
Physical Activity, but Not Glycaemic Load, Is Associated with Lower Real-Time Glycaemic Control in Free-Living Women with Gestational Diabetes Mellitus

 ,
,  and
and
Abstract
1. Introduction
2. Methods and Materials
2.1. Participants, Demographics and Ethics Approval
2.2. Dietary Education Session
2.3. Continuous Glucose Monitoring
2.4. Physical Activity and Sedentary Time
2.5. Dietary Intake—Nutrient, Food Groups and Carbohydrate Quality Analysis
2.6. GI and GL Calculations
2.7. Diet Quality
2.8. Statistical Analysis
3. Results
3.1. Participant Demographics
3.2. Glycaemic Load: Carbohydrate Quality and Quantity Assessment
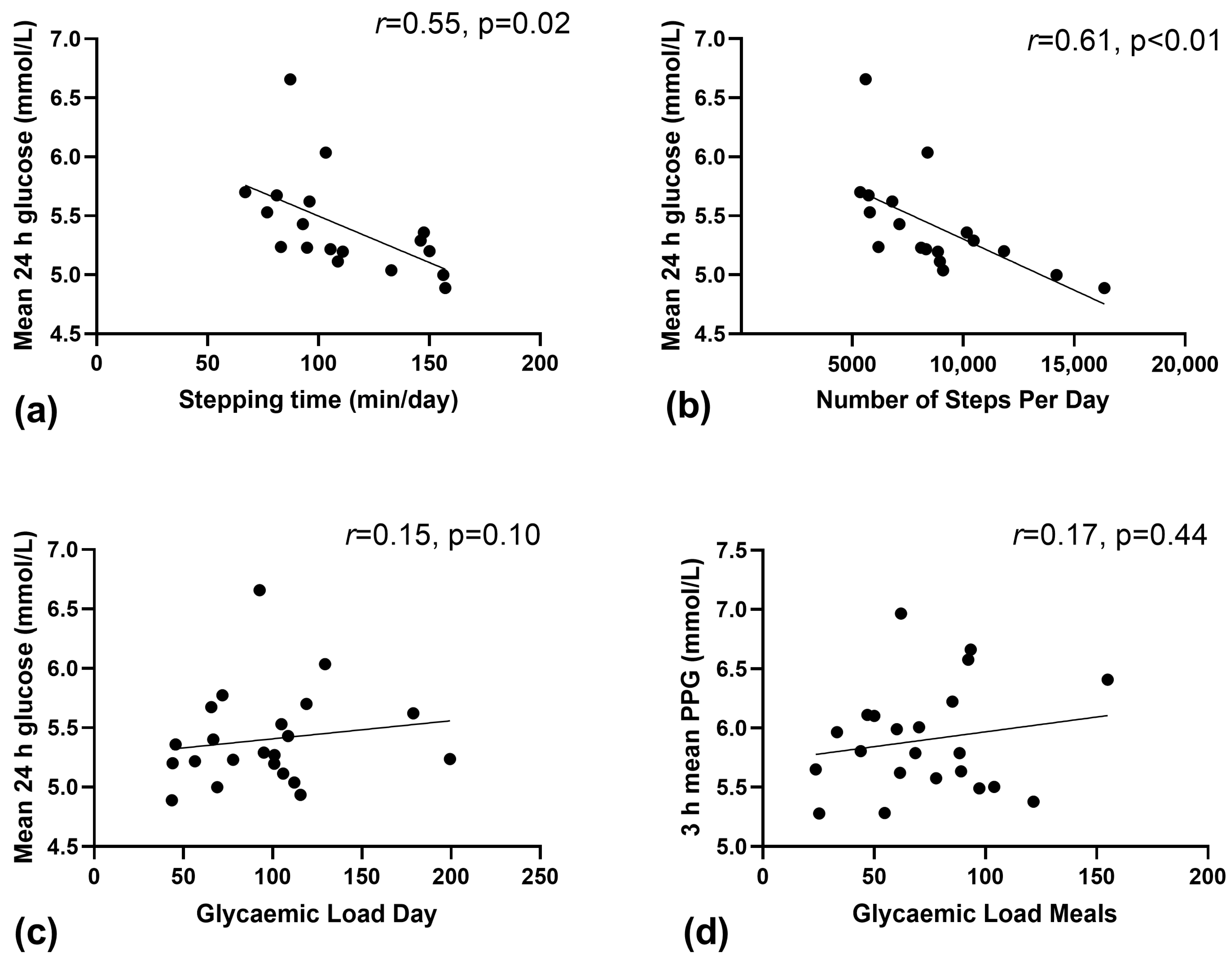
3.3. Relationship between Physical Activity, Sedentary Behaviour and CGM Data
3.4. Relationship between GL and Corresponding CGM Data
3.5. Hierarchical Linear Regression Analyses
3.6. Dietary Quality Assessment
Macro- and Micro-Nutrient Intake Assessment
3.7. Australian Guide to Healthy Eating (AGHE) Food Group Assessment
4. Discussion
4.1. Main Findings
4.2. Increasing the Number of Steps per Day; an Important Physical Activity Recommendation
4.3. Carbohydrate and Glycaemic Load
4.4. Achieving Nutrient Recommendations
4.5. Strengths and Limitations
4.6. Summary
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duarte-Gardea, M.O.; Gonzales-Pacheco, D.M.; Reader, D.M.; Thomas, A.M.; Wang, S.R.; Gregory, R.P.; Piemonte, T.A.; Thompson, K.L.; Moloney, L. Academy of Nutrition and dietetics gestational diabetes evidence-based nutrition practice guideline. J. Acad. Nutr. Diet. 2018, 118, 1719–1742. [Google Scholar] [CrossRef] [PubMed]
- Ovesen, P.G.; Fuglsang, J.; Andersen, M.B.; Wolff, C.; Petersen, O.B.; McIntyre, H.D. Temporal trends in gestational diabetes prevalence, treatment, and outcomes at Aarhus University Hospital, Skejby, between 2004 and 2016. J. Diabetes Res. 2018, 2018, 5937059. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Australia. Position Statement: Gestational Diabetes in Australia; Australian Diabetes Society: Canberra, ACT, Australia, August 2020. [Google Scholar]
- HAPO Study Cooperative Research Group. The hyperglycemia and adverse pregnancy outcome (HAPO) study. Int. J. Gynecol. Obstet. 2002, 78, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.M.; Wolever, T.M.; O’Connor, D.L.; Nisenbaum, R.; Josse, R.G. Effect of a low glycaemic index diet on blood glucose in women with gestational hyperglycaemia. Diabetes Res. Clin. Pract. 2011, 91, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.Y.; Markovic, T.P.; Perera, N.; Foote, D.; Petocz, P.; Ross, G.P.; Brand-Miller, J.C. A randomized controlled trial investigating the effects of a low-glycemic index diet on pregnancy outcomes in gestational diabetes mellitus. Diabetes Care 2011, 34, 2341–2346. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.-G.; Tan, R.-S.; Jin, D.; Li, W.; Zhou, X.-Y. A low glycemic index staple diet reduces postprandial glucose values in Asian women with gestational diabetes mellitus. J. Investig. Med. 2014, 62, 975–979. [Google Scholar] [CrossRef]
