
Dietary Arginine and Citrulline Supplements for Cardiovascular Health and Athletic Performance: A Narrative Review

 ,
,  ,
,  ,
,
Abstract
1. Introduction
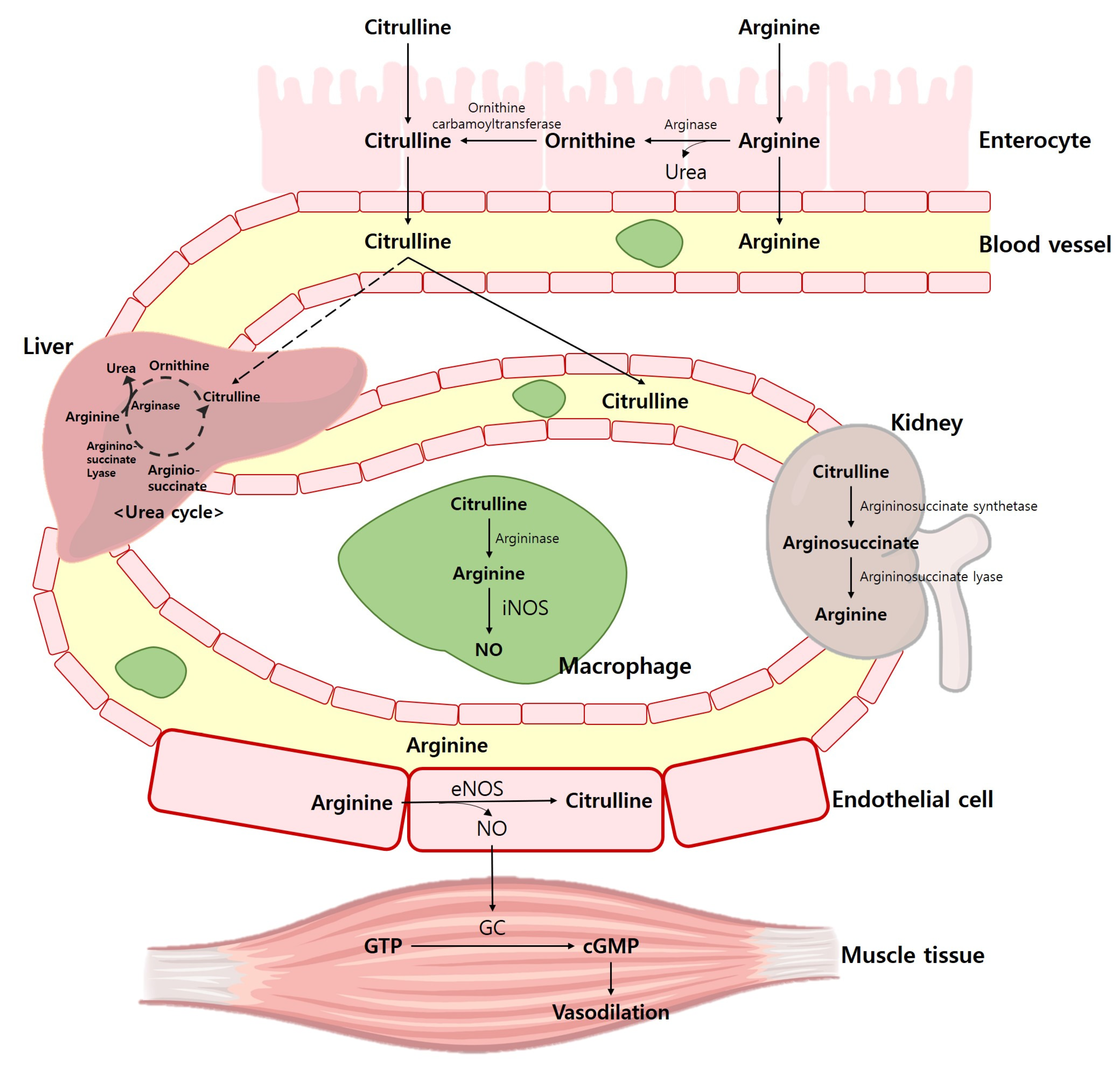
2. Physiological Role of Arginine and Citrulline in Human
Intake of Arginine and Citrulline Supplements
3. Effect of Cardiovascular Health
3.1. Hemodynamic Function
3.2. Endothelial Function
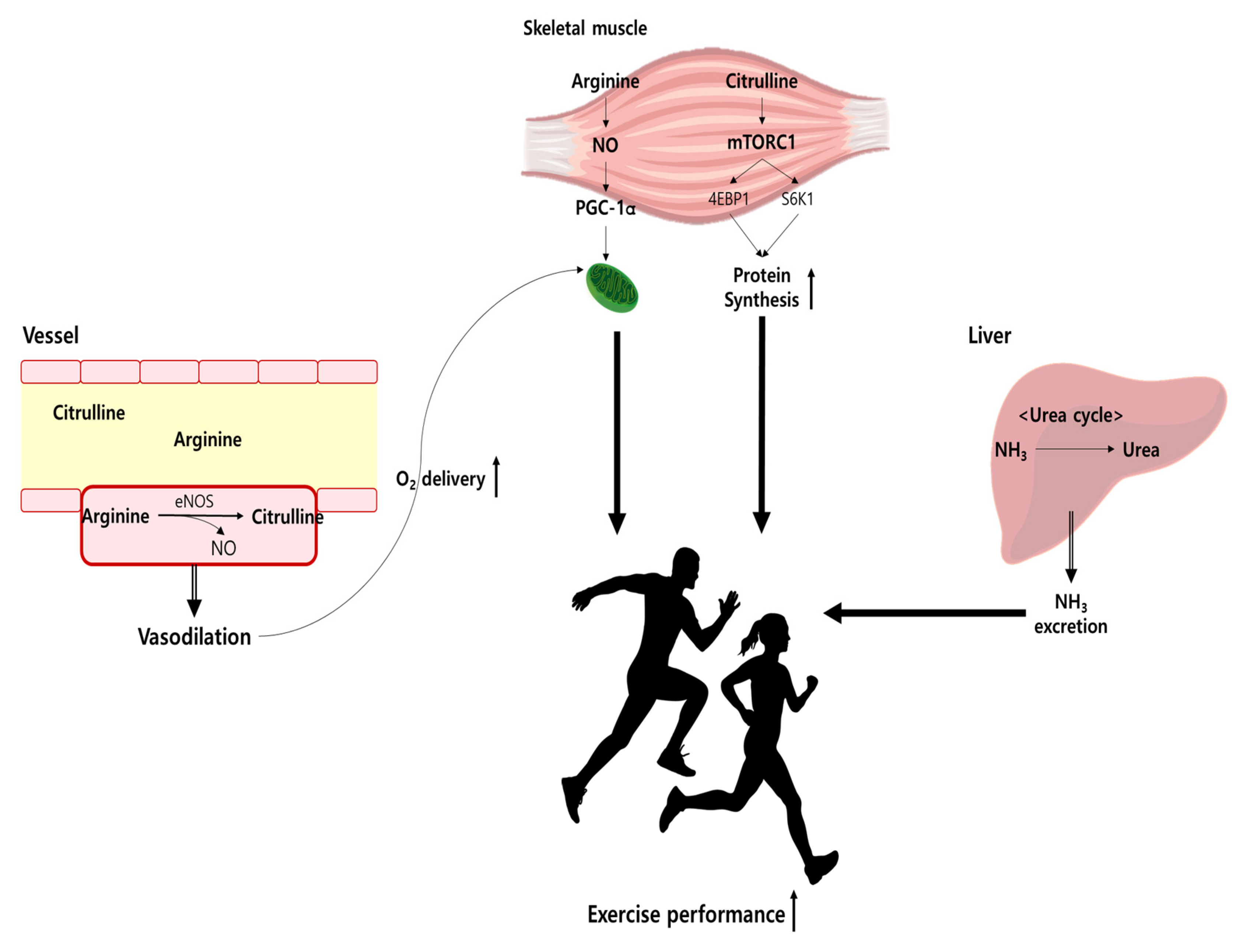
4. Effect of Athletic Performance
4.1. Anaerobic and Aerobic Capacity
4.2. Muscular Strength, Power, and Endurance Performances
5. Conclusions and Future Prospects
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nyawose, S.; Naidoo, R.; Naumovski, N.; McKune, A.J. The Effects of Consuming Amino Acids L-Arginine, L-Citrulline (and Their Combination) as a Beverage or Powder, on Athletic and Physical Performance: A Systematic Review. Beverages 2022, 8, 48. [Google Scholar] [CrossRef]
- Hys, K. Identification of the reasons why individual consumers purchase dietary supplements. In Perspectives on Consumer Behaviour; Springer: Cham, Switzerland, 2020; pp. 193–209. [Google Scholar]
- Research, G.V. Dietary Supplements Market Size Worth $327.4 Billion By 2030. Available online: https://www.grandviewresearch.com/press-release/global-dietary-supplements-market# (accessed on 15 November 2022).
