
Antioxidant and Anti-Inflammatory Effects of Oral Supplementation with a Highly-Concentrated Docosahexaenoic Acid (DHA) Triglyceride in Patients with Keratoconus: A Randomized Controlled Preliminary Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Intervention
2.3. Study Procedures
2.4. Laboratory Analyses
2.5. Statistical Analysis
3. Results
3.1. Baseline Data of Patients
3.2. Changes of Ophthalmological Variables
3.3. Changes of Biochemical Parameters
3.3.1. Lipidomic Variables
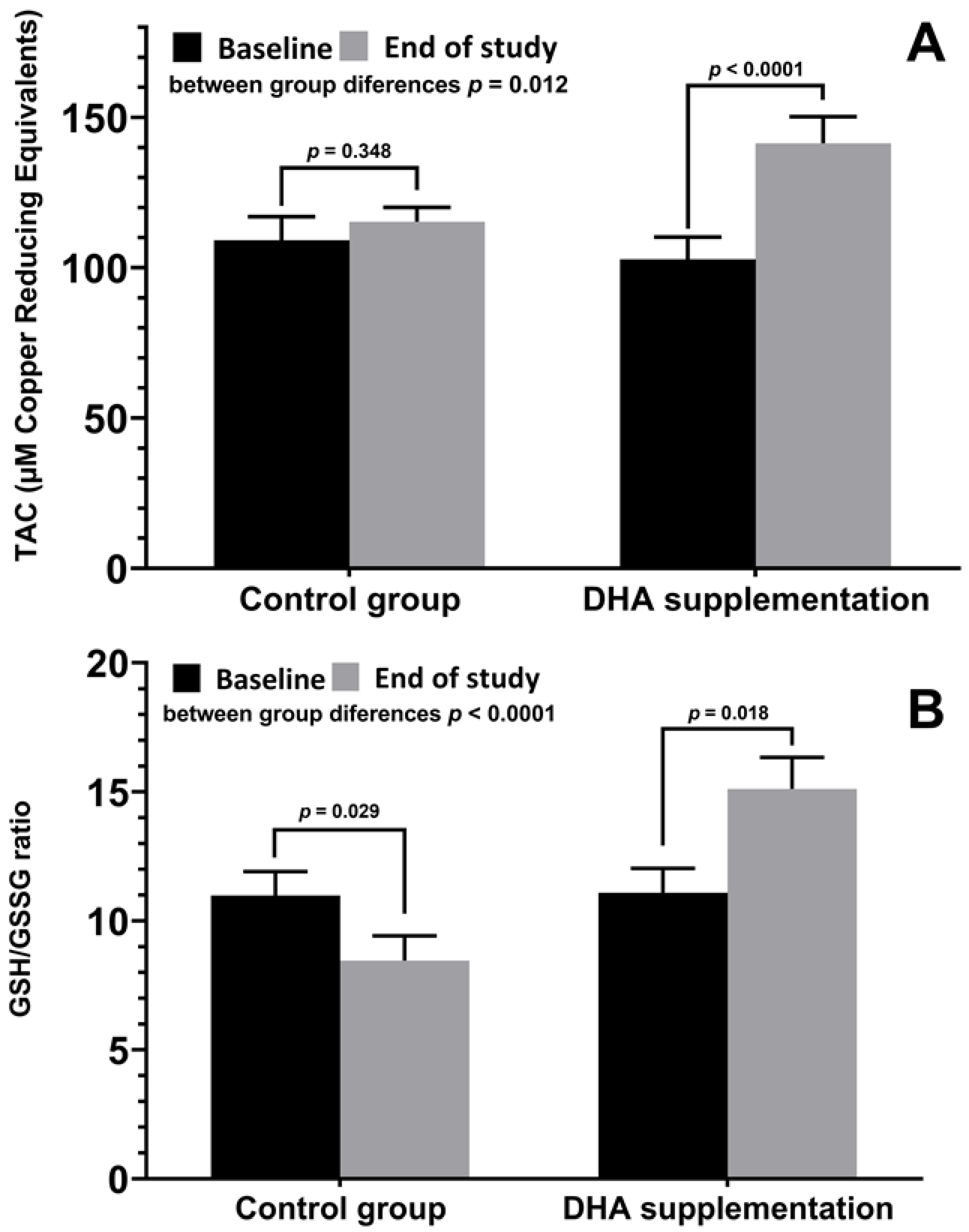
3.3.2. Antioxidant Variables
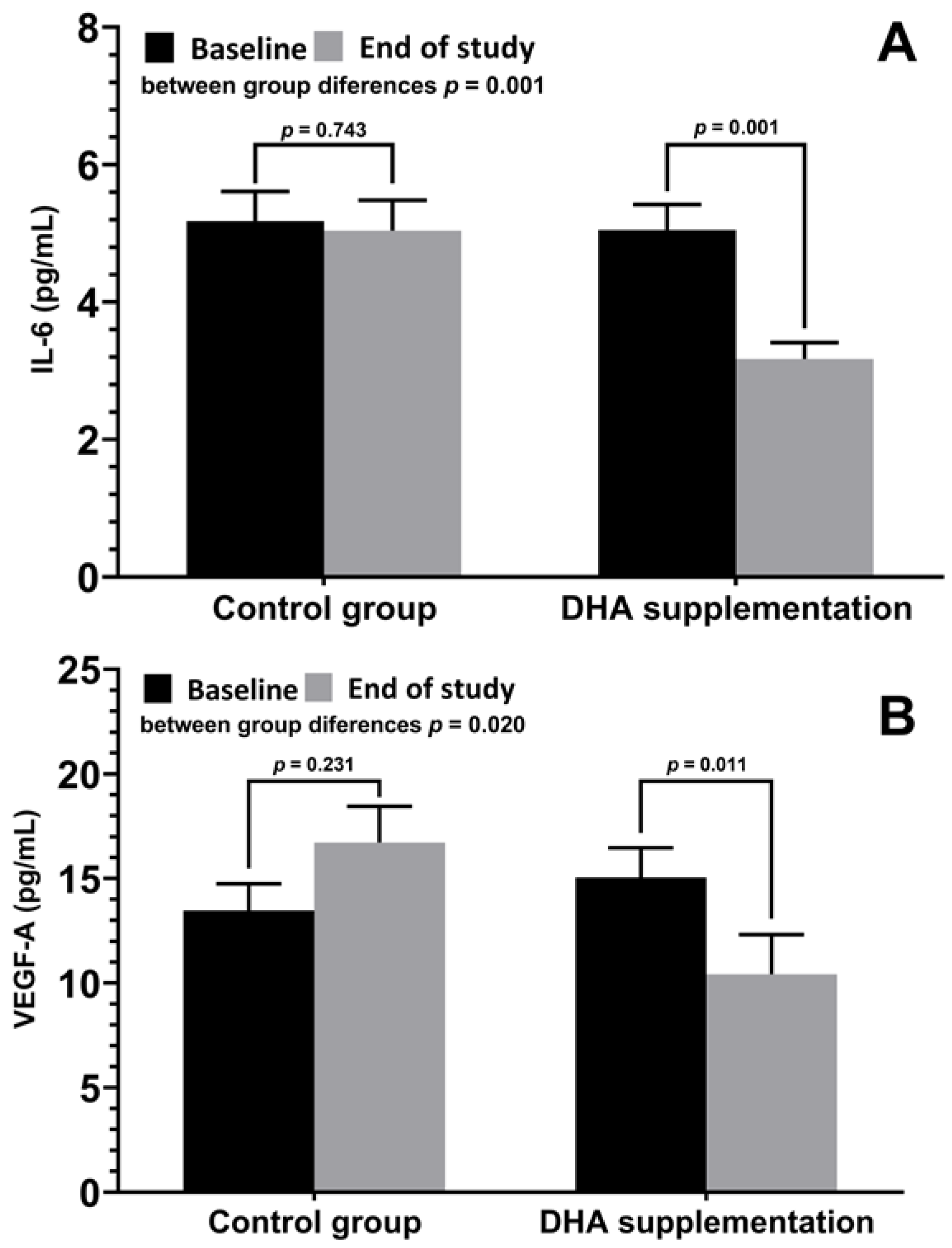
3.3.3. Inflammation-Related Variables
3.4. Correlations between Ophthalmological Variables and Biomarkers of Oxidative Stress and Inflammation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nowak, D.M.; Gajecka, M. The genetics of keratoconus. Middle East Afr. J. Ophthalmol. 2011, 18, 2–6. [Google Scholar]
- Gordon-Shaag, A.; Millodot, M.; Shneor, E.; Liu, Y. The genetic and environmental factors for keratoconus. Biomed. Res. Int. 2015, 2015, 795738. [Google Scholar] [CrossRef] [PubMed]
- Lasagni Vitar, R.M.; Bonelli, F.; Rama, P.; Ferrari, G. Nutritional and metabolic imbalance in keratoconus. Nutrients 2022, 14, 913. [Google Scholar] [CrossRef] [PubMed]
- Krachmer, J.H.; Feder, R.S.; Belin, M.W. Keratoconus and related noninflammatory corneal thinning disorders. Surv. Ophthalmol. 1984, 28, 293–322. [Google Scholar] [CrossRef] [PubMed]
- Galvis, V.; Sherwin, T.; Tello, A.; Merayo, J.; Barrera, R.; Acera, A. Keratoconus: An inflammatory disorder? Eye 2015, 29, 843–859. [Google Scholar] [CrossRef]
- Lema, I.; Durán, J.A. Inflammatory molecules in the tears of patients with keratoconus. Ophthalmology 2005, 112, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Arnal, E.; Peris-Martínez, C.; Menezo, J.L.; Johnsen-Soriano, S.; Romero, J.V. Oxidative stress in keratoconus? Investig. Ophthalmol. Vis. Sci. 2011, 52, 8592–8597. [Google Scholar] [CrossRef]
- Navel, V.; Malecaze, J.; Pereira, B.; Baker, J.S.; Malecaze, F.; Sapin, V.; Chiambaretta, F.; Dutheil, F. Oxidative and antioxidative stress markers in keratoconus: A systematic review and meta-analysis. Acta Ophthalmol. 2021, 99, e777–e794. [Google Scholar] [CrossRef]
- Wisse, R.P.; Kuiper, J.J.; Gans, R.; Imhof, S.; Radstake, T.R.; Van der Lelij, A. Cytokine expression in keratoconus and its corneal microenvironment: A systematic review. Ocul. Surf. 2015, 13, 272–283. [Google Scholar] [CrossRef]
