
The Effects of Multiple Micronutrient Fortified Beverage and Responsive Caregiving Interventions on Early Childhood Development, Hemoglobin, and Ferritin among Infants in Rural Guatemala
 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
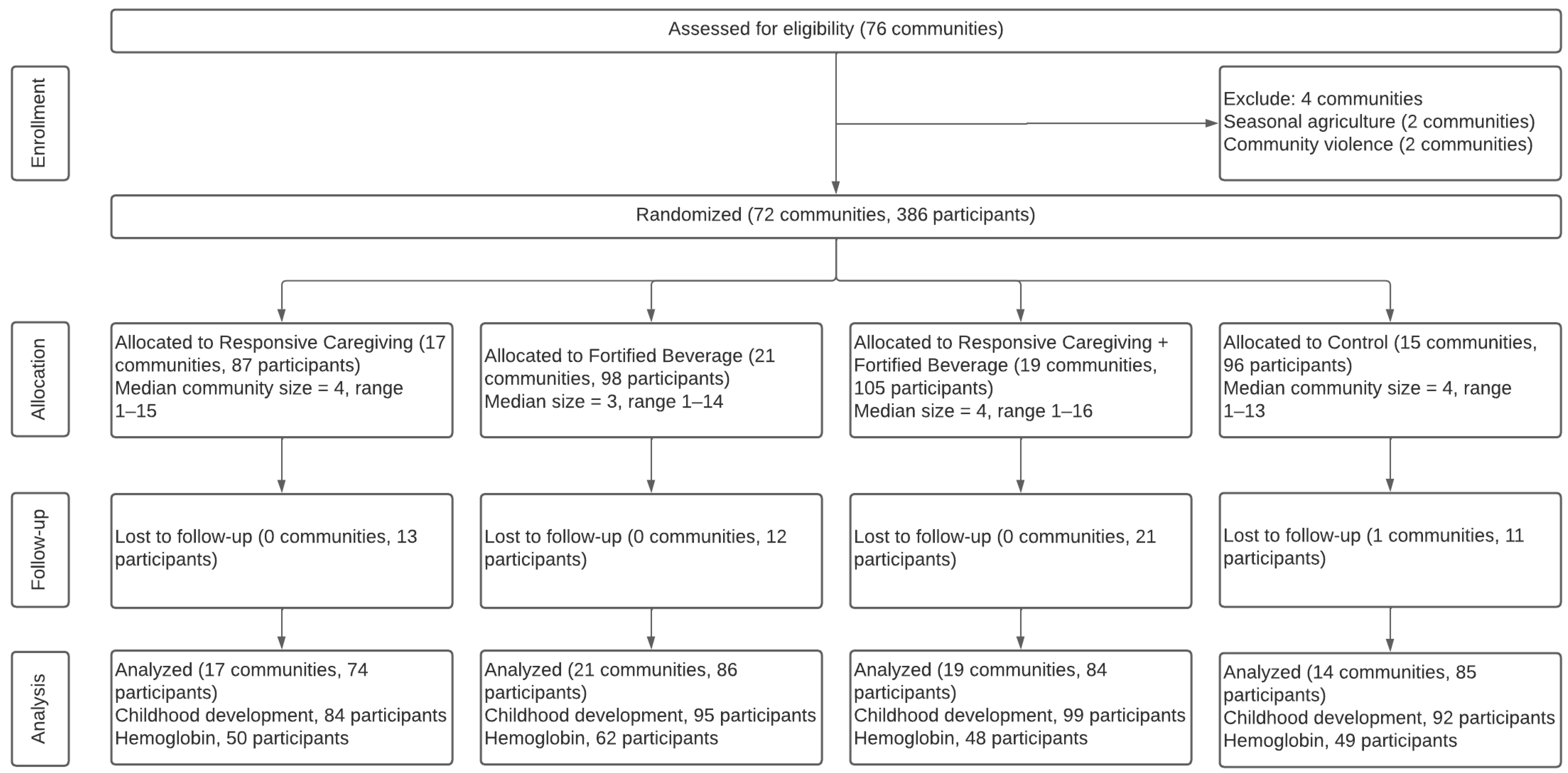
2.1. Site and Study Design
2.2. Sample Size
2.3. Ethical Approval
2.4. Recruitment
2.5. Multiple Micronutrient-Fortified Beverage/Placebo Interventions
2.6. Responsive Caregiving Intervention
2.7. Training and Intervention Delivery
2.8. Evaluation
2.9. Outcome Measures
2.9.1. Child Development
2.9.2. Nutrition Biomarkers
2.10. Control Measures
2.11. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Intervention Effects
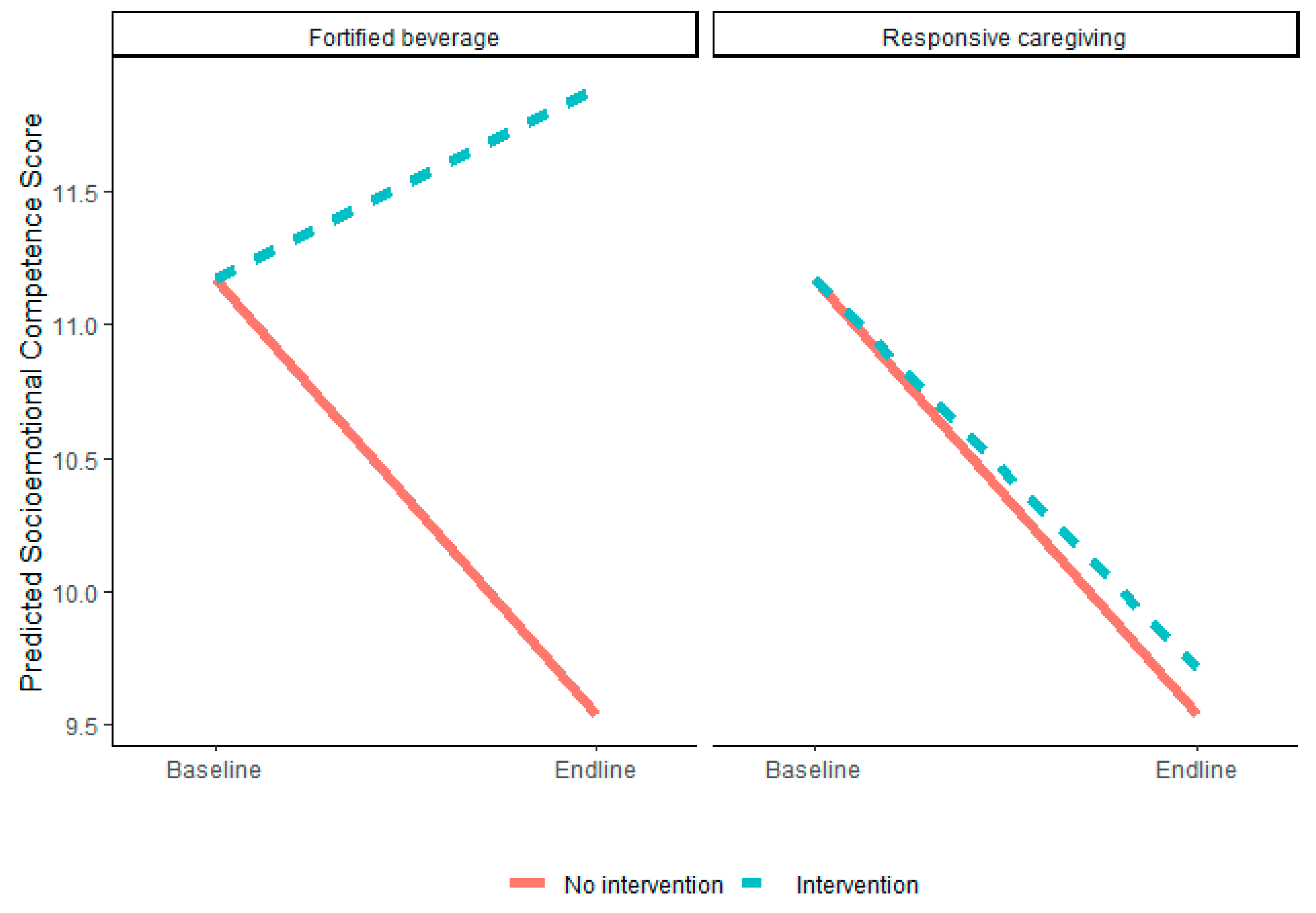
3.2.1. Fortified Beverage Intervention Effects
3.2.2. Responsive Caregiving Intervention Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Shonkoff, J.P.; Garner, A.S. The lifelong effects of early childhood adversity and toxic stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Black, M.M.; Richter, L.M. Risk of poor development in young children in low-income and middle-income countries: An estimation and analysis at the global, regional, and country level. Lancet Glob. Health 2016, 4, e916–e922. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.P.; Wachs, T.D.; Gardner, J.M.; Lozoff, B.; Wasserman, G.A.; Pollitt, E.; Carter, J.A. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007, 369, 145–157. [Google Scholar] [CrossRef]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C.H.; et al. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91–102. [Google Scholar] [CrossRef]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef]