- Binns, C.W.; Lee, M.K.; Lee, A.H. Problems and Prospects: Public Health Regulation of Dietary Supplements. Annu. Rev. Public Health 2018, 39, 403–420. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.A.; Bass, S. Injecting Safety into Supplements—Modernizing the Dietary Supplement Law. N. Engl. J. Med. 2019, 381, 2387–2389. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 52, 439–455. [Google Scholar] [CrossRef] [PubMed]
- Rawson, E.S.; Miles, M.P.; Larson-Meyer, D.E. Dietary Supplements for Health, Adaptation, and Recovery in Athletes. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 188–199. [Google Scholar] [CrossRef]
- Begg, P.M.; Wheatley, V.M. Fraud in dietary supplements. In Food Fraud; Academic Press: Cambridge, MA, USA, 2021; pp. 351–360. [Google Scholar]
- Gibson, M.E.; Schultz, J.; Glover, D. To Supplement or Not. Mo. Med. 2016, 113, 305–309. [Google Scholar]
- Collins, J.; Maughan, R.J.; Gleeson, M.; Bilsborough, J.; Jeukendrup, A.; Morton, J.P.; Phillips, S.M.; Armstrong, L.; Burke, L.M.; Close, G.L.; et al. UEFA expert group statement on nutrition in elite football. Current evidence to inform practical recommendations and guide future research. Br. J. Sports Med. 2021, 55, 416. [Google Scholar] [CrossRef] [PubMed]
- Orrù, S.; Imperlini, E.; Nigro, E.; Alfieri, A.; Cevenini, A.; Polito, R.; Daniele, A.; Buono, P.; Mancini, A. Role of Functional Beverages on Sport Performance and Recovery. Nutrients 2018, 10, 1470. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, S.; Gholamalizadeh, M.; Tabrizi, R.; Nowrouzi-Sohrabi, P.; Rastgoo, S.; Doaei, S. The effect of L-arginine supplementation on maximal oxygen uptake: A systematic review and meta-analysis. Physiol. Rep. 2021, 9, e14739. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.; Roberts, M.; Kerksick, C.; Wilborn, C.; Marcello, B.; Taylor, L.; Nassar, E.; Leutholtz, B.; Bowden, R.; Rasmussen, C.; et al. Pharmacokinetics, safety, and effects on exercise performance of L-arginine alpha-ketoglutarate in trained adult men. Nutrition 2006, 22, 872–881. [Google Scholar] [CrossRef]
- Fricke, O.; Baecker, N.; Heer, M.; Tutlewski, B.; Schoenau, E. The effect of L-arginine administration on muscle force and power in postmenopausal women. Clin. Physiol. Funct. Imaging 2008, 28, 307–311. [Google Scholar] [CrossRef]
- Koppo, K.; Taes, Y.E.; Pottier, A.; Boone, J.; Bouckaert, J.; Derave, W. Dietary arginine supplementation speeds pulmonary VO2 kinetics during cycle exercise. Med. Sci. Sports Exerc. 2009, 41, 1626–1632. [Google Scholar] [CrossRef]
- Maharaj, A.; Fischer, S.M.; Dillon, K.N.; Kang, Y.; Martinez, M.A.; Figueroa, A. Effects of L-Citrulline Supplementation on Endothelial Function and Blood Pressure in Hypertensive Postmenopausal Women. Nutrients 2022, 14, 4396. [Google Scholar] [CrossRef] [PubMed]
- Bode-Böger, S.M.; Muke, J.; Surdacki, A.; Brabant, G.; Böger, R.H.; Frölich, J.C. Oral L-arginine improves endothelial function in healthy individuals older than 70 years. Vasc. Med. 2003, 8, 77–81. [Google Scholar] [CrossRef]
- Lin, C.C.; Tsai, W.C.; Chen, J.Y.; Li, Y.H.; Lin, L.J.; Chen, J.H. Supplements of L-arginine attenuate the effects of high-fat meal on endothelial function and oxidative stress. Int. J. Cardiol. 2008, 127, 337–341. [Google Scholar] [CrossRef]
- Siasos, G.; Tousoulis, D.; Vlachopoulos, C.; Antoniades, C.; Stefanadi, E.; Ioakeimidis, N.; Andreou, I.; Zisimos, K.; Papavassiliou, A.G.; Stefanadis, C. Short-term treatment with L-arginine prevents the smoking-induced impairment of endothelial function and vascular elastic properties in young individuals. Int. J. Cardiol. 2008, 126, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wollman, Y.; Chernichovsky, T.; Iaina, A.; Sofer, M.; Matzkin, H. Effect of oral administration of high-dose nitric oxide donor L-arginine in men with organic erectile dysfunction: Results of a double-blind, randomized, placebo-controlled study. BJU Int. 1999, 83, 269–273. [Google Scholar] [CrossRef]
- Menafra, D.; de Angelis, C.; Garifalos, F.; Mazzella, M.; Galdiero, G.; Piscopo, M.; Castoro, M.; Verde, N.; Pivonello, C.; Simeoli, C.; et al. Long-term high-dose L-arginine supplementation in patients with vasculogenic erectile dysfunction: A multicentre, double-blind, randomized, placebo-controlled clinical trial. J. Endocrinol. Investig. 2022, 45, 941–961. [Google Scholar] [CrossRef]
