
The Effect of Vitamin D Supplementation in Pregnant Women with Overweight and Obesity: A Randomised Controlled Trial

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.4. Interventions
2.5. Outcomes
2.6. Sample Size
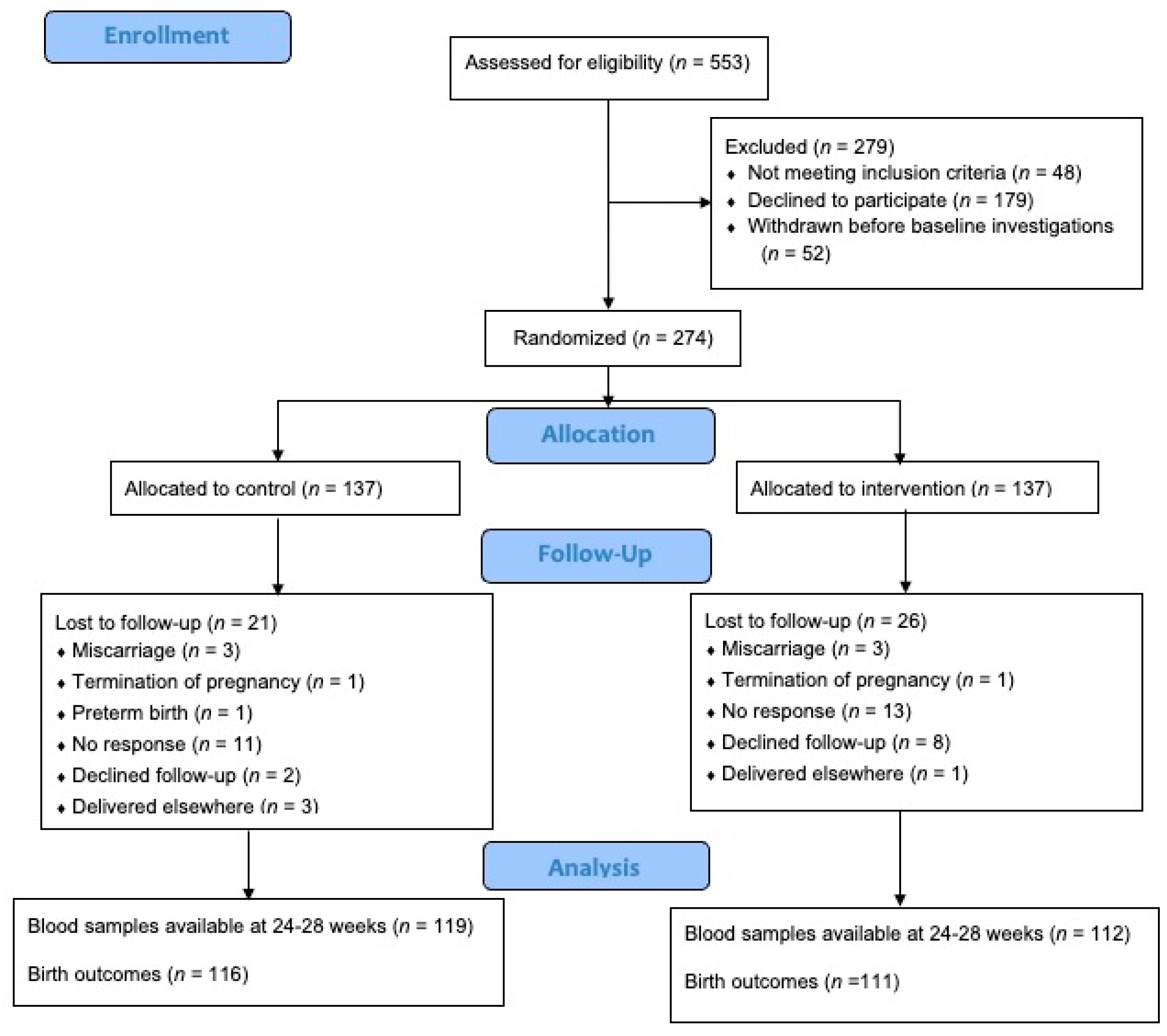
2.7. Randomisation
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vanchinathan, V.; Lim, H.W. A Dermatologist’s Perspective on Vitamin D. Mayo Clin. Proc. 2012, 87, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [PubMed]
- Haile, D.T.; Damote, T.T.; Sadamo, F.E.; Demissie, Z.G.; Dake, S.K. Vitamin D deficiency and associated factors among antenatal care attending pregnant women in Sodo town, South Ethiopia: A facility-based cross-sectional study. PLoS ONE 2022, 17, e0279975. [Google Scholar] [CrossRef] [PubMed]
- Loy, S.L.; Lek, N.; Yap, F.; Soh, S.E.; Padmapriya, N.; Tan, K.H.; Biswas, A.; Yeo, G.S.H.; Kwek, K.; Gluckman, P.D.; et al. Association of Maternal Vitamin D Status with Glucose Tolerance and Caesarean Section in a Multi-Ethnic Asian Cohort: The Growing Up in Singapore Towards Healthy Outcomes Study. PLoS ONE 2015, 10, e0142239. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Kovilam, O.; Agrawal, D.K. Vitamin D and its impact on maternal-fetal outcomes in pregnancy: A critical review. Crit. Rev. Food Sci. Nutr. 2017, 58, 755–769. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.R.; Braga, A.; Braga, J.; Marinho, A. Recurrent pregnancy loss and vitamin D: A review of the literature. Am. J. Reprod. Immunol. 2018, 80, e13022. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Zittermann, A.; Obeid, R.; Hahn, A.; Pludowski, P.; Trummer, C.; Lerchbaum, E.; Pérez-López, F.R.; Karras, S.N.; März, W. The Role of Vitamin D in Fertility and during Pregnancy and Lactation: A Review of Clinical Data. Int. J. Environ. Res. Public Health 2018, 15, 2241. [Google Scholar] [CrossRef]
- Gilani, S.; Janssen, P. Maternal Vitamin D Levels During Pregnancy and Their Effects on Maternal–Fetal Outcomes: A Systematic Review. J. Obstet. Gynaecol. Can. 2019, 42, 1129–1137. [Google Scholar] [CrossRef]
- Al-Ajlan, A.; Krishnaswamy, S.; Alokail, M.S.; Aljohani, N.J.; Al-Serehi, A.; Sheshah, E.; Alshingetti, N.M.; Fouda, M.; Turkistani, I.Z.; Al-Daghri, N.M. Vitamin D deficiency and dyslipidemia in early pregnancy. BMC Pregnancy Childbirth 2015, 15, 314. [Google Scholar] [CrossRef][Green Version]
- Mulligan, M.L.; Felton, S.K.; Riek, A.E.; Bernal-Mizrachi, C. Implications of vitamin D deficiency in pregnancy and lactation. Am. J. Obstet. Gynecol. 2010, 202, 429.e1–429.e9. [Google Scholar] [CrossRef]