- Stevens, G.A.; Beal, T.; Mbuya, M.N.N.; Luo, H.; Neufeld, L.M. Micronutrient deficiencies among preschool-aged children and women of reproductive age worldwide: A pooled analysis of individual-level data from population-representative surveys. Lancet Glob. Health 2022, 10, e1590–e1599. [Google Scholar] [CrossRef]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Keats, E.C.; Das, J.K.; Salam, R.A.; Lassi, Z.S.; Imdad, A.; Black, R.E.; Bhutta, Z.A. Effective interventions to address maternal and child malnutrition: An update of the evidence. Lancet Child Adolesc. Health 2021, 5, 367–384. [Google Scholar] [CrossRef]
- Tam, E.; Keats, E.C.; Rind, F.; Das, J.K.; Bhutta, A.Z.A. Micronutrient Supplementation and Fortification Interventions on Health and Development Outcomes among Children Under-Five in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 289. [Google Scholar] [CrossRef]
- Black, M.M.; Aboud, F.E. Responsive feeding is embedded in a theoretical framework of responsive parenting. J. Nutr. 2011, 141, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Landry, S.H.; Smith, K.E.; Swank, P.R.; Assel, M.A.; Vellet, S. Does early responsive parenting have a special importance for children’s development or is consistency across early childhood necessary? Dev. Psychol. 2001, 37, 387–403. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, M.H.; Tamis-LeMonda, C.S. Maternal responsiveness and cognitive development in children. New Dir. Child Adolesc. Dev. 1989, 43, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Jimenez, E.Y.; Dewey, K.G. Responsive Feeding Recommendations: Harmonizing Integration into Dietary Guidelines for Infants and Young Children. Curr. Dev. Nutr. 2021, 5, nzab076. [Google Scholar] [CrossRef]