- van de Poll, M.C.; Soeters, P.B.; Deutz, N.E.; Fearon, K.C.; Dejong, C.H. Renal metabolism of amino acids: Its role in interorgan amino acid exchange. Am. J. Clin. Nutr. 2004, 79, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Curis, E.; Nicolis, I.; Moinard, C.; Osowska, S.; Zerrouk, N.; Bénazeth, S.; Cynober, L. Almost all about citrulline in mammals. Amino Acids 2005, 29, 177–205. [Google Scholar] [CrossRef]
- Hou, X.; Chen, S.; Zhang, P.; Guo, D.; Wang, B. Targeted Arginine Metabolism Therapy: A Dilemma in Glioma Treatment. Front. Oncol. 2022, 12, 938847. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, R.J.; Williams, S.A.; Canale, R.E.; Farney, T.M.; Kabir, M.M. Acute effect of nitric oxide supplement on blood nitrate/nitrite and hemodynamic variables in resistance trained men. J. Strength Cond. Res. 2010, 24, 2587–2592. [Google Scholar] [CrossRef]
- Lorin, J.; Zeller, M.; Guilland, J.C.; Cottin, Y.; Vergely, C.; Rochette, L. Arginine and nitric oxide synthase: Regulatory mechanisms and cardiovascular aspects. Mol. Nutr. Food Res. 2014, 58, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Szefel, J.; Danielak, A.; Kruszewski, W.J. Metabolic pathways of L-arginine and therapeutic consequences in tumors. Adv. Med. Sci. 2019, 64, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, R.; Maté-Muñoz, J.L.; Cuenca, E.; García-Fernández, P.; Mata-Ordoñez, F.; Lozano-Estevan, M.C.; Veiga-Herreros, P.; da Silva, S.F.; Garnacho-Castaño, M.V. Effects of beetroot juice supplementation on intermittent high-intensity exercise efforts. J. Int. Soc. Sport Nutr. 2018, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef]
- Jones, A.M. Dietary nitric oxide precursors and exercise performance. Sports Sci. Exch. 2016, 28, 1–6. [Google Scholar]
- Álvares, T.S.; Meirelles, C.M.; Bhambhani, Y.N.; Paschoalin, V.M.; Gomes, P.S. L-Arginine as a potential ergogenic aid in healthy subjects. Sports Med. 2011, 41, 233–248. [Google Scholar] [CrossRef]
- Bailey, S.J.; Winyard, P.G.; Vanhatalo, A.; Blackwell, J.R.; DiMenna, F.J.; Wilkerson, D.P.; Jones, A.M. Acute L-arginine supplementation reduces the O2 cost of moderate-intensity exercise and enhances high-intensity exercise tolerance. J. Appl. Physiol. 2010, 109, 1394–1403. [Google Scholar] [CrossRef]
- Wylie, L.J.; Mohr, M.; Krustrup, P.; Jackman, S.R.; Ermιdis, G.; Kelly, J.; Black, M.I.; Bailey, S.J.; Vanhatalo, A.; Jones, A.M. Dietary nitrate supplementation improves team sport-specific intense intermittent exercise performance. Eur. J. Appl. Physiol. 2013, 113, 1673–1684. [Google Scholar] [CrossRef]
- Piknova, B.; Park, J.W.; Cassel, K.S.; Gilliard, C.N.; Schechter, A.N. Measuring Nitrite and Nitrate, Metabolites in the Nitric Oxide Pathway, in Biological Materials using the Chemiluminescence Method. J. Vis. Exp. 2016, 118, e54879. [Google Scholar] [CrossRef]
- Schaefer, A.; Piquard, F.; Geny, B.; Doutreleau, S.; Lampert, E.; Mettauer, B.; Lonsdorfer, J. L-arginine reduces exercise-induced increase in plasma lactate and ammonia. Int. J. Sport Med. 2002, 23, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.H.; Wu, C.L.; Chiang, C.W.; Lo, Y.W.; Tseng, H.F.; Chang, C.K. No effect of short-term arginine supplementation on nitric oxide production, metabolism and performance in intermittent exercise in athletes. J. Nutr. Biochem. 2009, 20, 462–468. [Google Scholar] [CrossRef]
- Alvares, T.S.; Conte-Junior, C.A.; Silva, J.T.; Paschoalin, V.M. L-arginine does not improve biochemical and hormonal response in trained runners after 4 weeks of supplementation. Nutr. Res. 2014, 34, 31–39. [Google Scholar] [CrossRef]
- Hiratsu, A.; Tataka, Y.; Namura, S.; Nagayama, C.; Hamada, Y.; Miyashita, M. The effects of acute and chronic oral l-arginine supplementation on exercise-induced ammonia accumulation and exercise performance in healthy young men: A randomised, double-blind, cross-over, placebo-controlled trial. J. Exerc. Sci. Fit. 2022, 20, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M. Dietary nitrate supplementation and exercise performance. Sport Med. 2014, 44 (Suppl. S1), 35–45. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Morita, M.; Hayashi, T.; Kamimura, A. The effects on plasma L-arginine levels of combined oral L-citrulline and L-arginine supplementation in healthy males. Biosci. Biotechnol. Biochem. 2017, 81, 372–375. [Google Scholar] [CrossRef]
- Morita, M.; Hayashi, T.; Ochiai, M.; Maeda, M.; Yamaguchi, T.; Ina, K.; Kuzuya, M. Oral supplementation with a combination of L-citrulline and L-arginine rapidly increases plasma L-arginine concentration and enhances NO bioavailability. Biochem. Biophys. Res. Commun. 2014, 454, 53–57. [Google Scholar] [CrossRef]