- Karolak, J.A.; Gajecka, M. Genomic strategies to understand causes of keratoconus. Mol. Genet. Genom. 2017, 292, 251–269. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; D’Souza, S.; Khamar, P.; Ghosh, A.; Nuijts, R.M.M.A.; Sethu, S. Biochemical markers and alterations in keratoconus. Asia Pac. J. Ophthalmol. 2020, 9, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Kenchegowda, S.; Bazan, H.E. Significance of lipid mediators in corneal injury and repair. J. Lipid Res. 2010, 51, 879–891. [Google Scholar] [CrossRef]
- López-López, M.; Regueiro, U.; Bravo, S.B.; Chantada-Vázquez, M.D.P.; Varela-Fernández, R.; Ávila-Gómez, P.; Hervella, P.; Lema, I. Tear proteomics in keratoconus: A quantitative SWATH-MS analysis. Investig. Ophthalmol. Vis. Sci. 2021, 62, 30. [Google Scholar] [CrossRef] [PubMed]
- Santodomingo-Rubido, J.; Carracedo, G.; Suzaki, A.; Villa-Collar, C.; Vincent, S.J.; Wolffsohn, J.S. Keratoconus: An updated review. Cont. Lens Anterior Eye 2022, 45, 101559. [Google Scholar] [CrossRef] [PubMed]
- Espandar, L.; Meyer, J. Keratoconus: Overview and update on treatment. Middle East Afr. J. Ophthalmol. 2010, 17, 15–20. [Google Scholar] [PubMed]
- Gupta, P.C.; Pathak, M.; Thakur, B.; Fogla, R.; Agarwal, A.; Ram, J. Association of keratoconus with serum levels of 25-hydroxyvitamin D and antioxidant trace elements: A systematic review and meta-analysis. Indian J. Ophthalmol. 2022, 70, 2818–2824. [Google Scholar]
- Lasagni Vitar, R.M.; Fonteyne, P.; Knutsson, K.A.; Bertuzzi, F.; Galli, L.; Rama, P.; Ferrari, G. Vitamin D supplementation impacts systemic biomarkers of collagen degradation and copper metabolism in patients with keratoconus. Transl. Vis. Sci. Technol. 2022, 11, 16. [Google Scholar] [CrossRef]
- Aslan, M.G.; Fındık, H.; Okutucu, M.; Aydın, E.; Oruç, Y.; Arpa, M.; Uzun, F. Serum 25-hydroxy vitamin D, vitamin B12, and folic acid levels in progressive and nonprogressive keratoconus. Cornea 2021, 40, 334–341. [Google Scholar] [CrossRef]
- Zarei-Ghanavati, S.; Yahaghi, B.; Hassanzadeh, S.; Mobarhan, M.G.; Hakimi, H.R.; Eghbali, P. Serum 25-hydroxyvitamin D, selenium, zinc and copper in patients with keratoconus. J. Curr. Ophthalmol. 2020, 32, 26–31. [Google Scholar] [CrossRef]
