
Damage from Carbonated Soft Drinks on Enamel: A Systematic Review

 ,
,  ,
,  ,
,  ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Processing
2.3. Eligibility Criteria
- Participants: Teeth of both children and adults were included, in vivo and in vitro.
- Interventions: Considerable consumption of any carbonated soft drink.
- Comparisons: No considerable consumption of any carbonated soft drink.
- Outcomes: Damage to dental enamel.
- Study: Clinical trials on human teeth, both in vivo and in vitro.
2.4. Data Processing
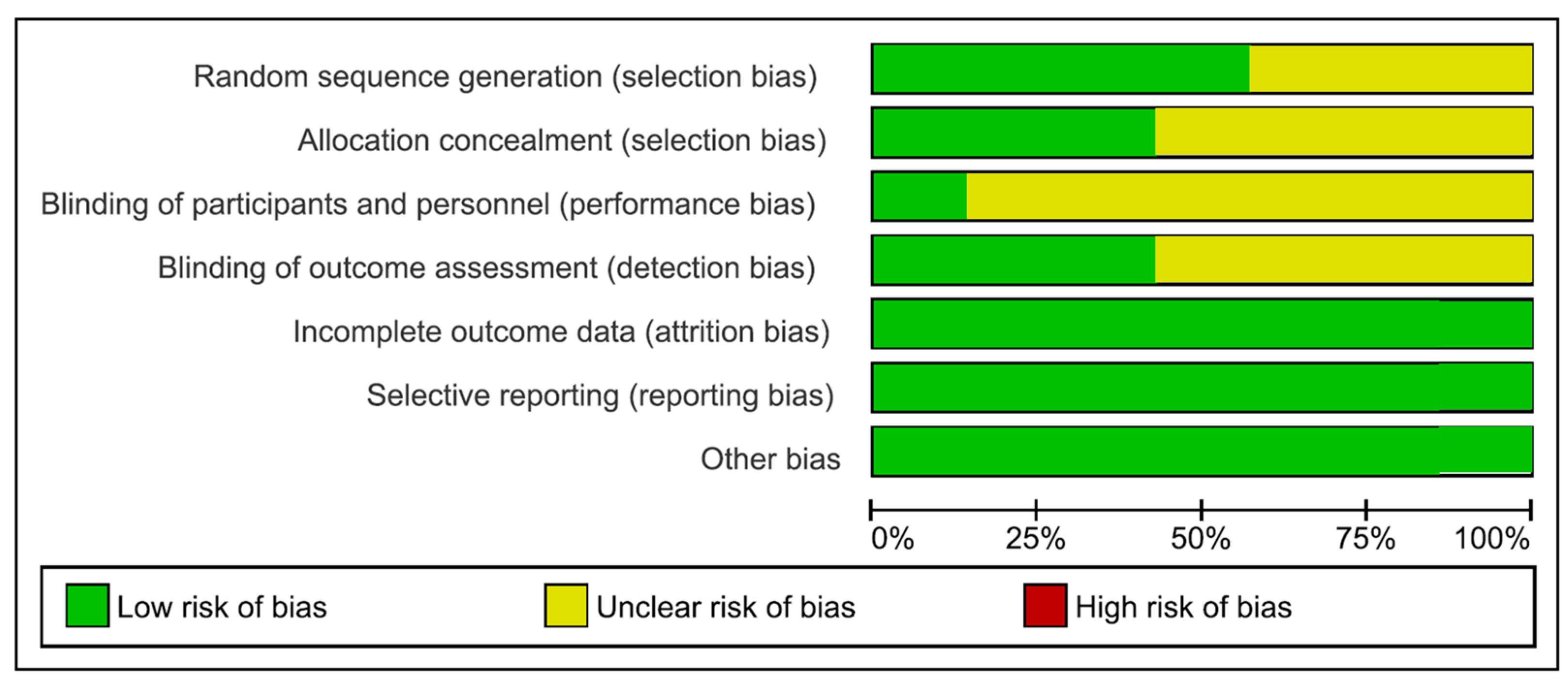
2.5. Risk of Bias Measurement
3. Results
Risk of Bias Measurement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DMFT | Decay, Missed and Filled Teeth (index) |
| ETW | Erosive Teeth Wear |
References
- Scardina, G.A.; Messina, P. Good Oral Health and Diet. J. Biomed. Biotechnol. 2012, 2012, 720692. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Mirowski, G.W. Nutrition and Oral Mucosal Diseases. Clin. Dermatol. 2010, 28, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Hemati, G.; Imani, M.M.; Choubsaz, P.; Inchingolo, F.; Sharifi, R.; Sadeghi, M.; Tadakamadla, S.K. Evaluation of Beta-Defensin 1 and Mannose-Binding Lectin 2 Polymorphisms in Children with Dental Caries Compared to Caries-Free Controls: A Systematic Review and Meta-Analysis. Children 2023, 10, 232. [Google Scholar] [CrossRef]
- Meurman, J.H.; Gate, J.M. Pathogenesis and Modifying Factors of Dental Erosion. Eur. J. Oral Sci. 1996, 104, 199–206. [Google Scholar] [CrossRef]
- Moynihan, P.; Petersen, P.E. Diet, Nutrition and the Prevention of Dental Diseases. Public Health Nutr. 2004, 7, 201–226. [Google Scholar] [CrossRef] [PubMed]
- Teshome, A.; Muche, A.; Girma, B. Prevalence of Dental Caries and Associated Factors in East Africa, 2000–2020: Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 645091. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Gentile, M.; Inchingolo, A.M.; Dipalma, G. Non-Syndromic Multiple Supernumerary Teeth in a Family Unit with a Normal Karyotype: Case Report. Int. J. Med. Sci. 2010, 7, 378–384. [Google Scholar] [CrossRef]
- Touger-Decker, R.; van Loveren, C. Sugars and Dental Caries. Am. J. Clin. Nutr. 2003, 78, 881S–892S. [Google Scholar] [CrossRef]
- Lussi, A.; Jaeggi, T.; Zero, D. The Role of Diet in the Aetiology of Dental Erosion. Caries Res 2004, 38 (Suppl. S1), 34–44. [Google Scholar] [CrossRef]
- Scheutzel, P. Etiology of Dental Erosion ? Intrinsic Factors. Eur. J. Oral Sci. 1996, 104, 178–190. [Google Scholar] [CrossRef]
- Pachori, A.; Kambalimath, H.; Maran, S.; Niranjan, B.; Bhambhani, G.; Malhotra, G. Evaluation of Changes in Salivary PH after Intake of Different Eatables and Beverages in Children at Different Time Intervals. Int. J. Clin. Pediatr. Dent. 2018, 11, 177–182. [Google Scholar] [CrossRef]
- von Wirén, N.; Khodr, H.; Hider, R.C. Hydroxylated Phytosiderophore Species Possess an Enhanced Chelate Stability and Affinity for Iron(III). Plant Physiol. 2000, 124, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Mapping the Human Genetic Architecture of COVID-19. Nature 2021, 600, 472–477. [CrossRef] [PubMed]
- Ojetti, V.; Saviano, A.; Covino, M.; Acampora, N.; Troiani, E.; Franceschi, F.; Abbate, V.; Acampora, N.; Addolorato, G.; Agostini, F.; et al. COVID-19 and Intestinal Inflammation: Role of Fecal Calprotectin. Dig. Liver Dis. 2020, 52, 1231–1233. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Dipalma, G.; Inchingolo, A.M.; Malcangi, G.; Santacroce, L.; D’Oria, M.T.; Isacco, C.G.; Bordea, I.R.; Candrea, S.; Scarano, A.; et al. The 15-Months Clinical Experience of SARS-CoV-2: A Literature Review of Therapies and Adjuvants. Antioxidants 2021, 10, 881. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Gargiulo, C.I.; Malcangi, G.; Ciocia, A.M.; Patano, A.; Azzollini, D.; Piras, F.; Barile, G.; Settanni, V.; Mancini, A.; et al. Diagnosis of SARS-CoV-2 during the Pandemic by Multiplex RT-RPCR HCoV Test: Future Perspectives. Pathogens 2022, 11, 1378. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease through Viral Genomic and Receptor Implications: An Overview of Diagnostic and Immunology Breakthroughs. Microorganisms 2021, 9, 793. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Xhajanka, E.; Scarano, A.; Lorusso, F.; Farronato, M.; Tartaglia, G.M.; Isacco, C.G.; et al. SARS-CoV-2 Disease Adjuvant Therapies and Supplements Breakthrough for the Infection Prevention. Microorganisms 2021, 9, 525. [Google Scholar] [CrossRef] [PubMed]