- Suzuki, I.; Sakuraba, K.; Horiike, T.; Kishi, T.; Yabe, J.; Suzuki, T.; Morita, M.; Nishimura, A.; Suzuki, Y. A combination of oral L-citrulline and L-arginine improved 10-min full-power cycling test performance in male collegiate soccer players: A randomized crossover trial. Eur. J. Appl. Physiol. 2019, 119, 1075–1084. [Google Scholar] [CrossRef]
- Mor, A.; Atan, T.; Agaoglu, S.A.; Ayyildiz, M. Effect of arginine supplementation on footballers’ anaerobic performance and recovery. Prog. Nutr. 2018, 20, 104–112. [Google Scholar]
- Chen, I.F.; Wu, H.J.; Chen, C.Y.; Chou, K.M.; Chang, C.K. Branched-chain amino acids, arginine, citrulline alleviate central fatigue after 3 simulated matches in taekwondo athletes: A randomized controlled trial. J. Int. Soc. Sport Nutr. 2016, 13, 28. [Google Scholar] [CrossRef]
- Agarwal, U.; Didelija, I.C.; Yuan, Y.; Wang, X.; Marini, J.C. Supplemental Citrulline Is More Efficient Than Arginine in Increasing Systemic Arginine Availability in Mice. J. Nutr. 2017, 147, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Su, Y.T.; Liu, T.Y.; Tsai, C.M.; Chang, C.H.; Yu, H.R. L-Arginine and L-Citrulline Supplementation Have Different Programming Effect on Regulatory T-Cells Function of Infantile Rats. Front. Immunol. 2018, 9, 2911. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Machida, M.; Kohara, A.; Omi, N.; Takemasa, T. Effects of citrulline supplementation on fatigue and exercise performance in mice. J. Nutr. Sci. Vitaminol. 2011, 57, 246–250. [Google Scholar] [CrossRef]
- Martínez-Sánchez, A.; Ramos-Campo, D.J.; Fernández-Lobato, B.; Rubio-Arias, J.A.; Alacid, F.; Aguayo, E. Biochemical, physiological, and performance response of a functional watermelon juice enriched in L-citrulline during a half-marathon race. Food Nutr. Res. 2017, 61, 1330098. [Google Scholar] [CrossRef]
- Glenn, J.M.; Gray, M.; Jensen, A.; Stone, M.S.; Vincenzo, J.L. Acute citrulline-malate supplementation improves maximal strength and anaerobic power in female, masters athletes tennis players. Eur. J. Sport Sci. 2016, 16, 1095–1103. [Google Scholar] [CrossRef]
- Pérez-Guisado, J.; Jakeman, P.M. Citrulline malate enhances athletic anaerobic performance and relieves muscle soreness. J. Strength Cond. Res. 2010, 24, 1215–1222. [Google Scholar] [CrossRef]
- Wax, B.; Kavazis, A.N.; Luckett, W. Effects of Supplemental Citrulline-Malate Ingestion on Blood Lactate, Cardiovascular Dynamics, and Resistance Exercise Performance in Trained Males. J. Diet. Suppl. 2016, 13, 269–282. [Google Scholar] [CrossRef]
- Wax, B.; Kavazis, A.N.; Weldon, K.; Sperlak, J. Effects of supplemental citrulline malate ingestion during repeated bouts of lower-body exercise in advanced weightlifters. J. Strength Cond. Res. 2015, 29, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.M.; Trexler, E.T. Effects of Citrulline Supplementation on Exercise Performance in Humans: A Review of the Current Literature. J. Strength Cond. Res. 2020, 34, 1480–1495. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Wong, A.; Jaime, S.J.; Gonzales, J.U. Influence of L-citrulline and watermelon supplementation on vascular function and exercise performance. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Bendahan, D.; Mattei, J.P.; Ghattas, B.; Confort-Gouny, S.; Le Guern, M.E.; Cozzone, P.J. Citrulline/malate promotes aerobic energy production in human exercising muscle. Br. J. Sports Med. 2002, 36, 282–289. [Google Scholar] [CrossRef]
- Trexler, E.T.; Persky, A.M.; Ryan, E.D.; Schwartz, T.A.; Stoner, L.; Smith-Ryan, A.E. Acute Effects of Citrulline Supplementation on High-Intensity Strength and Power Performance: A Systematic Review and Meta-Analysis. Sport Med. 2019, 49, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Rhim, H.C.; Kim, S.J.; Park, J.; Jang, K.M. Effect of citrulline on post-exercise rating of perceived exertion, muscle soreness, and blood lactate levels: A systematic review and meta-analysis. J. Sport Health Sci. 2020, 9, 553–561. [Google Scholar] [CrossRef]
- Viribay, A.; Burgos, J.; Fernández-Landa, J.; Seco-Calvo, J.; Mielgo-Ayuso, J. Effects of Arginine Supplementation on Athletic Performance Based on Energy Metabolism: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1300. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, D.; Krüger, M.; Wehland, M.; Infanger, M.; Grimm, D. The Effects of Oral L-Arginine and L-Citrulline Supplementation on Blood Pressure. Nutrients 2019, 11, 1679. [Google Scholar] [CrossRef]