- McKay, T.B.; Priyadarsini, S.; Rowsey, T.; Karamichos, D. Arginine supplementation promotes extracellular matrix and metabolic changes in keratoconus. Cells 2021, 10, 2076. [Google Scholar] [CrossRef]
- Sun, G.Y.; Simonyi, A.; Fritsche, K.L.; Chuang, D.Y.; Hannink, M.; Gu, Z.; Greenlief, C.M.; Yao, J.K.; Lee, J.C.; Beversdorf, D.Q. Docosahexaenoic acid (DHA): An essential nutrient and a nutraceutical for brain health and diseases. Prostaglandins Leukot. Essent. Fatty Acids 2018, 136, 3–13. [Google Scholar] [CrossRef]
- Swanson, D.; Block, R.; Mousa, S.A. Omega-3 fatty acids EPA and DHA: Health benefits throughout life. Adv. Nutr. 2012, 3, 1–7. [Google Scholar] [CrossRef]
- Troesch, B.; Eggersdorfer, M.; Laviano, A.; Rolland, Y.; Smith, A.D.; Warnke, I.; Weimann, A.; Calder, P.C. Expert opinion on benefits of long-chain omega-3 fatty acids (DHA and EPA) in aging and clinical nutrition. Nutrients 2020, 12, 2555. [Google Scholar] [CrossRef] [PubMed]
- Lafuente, M.; Rodríguez González-Herrero, M.E.; Romeo Villadóniga, S.; Domingo, J.C. Antioxidant activity and neuroprotective role of docosahexaenoic acid (DHA) supplementation in eye diseases that can lead to blindness: A narrative review. Antioxidants 2021, 10, 386. [Google Scholar] [CrossRef] [PubMed]
- Piñas García, P.; Hernández Martínez, F.J.; Aznárez López, N.; Castillón Torre, L.; Tena Sempere, M.E. Supplementation with a highly concentrated docosahexaenoic acid (DHA) in non-proliferative diabetic retinopathy: A 2-year randomized double-blind placebo-controlled study. Antioxidants 2022, 11, 116. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez González-Herrero, M.E.; Ruiz, M.; López Román, F.J.; Marín Sánchez, J.M.; Domingo, J.C. Supplementation with a highly concentrated docosahexaenoic acid plus xanthophyll carotenoid multivitamin in nonproliferative diabetic retinopathy: Prospective controlled study of macular function by fundus microperimetry. Clin. Ophthalmol. 2018, 12, 1011–1020. [Google Scholar] [CrossRef]
- Lafuente, M.; Ortín, L.; Argente, M.; Guindo, J.L.; López-Bernal, M.D.; López-Román, F.J.; García, M.J.; Domingo, J.C.; Lajara, J. Combined intravitreal ranibizumab and oral supplementation with docosahexaenoic acid and antioxidants for diabetic macular edema: Two-year randomized single-blind controlled trial results. Retina 2017, 37, 1277–1286. [Google Scholar] [CrossRef]