- Camargo, C.A., Jr.; Ingham, T.; Wickens, K.; Thadhani, R.; Silvers, K.M.; Epton, M.J.; Town, G.I.; Pattemore, P.K.; Espinola, J.A.; Crane, J.; et al. Cord-Blood 25-Hydroxyvitamin D Levels and Risk of Respiratory Infection, Wheezing, and Asthma. Pediatrics 2011, 127, e180–e187. [Google Scholar] [CrossRef] [PubMed]
- Devereux, G.; A Litonjua, A.; Turner, S.W.; Craig, L.C.; McNeill, G.; Martindale, S.; Helms, P.J.; Seaton, A.; Weiss, S.T. Maternal vitamin D intake during pregnancy and early childhood wheezing. Am. J. Clin. Nutr. 2007, 85, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Curtis, E.M.; Moon, R.J.; Harvey, N.C.; Cooper, C. Maternal vitamin D supplementation during pregnancy. Br. Med. Bull. 2018, 126, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Pérez-López, F.R.; Pilz, S.; Chedraui, P. Vitamin D supplementation during pregnancy: An overview. Curr. Opin. Obstet. Gynecol. 2020, 32, 316–321. [Google Scholar] [CrossRef]
- Motamed, S.; Nikooyeh, B.; Kashanian, M.; Chamani, M.; Hollis, B.W.; Neyestani, T.R. Evaluation of the efficacy of two doses of vitamin D supplementation on glycemic, lipidemic and oxidative stress biomarkers during pregnancy: A randomized clinical trial. BMC Pregnancy Childbirth 2020, 20, 619. [Google Scholar] [CrossRef] [PubMed]
- Rostami, M.; Tehrani, F.R.; Simbar, M.; Bidhendi Yarandi, R.; Minooee, S.; Hollis, B.W.; Hosseinpanah, F. Effectiveness of Prenatal Vitamin D Deficiency Screening and Treatment Program: A Stratified Randomized Field Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2936–2948. [Google Scholar] [CrossRef]
- Mozaffari-Khosravi, H.; Hosseinzadeh-Shamsi-Anar, M.; Salami, M.-A.; Hadinedoushan, H.; Mozayan, M. Effects of a single post-partum injection of a high dose of vitamin D on glucose tolerance and insulin resistance in mothers with first-time gestational diabetes mellitus. Diabet. Med. 2011, 29, 36–42. [Google Scholar] [CrossRef]
- Yazdchi, R.; Gargari, B.P.; Asghari-Jafarabadi, M.; Sahhaf, F. Effects of vitamin D supplementation on metabolic indices and hs-CRP levels in gestational diabetes mellitus patients: A randomized, double-blinded, placebo-controlled clinical trial. Nutr. Res. Pract. 2016, 10, 328–335. [Google Scholar] [CrossRef][Green Version]
- Alhomaid, R.M.; Mulhern, M.S.; Strain, J.; Laird, E.; Healy, M.; Parker, M.J.; McCann, M.T. Maternal obesity and baseline vitamin D insufficiency alter the response to vitamin D supplementation: A double-blind, randomized trial in pregnant women. Am. J. Clin. Nutr. 2021, 114, 1208–1218. [Google Scholar] [CrossRef]