- De Maria, L.; Sponselli, S.; Caputi, A.; Stefanizzi, P.; Pipoli, A.; Giannelli, G.; Delvecchio, G.; Tafuri, S.; Inchingolo, F.; Migliore, G.; et al. SARS-CoV-2 Breakthrough Infections in Health Care Workers: An Italian Retrospective Cohort Study on Characteristics, Clinical Course and Outcomes. J. Clin. Med. 2023, 12, 628. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Nutritional Recommendations for CoVID-19 Quarantine. Eur. J. Clin. Nutr. 2020, 74, 850–851. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhu, J.; Zhao, J.; Sun, Z.; Zhu, B.; Lu, H.; Zheng, Y. Dental Caries Status and Its Associated Factors among Schoolchildren Aged 6–8 Years in Hangzhou, China: A Cross-Sectional Study. BMC Oral Health 2023, 23, 94. [Google Scholar] [CrossRef] [PubMed]
- Hadilou, M.; Somi, M.H.; Faramarzi, E.; Nikniaz, L. Effect of Beverage Consumption Frequency on DMFT Index among Iranian Adult Population: An AZAR Cohort Study. Int. J. Dent. 2022, 2022, 9142651. [Google Scholar] [CrossRef]
- Shenkin, J.D.; Heller, K.E.; Warren, J.J.; Marshall, T.A. Soft Drink Consumption and Caries Risk in Children and Adolescents. Gen. Dent. 2003, 51, 30–36. [Google Scholar]
- Tahmassebi, J.; Duggal, M.; Malik, G.; Curzon, M.E.J. Soft Drinks and Dental Health: A Review of the Current Literature. J. Dent. 2006, 34, 2–11. [Google Scholar] [CrossRef]
- Harnack, L.; Stang, J.; Story, M. Soft Drink Consumption Among US Children and Adolescents: Nutritional Consequences. J. Am. Diet. Assoc. 1999, 99, 436–441. [Google Scholar] [CrossRef]
- Zisowsky, J.; Krause, A.; Dingemanse, J. Drug Development for Pediatric Populations: Regulatory Aspects. Pharmaceutics 2010, 2, 364. [Google Scholar] [CrossRef]
- Matar, M.; Darwish, S.; Salma, R. Erosive Potential of Some Beverages on the Enamel Surface of Primary Molars. J. Dent. Med. Sci. 2021, 20, 43–46. [Google Scholar] [CrossRef]
- Olas, B. New Perspectives on the Effect of Dandelion, Its Food Products and Other Preparations on the Cardiovascular System and Its Diseases. Nutrients 2022, 14, 1350. [Google Scholar] [CrossRef]
- Cheng, R.; Yang, H.; Shao, M.; Hu, T.; Zhou, X. Dental Erosion and Severe Tooth Decay Related to Soft Drinks: A Case Report and Literature Review. J. Zhejiang Univ. Sci. B 2009, 10, 395. [Google Scholar] [CrossRef]
- Elmore, B.J. The American Beverage Industry and the Development of Curbside Recycling Programs, 1950–2000. Bus. Hist. Rev. 2012, 86, 477–501. [Google Scholar] [CrossRef]
- Guthrie, J.F.; Morton, J.F. Food Sources of Added Sweeteners in the Diets of Americans. J. Am. Diet. Assoc. 2000, 100, 43–51. [Google Scholar] [CrossRef]
- Johnson, R.K.; Frary, C. Choose Beverages and Foods to Moderate Your Intake of Sugars: The 2000 Dietary Guidelines for Americans—What’s All the Fuss About? J. Nutr. 2001, 131, 2766S–2771S. [Google Scholar] [CrossRef] [PubMed]
- Vågstrand, K.; Linné, Y.; Karlsson, J.; Elfhag, K.; Lindroos, A.K. Correlates of Soft Drink and Fruit Juice Consumption among Swedish Adolescents. Br. J. Nutr. 2009, 101, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Huse, O.; Reeve, E.; Bell, C.; Sacks, G.; Baker, P.; Wood, B.; Backholer, K. Strategies Used by the Soft Drink Industry to Grow and Sustain Sales: A Case-Study of The Coca-Cola Company in East Asia. BMJ Glob. Health 2022, 7, e010386. [Google Scholar] [CrossRef]
