciferol | decreased cross-sectional area of the lesions | mechanism of action was not indicated | |
| Yildirim et al., 2014 [46] | 21 rats divided into three equal groups | supplementation with 0.05 μg/kg of 1,25(OH)2D3 for 4 weeks in 2 groups | decreased weight and decreased volume of lesions | mechanism of action was not indicated | |
| Akyol et al., 2016 [47] | 30 rats divided into three equal groups | supplementation with 42 μg/kg per day of cholecalciferol | no observed changes | - | |
| Matrix Metalloproteinases (MMPs) | Yildrim et al., 2014 [46] | 21 rats divided into three equal groups | supplementation with 0.05 μg/kg of 1,25(OH)2D3 for 4 weeks in 2 groups | decreased MMP-9 expression | mechanism of action was not indicated |
| Miyashita et al., 2016 [48] | isolated human endometriotic stromal cells (hESCs) isolated from 7 patients with endometriosis | incubation with 109 or 107 M 1,25(OH)2D3 | decreased MMP-9 and MMP-2 expression | mechanism of action was not indicated | |
| Ingles et al., 2017 [49] | human endometriotic stromal cells (43 tissue samples) | incubation with 0.1 μM 1,25(OH)2D3 | decreased MMP production | upregulation of the Matrix Metalloproteinase Inhibition pathway | |
| Proinflammatory molecules | Burjiah et al., 2022 [44] | 24 mice divided into four equal groups | supplementation with 8, 16, or 24 IU of vitamin D for 3 weeks | reduced inflammation | decreased production of IL-17 |
| Akyol et al., 2016 [47] | 30 rats divided into three equal groups | supplementation with 42 μg/kg per day of cholecalciferol | reduced inflammation | decreased production of IL-6 | |
| Delbandi et al., 2016 [50] | human endometriotic stromal cells (hESCs) isolated from 25 patients with endometriosis | 107 M 1,25(OH)2 vitamin D3 | reduced inflammation | decreased production of IL-6 | |
| Miyashita et al., 2016 [48] | isolated human endometriotic stromal cells (hESCs) isolated from 7 patients with endometriosis | incubation with 109 or 107 M 1,25(OH)2D3 | reduced inflammation | decreased production of IL-8; decreased production of PGE2; decreased expression of COX-2 mRNA; decreased expression of mPGES1 mRNA; decreased expression of mPGES2 mRNA | |
| Angiogenesis | Delbandi et al., 2016 [50] | human endometriotic stromal cells (hESCs) isolated from 25 patients with endometriosis | 107 M 1,25(OH)2 vitamin D3 | decreased angiogenesis | decreased VEGF-A gene expression |
| Miyashita et al., 2016 [48] | human endometriotic stromal cells (hESCs) isolated from 7 patients with endometriosis | incubation with 109 or 107 M 1,25(OH)2D3 | decreased angiogenesis | inhibition of NF-κB pathway | |
| Invasion | Delbandi et al., 2016 [50] | human endometriotic stromal cells (hESCs) isolated from 25 patients with endometriosis | 107 M 1,25(OH)2 vitamin D3 | reduced invasion, shown as a lower ability of endometriotic cells to digest and migration through the membrane | mechanism of action was not indicated |
| Pazhohan et al., 2018 [51] | blood, endometrial fluid, and tissue samples isolated from 16 patients with endometriosis | supplementation with 50,000 IU of vitamin D weekly for 12–14 weeks | decreased endometriosis cell invasion | elevated expression of CD44 glycoprotein | |
| Proliferation | Delbandi et al., 2016 [50] | human endometriotic stromal cells (hESCs) isolated from 25 patients with endometriosis | 107 M 1,25(OH)2 vitamin D3 | decreased proliferation of endometriosis cells | mechanism of action was not indicated |
| Miyashita et al., 2016 [48] | human endometriotic stromal cells (hESCs) isolated from 7 patients with endometriosis | incubation with 109 or 107 M 1,25(OH)2D3 | decreased proliferation of endometriosis cells | suppressed inhibition of IκBα, leading to reduction of NF-κB pathway activity | |
| Inges et al., 2017 [49] | human endometriotic stromal cells (43 tissue samples) | incubation with 0.1 μM 1,25(OH)2D3 | decreased proliferation of endometriosis cells | down-regulation of genes involved in the axonal guidance pathway | |
| Pazhohan et al., 2021 [51] | blood, endometrial fluid, and tissue samples isolated from 16 patients with endometriosis | supplementation with 50,000 IU of vitamin D weekly for 12–14 weeks | decreased proliferation of endometriosis cells | reduced activity of β-catenin | |
| Apoptosis | Abbas et al., 2013 [45] | 21 rats divided into three equal groups | supplementation with 42 μg/kg of cholecalciferol | increased apoptosis of endometriosis cells | increased number of apoptotic cells |
| Miyashita et al., 2016 [48] | human endometriotic stromal cells (hESCs) isolated from 7 patients with endometriosis | incubation with 109 or 107 M 1,25(OH)2D3 | no observed changes | - | |
| Delbandi et al., 2016 [50] | human endometriotic stromal cells (hESCs) isolated from 25 patients with endometriosis | 107 M 1,25(OH)2 vitamin D3 | no observed changes | - | |
| Rashidi et al., 2023 [52] | human endometrial stromal cells (hESCs) isolated from 10 women with endometriosis | incubation with 10 nmol/L 1,25(OH)2D3 | increased apoptosis of endometriosis cells | arresting of endometriosis cells into phase G0/G1 of the cell cycle |
| Authors and Year of the Study | Type of the Study | Applied Intervention | Main Results |
|---|---|---|---|
| Akyol et al., 2016 [47] | preclinical animal | supplementation with vitamin D and omega-3-PUFAs in rats |
|
| Tomio et al., 2013 [141] | preclinical animal | use of transgenic mice able to convert omega-6-PUFAs to omega-3-PUFAs and mice without such properties |
|
| Attaman et al., 2014 [142] | preclinical animal | use of transgenic mice able to convert omega-6-PUFAs to omega-3-PUFAs and mice without such properties |
|
| Herington et al., 2013 [143] | preclinical animal | supplementation with fish oil |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abramiuk, M.; Mertowska, P.; Frankowska, K.; Świechowska-Starek, P.; Satora, M.; Polak, G.; Dymanowska-Dyjak, I.; Grywalska, E. How Can Selected Dietary Ingredients Influence the Development and Progression of Endometriosis? Nutrients 2024, 16, 154. https://doi.org/10.3390/nu16010154
Abramiuk M, Mertowska P, Frankowska K, Świechowska-Starek P, Satora M, Polak G, Dymanowska-Dyjak I, Grywalska E. How Can Selected Dietary Ingredients Influence the Development and Progression of Endometriosis? Nutrients. 2024; 16(1):154. https://doi.org/10.3390/nu16010154
Chicago/Turabian StyleAbramiuk, Monika, Paulina Mertowska, Karolina Frankowska, Paulina Świechowska-Starek, Małgorzata Satora, Grzegorz Polak, Izabela Dymanowska-Dyjak, and Ewelina Grywalska. 2024. "How Can Selected Dietary Ingredients Influence the Development and Progression of Endometriosis?" Nutrients 16, no. 1: 154. https://doi.org/10.3390/nu16010154
APA StyleAbramiuk, M., Mertowska, P., Frankowska, K., Świechowska-Starek, P., Satora, M., Polak, G., Dymanowska-Dyjak, I., & Grywalska, E. (2024). How Can Selected Dietary Ingredients Influence the Development and Progression of Endometriosis? Nutrients, 16(1), 154. https://doi.org/10.3390/nu16010154