- McNeal, C.J.; Meininger, C.J.; Reddy, D.; Wilborn, C.D.; Wu, G. Safety and Effectiveness of Arginine in Adults. J. Nutr. 2016, 146, S2587–S2593. [Google Scholar] [CrossRef]
- Ástvaldsdóttir, Á.; Naimi-Akbar, A.; Davidson, T.; Brolund, A.; Lintamo, L.; Granath, A.A.; Tranæus, S.; Östlund, P. Arginine and Caries Prevention: A Systematic Review. Caries Res. 2016, 50, 383–393. [Google Scholar] [CrossRef]
- Melik, Z.; Zaletel, P.; Virtic, T.; Cankar, K. L-Arginine as dietary supplement for improving microvascular function. Clin. Hemorheol. Microcirc. 2017, 65, 205–217. [Google Scholar] [CrossRef]
- Zarezadeh, M.; Emami, M.R.; Kord-Varkane, H.; Mousavi, S.M.; Alizadeh, H.; Asbaghi, O.; Olang, B.; Khorshidi, M. The effect of oral L-arginine supplementation on asymmetric dimethylarginine levels: A systematic review and meta-analysis of randomized clinical trials. Adv. Integr. Med. 2020, 7, 61–66. [Google Scholar] [CrossRef]
- Siani, A.; Pagano, E.; Iacone, R.; Iacoviello, L.; Scopacasa, F.; Strazzullo, P. Blood pressure and metabolic changes during dietary L-arginine supplementation in humans. Am. J. Hypertens. 2000, 13, 547–551. [Google Scholar] [CrossRef]
- Ast, J.; Jablecka, A.; Bogdanski, P.; Smolarek, I.; Krauss, H.; Chmara, E. Evaluation of the antihypertensive effect of L-arginine supplementation in patients with mild hypertension assessed with ambulatory blood pressure monitoring. Med. Sci. Monit. 2010, 16, CR266–CR271. [Google Scholar] [CrossRef] [PubMed]
- Rytlewski, K.; Olszanecki, R.; Korbut, R.; Zdebski, Z. Effects of prolonged oral supplementation with l-arginine on blood pressure and nitric oxide synthesis in preeclampsia. Eur. J. Clin. Investig. 2005, 35, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.Y.; Qin, L.Q.; Zhang, Z.; Zhao, Y.; Wang, J.; Arigoni, F.; Zhang, W. Effect of oral L-arginine supplementation on blood pressure: A meta-analysis of randomized, double-blind, placebo-controlled trials. Am. Heart J. 2011, 162, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Neri, I.; Monari, F.; Sgarbi, L.; Berardi, A.; Masellis, G.; Facchinetti, F. L-arginine supplementation in women with chronic hypertension: Impact on blood pressure and maternal and neonatal complications. J. Matern. Neonatal Med. 2010, 23, 1456–1460. [Google Scholar] [CrossRef] [PubMed]
- Chin-Dusting, J.P.; Alexander, C.T.; Arnold, P.J.; Hodgson, W.C.; Lux, A.S.; Jennings, G.L. Effects of in vivo and in vitro L-arginine supplementation on healthy human vessels. J. Cardiovasc. Pharmacol. 1996, 28, 158–166. [Google Scholar] [CrossRef]
- Moinard, C.; Nicolis, I.; Neveux, N.; Darquy, S.; Bénazeth, S.; Cynober, L. Dose-ranging effects of citrulline administration on plasma amino acids and hormonal patterns in healthy subjects: The Citrudose pharmacokinetic study. Br. J. Nutr. 2008, 99, 855–862. [Google Scholar] [CrossRef]
- Schwedhelm, E.; Maas, R.; Freese, R.; Jung, D.; Lukacs, Z.; Jambrecina, A.; Spickler, W.; Schulze, F.; Böger, R.H. Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: Impact on nitric oxide metabolism. Br. J. Clin. Pharmacol. 2008, 65, 51–59. [Google Scholar] [CrossRef]
- Kim, I.Y.; Schutzler, S.E.; Schrader, A.; Spencer, H.J.; Azhar, G.; Deutz, N.E.; Wolfe, R.R. Acute ingestion of citrulline stimulates nitric oxide synthesis but does not increase blood flow in healthy young and older adults with heart failure. Am. J. Physiol. Endocrinol. Metab. 2015, 309, E915–E924. [Google Scholar] [CrossRef]
- Bailey, S.J.; Blackwell, J.R.; Williams, E.; Vanhatalo, A.; Wylie, L.J.; Winyard, P.G.; Jones, A.M. Two weeks of watermelon juice supplementation improves nitric oxide bioavailability but not endurance exercise performance in humans. Nitric Oxide 2016, 59, 10–20. [Google Scholar] [CrossRef]
- Le Roux-Mallouf, T.; Vibert, F.; Doutreleau, S.; Verges, S. Effect of acute nitrate and citrulline supplementation on muscle microvascular response to ischemia-reperfusion in healthy humans. Appl. Physiol. Nutr. Metab. 2017, 42, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.J.; Blackwell, J.R.; Lord, T.; Vanhatalo, A.; Winyard, P.G.; Jones, A.M. l-Citrulline supplementation improves O2 uptake kinetics and high-intensity exercise performance in humans. J. Appl. Physiol. 2015, 119, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sánchez, A.; Alacid, F.; Rubio-Arias, J.A.; Fernández-Lobato, B.; Ramos-Campo, D.J.; Aguayo, E. Consumption of Watermelon Juice Enriched in l-Citrulline and Pomegranate Ellagitannins Enhanced Metabolism during Physical Exercise. J. Agric. Food Chem. 2017, 65, 4395–4404. [Google Scholar] [CrossRef] [PubMed]