- Hengist, A.; Perkin, O.; Gonzalez, J.T.; Betts, J.A.; Hewison, M.; Manolopoulos, K.N.; Jones, K.S.; Koulman, A.; Thompson, D. Mobilising vitamin D from adipose tissue: The potential impact of exercise. Nutr. Bull. 2019, 44, 25–35. [Google Scholar] [CrossRef]
- Fernández-Arroyo, S.; Hernández-Aguilera, A.; de Vries, M.A.; Burggraaf, B.; van der Zwan, E.; Pouw, N.; Joven, J.; Cabezas, M.C. Effect of Vitamin D3 on the Postprandial Lipid Profile in Obese Patients: A Non-Targeted Lipidomics Study. Nutrients 2019, 11, 1194. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Retracted: Vitamin D Supplementation Affects Serum High-Sensitivity C-Reactive Protein, Insulin Resistance, and Biomarkers of Oxidative Stress in Pregnant Women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Lepsch, J.; Eshriqui, I.; Farias, D.R.; Vaz, J.S.; Figueiredo, A.C.C.; Adegboye, A.R.A.; Brito, A.; Mokhtar, R.; Allen, L.H.; Holick, M.F.; et al. Association between early pregnancy vitamin D status and changes in serum lipid profiles throughout pregnancy. Metabolism 2017, 70, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Jin, D.; Yao, M.N.; Yin, W.J.; Zhu, P. The association of Vitamin D levels with lipid metabolism during pregnancy. Chin. J. Prev. Med. 2019, 53, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Harreiter, J.; Mendoza, L.C.; Simmons, D.; Desoye, G.; Devlieger, R.; Galjaard, S.; Damm, P.; Mathiesen, E.R.; Jensen, D.M.; Andersen, L.L.T.; et al. Vitamin D3 Supplementation in Overweight/Obese Pregnant Women: No Effects on the Maternal or Fetal Lipid Profile and Body Fat Distribution-A Secondary Analysis of the Multicentric, Randomized, Controlled Vitamin D and Lifestyle for Gestational Diabetes Prevention Trial (DALI). Nutrients 2022, 14, 3781. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Fu, J.; Zhao, R.; Wang, B.; Zhang, M.; Li, L.; Shi, C. The effect of combined supplementation with vitamin D and omega-3 fatty acids on blood glucose and blood lipid levels in patients with gestational diabetes. Ann. Palliat. Med. 2021, 10, 5652–5658. [Google Scholar] [CrossRef]
- Bi, W.G.; Nuyt, A.M.; Weiler, H.; LeDuc, L.; Santamaria, C.; Wei, S.Q. Association between Vitamin D Supplementation During Pregnancy and Offspring Growth, Morbidity, and Mortality: A Systematic Review and Meta-analysis. JAMA Pediatr. 2018, 172, 635–645. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- SACN U. Vitamin D and Health. 2016. Available online: https://www.gov.uk/government/groups/scientific-advisory-committee-on-nutrition (accessed on 3 September 2020).