- Kearney, J. Food Consumption Trends and Drivers. Philos. Trans. R. Soc. Lond B Biol. Sci. 2010, 365, 2793–2807. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C. Uneven Dietary Development: Linking the Policies and Processes of Globalization with the Nutrition Transition, Obesity and Diet-Related Chronic Diseases. Glob. Health 2006, 2, 4. [Google Scholar] [CrossRef]
- Gondivkar, S.M.; Gadbail, A.R.; Shroff, P.; Kumbhare, S.P. Analyses of the Erosive Potential of Various Soft Drinks and Packaged Fruit Juices on Teeth. J. Contemp. Dent. Pract. 2018, 19, 1547–1552. [Google Scholar] [CrossRef]
- Al-Zwaylif, L.H.; O’Toole, S.; Bernabé, E. Type and Timing of Dietary Acid Intake and Tooth Wear among American Adults. J. Public Health Dent. 2018, 78, 214–220. [Google Scholar] [CrossRef]
- Davari, A.; Ataei, E.; Assarzadeh, H. Dentin Hypersensitivity: Etiology, Diagnosis and Treatment; A Literature Review. J. Dent. 2013, 14, 136–145. [Google Scholar]
- Alcântara, P.M.; Barroso, N.F.F.; Botelho, A.M.; Douglas-de-Oliveira, D.W.; Gonçalves, P.F.; Flecha, O.D. Associated Factors to Cervical Dentin Hypersensitivity in Adults: A Transversal Study. BMC Oral Health 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Santacroce, L.; Marinelli, G.; Mancini, A.; Vimercati, L.; Maggiore, M.E.; D’Oria, M.T.; Hazballa, D.; et al. COVID-19 Infection in Children, Infants and Pregnant Subjects: An Overview of Recent Insights and Therapies. Microorganisms 2021, 9, 1964. [Google Scholar] [CrossRef]
- Imfeld, T. Dental Erosion. Definition, Classification and Links. Eur. J. Oral Sci. 1996, 104, 151–155. [Google Scholar] [CrossRef]
- Lussi, A.; Schlueter, N.; Rakhmatullina, E.; Ganss, C. Dental Erosion—An Overview with Emphasis on Chemical and Histopathological Aspects. CRE 2011, 45, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.-K.; Omar, R.; Carlsson, G.E.; Johansson, A. Dental Erosion and Its Growing Importance in Clinical Practice: From Past to Present. Int. J. Dent. 2012, 2012, 632907. [Google Scholar] [CrossRef] [PubMed]
- Linnett, V.; Seow, W.K. Dental Erosion in Children: A Literature Review. Pediatr. Dent. 2001, 23, 37–43. [Google Scholar] [PubMed]
- Hans, R.; Thomas, S.; Garla, B.; Dagli, R.J.; Hans, M.K. Effect of Various Sugary Beverages on Salivary PH, Flow Rate, and Oral Clearance Rate amongst Adults. Scientifica 2016, 2016, 5027283. [Google Scholar] [CrossRef]
- Morgado, M.; Ascenso, C.; Carmo, J.; Mendes, J.J.; Manso, A.C. PH Analysis of Still and Carbonated Bottled Water: Potential Influence on Dental Erosion. Clin. Exp. Dent. Res. 2022, 8, 552–560. [Google Scholar] [CrossRef]
- Jensdottir, T.; Bardow, A.; Holbrook, P. Properties and Modification of Soft Drinks in Relation to Their Erosive Potential in Vitro. J. Dent. 2005, 33, 569–575. [Google Scholar] [CrossRef]
- Kregiel, D. Health Safety of Soft Drinks: Contents, Containers, and Microorganisms. Biomed. Res. Int. 2015, 2015, 128697. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.; Norris, D.F.; Momeni, S.S.; Waldo, B.; Ruby, J.D. The PH of Beverages Available to the American Consumer. J. Am. Dent. Assoc. 2016, 147, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Balzanelli, M.G.; Distratis, P.; Dipalma, G.; Vimercati, L.; Inchingolo, A.D.; Lazzaro, R.; Aityan, S.K.; Maggiore, M.E.; Mancini, A.; Laforgia, R.; et al. SARS-CoV-2 Virus Infection May Interfere CD34+ Hematopoietic Stem Cells and Megakaryocyte-Erythroid Progenitors Differentiation Contributing to Platelet Defection towards Insurgence of Thrombocytopenia and Thrombophilia. J. Conserv. Dent. 2021, 9, 1632. [Google Scholar] [CrossRef]
- Singh, S.; Jindal, R. Evaluating the Buffering Capacity of Various Soft Drinks, Fruit Juices and Tea. J. Conserv. Dent. 2010, 13, 129–131. [Google Scholar] [CrossRef]
- Barbour, M.E.; Lussi, A. Erosion in Relation to Nutrition and the Environment. Erosive. Tooth Wear 2014, 25, 143–154. [Google Scholar] [CrossRef]