- Jeong, J.; Franchett, E.E.; Ramos de Oliveira, C.V.; Rehmani, K.; Yousafzai, A.K. Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Med. 2021, 18, e1003602. [Google Scholar] [CrossRef]
- Zhang, L.; Ssewanyana, D.; Martin, M.C.; Lye, S.; Moran, G.; Abubakar, A.; Marfo, K.; Marangu, J.; Proulx, K.; Malti, T. Supporting Child Development Through Parenting Interventions in Low- to Middle-Income Countries: An Updated Systematic Review. Front. Public Health 2021, 9, 671988. [Google Scholar] [CrossRef]
- Dulal, S.; Prost, A.; Karki, S.; Saville, N.; Merom, D. Characteristics and effects of integrated nutrition and stimulation interventions to improve the nutritional status and development of children under 5 years of age: A systematic review and meta-analysis. BMJ Glob. Health 2021, 6, e003872. [Google Scholar] [CrossRef]
- Jeong, J.; Franchett, E.; Yousafzai, A.K. World Health Organization Recommendations on Caregiving Interventions to Support Early Child Development in the First Three Years of Life: Report of The Systematic Review Of Evidence; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Prado, E.L.; Larson, L.M.; Cox, K.; Bettencourt, K.; Kubes, J.N.; Shankar, A.H. Do effects of early life interventions on linear growth correspond to effects on neurobehavioural development? A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e1398–e1413. [Google Scholar] [CrossRef]
- Ministerio de Salud Pública y Asistencia Social (MSPAS); Instituto Nacional de Estadística (INE); ICF International. Encuesta Nacional de Salud Materno Infantil 2014–2015. Informe Final. Guatemala, MSPAS/INE/ICF. 2017. Available online: https://www.ine.gob.gt/images/2017/encuestas/ensmi2014_2015.pdf (accessed on 10 February 2023).