- Bouillon, R.; Carmeliet, G. Vitamin D insufficiency: Definition, diagnosis and management. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 669–684. [Google Scholar] [CrossRef]
- Corcoy, R.; Mendoza, L.C.; Simmons, D.; Desoye, G.; Adelantado, J.; Chico, A.; Devlieger, R.; van Assche, A.; Galjaard, S.; Timmerman, D.; et al. The DALI vitamin D randomized controlled trial for gestational diabetes mellitus prevention: No major benefit shown besides vitamin D sufficiency. Clin. Nutr. 2019, 39, 976–984. [Google Scholar] [CrossRef]
- Martins, J.; Steyn, N.; Rossouw, H.M.; Pillay, T.S. Best practice for LDL-cholesterol: When and how to calculate. J. Clin. Pathol. 2023, 76, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.J.; Ghosh, M.; Churchill, D.; Viswanath, A. An assessment of the international association of diabetes in pregnancy study group (IADPSG) criteria for diagnosing gestational diabetes mellitus. Arch. Dis. Child. Fetal Neonatal Ed. 2011, 96, Fa110. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Preeclampsia and High Blood Pressure during Pregnancy. Available online: https://www.acog.org/womens-health/faqs/preeclampsia-and-high-blood-pressure-during-pregnancy (accessed on 12 August 2023).
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; National Academies Press: Washington, DC, USA, 2009; ISBN 978-0-309-13113-1. [Google Scholar]
- Enkhmaa, D.; Tanz, L.; Ganmaa, D.; Enkhtur, S.; Oyun-Erdene, B.; Stuart, J.; Chen, G.; Carr, A.; Seely, E.; Fitzmaurice, G.; et al. Randomized trial of three doses of vitamin D to reduce deficiency in pregnant Mongolian women. EBioMedicine 2018, 39, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Kanani, F.H.; Ramzan, S.; Kausar, R.; Ayaz, S.; Khanani, R.; Pal, L. Obstetric and Neonatal Outcomes of Maternal Vitamin D Supplementation: Results of an Open-Label, Randomized Controlled Trial of Antenatal Vitamin D Supplementation in Pakistani Women. J. Clin. Endocrinol. Metab. 2014, 99, 2448–2455. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.C.; Stewart, A.W.; Scragg, R.; Milne, T.; Rowden, J.; Ekeroma, A.; Wall, C.; Mitchell, E.A.; Crengle, S.; Trenholme, A.; et al. Vitamin D During Pregnancy and Infancy and Infant Serum 25-Hydroxyvitamin D Concentration. Pediatrics 2014, 133, e143–e153. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Functional indices of vitamin D status and ramifications of vitamin D deficiency. Am. J. Clin. Nutr. 2004, 80, 1706S–1709S. [Google Scholar] [CrossRef]
- Mazahery, H.; Von Hurst, P.R. Factors Affecting 25-Hydroxyvitamin D Concentration in Response to Vitamin D Supplementation. Nutrients 2015, 7, 5111–5142. [Google Scholar] [CrossRef]
- Wang, Y.; Si, S.; Liu, J.; Wang, Z.; Jia, H.; Feng, K.; Sun, L.; Song, S.J. The Associations of Serum Lipids with Vitamin D Status. PLoS ONE 2016, 11, e0165157. [Google Scholar] [CrossRef]
- Huang, X.; Yang, Y.; Jiang, Y.; Zhou, Z.; Zhang, J. Association between vitamin D deficiency and lipid profiles in overweight and obese adults: A systematic review and meta-analysis. BMC Public Health 2023, 23, 1653. [Google Scholar] [CrossRef]
- Wu, D.; Shen, M.; Chu, N. Relationship between plasma leptin levels and lipid profiles among school children in Taiwan—The Taipei Children Heart Study. Eur. J. Epidemiol. 2001, 17, 911–916. [Google Scholar] [CrossRef]
- Wild, R.; Feingold, K.R. Effect of Pregnancy on Lipid Metabolism and Lipoprotein Levels. Available online: https://www.ncbi.nlm.nih.gov/books/NBK498654/ (accessed on 20 August 2023).