- Buzalaf, M.A.R.; Hannas, A.R.; Kato, M.T. Saliva and Dental Erosion. J. Appl. Oral Sci. 2012, 20, 493–502. [Google Scholar] [CrossRef]
- Alessio, D.; Inchingolo; Rapone, B.; Patano, A.; Cardarelli, F.; Montenegro, V.; Ceci, S.; Inchingolo, A.; Semjonova, A.; Palmieri, G.; et al. Early Functional Orthodontic Treatment of Bad Oral Habits with AMCOP ® Bio-Activators. J. Biol. Regul. Homeost. Agents 2022, 36, 91–110. [Google Scholar]
- Pessoa-Lima, C.; Tostes-Figueiredo, J.; Macedo-Ribeiro, N.; Hsiou, A.S.; Muniz, F.P.; Maulin, J.A.; Franceschini-Santos, V.H.; de Sousa, F.B.; Barbosa, F.; Line, S.R.P.; et al. Structure and Chemical Composition of ca. 10-Million-Year-Old (Late Miocene of Western Amazon) and Present-Day Teeth of Related Species. Biology 2022, 11, 1636. [Google Scholar] [CrossRef]
- MP, C.; Motwani, M. Evaluation of Enamel Solubility on Exposure to Hard Drinks: An In-Vitro Study. Int. J. Dent. Oral Sci. 2019, 6, 697–702. [Google Scholar] [CrossRef]
- Seredin, P.; Goloshchapov, D.; Kashkarov, V.; Emelyanova, A.; Buylov, N.; Barkov, K.; Ippolitov, Y.; Khmelevskaia, T.; Mahdy, I.A.; Mahdy, M.A.; et al. Biomimetic Mineralization of Tooth Enamel Using Nanocrystalline Hydroxyapatite under Various Dental Surface Pretreatment Conditions. Biomimetics 2022, 7, 111. [Google Scholar] [CrossRef]
- Gotouda, H.; Nasu, I.; Kono, T.; Ootani, Y.; Kanno, T.; Tamamura, R.; Kuwada, T.; Suzuki, K.; Hirayama, T.; Hirayama, T.; et al. Erosion by an Acidic Soft Drink of Human Molar Teeth Assessed by X-Ray Diffraction Analysis. J. Hard Tissue Biol. 2017, 26, 81–86. [Google Scholar] [CrossRef]
- Panic, Z.; Stojsin, I.; Jankovic, O.; Vukoje, K.; Brkanić, T.; Tadic-Latinovic, L. In Vitro Investigation of Erosive Effect of Carbonated Beverages on Enamel and Dentin. Vojnosanit. Pregl. Mil.-Med. Pharm. Rev. 2019, 76, 422–431. [Google Scholar] [CrossRef]
- Tanykova, N.; Petrova, Y.; Kostina, J.; Kozlova, E.; Leushina, E.; Spasennykh, M. Study of Organic Matter of Unconventional Reservoirs by IR Spectroscopy and IR Microscopy. Geosciences 2021, 11, 277. [Google Scholar] [CrossRef]
- González-Aragón Pineda, Á.E.; Borges-Yáñez, S.A.; Irigoyen-Camacho, M.E.; Lussi, A. Relationship between Erosive Tooth Wear and Beverage Consumption among a Group of Schoolchildren in Mexico City. Clin. Oral Investig. 2019, 23, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Hasheminejad, N.; Malek Mohammadi, T.; Mahmoodi, M.R.; Barkam, M.; Shahravan, A. The Association between Beverage Consumption Pattern and Dental Problems in Iranian Adolescents: A Cross Sectional Study. BMC Oral Health 2020, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Tellez, M.; Ismail, A.I. Estimating a Dynamic Effect of Soda Intake on Pediatric Dental Caries Using Targeted Maximum Likelihood Estimation Method. Caries Res. 2019, 53, 532–540. [Google Scholar] [CrossRef]
- Schmidt, J.; Huang, B. Awareness and Knowledge of Dental Erosion and Its Association with Beverage Consumption: A Multidisciplinary Survey. BMC Oral Health 2022, 22, 35. [Google Scholar] [CrossRef]
- Tudoroniu, C.; Popa, M.; Iacob, S.M.; Pop, A.L.; Năsui, B.A. Correlation of Caries Prevalence, Oral Health Behavior and Sweets Nutritional Habits among 10 to 19-Year-Old Cluj-Napoca Romanian Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6923. [Google Scholar] [CrossRef]
- Al-Amri, I.; Albounni, R.; Binalrimal, S. Evaluation of the Effect of Soft Drinks on the Surface Roughness of Dental Enamel in Natural Human Teeth. F1000Res 2021, 10, 1138. [Google Scholar] [CrossRef]
- Arafa, A.; Filfilan, S.S.; Fansa, H.A. Erosive Effect of Beverages on Surface Hardness and Ultra-Structure of Deciduous Teeth Enamel. Pediatr. Dent. J. 2022, 32, 186–192. [Google Scholar] [CrossRef]
- Kono, T.; Watanabe, A.; Kanno, T.; Ootani, Y.; Tamamura, R.; Sakae, T.; Okada, H. Second Order Differentiation Analysis of Micro FTIR Method Revealed the Variable Erosion Characteristics of Carbonated Soft Drink for the Individual Human Teeth Enamel. J. Hard Tissue Biol. 2019, 28, 7–12. [Google Scholar] [CrossRef]