- Lafuente, M.; Ortín, L.; Argente, M.; Guindo, J.L.; López-Bernal, M.D.; López-Román, F.J.; Domingo, J.C.; Lajara, J. Three-year outcomes in a randomized single-blind controlled trial of intravitreal ranibizumab and oral supplementation with docosahexaenoic acid and antioxidants for diabetic macular edema. Retina 2019, 39, 1083–1090. [Google Scholar] [CrossRef]
- Pinazo-Durán, M.D.; Galbis-Estrada, C.; Pons-Vázquez, S.; Cantú-Dibildox, J.; Marco-Ramírez, C.; Benítez-del-Castillo, J. Effects of a nutraceutical formulation based on the combination of antioxidants and ω-3 essential fatty acids in the expression of inflammation and immune response mediators in tears from patients with dry eye disorders. Clin. Interv. Aging 2013, 8, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Galbis-Estrada, C.; Pinazo-Durán, M.D.; Cantú-Dibildox, J.; Marco-Ramírez, C.; Díaz-Llópis, M.; Benítez-del-Castillo, J. Patients undergoing long-term treatment with antihypertensive eye drops responded positively with respect to their ocular surface disorder to oral supplementation with antioxidants and essential fatty acids. Clin. Interv. Aging 2013, 8, 711–719. [Google Scholar]
- Oleñik, A.; Mahillo-Fernández, I.; Alejandre-Alba, N.; Fernández-Sanz, G.; Pérez, M.A.; Luxan, S.; Quintana, S.; Martínez de Carneros Llorente, A.; García-Sandoval, B.; Jiménez-Alfaro, I. Benefits of omega-3 fatty acid dietary supplementation on health-related quality of life in patients with meibomian gland dysfunction. Clin. Ophthalmol. 2014, 30, 831–836. [Google Scholar] [CrossRef]
- Oleñik, A.; Jiménez-Alfaro, I.; Alejandre-Alba, N.; Mahillo-Fernández, I. A randomized, double-masked study to evaluate the effect of omega-3 fatty acids supplementation in meibomian gland dysfunction. Clin. Interv. Aging 2013, 8, 1133–1138. [Google Scholar] [CrossRef]
- Romeo Villadóniga, S.; Rodríguez García, E.; Sagastagoia Epelde, O.; Álvarez Díaz, M.D.; Domingo Pedrol, J.C. Effects of oral supplementation with docosahexaenoic acid (DHA) plus antioxidants in pseudoexfoliative glaucoma: A 6-month open-label randomized trial. J. Ophthalmol. 2018, 2018, 8259371. [Google Scholar] [CrossRef]
- Krumeich, J.H.; Daniel, J.; Knülle, A. Live-epikeratophakia for keratoconus. J. Cataract Refract. Surg. 1998, 24, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, Y.S. Keratoconus. Surv. Ophthalmol. 1998, 42, 297–319. [Google Scholar] [CrossRef] [PubMed]