- Jorde, R.; Grimnes, G. Vitamin D and metabolic health with special reference to the effect of vitamin D on serum lipids. Prog. Lipid Res. 2011, 50, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Kong, L.; Yang, Y.; Wei, Y.; Zhu, W.; Su, R.; Lin, L.; Yang, H. Recommended reference values for serum lipids during early and middle pregnancy: A retrospective study from China. Lipids Health Dis. 2018, 17, 246. [Google Scholar] [CrossRef] [PubMed]
- Arshad, R.; Sameen, A.; Murtaza, M.A.; Sharif, H.R.; Haq, I.U.; Dawood, S.; Ahmed, Z.; Nemat, A.; Manzoor, M.F. Impact of vitamin D on maternal and fetal health: A review. Food Sci. Nutr. 2022, 10, 3230–3240. [Google Scholar] [CrossRef] [PubMed]
- Miliku, K.; Vinkhuyzen, A.; Blanken, L.M.; McGrath, J.J.; Eyles, D.W.; Burne, T.H.; Hofman, A.; Tiemeier, H.; AP Steegers, E.; Gaillard, R.; et al. Maternal vitamin D concentrations during pregnancy, fetal growth patterns, and risks of adverse birth outcomes. Am. J. Clin. Nutr. 2016, 103, 1514–1522. [Google Scholar] [CrossRef]
- Kaushal, M.; Magon, N. Vitamin D in pregnancy: A metabolic outlook. Indian J. Endocrinol. Metab. 2013, 17, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Rastegar, M.; Fateh, M.; Rahnama, A.; Sheybani-Arani, M.; Asl, A.S.; Rajaei, S. Evaluation of the relationship between vitamin D level during pregnancy and the rate of fetal heart problems: A cross-sectional study. Clin. Nutr. ESPEN 2022, 51, 262–266. [Google Scholar] [CrossRef]
- Cannell, J.J. Vitamin D and autism, what’s new? Rev. Endocr. Metab. Disord. 2017, 18, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Nimitphong, H.; Holick, M.F. Vitamin D status and sun exposure in southeast Asia. Dermato-Endocrinology 2013, 5, 34–37. [Google Scholar] [CrossRef]
- Yeum, K.-J.; Song, B.C.; Joo, N.-S. Impact of Geographic Location on Vitamin D Status and Bone Mineral Density. Int. J. Environ. Res. Public Health 2016, 13, 184. [Google Scholar] [CrossRef]
- Darling, A.L. Vitamin D deficiency in western dwelling South Asian populations: An unrecognised epidemic. Proc. Nutr. Soc. 2020, 79, 259–271. [Google Scholar] [CrossRef]
- Sutherland, J.P.; Zhou, A.; Leach, M.J.; Hyppönen, E. Differences and determinants of vitamin D deficiency among UK biobank participants: A cross-ethnic and socioeconomic study. Clin. Nutr. 2020, 40, 3436–3447. [Google Scholar] [CrossRef] [PubMed]
- Lowe, N.M.; Bhojani, I. Special considerations for vitamin D in the south Asian population in the UK. Ther. Adv. Musculoskelet. Dis. 2017, 9, 137–144. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total (n = 274) | Control (n = 137) | Intervention (n = 137) | p |