- Perumal, N.; Bassani, D.G.; Roth, D.E. Use and Misuse of Stunting as a Measure of Child Health. J. Nutr. 2018, 148, 311–315. [Google Scholar] [CrossRef]
- Alfonso, V.; de Ponce, S.; Barrantes, L.; Villanueva, L.; Casasola, D.; Reinhart, G.A. Anthropometric assessment of young children in Retalhuleu, Guatemala. FASEB J. 2013, 27, 618.13. [Google Scholar] [CrossRef]
- Retalhuleu Department in Guatemala. Available online: https://www.citypopulation.de/en/guatemala/admin/11__retalhuleu/ (accessed on 15 February 2023).
- Montgomery, A.A.; Peters, T.J.; Little, P. Design, analysis and presentation of factorial randomised controlled trials. BMC Med. Res. Methodol. 2003, 3, 26. [Google Scholar] [CrossRef] [PubMed]
- Palacios, A.M.; Villanueva, L.M.; Cuy Castellanos, D.; Reinhart, G.A. Aceptabilidad de un atole fortificado con 21 micronutrientes e impacto en la salud y nutrición de niños menores de 6 años de edad en la Ciudad de Guatemala. Arch. Latinoam. De Nutr. 2017, 67, 15–22. [Google Scholar]
- Reinhart, G.A.; Villanueva, L.M. A fortified corn/soy atole increases growth, decreases morbidity and improves nutritional status in urban Guatemalan toddlers and young children. FASEB J. 2012, 26, 1031.6. [Google Scholar] [CrossRef]
- Villanueva, L.; de Ponce, S.; Alfonso, V.; Reinhart, G. Effect of providing a micronutrient-fortified corn/soy atole or milk powder on linear growth in young Guatemalan children (828.6). FASEB J. 2014, 28, 828.6. [Google Scholar] [CrossRef]
- Lucas, J.E.; Richter, L.M.; Daelmans, B. Care for Child Development: An intervention in support of responsive caregiving and early child development. Child Care Health Dev. 2018, 44, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Rao, S.; Hurley, K.M.; Nair, K.M.; Balakrishna, N.; Radhakrishna, K.V.; Ravinder, P.; Tilton, N.; Harding, K.B.; Reinhart, G.A.; Black, M.M. Integrating nutrition and early child-development interventions among infants and preschoolers in rural India. Ann. N. Y. Acad. Sci. 2014, 1308, 218–231. [Google Scholar] [CrossRef]
- Bayley, N. Bayley Scales of Infant and Toddler Development, Version III; Psychological Corporation: San Antonio, TX, USA, 2006. [Google Scholar]
- Briggs-Gowan, M.J.; Carter, A.S.; Irwin, J.R.; Wachtel, K.; Cicchetti, D.V. The Brief Infant-Toddler Social and Emotional Assessment: Screening for social-emotional problems and delays in competence. J. Pediatr. Psychol. 2004, 29, 143–155. [Google Scholar] [CrossRef]
- Namaste, S.M.; Rohner, F.; Huang, J.; Bhushan, N.L.; Flores-Ayala, R.; Kupka, R.; Mei, Z.; Rawat, R.; Williams, A.M.; Raiten, D.J.; et al. Adjusting ferritin concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 359S–371S. [Google Scholar] [CrossRef]
- Coates, J.; Frongillo, E.A.; Rogers, B.L.; Webb, P.; Wilde, P.E.; Houser, R. Commonalities in the experience of household food insecurity across cultures: What are measures missing? J. Nutr. 2006, 136, 1438S–1448S. [Google Scholar] [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2006, 450, 76–85. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Lozoff, B.; Clark, K.M.; Jing, Y.; Armony-Sivan, R.; Angelilli, M.L.; Jacobson, S.W. Dose-response relationships between iron deficiency with or without anemia and infant social-emotional behavior. J. Pediatr. 2008, 152, 696–702. [Google Scholar] [CrossRef]