- Brudy Technology SL. Use of DHA for Treating a Pathology Associated with Cellular Oxidative Damage. European Patent EP 1962825 B1, 2 April 2014. [Google Scholar]
- Gasso, F.; Bogdanov, P.; Domingo, J.C. Docosahexaenoic acid improves endogenous antioxidant defense in ARPE-19 cells. Investig. Ophthalmol. Vis. Sci. 2008, 49, 5932. [Google Scholar]
- Nishtala, K.; Pahuja, N.; Shetty, R.; Nuijts, R.M.; Ghosh, A. Tear biomarkers for keratoconus. Eye Vis. 2016, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, I.C.; Corbu, C.G.; Tanase, C.; Ionita, G.; Nicula, C.; Coviltir, V.; Potop, V.; Constantin, M.; Codrici, E.; Mihai, S.; et al. Overexpression of tear inflammatory cytokines as additional finding in keratoconus patients and their first degree family members. Mediat. Inflamm. 2018, 2018, 4285268. [Google Scholar] [CrossRef]
- Sorkhabi, R.; Ghorbanihaghjo, A.; Taheri, N.; Ahoor, M.H. Tear film inflammatory mediators in patients with keratoconus. Int. Ophthalmol. 2015, 35, 467–472. [Google Scholar] [CrossRef]
- Peyman, A.; Namgar, M.; Feizi, A.; Hakemi, M.G.; Nasab, F.H.; Pourazizi, M. Interleukin-6 and tumor necrosis factor-α levels in tear film of keratoconus patients. J. Res. Med. Sci. 2021, 26, 75. [Google Scholar] [CrossRef]
- Zhang, H.; Cao, X.; Liu, Y.; Wang, P.; Li, X. Tear levels of inflammatory cytokines in keratoconus: A meta-analysis of case-control and cross-sectional studies. Biomed. Res. Int. 2021, 2021, 6628923. [Google Scholar] [CrossRef] [PubMed]
- Lema, I.; Sobrino, T.; Durán, J.A.; Brea, D.; Díez-Feijoo, E. Subclinical keratoconus and inflammatory molecules from tears. Br. J. Ophthalmol. 2009, 93, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Cagini, C.; Messina, M.; Torroni, G.; Riccitelli, F.; Mariniello, M.; Dua, H.S. Efficacy of topical microemulsion of fatty acids of the ω-3 series on the sub-epithelial corneal nerves regeneration after epithelium-off corneal collagen cross-linking for keratoconus. Int. Ophthalmol. 2020, 40, 205–212. [Google Scholar] [CrossRef]
- Ondes Yilmaz, F.; Kepez Yildiz, B.; Tunc, U.; Kandemir Besek, N.; Yildirim, Y.; Demirok, A. Comparison of topical omega-3 fatty acids with topical sodium hyaluronate after corneal crosslinking: Short term results. Ocul. Immunol. Inflamm. 