|---|---|---|---|---|
| Age, mean (SD), years | 30.58 (4.46) | 30.67 (4.22) | 30.50 (4.69) | 0.746 |
| Gestation age at recruitment, mean (SD), weeks | 11.78 (2.11) | 11.89 (2.21) | 11.66 (2.01) | 0.367 |
| Body mass index at recruitment, mean (SD), kg/m2 | 30.00 (4.25) | 29.71 (4.14) | 30.3 (4.35) | 0.274 |
| Ethnicity, n (%) | 0.312 | |||
| Chinese | 72 (26.3) | 38 (27.7) | 34 (24.8) | |
| Malay | 157 (57.3) | 73 (53.3) | 84 (61.3) | |
| Indian | 26 (9.5) | 13 (9.5) | 13 (9.5) | |
| Others | 19 (6.9) | 13 (9.5) | 6 (4.4) | |
| Education, mean (SD), years | 14.0 (3.52) | 14.1 (3.64) | 13.9 (3.40) | 0.601 |
| Employment status, n (%) | 0.559 | |||
| Unemployed | 60 (21.9) | 32 (23.4) | 28 (20.4) | |
| Employed | 214 (78.1) | 105 (76.6) | 109 (79.6) | |
| Sun exposure 11 a.m.–3 p.m., n (%) | 0.460 | |||
| <20 min/ day | 164 (59.9) | 79 (57.7) | 85 (62.0) | |
| ≥20 min/ day | 110 (40.1) | 58 (42.3) | 52 (38.0) | |
| Sunscreen usage, n (%) | 0.390 | |||
| None | 151 (55.1) | 76 (55.5) | 75 (54.7) | |
| 1–5 times/week | 67 (24.5) | 37 (27.0) | 30 (21.9) | |
| 6–7 times/week | 56 (20.4) | 24 (17.5) | 32 (23.4) | |
| Consumption of supplements containing Vitamin D or calcium, n (%) | 0.889 | |||
| No | 205 (74.8) | 103 (75.2) | 102 (74.5) | |
| Yes | 69 (25.2) | 34 (24.8) | 35 (25.5) | |
| Consumption of cod liver oil or omega-3 fatty acids supplements, n (%) | 0.254 | |||
| No | 229 (83.6) | 111 (81.0) | 118 (86.1) | |
| Yes | 45 (16.4) | 26 (19.0) | 19 (13.9) | |
| Dietary Vitamin D intake, median (25th75th centiles), µg/ day | 5.31 (2.55–10.80) | 5.24 (2.65–10.74) | 5.64 (2.37–12.23) | 0.833 |
| Dietary Calcium intake, median (25th–75th centiles), mg/ day | 306.43 (128.63–551.72) | 271.01 (125.46–490.07) | 320.11 (136.38–605.66) | 0.247 |
| Active smoking, n (%) | 0.146 | |||
| Never | 229 (83.6) | 120 (87.6) | 109 (79.6) | |
| Stopped smoking | 37 (13.5) | 15 (10.9) | 22 (16.1) | |
| Current or in the past one month | 8 (2.9) | 2 (1.5) | 6 (4.4) | |
| Passive smoking, n (%) | 0.600 | |||
| No | 190 (69.3) | 93 (67.9) | 97 (70.8) | |
| Yes | 84 (30.7) | 44 (32.1) | 40 (29.2) | |
| Physical activity, n (%) | 0.822 | |||
| Inactive (<600 MET-min/week) | 29 (10.6) | 15 (10.9) | 14 (10.2) | |
| Minimally active (600 to <3000 MET-min/week | 101 (36.9) | 48 (35.0) | 53 (38.7) | |
| Highly active (≥3000 MET-min/week) | 144 (52.6) | 74 (54.0) | 70 (51.1) | |
| Sedentary activity, n (%) | 0.260 | |||
| ≤8 h | 101 (36.9) | 46 (33.6) | 55 (40.1) | |
| >8 h | 173 (63.1) | 91 (66.4) | 82 (59.9) | |
| Vitamin D, mean (SD), nmol/L | 39.44 (14.71) | 38.94 (11.97) | 39.94 (17.05) | 0.575 |