- Pasricha, S.R.; Hasan, M.I.; Braat, S.; Larson, L.M.; Tipu, S.M.M.; Hossain, S.J.; Shiraji, S.; Baldi, A.; Bhuiyan, M.S.A.; Tofail, F.; et al. Benefits and Risks of Iron Interventions in Infants in Rural Bangladesh. N. Engl. J. Med. 2021, 385, 982–995. [Google Scholar] [CrossRef] [PubMed]
- McCann, S.; Perapoch Amadó, M.; Moore, S.E. The Role of Iron in Brain Development: A Systematic Review. Nutrients 2020, 12, 2001. [Google Scholar] [CrossRef] [PubMed]
- Buril, F. Tackling Electoral Violence on Several Fronts in Guatemala. Available online: https://www.ifes.org/news/tackling-electoral-violence-several-fronts-guatemala (accessed on 15 February 2023).
- Martinez, B.; Webb, M.F.; Gonzalez, A.; Douglas, K.; Grazioso, M.D.P.; Rohloff, P. Complementary feeding intervention on stunted Guatemalan children: A randomised controlled trial. BMJ Paediatr. Open 2018, 2, e000213. [Google Scholar] [CrossRef] [PubMed]
- Vazir, S.; Engle, P.; Balakrishna, N.; Griffiths, P.L.; Johnson, S.L.; Creed-Kanashiro, H.; Fernandez Rao, S.; Shroff, M.R.; Bentley, M.E. Cluster-randomized trial on complementary and responsive feeding education to caregivers found improved dietary intake, growth and development among rural Indian toddlers. Matern. Child Nutr. 2013, 9, 99–117. [Google Scholar] [CrossRef]
- Torres, V.M.; Goicolea, I.; Edin, K.; Ohman, A. ’Expanding your mind’: The process of constructing gender-equitable masculinities in young Nicaraguan men participating in reproductive health or gender training programs. Glob. Health Action 2012, 5, 17262. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Quantity per Serving a | ||
|---|---|---|
| Chispuditos® | Placebo | |
| Calories (Energy) | 73 kcal | 73 kcal |
| Protein | 4 g | 4 g |
| Fat | 1 g | 1 g |
| Dietary Fiber | 2 g | 2 g |
| Carbohydrates | 12 g | 12 g |
| Sugars | 0 g | 0 g |
| Micronutrients | ||
| Iron | 12 mg | - |
| Folic Acid | 150 mcg | - |
| Zinc | 9 mg | |
| Iodine | 90 mcg | - |
| Vit A | 250 mcg | - |
| Vit C | 40 mg | - |
| Vit B12 | 0.9 mcg | - |
| Thiamine | 0.5 mg | - |
| Niacin | 6 mg | - |
| Riboflavin | 0.5 mg | 0.5 mg |
| Vit B6 | 0.5 mg | - |
| Copper | 300 mcg | - |
| Vitamin D3 | 5 mcg | - |
| Vitamin E | 5 mg | - |
| Calcium | 200 mg | - |
| Phosphorus | 150 mg | - |
| Magnesium | 40 mg | - |
| Selenium | 17 mcg | - |
| Manganese | 0.17 mg | - |
| Biotin | 8 mcg | - |
| Vitamin B5 | 1.8 mg | - |
| Age Group | Lesson Number | Message | Category a | Picture b |
|---|---|---|---|---|
| 6–12 months | 1 | Smile and look at the child during feeding. Sonría y mire a su hijo(a) mientras lo(a) alimenta. | RF, RC | Mother and child looking, smiling, feeding |
| 2 | Give your child opportunities to explore objects and people. Tummy time. Dele a su hijo(a) la oportunidad de explorar nuevos objetos, personas y alimentos. Es tiempo de estar boca abajo! | RC | Child on tummy playing | |