2022, 30, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, T.; Funnell, C.L.; Cassels-Brown, A.; O’Conor, R. Influence of ethnic origin on the incidence of keratoconus and associated atopic disease in Asians and white patients. Eye 2004, 18, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Kristianslund, O.; Drolsum, L. Prevalence of keratoconus in persons with Down syndrome: A review. BMJ Open Ophthalmol. 2021, 6, e000754. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All Patients (n = 34) | Control Group (n = 15) | DHA Group (n = 19) | p Value |
|---|---|---|---|---|
| Gender, n (%) | 0.638 | |||
| Men | 25 (73.5) | 12 (80) | 13 (68.4) | |
| Women | 9 (26.5) | 3 (20) | 6 (31.6) | |
| Age, years, mean (SD) | 31 (10) | 33 (9) | 30 (11) | 0.484 |
| Time since diagnosis, months, mean (SD) | 3.7 (2.8) | 4.3 (4.1) | 3.3 (0.8) | 0.366 |
| Variables | Control Group (n = 15) | DHA Group (n = 19) | Within-Group p Value | Between-Group p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | Baseline | End of Study | Control Group | DHA Group | Baseline | End of Study | |
| K1, diopters | 43.5 (3.0) | 43.6 (3.1) | 44.9 (2.9) | 44.0 (2.8) | 0.571 | 0.387 | 0.176 | 0.163 |
| K2, diopters | 47.0 (3.5) | 47.1 (3.4) | 48.8 (3.8) | 48.8 (3.7) | 0.221 | 0.779 | 0.155 | 0.174 |
| Kmax, diopters | 53.2 (6.0) | 53.2 (5.8) | 54.9 (5.6) | 54.8 (5.6) | 0.671 | 0.271 | 0.407 | 0.440 |
| Km, diopters | 45.1 (3.1) | 45,2 (3.1) | 46.8 (3.0) | 46.8 (2.9) | 0.299 | 0.409 | 0.147 | 0.145 |
| Astigmatism axis, degrees | 124.4 (52.7) | 119.7 (58.4) | 66.0 (63.6) | 69.7 (60.8) | 0.369 | 0.310 | 0.006 | 0.021 |
| Astigmatism degree diopters | 3.4 (1.6) | 3.5 (1.7) | 3.8 (2.7) | 3.8 (2.7) | 0.539 | 0.494 | 0.578 | 0.711 |
| Asphericity coefficient (D) | ||||||||
| Horizontal hemi-axis | −0.4 (0.4) | −0.4 (0.4) | −0.7 (0.3) | −0.7 (0.3) | 0.612 | 0.119 | 0.022 | 0.015 |
| Vertical hemi-axis | −0.4 (0.3) | −0.4 (0.4) | −0.8 (0.3) | −0.8 (0.3) | 0.346 | 0.771 | 0.008 | 0.007 |
| CAT, µm | 489.8 (38.7) | 491.6 (39.2) | 469,3 (46.7) | 470.3 (46.7) | 0.147 | 0.318 | 0.172 | 0.157 |
| CCT, µm | 495.8 (37.2) | 498.2 (37.6) | 478.1 (44.6) | 478.4 (44.7) | 0.045 | 0.734 | 0.217 | 0.171 |
| MCT, µm | 470.4 (51.9) | 470.7 (50.6) | 459.8 (46.5) | 461.0 (46.4) | 0.830 | 0.252 | 0.541 | 0.568 |
| CA, mm | 2.4 (1.8) | 2.4 (1.8) | 2.2 (1.3) | 2.3 (1.3) | 0.111 | 0.528 | 0.675 | 0.900 |
| IOP GAT, mmHg | 10.8 (2.4) | 11.9 (4.0) | 11.5 (3.2) | 10.3 (3.0) | 0.214 | 0.052 | 0.373 | 0.192 |