- Moses, R.G.; Barker, M.; Winter, M.; Petocz, P.; Brand-Miller, J.C. Can a low–glycemic index diet reduce the need for insulin in gestational diabetes mellitus? A randomized trial. Diabetes Care 2009, 32, 996–1000. [Google Scholar] [CrossRef]
- Kizirian, N.V.; Goletzke, J.; Brodie, S.; Atkinson, F.S.; Markovic, T.P.; Ross, G.P.; Buyken, A.; Brand-Miller, J.P. Lower glycemic load meals reduce diurnal glycemic oscillations in women with risk factors for gestational diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000351. [Google Scholar] [CrossRef]
- Louie, J.C.Y.; Markovic, T.P.; Ross, G.P.; Foote, D.; Brand-Miller, J.C. Higher glycemic load diet is associated with poorer nutrient intake in women with gestational diabetes mellitus. Nutr. Res. 2013, 33, 259–265. [Google Scholar] [CrossRef]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary behavior, exercise, and cardiovascular health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C.; et al. Associations of diet and physical activity with risk for gestational diabetes mellitus: A systematic review and meta-analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef]
- Tobias, D.K.; Zhang, C.; van Dam, R.M.; Bowers, K.; Hu, F.B. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: A meta-analysis. Diabetes Care 2011, 34, 223–229. [Google Scholar] [CrossRef]
- Hayashi, A.; Oguchi, H.; Kozawa, Y.; Ban, Y.; Shinoda, J.; Suganuma, N. Daily walking is effective for the management of pregnant women with gestational diabetes mellitus. J. Obstet. Gynaecol. Res. 2018, 44, 1731–1738. [Google Scholar] [CrossRef]
- Wagnild, J.M.; Hinshaw, K.; Pollard, T.M. Associations of sedentary time and self-reported television time during pregnancy with incident gestational diabetes and plasma glucose levels in women at risk of gestational diabetes in the UK. BMC Public Health 2019, 19, 575. [Google Scholar] [CrossRef]
- Nankervis, A.; McIntyre, H.D.; Moses, R.; Ross, G.P.; Callaway, L.; Porter, C.; Jeffries, W.; Boorman, C.; De Vries, B.; McElduff, A. ADIPS Consensus Guidelines for the Testing and Diagnosis of Gestational Diabetes Mellitus in Australia; Australasian Diabetes in Pregnancy Society: Sydney, NSW, Australia, 2014; pp. 1–8. [Google Scholar]
- NHMRC. Eat for Health. Healthy Eating during Your Pregnancy; Department of Health and Ageing, Australian Government ACT: Canberra, ACT, Australia, 2015.