| Give your child family food of soft and thick consistency Alimente a su hijo(a)con comida de consistencia suave y espesa. | RF | Soft, thick food | ||
| 3 | Eat and play with your child. Coma y juegue con su hijo(a). | RF, RC | Mother and child facing playing peek-a-boo, playing with household items | |
| Respond to your child’s cues of hunger and satiety. Reconozca las señales de hambre y saciedad de su niño. | RF | Mother feeding eager child | ||
| 4 | Talk and sing to your child during daily activities. Háblele y cántele a su hijo(a) durante las actividades diarias. | RC | Mother singing and looking at child | |
| Have patience, love, and good humor when feeding your child. Cuando alimente a su niño tenga paciencia, amor y buen humor. | RF, RC | Mother feeding with a smile | ||
| 5 | Imitate your child’s actions and gestures. Imite las acciones y gestos de su hijo(a). | RC | Mother imitating child | |
| Offer finger foods. Ofrezca alimentos que se puedan comer con la mano. | RF | Child picking up food with fingers | ||
| 6 | Help your child learn signals, such as bye-bye. Ayude a su niño a reconocer señales, por ejemplo adiós. | RC | Child waving | |
| Feed your child an adequate amount and variety of food. Dele a su hijo(a) una alimentación apropiada, variada, especialmente de frutas y verduras. | RF | Mother feeding child; family meal | ||
| 12–18 months | 1 | Offer finger foods. Déle a su niño alimentos que se puedan comer con la mano. | RF | Child picking up food with fingers |
| Imitate your child’s actions. Imite las acciones de su hijo(a). | RC | Mother doing what child is doing | ||
| 2 | Play with your child. Juegue con su hijo. | RC | Mother and child facing playing peek-a-boo, with a ball | |
| Respond to your child’s cues of hunger and satiety. Responda las señales de hambre y saciedad de su hijo(a). | RF | Child turning away from food, mother not forcing | ||
| 3 | Establish a routine where you look at a book with your child. Establezca una rutina para observar un libro de cuentos con su hijo(a). | RC | Child in bed, mother with a book | |
| Eat in a calm, relaxed environment without distractions, such as TV or radio. Coma en un lugar tranquiloy sin distracciones. | RF | Family eating food together | ||
| 4 | Talk and sing to your child throughout the day. Háblele y cántele a su hijo(a) a lo largo del día. | RC | Mother talking to child | |
| Take away uneaten food without comments. Retire los alimentos que el niño(a) no se comió sin decir nada. | RF | Mother picking up plate from child with food on it | ||
| Talk to your child about daily household objects and activities. Hable con su hijo(a) acerca de objetos domésticos cotidianos y sobre actividades diarias. | RC | Child playing with household items | ||
| 5 | Play matching games with your child. Juegue con su hijo(a) a buscar parejas (juegos de asociación). | RP | Mother and child looking at pictures in a book | |
| Make positive comments about the food (yummy). Haga comentarios positivos acerca de la comida. | RF | Mother smiling and eating with child | ||