| Deficiency <25 nmol/L, n (%) | 41 (15.0) | 18 (13.1) | 23 (16.8) | 0.069 |
| Insufficiency 25 to <50 nmol/L, n (%) | 174 (63.5) | 96 (70.1) | 78 (56.9) | |
| Sufficiency ≥50 nmol/L, n (%) | 59 (21.5) | 23 (16.8) | 36 (26.3) | |
| Total cholesterol, mean (SD), mmol/L | 5.04 (0.82) | 4.98 (0.82) | 5.10 (0.81) | 0.223 |
| HDL-cholesterol, mean (SD), mmol/L | 1.60 (0.32) | 1.58 (0.33) | 1.63 (0.32) | 0.204 |
| LDL-cholesterol, mean (SD), mmol/L | 2.77 (0.71) | 2.76 (0.65) | 2.79 (0.77) | 0.786 |
| Triglyceride, mean (SD), mmol/L | 1.44 (0.60) | 1.40 (0.54) | 1.49 (0.65) | 0.203 |
| Variable | Control (n = 119) | Intervention (n = 112) | Mean Difference (95% CI) | p b | Adjusted Difference (95% CI) | p c |
|---|---|---|---|---|---|---|
| Vitamin D, mean (SD), nmol/L | 53.46 (16.20) | 61.45 (16.74) | 8.00 (3.72, 12.27) | <0.001 | 6.52 (2.74, 10.31) | 0.001 |
| Deficiency <25 nmol/L, n (%) | 3 (2.5) | 0 (0.0) | NA | <0.001 | NA | NA |
| Insufficiency 25 to <50 nmol/L, n (%) | 50 (42.0) | 25 (22.3) | NA | NA | NA | NA |
| Sufficiency ≥50 nmol/L, n (%) | 66 (55.5) | 87 (77.7) | NA | NA | NA | NA |
| Total cholesterol, mean (SD), mmol/L | 6.1 (1.02) | 6.13 (1.08) | 0.02 (0.25, 0.29) | 0.885 | 0.07 (0.11, 0.24) | 0.472 |
| HDL-cholesterol, mean (SD), mmol/L | 1.80 (0.36) | 1.81 (0.35) | 0.01 (0.09, 0.10) | 0.773 | 0.03 (0.03, 0.09) | 0.403 |
| LDL-cholesterol, mean (SD), mmol/L | 3.30 (0.87) | 3.30 (0.95) | 0.00 (0.24, 0.24) | >0.950 | 0.00 (0.19, 0.20) | >0.950 |
| Triglyceride, mean (SD), mmol/L | 2.23 (0.82) | 2.18 (0.80) | −0.05 (−0.26, −0.16) | 0.641 | −0.10 (−0.29, −0.08) | 0.263 |
| Fasting glucose, mean (SD), mmol/L | 4.49 (0.75) | 4.43 (0.47) | −0.06 (−0.23, −0.11) | 0.480 | −0.06 (−0.22, −0.11) | 0.517 |
| 1 h glucose, mean (SD), mmol/L | 8.15 (2.07) | 7.95 (1.75) | −0.20 (−0.71, −0.30) | 0.427 | −0.21 (−0.72, −0.30) | 0.422 |
| 2 h glucose, mean (SD), mmol/L | 6.56 (1.77) | 6.69 (1.40) | 0.13 (0.29, 0.55) | 0.554 | 0.14 (0.28, 0.56) | 0.517 |
| Gestational diabetes, n (%) a | 0.547 | |||||
| No | 94 (80.3) | 84 (77.1) | NA | NA | NA | NA |
| Yes | 23 (19.7) | 25 (22.9) | NA | NA | NA | NA |
| Variable | Total (n = 227) | Control (n = 116) | Intervention (n = 111) | p |
|---|---|---|---|---|
| Neonatal birth weight, mean (SD), g | 3145.81 (436.83) | 3122.63 (434.04) | 3170.03 (440.39) | 0.415 |
| Low birth weight, n (%) | 0.751 | |||
| Yes | 24 (10.6) | 13 (11.2) | 11 (9.9) | |
| No | 203 (89.4) | 103 (88.8) | 100 (90.1) | |
| Neonatal birth length, mean (SD), cm | 48.48 (2.05) | 48.26 (2.15) | 48.70 (1.92) | 0.103 |
| Neonatal head circumference, mean (SD), cm | 33.82 (1.38) | 33.71 (1.32) | 33.93 (1.43) | 0.237 |