- Manaswini, Y.H.; Uloopi, K.S.; Vinay, C.; Chandrasekhar, R.; RojaRamya, K.S. Impact of Calcium Glycerophosphate-Supplemented Carbonated Beverages in Reducing Mineral Loss from the Enamel Surface. Int. J. Clin. Pediatr. Dent. 2020, 13, 1–5. [Google Scholar] [CrossRef] [PubMed]
- De Paula, R.M.; Apolinário, R.d.S.; Martins, I.C.F.; Gonçalves, H.R.M.; Vieira, J.L.F.; Chaves, M.D.G.A.M.; Barb, N.R. Ex Vivo Evaluation of the Erosive Potential of Typical Fruit Juices from Brazilian Tropical Forests. JCDR 2019, 13, ZC36–ZC40. [Google Scholar] [CrossRef]
- Ramya, G.; Muralidharan, N.P. Estimation of Demineralisation Activity of Soft Drinks on Extracted Teeth—In Vitro Study. Biosci. Biotech. Res. Commun. 2020, 13, 468–471. [Google Scholar] [CrossRef]
- Sooksompien, P.; Sirimaharaj, V.; Wanachantararak, S. Carbonated Soft Drinks Induced Erosive Changes on Enamel Surfaces of Primary Teeth: SEM-EDS Analysis. J. Int. Dent. Med. Res. 2022, 15, 1046–1052. [Google Scholar]
- Bayne, S.C. Correlation of Clinical Performance with ‘in Vitro Tests’ of Restorative Dental Materials That Use Polymer-Based Matrices. Dent. Mater. 2012, 28, 52–71. [Google Scholar] [CrossRef]
- Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Lo, E.C.-M.; Chu, C.-H. A Review of the Common Models Used in Mechanistic Studies on Demineralization-Remineralization for Cariology Research. Dent. J. 2017, 5, 20. [Google Scholar] [CrossRef]
- Renton, C. Managing Dental Erosion. BDJ Team 2014, 1, 18–20. [Google Scholar] [CrossRef]
- Jaeggi, T.; Lussi, A. Prevalence, Incidence and Distribution of Erosion. Monogr. Oral Sci. 2006, 20, 44–65. [Google Scholar] [CrossRef]
- Wiegand, A.; Müller, J.; Werner, C.; Attin, T. Prevalence of Erosive Tooth Wear and Associated Risk Factors in 2–7-Year-Old German Kindergarten Children. Oral Dis. 2006, 12, 117–124. [Google Scholar] [CrossRef]
- de Carvalho, A.-C.-G.; de Souza, T.-F.; Liporoni, P.-C.-S.; Pizi, E.-C.-G.; Matuda, L.-S.A.; Catelan, A. Effect of Bleaching Agents on Hardness, Surface Roughness and Color Parameters of Dental Enamel. J. Clin. Exp. Dent. 2020, 12, e670–e675. [Google Scholar] [CrossRef]
- Larsen, M.J.; Nyvad, B. Enamel Erosion by Some Soft Drinks and Orange Juices Relative to Their PH, Buffering Effect and Contents of Calcium Phosphate. CRE 1999, 33, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Mutahar, M.; Carpenter, G.; Bartlett, D.; German, M.; Moazzez, R. The Presence of Acquired Enamel Pellicle Changes Acid-Induced Erosion from Dissolution to a Softening Process. Sci. Rep. 2017, 7, 10920. [Google Scholar] [CrossRef] [PubMed]
- Lagerlof, F.; Dawes, C. The Volume of Saliva in the Mouth Before and After Swallowing. J. Dent. Res. 1984, 63, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Chawhuaveang, D.D.; Yu, O.Y.; Yin, I.X.; Lam, W.Y.-H.; Mei, M.L.; Chu, C.-H. Acquired Salivary Pellicle and Oral Diseases: A Literature Review. J. Dent. Sci. 2021, 16, 523–529. [Google Scholar] [CrossRef]
- Fuzio, D.; Inchingolo, A.M.; Ruggieri, V.; Fasano, M.; Federico, M.; Mandorino, M.; Dirienzo, L.; Scacco, S.; Rizzello, A.; Delvecchio, M.; et al. Inflammation as Prognostic Hallmark of Clinical Outcome in Patients with SARS-CoV-2 Infection. Life 2023, 13, 322. [Google Scholar] [CrossRef]
- Iorgulescu, G. Saliva between Normal and Pathological. Important Factors in Determining Systemic and Oral Health. J. Med. Life 2009, 2, 303–307. [Google Scholar]
- Ghallab, A. In Vitro Test Systems and Their Limitations. EXCLI J. 2013, 12, 1024–1026. [Google Scholar]
- Nayak, P.; Singla, N.; Prasad, K.V.; Rao, N. Are Soft Drinks Soft on Teeth? A Study on Dental Erosion Caused by Soft Drinks Marketed in India. Indian J. Public Health Res. Dev. 2019, 10, 245. [Google Scholar] [CrossRef]