| 6 | Give adequate amounts of food at every meal. Dele a su hijo(a) cantidades adecuadas de alimentos en cada comida. | RF | Mother serving child | |
| Praise your child for good efforts even if he does not succeed. Felicite a su niño por los buenos esfuerzos a pesar de que no haya tenido éxito. | RC | Mother smiling at child | ||
| Be sure that your child is hungry at meals and has not filled up on sweetened drinks or snacks. Asegúrese de que su niño tiene hambre en las comidas, y que no se haya llenado de bebidas dulces o golosinas no nutritivas. | RF | Child looking ready to eat |
| Characteristic | Responsive Caregiving (n = 87) | Fortified Beverage (n = 98) | Responsive Caregiving + Fortified Beverage (n = 105) | Control (n = 96) | p b |
|---|---|---|---|---|---|
| Household | |||||
| Family ethnicity, n (%) indigenous | 14 (19%) | 14 (17%) | 10 (11%) | 12 (15%) | 0.59 |
| Food insecurity, n (%) | 52 (61%) | 55 (59%) | 55 (56%) | 55 (60%) | 0.90 |
| Household assets, n | 6.45 (2.66) | 6.9 (2.93) | 6.94 (3.14) | 7.06 (3.02) | 0.53 |
| Household CHAOS score | 14.12 (4.7) | 15.3 (5.79) | 13.49 (5.05) | 14.33 (5.41) | 0.12 |
| Mother | |||||
| Age, y | 27.62 (7.85) | 28.76 (8.87) | 26 (6.6) | 27.84 (8.75) | 0.10 |
| Married/in a relationship, n (%) | 75 (86%) | 82 (84%) | 93 (89%) | 80 (83%) | 0.69 |
| <Primary schooling | 17 (20%) | 16 (17%) | 20 (19%) | 20 (21%) | 1.0 |
| Completed primary schooling | 46 (53%) | 50 (53%) | 55 (52%) | 49 (51%) | |
| ≥Secondary schooling | 24 (28%) | 29 (31%) | 30 (29%) | 27 (28%) | |
| Child | |||||
| Age, months | 12.87 (4.37) | 12.78 (4.73) | 13.19 (4.81) | 13.02 (4.26) | 0.93 |
| Male sex, n (%) | 43 (49%) | 52 (53%) | 49 (47%) | 47 (49%) | 0.84 |
| LAZ | −1.6 (0.91) | −1.53 (1.05) | −1.37 (1.06) | −1.71 (1.01) | 0.14 |
| WAZ | −0.74 (0.93) | −0.79 (0.95) | −0.68 (0.92) | −0.96 (0.92) | 0.20 |
| WHZ | 0.02 (0.93) | −0.02 (1.1) | 0.01 (0.93) | −0.13 (0.95) | 0.73 |
| BMIZ | 0.23 (0.94) | 0.17 (1.15) | 0.2 (0.96) | 0.09 (0.94) | 0.82 |
| Child development | |||||
| Cognitive score | 91.73 (11.21) | 94.11 (11.55) | 93.18 (12.19) | 94.78 (12.22) | 0.35 |
| Language score | 84.04 (15.31) | 86.13 (14.73) | 84.07 (15.6) | 86.13 (14.21) | 0.62 |
| Motor score | 85.86 (10.78) | 87.46 (11.89) | 86.17 (12.33) | 88.34 (13.78) | 0.49 |
| Socioemotional competence | 10.4 (5.67) | 11.6 (5.64) | 11.15 (5.97) | 11.47 (6.05) | 0.62 |
| Socioemotional problems | 17.1 (9.34) | 19.7 (10.57) | 16.87 (8.58) | 17.86 (9.5) | 0.21 |
| Nutrition biomarkers | |||||
| Hemoglobin | 10.98 (1.32) | 10.86 (1.12) | 10.61 (1.49) | 10.76 (1.29) | 0.58 |
| Ferritin c | 10.4 (25.28) | 12.48 (18.99) | 8.05 (6.06) | 11.29 (15.10) | 0.05 * |
| Wave | Fortified Beverage (n = 203) | No Fortified Beverage (n = 183) | Responsive Caregiving (n = 192) | No Responsive Caregiving (n = 194) | Fortified Beverage vs. No Fortified Beverage (95% CI) c | Responsive Caregiving vs. No Responsive Caregiving (95% CI) c | |
|---|---|---|---|---|---|---|---|
| Child development | |||||||