- Shabeeh, H.; Seddon, M.; Brett, S.; Melikian, N.; Casadei, B.; Shah, A.M.; Chowienczyk, P. Sympathetic activation increases NO release from eNOS but neither eNOS nor nNOS play an essential role in exercise hyperemia in the human forearm. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, H1225–H1230. [Google Scholar] [CrossRef]
- Allerton, T.D.; Proctor, D.N.; Stephens, J.M.; Dugas, T.R.; Spielmann, G.; Irving, B.A. l-Citrulline Supplementation: Impact on Cardiometabolic Health. Nutrients 2018, 10, 921. [Google Scholar] [CrossRef]
- Collins, J.K.; Wu, G.; Perkins-Veazie, P.; Spears, K.; Claypool, P.L.; Baker, R.A.; Clevidence, B.A. Watermelon consumption increases plasma arginine concentrations in adults. Nutrition 2007, 23, 261–266. [Google Scholar] [CrossRef]
- Tarazona-Díaz, M.P.; Martínez-Sánchez, A.; Aguayo, E. Preservation of bioactive compounds and quality parameters of watermelon juice enriched with L-Citrulline through short thermal treatment. J. Food Qual. 2017, 2017, 3283054. [Google Scholar] [CrossRef]
- Thoonen, R.; Sips, P.Y.; Bloch, K.D.; Buys, E.S. Pathophysiology of hypertension in the absence of nitric oxide/cyclic GMP signaling. Curr. Hypertens. Rep. 2013, 15, 47–58. [Google Scholar] [CrossRef]
- Figueroa, A.; Sanchez-Gonzalez, M.A.; Wong, A.; Arjmandi, B.H. Watermelon extract supplementation reduces ankle blood pressure and carotid augmentation index in obese adults with prehypertension or hypertension. Am. J. Hypertens. 2012, 25, 640–643. [Google Scholar] [CrossRef]
- Ochiai, M.; Hayashi, T.; Morita, M.; Ina, K.; Maeda, M.; Watanabe, F.; Morishita, K. Short-term effects of L-citrulline supplementation on arterial stiffness in middle-aged men. Int. J. Cardiol. 2012, 155, 257–261. [Google Scholar] [CrossRef]
- Sanchez-Gonzalez, M.A.; Koutnik, A.P.; Ramirez, K.; Wong, A.; Figueroa, A. The effects of short term L-citrulline supplementation on wave reflection responses to cold exposure with concurrent isometric exercise. Am. J. Hypertens. 2013, 26, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Wong, A.; Hooshmand, S.; Sanchez-Gonzalez, M.A. Effects of watermelon supplementation on arterial stiffness and wave reflection amplitude in postmenopausal women. Menopause 2013, 20, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Sanchez-Gonzalez, M.A.; Perkins-Veazie, P.M.; Arjmandi, B.H. Effects of watermelon supplementation on aortic blood pressure and wave reflection in individuals with prehypertension: A pilot study. Am. J. Hypertens. 2011, 24, 40–44. [Google Scholar] [CrossRef]
- Massa, N.M.; Silva, A.S.; Toscano, L.T.; Silva, J.D.; Persuhn, D.C.; Gonçalves, M.D.C.R. Watermelon extract reduces blood pressure but does not change sympathovagal balance in prehypertensive and hypertensive subjects. Blood Press 2016, 25, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Orozco-Gutiérrez, J.J.; Castillo-Martínez, L.; Orea-Tejeda, A.; Vázquez-Díaz, O.; Valdespino-Trejo, A.; Narváez-David, R.; Keirns-Davis, C.; Carrasco-Ortiz, O.; Navarro-Navarro, A.; Sánchez-Santillán, R. Effect of L-arginine or L-citrulline oral supplementation on blood pressure and right ventricular function in heart failure patients with preserved ejection fraction. Cardiol. J. 2010, 17, 612–618. [Google Scholar]
- Wong, A.; Alvarez-Alvarado, S.; Jaime, S.J.; Kinsey, A.W.; Spicer, M.T.; Madzima, T.A.; Figueroa, A. Combined whole-body vibration training and l-citrulline supplementation improves pressure wave reflection in obese postmenopausal women. Appl. Physiol. Nutr. Metab. 2016, 41, 292–297. [Google Scholar] [CrossRef]
- Figueroa, A.; Alvarez-Alvarado, S.; Jaime, S.J.; Kalfon, R. l-Citrulline supplementation attenuates blood pressure, wave reflection and arterial stiffness responses to metaboreflex and cold stress in overweight men. Br. J. Nutr. 2016, 116, 279–285. [Google Scholar] [CrossRef]
- Figueroa, A.; Trivino, J.A.; Sanchez-Gonzalez, M.A.; Vicil, F. Oral L-citrulline supplementation attenuates blood pressure response to cold pressor test in young men. Am. J. Hypertens. 2010, 23, 12–16. [Google Scholar] [CrossRef]
- Pahlavani, N.; Entezari, M.H.; Nasiri, M.; Miri, A.; Rezaie, M.; Bagheri-Bidakhavidi, M.; Sadeghi, O. The effect of l-arginine supplementation on body composition and performance in male athletes: A double-blinded randomized clinical trial. Eur. J. Clin. Nutr. 2017, 71, 544–548. [Google Scholar] [CrossRef]