| IOP rebound, mmHg | 10.4 (3.3) | 10.8 (2.8) | 10.6 (3.2) | 9.9 (3.0) | 0.672 | 0.371 | 0.839 | 0.381 |
| Variables | Control Group (n = 15) | DHA Group (n = 19) | Within-Group p Value | Between-Group p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | Baseline | End of Study | Control Group | DHA Group | Baseline | End of Study | |
| DHA, % total fatty acids | 2.98 (0.19) | 2.97 (0.18) | 3.02 (0.23) | 4.95 (0.13) | 0.945 | <0.0001 | 0.925 | <0.0001 |
| ARA, % total fatty acids | 12.93 (0.16) | 12.58 (0.20) | 12.85 (0.23) | 11.52 (0.25) | 0.009 | <0.0001 | 0.831 | 0.005 |
| n-6 PUFA/n-3 PUFA | 6.61 (0.50) | 6.43 (0.49) | 6.55 (0.51) | 3.79 (0.14) | 0.304 | <0.0001 | 0.878 | <0.0001 |
| Omega-3 index | 3.23 (0.21) | 3.21 (0.19) | 3.30 (0.26) | 5.46 (0.16) | 0.890 | <0.0001 | 0.939 | <0.0001 |
| Variables | Control Group (n = 15) | DHA Group (n = 19) | Within-Group p Value | Between-Group p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | Baseline | End of Study | Control Group | DHA Group | Baseline | End of Study | |
| TAC, µ Cu reducing equiv. | 109.20 (7.80) | 115.30 (4.76) | 102.80 (7.37) | 141.40 (8.82) | 0.348 | <0.0001 | 0.556 | 0.012 |
| MDA, µM | 4.02 (0.23) | 4.36 (0.29) | 3.84 (0.17) | 3.15 (0.24) | 0.322 | 0.004 | 0.701 | 0.0007 |
| GSH, total, mmol/mg protein | 10.67 (0.55) | 10.12 (0.50) | 9.44 (0.55) | 10.30 (0.52) | 0.246 | 0.229 | 0.126 | 0.912 |
| GSH, free, mmol/mg protein | 8.87 (0.43) | 7.93 (0.45) | 7.90 (0.49) | 9.01 (0.48) | 0.118 | 0.121 | 0.224 | 0.071 |
| GSH/GSSG ratio | 10.98 (0.93) | 8.46 (0.96) | 11.09 (0.94) | 15.11 (1.22) | 0.029 | 0.018 | 0.986 | <0.0001 |
| Variables | Control Group (n = 15) | DHA Group (n = 19) | Within-Group p Value | Between-Group p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | Baseline | End of Study | Control Group | DHA Group | Baseline | End of Study | |
| IL-1β, pg/mL | 5.02 (0.43) | 7.43 (0.66) | 5.21 (0.47) | 6.24 (0.60) | 0.002 | 0.129 | 0.701 | 0.146 |
| IL-4, pg/mL | 2.84 (0.29) | 3.65 (0.34) | 2.89 (0.28) | 2.19 (0.22) | 0.002 | 0.087 | 0.805 | 0.0003 |
| IL-6, pg/mL | 5.18 (0.43) | 5.04 (0.44) | 5.05 (0.37) | 3.17 (0.24) | 0.743 | 0.0002 | 0.714 | 0.001 |
| IL-10, pg/mL | 4.21 (0.37) | 5.66 (0.52) | 4.15 (0.32) | 4.81 (0.54) | 0.015 | 0.404 | 0.939 | 0.167 |
| IL-18, pg/mL | 73.0 (6.09) | 74.97 (6.39) | 80.52 (7.17) | 79.74 (6.57) | 0.745 | 0.999 | 0.522 | 0.652 |