| Cognitive score d | BL | 93.63 (11.86) | 93.32 (11.82) | 92.51 (11.74) | 94.44 (11.86) | −1.23 (−3.52, 1.06) | −0.59 (−2.88, 1.7) |
| EL | 88.76 (9.8) | 89.97 (9.32) | 88.79 (9.7) | 89.85 (9.46) | |||
| Language score d | BL | 85.08 (15.17) | 85.13 (14.74) | 84.05 (15.42) | 86.13 (14.43) | 0.13 (−2.71, 2.97) | 0.06 (−2.78, 2.91) |
| EL | 82.98 (11.35) | 82.78 (11.52) | 82.66 (11.7) | 83.09 (11.18) | |||
| Motor score d | BL | 86.8 (12.1) | 87.15 (12.47) | 86.03 (11.62) | 87.89 (12.82) | −0.14 (−2.65, 2.38) | −0.36 (−2.87, 2.16) |
| EL | 87.89 (11.3) | 88.27 (12.13) | 87.57 (11.59) | 88.55 (11.8) | |||
| Socioemotional competence e | BL | 11.35 (5.81) | 10.98 (5.88) | 10.83 (5.84) | 11.53 (5.84) | 2.34 (0.98, 3.7) ** | 0.17 (−1.19, 1.53) |
| EL | 11.97 (6.7) | 9.61 (6.44) | 10.96 (6.59) | 10.7 (6.76) | |||
| Socioemotional problems e | BL | 18.15 (9.61) | 17.49 (9.4) | 16.97 (8.91) | 18.75 (10.05) | 1.26 (−0.5, 3.02) | −0.83 (−2.59, 0.93) |
| EL | 11.05 (6.62) | 9.64 (5.83) | 9.86 (5.36) | 10.84 (7) | |||
| Nutrition biomarkers | |||||||
| Hemoglobin, g/dL | BL | 10.75 (1.3) | 10.87 (1.3) | 10.79 (1.42) | 10.82 (1.19) | 0.13 (−0.23, 0.49) | −0.15 (−0.51, 0.22) |
| EL | 11.07 (0.98) | 10.98 (0.99) | 10.95 (0.9) | 11.09 (1.04) | |||
| Ferritin, µg/L f | BL | 9.79 (14.85) | 10.82 (19.31) | 8.74 (12.65) | 11.75 (17.1) | 0.1 (−0.24, 0.45) | 0.14 (−0.21, 0.49) |
| EL | 35.72 (87.3) | 31.1 (76.73) | 34.2 (76.13) | 31.24 (90.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalski, A.J.; Mayen, V.A.; de Ponce, S.; Lambden, K.B.; Tilton, N.; Villanueva, L.M.; Palacios, A.M.; Reinhart, G.A.; Hurley, K.M.; Black, M.M. The Effects of Multiple Micronutrient Fortified Beverage and Responsive Caregiving Interventions on Early Childhood Development, Hemoglobin, and Ferritin among Infants in Rural Guatemala. Nutrients 2023, 15, 2062. https://doi.org/10.3390/nu15092062
Kowalski AJ, Mayen VA, de Ponce S, Lambden KB, Tilton N, Villanueva LM, Palacios AM, Reinhart GA, Hurley KM, Black MM. The Effects of Multiple Micronutrient Fortified Beverage and Responsive Caregiving Interventions on Early Childhood Development, Hemoglobin, and Ferritin among Infants in Rural Guatemala. Nutrients. 2023; 15(9):2062. https://doi.org/10.3390/nu15092062
Chicago/Turabian StyleKowalski, Alysse J., Victor Alfonso Mayen, Silvia de Ponce, Kaley B. Lambden, Nick Tilton, Lisa M. Villanueva, Ana M. Palacios, Gregory A. Reinhart, Kristen M. Hurley, and Maureen M. Black. 2023. "The Effects of Multiple Micronutrient Fortified Beverage and Responsive Caregiving Interventions on Early Childhood Development, Hemoglobin, and Ferritin among Infants in Rural Guatemala" Nutrients 15, no. 9: 2062. https://doi.org/10.3390/nu15092062
APA StyleKowalski, A. J., Mayen, V. A., de Ponce, S., Lambden, K. B., Tilton, N., Villanueva, L. M., Palacios, A. M., Reinhart, G. A., Hurley, K. M., & Black, M. M. (2023). The Effects of Multiple Micronutrient Fortified Beverage and Responsive Caregiving Interventions on Early Childhood Development, Hemoglobin, and Ferritin among Infants in Rural Guatemala. Nutrients, 15(9), 2062. https://doi.org/10.3390/nu15092062