- Poureslami, H.R.; Hoseinifar, R.; Hoseinifar, R.; Sharifi, H.; Poureslami, P. Concentration of Calcium, Phosphate and Fluoride Ions in Microbial Plaque and Saliva after Using CPP-ACP Paste in 6–9 Year-Old Children. J. Dent. Biomater. 2016, 3, 214–219. [Google Scholar]
- Maladkar, S.R.; Yadav, P.; Muniraja, A.N.A.; Uchil, G.S.; George, L.V.; Augustine, D.; Rao, R.S.; Patil, S.; Sowmya, S.V.; Haragannavar, V.C. Erosive Effect of Acidic Beverages and Dietary Preservatives on Extracted Human Teeth—An In Vitro Analysis. Eur. J. Dent. 2022, 16, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Gallo, S.; Chiesa, M.; Poggio, C.; Scribante, A.; Zampetti, P.; Pietrocola, G. In Vitro Weight Loss of Dental Composite Resins and Glass-Ionomer Cements Exposed to a Challenge Simulating the Oral Intake of Acidic Drinks and Foods. J. Compos. Sci. 2021, 5, 298. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Polimeni, A.; Di Iorio, D.; Carinci, F. Bacterial Adhesion on Commercially Pure Titanium and Anatase-Coated Titanium Healing Screws: An in Vivo Human Study. J. Periodontol. 2010, 81, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Barros, R.R.M.; Iezzi, G.; Piattelli, A.; Novaes, A.B. Acellular Dermal Matrix Graft for Gingival Augmentation: A Preliminary Clinical, Histologic, and Ultrastructural Evaluation. J. Periodontol. 2009, 80, 253–259. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Scardina, G.A.; Pezzullo, S.; Scribante, A. Home Oral Care Domiciliary Protocol for the Management of Dental Erosion in Rugby Players: A Randomized Clinical Trial. J. Clin. Med. 2022, 11, 4893. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; De Biase, C.; Cazzolla, A.P.; Campobasso, A.; Dioguardi, M.; Piancino, M.G.; Mattia, L.; Ribatti, D.; Di Comite, M. Effects of Contact Sports on Temporomandibular Disorders: An Observational Study. Dent. J. 2022, 10, 180. [Google Scholar] [CrossRef]
- Kumar, N.; Amin, F.; Hashem, D.; Khan, S.; Zaidi, H.; Rahman, S.; Farhan, T.; Mahmood, S.J.; Asghar, M.A.; Zafar, M.S. Evaluating the PH of Various Commercially Available Beverages in Pakistan: Impact of Highly Acidic Beverages on the Surface Hardness and Weight Loss of Human Teeth. Biomimetics 2022, 7, 102. [Google Scholar] [CrossRef]
- Noble, W.; Donovan, T.; Geissberger, M. Sports Drinks and Dental Erosion. J. Calif. Dent. Assoc. 2011, 39, 233–238. [Google Scholar] [CrossRef]
- Nijakowski, K.; Walerczyk-Sas, A.; Surdacka, A. Regular Physical Activity as a Potential Risk Factor for Erosive Lesions in Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 3002. [Google Scholar] [CrossRef]
- Nijakowski, K.; Zdrojewski, J.; Nowak, M.; Podgórski, F.; Surdacka, A. Regular Physical Activity and Dental Erosion: A Systematic Review. Appl. Sci. 2022, 12, 1099. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | KEYWORDS: A: soft drinks; B: tooth |
| Boolean Indicators: A AND B | |
| Timespan: 2018–2023. | |
| Electronic databes: Pubmed; Scopus; WOS. |
| Authors (Year) | Type of the Study | Aim of the Study | Materials | Results |
|---|---|---|---|---|
| Al-Zwaylif et al. (2018) [40] | Study in vivo | Explore the interrelationship between -type and timing of dietary acid intake and -tooth wear. | 3586 participants. Data collected: -on four different types of acidic meals, -on the time at which they were consumed, -on the amount of surface area with moderate to severe tooth wear, and -on the type and -timing of acid consumption in the diet. | Dental deterioration has been linked to daily use of soft drinks. Consumption of soft drinks with meals has been linked to mild or severe tooth decay. Other meals and acidic drinks were not linked to tooth deterioration, regardless of when they were consumed. |
| González-Aragón Pined et al. (2019) [64] | Cross-sectional study in vivo | Evaluate the relationship: use of various drinks–erosive tooth wear. | To calculate ETW (Erosive Teeth Wear), a questionnaire was used to monitor the frequency of beverage intake, which included