| TNF-α, pg/mL | 39.45 (3.81) | 43.29 (4.07) | 58.53 (5.17) | 49.36 (4.28) | 0.274 | 0.059 | 0.009 | 0.437 |
| VEGF-A, pg/mL | 13.46 (1.28) | 16.72 (1.73) | 15.04 (1.42) | 10.42 (1.90) | 0.231 | 0.011 | 0.528 | 0.020 |
| Ophthalmological Variables | Oxidative Stress/ Inflammatory Biomarkers | Correlation Coefficient (95% Confidence Interval) |
|---|---|---|
| K1, flat keratometry |
| −0.51 (−0.79 to −0.006) |
| 0.46 (−0.01 to 0.76) | |
| K2, steep keratometry |
| 0.65 (0.27 to 0.86) |
| 0.53 (0.09 to 0.80) | |
| Astigmatism axis |
| −0.49 (−0.78 to −0.03) |
| Astigmatism degree |
| 0.47 (0.0 to 0.77) |
| Central corneal thickness (CCT) |
| −0.46 (−0.76 to 0.0) |
| Chromatic aberration (CA) |
| 0.55 (0.11 to 0.81) |
| Intraocular pressure (IOP) (Goldmann applanation tonometry) |
| 0.50 (00.5 to 0.78) |
| 0.62 (0.21 to 0.84) | |
| 0.68 (0.31 to 0.87) | |
| −0.59 (−0.83 to −0.17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peris-Martínez, C.; Piá-Ludeña, J.V.; Rog-Revert, M.J.; Fernández-López, E.; Domingo, J.C. Antioxidant and Anti-Inflammatory Effects of Oral Supplementation with a Highly-Concentrated Docosahexaenoic Acid (DHA) Triglyceride in Patients with Keratoconus: A Randomized Controlled Preliminary Study. Nutrients 2023, 15, 1300. https://doi.org/10.3390/nu15051300
Peris-Martínez C, Piá-Ludeña JV, Rog-Revert MJ, Fernández-López E, Domingo JC. Antioxidant and Anti-Inflammatory Effects of Oral Supplementation with a Highly-Concentrated Docosahexaenoic Acid (DHA) Triglyceride in Patients with Keratoconus: A Randomized Controlled Preliminary Study. Nutrients. 2023; 15(5):1300. https://doi.org/10.3390/nu15051300
Chicago/Turabian StylePeris-Martínez, Cristina, José Vicente Piá-Ludeña, María José Rog-Revert, Ester Fernández-López, and Joan Carles Domingo. 2023. "Antioxidant and Anti-Inflammatory Effects of Oral Supplementation with a Highly-Concentrated Docosahexaenoic Acid (DHA) Triglyceride in Patients with Keratoconus: A Randomized Controlled Preliminary Study" Nutrients 15, no. 5: 1300. https://doi.org/10.3390/nu15051300
APA StylePeris-Martínez, C., Piá-Ludeña, J. V., Rog-Revert, M. J., Fernández-López, E., & Domingo, J. C. (2023). Antioxidant and Anti-Inflammatory Effects of Oral Supplementation with a Highly-Concentrated Docosahexaenoic Acid (DHA) Triglyceride in Patients with Keratoconus: A Randomized Controlled Preliminary Study. Nutrients, 15(5), 1300. https://doi.org/10.3390/nu15051300