- Hernandez, T.L.; Barbour, L.A. A standard approach to continuous glucose monitor data in pregnancy for the study of fetal growth and infant outcomes. Diabetes Technol. Ther. 2013, 15, 172–179. [Google Scholar] [CrossRef]
- Grant, P.M.; Ryan, C.G.; Tigbe, W.; Granat, M.H. The validation of a novel activity monitor in the measurement of posture and motion during everyday activities. Br. J. Sport. Med. 2006, 40, 992–997. [Google Scholar] [CrossRef]
- Louie, J.; Barclay, A.; Brand-Miller, J. Assigning glycemic index to foods in a recent Australian food composition database. Eur. J. Clin. Nutr. 2016, 70, 280–281. [Google Scholar] [CrossRef]
- Brand-Miller, J.C.; Holt, S.H.; Petocz, P. Reply to R Mendosa. Am. J. Clin. Nutr. 2003, 77, 994–995. [Google Scholar] [CrossRef]
- NHMRC. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; Commonwealth of Australia: Canberra, ACT, Australia, 2006. [Google Scholar]
- Combs, C.A.; Gunderson, E.; Kitzmiller, J.L.; Gavin, L.A.; Main, E.K. Relationship of fetal macrosomia to maternal postprandial glucose control during pregnancy. Diabetes Care 1992, 15, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Radulian, G.; Rusu, E.; Dragomir, A.; Posea, M. Metabolic effects of low glycaemic index diets. Nutr. J. 2009, 8, 5. [Google Scholar] [CrossRef]
- Ruchat, S.M.; Mottola, M.F. The important role of physical activity in the prevention and management of gestational diabetes mellitus. Diabetes/Metab. Res. Rev. 2013, 29, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Sabag, A.; Houston, L.; Neale, E.P.; Christie, H.E.; Roach, L.A.; Russell, J.; Cortie, C.H.; Batterham, M.; Meyer, B.J.; Francois, M.E. Supports and Barriers to Lifestyle Interventions in Women with Gestational Diabetes Mellitus in Australia: A National Online Survey. Nutrients 2023, 15, 487. [Google Scholar] [CrossRef] [PubMed]
- Hayman, M.; Reaburn, P.; Alley, S.; Cannon, S.; Short, C. What exercise advice are women receiving from their healthcare practitioners during pregnancy? Women Birth 2020, 33, e357–e362. [Google Scholar] [CrossRef]
- Mørkrid, K.; Jenum, A.K.; Berntsen, S.; Sletner, L.; Richardsen, K.R.; Vangen, S.; Holme, I.; Birkeland, K.I. Objectively recorded physical activity and the association with gestational diabetes. Scand. J. Med. Sci. Sport. 2014, 24, e389–e397. [Google Scholar] [CrossRef]
- Zhou, S.J.; Flynn, A.C.; Malek, L.; Greco, R.; Moran, L.; Martin, J.C. The assessment of diet quality and its effects on health outcomes pre-pregnancy and during pregnancy. In Seminars in Reproductive Medicine; Thieme Medical Publishers: New York, NY, USA, 2016. [Google Scholar]
- Chen, H.; Qin, L.; Gao, R.; Jin, X.; Cheng, K.; Zhang, S.; Hu, X.; Xu, W.; Wang, H. Neurodevelopmental effects of maternal folic acid supplementation: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2021, 1–17. [Google Scholar] [CrossRef]


{kind=link}
| Nutrient | Unit/Day | Mean (±SD) | Range: Min–Max | % Meeting NRVs: Diet Only | % Meeting NRVs through Supplements |
|---|---|---|---|---|---|
| EAR | |||||
| Macronutrients | |||||
| Protein | g | 92.5 (17.3) | 48.9–116.7 | 94 | 94 |
| Carbohydrate ¶ | g | 176.3 (47.3) | 96.9–266.9 | 56 ¶ | 56 |
| Dietary Fibre | g | 26.8 (6.5) | 16.7–40.4 | 33 | 33 |