| Consuming milk and milk derivatives might serve as a dietary substitute for sugary carbonated beverages in order to help avoid ETW. |
| Hasheminejad et al. (2020) [65] | Study in vivo | Valuate association beverage intake pattern–dental caries–tooth erosion. | A questionnaire was used to determine normal drinking frequency of 600 adolescents. | Adolescents have a propensity to drink harmful beverages.
|
| Lim et al. (2019) [66] | Study in vivo | The long-term impact of soda intake on dental cavities in young children can alter. Assessing a dynamic impact might be difficult due to follow-up loss and time-varying confounding. The goal of this work is to show how the targeted maximum likelihood estimate technique may be used to overcome obstacles with longitudinal data analysis and estimate the dynamic effect of soda consumption on pediatric caries. | 995 pairs of caregivers. The task was to monitor the tooth surface of the children. Variables included -caregiver smoking, -oral health fatalism, and -social support. Children who drank lots of sodas had more cavities than those who did not. The association between soda drinking patterns and caries was investigated using targeted maximum likelihood estimation. | Improper nutrition in childhood resulted in a carious tooth surface. The study demonstrates the use of targeted maximum likelihood estimation in pediatric research because it can address the modeling challenges associated with longitudinal data. |
| Morgado et al. (2022) [49] | Study in vivo | Prevent the growing issue of dental erosion, especially in the most at-risk patients evaluating the pH values of bottled water and inform patients and clinicians about its erosive potential. | Ph analysis of 105 types of bottled water analyzed: -32 of these were carbonated water; -73 were still water. | The pH of several tested waters is below the safe level for makeup and/or teeth, implying that they are more dangerous to consume than others. |
| Schmidt et al. (2022) [67] | Study in vivo | Determine the correlations between -sociodemographic characteristics, -awareness and knowledge of dental erosion, and -beverage consumption behaviors by measuring the awareness of dental erosion. | 418 students completed an online survey. |
|
| Tudoroniu et al. (2020) [68] | Study in vivo | Determine the presence of caries among adolescents and analyze the relationship between oral hygiene practices and consumption of sugary foods. | 650 adolescents answered a questionnaire to analyze the correlation between -the DMFT index, -oral hygiene, and -food habits | Adolescents continue to have a significant prevalence of caries determined by their eating habits. |
| Authors (Year) | Type of the Study | Aim of the Study | Materials | Results |
|---|---|---|---|---|
| Al-Amri et al. (2021) [69] | Study in vitro | The enamel exposed to sweet drinks undergoes microscopic changes due to -pH, -time of exhibition, and -other ingredients in the drinks. | three sets of extracted teeth immersed: -in sweet drinks and -in saliva presented, with the use of a profilometer, alterations in tooth surface roughness. | Exposure to sweet drinks increased surface roughness on teeth. |
| Arafa et al. (2022) [70] | Study in vitro | Dental dentin and enamel respond to carbonated soft drinks. | After one week of exposure to soft drinks, teeth showed, microscopically and with X-ray microdiffraction analysis, a wide range of enamel decay. | Soft drinks caused high erosive effect on the enamel surface of teeth, while milk showed no difference from saliva. |
| Charpe et al. (2019) [59] | Study in vitro | Assess and contrast the solubility of tooth enamel after exposure to alcoholic beverages across various time periods. | Three distinct beverages were tested for enamel solubility at various time intervals, with extracted teeth. Calcium released into the drinks was analyzed and determined using a semi-automatic analyzer and the Calcium Reagent Set. | Considerable mean calcium is lost beacause of -soft drinks and -beer, whiskey and hard drinks. |