| Neonatal status, n (%) | 0.927 | |||
| Healthy live birth | 211 (93.0) | 108 (93.1) | 103 (92.8) | |
| Special care unit admission | 16 (7.0) | 8 (6.9) | 8 (7.2) | |
| Preterm birth, n (%) | 0.348 | |||
| No | 214 (94.3) | 111 (95.7) | 103 (92.8) | |
| Yes | 13 (5.7) | 5 (4.3) | 8 (7.2) | |
| Gestational hypertension, n (%) a | 0.394 | |||
| No | 216 (95.2) | 109 (94.0) | 107 (96.4) | |
| Yes | 11 (4.8) | 7 (6.0) | 4 (3.6) | |
| Gestational weight gain, n (%) b | 0.307 | |||
| Adequacy | 87 (39.7) | 39 (34.8) | 48 (44.9) | |
| Insufficiency | 44 (20.1) | 25 (22.3) | 19 (17.8) | |
| Excessive | 88 (40.2) | 48 (42.9) | 40 (37.4) | |
| Mode of delivery, n (%) | 0.724 | |||
| Normal vaginal delivery | 137 (60.4) | 69 (59.5) | 68 (61.3) | |
| Instrumental (forceps/vacuum) vaginal delivery | 18 (7.9) | 11 (9.5) | 7 (6.3) | |
| Elective caesarean section delivery | 27 (11.9) | 12 (10.3) | 15 (13.5) | |
| Emergency caesarean section delivery | 45 (19.8) | 24 (20.7) | 21 (18.9) |
| Vitamin D (Plasma 25OHD) | |||
|---|---|---|---|
| Deficiency < 25 nmol/L | Insufficiency 25 to <50 nmol/L | Sufficiency ≥ 50 nmol/L | |
| Total cholesterol, mean (SD), mmol/L | 5.01 (0.87) | 5.04 (0.82) | 5.05 (0.78) |
| HDL-cholesterol, mean (SD), mmol/L | 1.50 (0.29) | 1.61 (0.33) | 1.65 (0.32) |
| LDL-cholesterol, mean (SD), mmol/L | 2.81 (0.81) | 2.80 (0.68) | 2.67 (0.74) |
| Triglyceride, mean (SD), mmol/L | 1.47 (0.60) | 1.39 (0.52) | 1.59 (0.78) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ku, C.W.; Lee, A.J.W.; Oh, B.; Lim, C.H.F.; Chang, T.Y.; Yap, F.; Chan, J.K.Y.; Loy, S.L. The Effect of Vitamin D Supplementation in Pregnant Women with Overweight and Obesity: A Randomised Controlled Trial. Nutrients 2024, 16, 146. https://doi.org/10.3390/nu16010146
Ku CW, Lee AJW, Oh B, Lim CHF, Chang TY, Yap F, Chan JKY, Loy SL. The Effect of Vitamin D Supplementation in Pregnant Women with Overweight and Obesity: A Randomised Controlled Trial. Nutrients. 2024; 16(1):146. https://doi.org/10.3390/nu16010146
Chicago/Turabian StyleKu, Chee Wai, Angeline Jia Wen Lee, Benjarat Oh, Celeste Hong Fei Lim, Ting Yu Chang, Fabian Yap, Jerry Kok Yen Chan, and See Ling Loy. 2024. "The Effect of Vitamin D Supplementation in Pregnant Women with Overweight and Obesity: A Randomised Controlled Trial" Nutrients 16, no. 1: 146. https://doi.org/10.3390/nu16010146
APA StyleKu, C. W., Lee, A. J. W., Oh, B., Lim, C. H. F., Chang, T. Y., Yap, F., Chan, J. K. Y., & Loy, S. L. (2024). The Effect of Vitamin D Supplementation in Pregnant Women with Overweight and Obesity: A Randomised Controlled Trial. Nutrients, 16(1), 146. https://doi.org/10.3390/nu16010146