| Vitamins | |||||
| Thiamin | mg | 1.9 (1.2) | 0.7–5.5 | 67 | 94 |
| Riboflavin | mg | 2.0 (0.50) | 0.9–2.9 | 94 | 100 |
| Niacin Eq. | mg | 21.2 (5.0) | 12.6–29.3 | 89 | 100 |
| Vit B6 | mg | 1.5 (0.3) | 1.1–2.0 | 39 | 83 |
| Vit B12 | µg | 4.2 (1.2) | 2.1–6.4 | 94 | 94 |
| Folate | µg | 494.5 (134.7) | 293.9–723.3 | 56 | 89 |
| Vit A | µg | 1154.2 (734.8) | 299.8–2898.1 | 83 | 94 |
| Vit C | mg | 94.8 (48.2) | 36.5–222.3 | 94 | 100 |
| Minerals/Trace Elements | |||||
| Calcium | mg | 1014.5 (304.6) | 419.2–1436.9 | 83 | 83 |
| Phosphorus | mg | 1576.6 (347.8) | 1092.9–2483.5 | 100 | 100 |
| Zinc | mg | 11.9 (2.8) | 8.2–17.2 | 89 | 100 |
| Iron | mg | 11.0 (2.9) | 7.1–17.2 | 0 | 39 |
| Iodine | µg | 160.1 (38.2) | 90.4–219.3 | 50 | 78 |
| Selenium | µg | 80.4 (31.4) | 29.4–172.1 | 83 | 100 |
| AI | |||||
| Macronutrients | |||||
| Polyunsaturated Fatty Acids | |||||
| Linoleic Acid (N-6) | g | 12.3 (5.1) | 5.3–26.4 | 61 | 61 |
| A-Linolenic Acid | g | 2.0 (0.9) | 0.8–3.6 | 94 | 94 |
| Omega-3 Long Chain PUFA DHA/EPA/DPA | g | 0.2 (0.3) | 0.0–1.1 | 56 | 72 |
| Vitamins | |||||
| Vit E | mg | 14.3 (5.7) | 5.3–27.3 | 94 | 100 |
| Minerals/Trace Elements | |||||
| Magnesium | mg | 340.6 (90.4) | 237.8–588.3 | 61 Ɨ | 83 |
| Potassium | mg | 2879.9 (503.3) | 2148.2–3726.8 | 44 | 44 |
| Sodium | mg | 2696.7 (757.2) | 1571.1–4314.2 | 100 | 100 |
| Food Group | No. Serves Mean ± SD | Range: Min–Max | % within ± 1 Serve of AGHE Recommendations | % Exceeding AGHE Recommendations | % below AGHE Recommendations |
|---|---|---|---|---|---|
| Grain (Cereal) | 9.1 ± 4.6 | 1.2–17.4 | 28% | 50% | 22% |
| Vegetables and Legumes/Beans | 5.5 ± 2.4 | 1.0–11.1 | 56% | 28% | 17% |
| Fruit | 2.1 ± 1.4 | 0.0–5.1 | 67% | 22% | 11% |
| Milk, Yoghurt, Cheese and/or Alternatives | 4.5 ± 3.6 | 1.3–14.1 | 28% | 61% | 11% |
| Meats and/or Alternatives § | 5.8 ± 2.9 | 1.7–13.5 | 22% | 67% | 11% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jardine, I.R.; Christie, H.E.; Oetsch, K.; Sabag, A.; Kennedy, M.; Meyer, B.J.; Francois, M.E. Physical Activity, but Not Glycaemic Load, Is Associated with Lower Real-Time Glycaemic Control in Free-Living Women with Gestational Diabetes Mellitus. Nutrients 2023, 15, 1974. https://doi.org/10.3390/nu15081974
Jardine IR, Christie HE, Oetsch K, Sabag A, Kennedy M, Meyer BJ, Francois ME. Physical Activity, but Not Glycaemic Load, Is Associated with Lower Real-Time Glycaemic Control in Free-Living Women with Gestational Diabetes Mellitus. Nutrients. 2023; 15(8):1974. https://doi.org/10.3390/nu15081974
Chicago/Turabian StyleJardine, Isabelle R., Hannah E. Christie, Kate Oetsch, Angelo Sabag, Meredith Kennedy, Barbara J. Meyer, and Monique E. Francois. 2023. "Physical Activity, but Not Glycaemic Load, Is Associated with Lower Real-Time Glycaemic Control in Free-Living Women with Gestational Diabetes Mellitus" Nutrients 15, no. 8: 1974. https://doi.org/10.3390/nu15081974
APA StyleJardine, I. R., Christie, H. E., Oetsch, K., Sabag, A., Kennedy, M., Meyer, B. J., & Francois, M. E. (2023). Physical Activity, but Not Glycaemic Load, Is Associated with Lower Real-Time Glycaemic Control in Free-Living Women with Gestational Diabetes Mellitus. Nutrients, 15(8), 1974. https://doi.org/10.3390/nu15081974