| Gotouda et al. (2017) [61] | Study in vitro | Reaction of different types of dentin and enamel to carbonated beverages. | X-ray microdiffraction analysis showed a wide range of white stain areas in the enamel, ranging from barely perceptible to nearly complete decay. | This research provides fundamental crystallographic information that will soon be used in preventive dentistry. |
| Kono et al. (2019) [71] | Study in vitro | Micro-FTIR spectroscopic analysis of teeth sections to clarify chemical processes of dental caries. | X-ray microdiffraction analysis showed a wide range of white stain areas in the enamel, ranging from barely perceptible to nearly complete decay. | This study demonstrated the range and normalcy of dental enamel features. |
| Manaswini et al. (2020) [72] | Study in vitro | This study’s objective was to compare the mineral loss and surface microhardness of enamel exposed to carbonated drinks with and without calcium glycerophosphate (CaGP). | The surface microhardness of 40 samples of enamel was assessed to determine mineral loss, using -four cycles of intermittent blotting and -spectrophotometric analysis | The decline in the enamel’s surface microhardness and mineral loss were both dramatically halted by the addition of CaGP to the carbonated drinks. |
| Panic et al. (2019) [62] | Study in vitro | Ascertain how carbonated beverages affected enamel and dentin at various times. | SEM was used to assess and take pictures of 20 samples after: -60 min, -24 h, and -7 days of exposure to the drinks. ANOVA was used to examine the data. | The pH values of the drinks were below the critical pH of the enamel: after as little as 60 min of exposure there were signs of erosion. |
| Paula et al. (2019) [73] | Study in vitro | Evaluation of: -pH, -acidity, and -erosive potential of juices. |
| Juices have an acidic pH, which can lead to erosiveness. |
| Ramya et al. (2020) [74] | Study in vitro | Examine how soft drinks affect removed teeth’s demineralization. |
| Carbonated and non-carbonated drinks have different effects on tooth structure. |
| Shroff et al. (2018) [39] | Study in vitro | erosive potential 20 drinks should be evaluated. |
| The experimental beverages had higher acidity values than the packaged fruit juices, resulting in significantly different weight loss after 6 and 24 h of immersion in carbonated beverages. |
| Sooksompien et al. (2022) [75] | Study in vitro |
| Soft drinks acid pH caused changes on the enamel surfaces. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.M.; Malcangi, G.; Ferrante, L.; Del Vecchio, G.; Viapiano, F.; Mancini, A.; Inchingolo, F.; Inchingolo, A.D.; Di Venere, D.; Dipalma, G.; et al. Damage from Carbonated Soft Drinks on Enamel: A Systematic Review. Nutrients 2023, 15, 1785. https://doi.org/10.3390/nu15071785
Inchingolo AM, Malcangi G, Ferrante L, Del Vecchio G, Viapiano F, Mancini A, Inchingolo F, Inchingolo AD, Di Venere D, Dipalma G, et al. Damage from Carbonated Soft Drinks on Enamel: A Systematic Review. Nutrients. 2023; 15(7):1785. https://doi.org/10.3390/nu15071785
Chicago/Turabian StyleInchingolo, Angelo Michele, Giuseppina Malcangi, Laura Ferrante, Gaetano Del Vecchio, Fabio Viapiano, Antonio Mancini, Francesco Inchingolo, Alessio Danilo Inchingolo, Daniela Di Venere, Gianna Dipalma, and et al. 2023. "Damage from Carbonated Soft Drinks on Enamel: A Systematic Review" Nutrients 15, no. 7: 1785. https://doi.org/10.3390/nu15071785
APA StyleInchingolo, A. M., Malcangi, G., Ferrante, L., Del Vecchio, G., Viapiano, F., Mancini, A., Inchingolo, F., Inchingolo, A. D., Di Venere, D., Dipalma, G., & Patano, A. (2023). Damage from Carbonated Soft Drinks on Enamel: A Systematic Review. Nutrients, 15(7), 1785. https://doi.org/10.3390/nu15071785