- Kang, Y.; Dillon, K.N.; Martinez, M.A.; Maharaj, A.; Fischer, S.M.; Figueroa, A. Combined L-Citrulline Supplementation and Slow Velocity Low-Intensity Resistance Training Improves Leg Endothelial Function, Lean Mass, and Strength in Hypertensive Postmenopausal Women. Nutrients 2022, 15, 74. [Google Scholar] [CrossRef]
- Churchward-Venne, T.A.; Cotie, L.M.; MacDonald, M.J.; Mitchell, C.J.; Prior, T.; Baker, S.K.; Phillips, S.M. Citrulline does not enhance blood flow, microvascular circulation, or myofibrillar protein synthesis in elderly men at rest or following exercise. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E71–E83. [Google Scholar] [CrossRef] [PubMed]
- Brandes, R.P.; Fleming, I.; Busse, R. Endothelial aging. Cardiovasc. Res. 2005, 66, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Gori, T.; Keaney, J.F., Jr.; Maack, C.; Daiber, A. Pathophysiological role of oxidative stress in systolic and diastolic heart failure and its therapeutic implications. Eur. Heart J. 2015, 36, 2555–2564. [Google Scholar] [CrossRef]
- Klawitter, J.; Hildreth, K.L.; Christians, U.; Kohrt, W.M.; Moreau, K.L. A relative L-arginine deficiency contributes to endothelial dysfunction across the stages of the menopausal transition. Physiol. Rep. 2017, 5, e13409. [Google Scholar] [CrossRef]
- Wijnands, K.A.; Meesters, D.M.; van Barneveld, K.W.; Visschers, R.G.; Briedé, J.J.; Vandendriessche, B.; van Eijk, H.M.; Bessems, B.A.; van den Hoven, N.; von Wintersdorff, C.J.; et al. Citrulline Supplementation Improves Organ Perfusion and Arginine Availability under Conditions with Enhanced Arginase Activity. Nutrients 2015, 7, 5217–5238. [Google Scholar] [CrossRef] [PubMed]
- Cynober, L. Pharmacokinetics of arginine and related amino acids. J. Nutr. 2007, 137, S1646–S1649. [Google Scholar] [CrossRef]
- Hecker, M.; Sessa, W.C.; Harris, H.J.; Anggård, E.E.; Vane, J.R. The metabolism of L-arginine and its significance for the biosynthesis of endothelium-derived relaxing factor: Cultured endothelial cells recycle L-citrulline to L-arginine. Proc. Natl. Acad. Sci. USA 1990, 87, 8612–8616. [Google Scholar] [CrossRef]
- Morita, M.; Sakurada, M.; Watanabe, F.; Yamasaki, T.; Doi, H.; Ezaki, H.; Morishita, K.; Miyakex, T. Effects of Oral L-Citrulline Supplementation on Lipoprotein Oxidation and Endothelial Dysfunction in Humans with Vasospastic Angina. Immunol. Endocr. Metab. Agents Med. Chem. 2013, 13, 214–220. [Google Scholar] [CrossRef]
- Bai, Y.; Sun, L.; Yang, T.; Sun, K.; Chen, J.; Hui, R. Increase in fasting vascular endothelial function after short-term oral L-arginine is effective when baseline flow-mediated dilation is low: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2009, 89, 77–84. [Google Scholar] [CrossRef]
- Gates, P.E.; Boucher, M.L.; Silver, A.E.; Monahan, K.D.; Seals, D.R. Impaired flow-mediated dilation with age is not explained by L-arginine bioavailability or endothelial asymmetric dimethylarginine protein expression. J. Appl. Physiol. 2007, 102, 63–71. [Google Scholar] [CrossRef]
- Baker, P.R., II; Boyle, K.E.; Koves, T.R.; Ilkayeva, O.R.; Muoio, D.M.; Houmard, J.A.; Friedman, J.E. Metabolomic analysis reveals altered skeletal muscle amino acid and fatty acid handling in obese humans. Obesity 2015, 23, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Donato, A.J.; Eskurza, I.; Silver, A.E.; Levy, A.S.; Pierce, G.L.; Gates, P.E.; Seals, D.R. Direct evidence of endothelial oxidative stress with aging in humans: Relation to impaired endothelium-dependent dilation and upregulation of nuclear factor-kappaB. Circ. Res. 2007, 100, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Inflammation and cardiovascular disease mechanisms. Am. J. Clin. Nutr. 2006, 83, 456S–460S. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mañas, L.; El-Assar, M.; Vallejo, S.; López-Dóriga, P.; Solís, J.; Petidier, R.; Montes, M.; Nevado, J.; Castro, M.; Gómez-Guerrero, C.; et al. Endothelial dysfunction in aged humans is related with oxidative stress and vascular inflammation. Aging Cell 2009, 8, 226–238. [Google Scholar] [CrossRef]
- Forbes, S.C.; Harber, V.; Bell, G.J. The acute effects of L-arginine on hormonal and metabolic responses during submaximal exercise in trained cyclists. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 369–377. [Google Scholar] [CrossRef]
- Meirelles, C.M.; Matsuura, C. Acute supplementation of L-arginine affects neither strength performance nor nitric oxide production. J. Sport Med. Phys. Fit. 2018, 58, 216–220. [Google Scholar] [CrossRef]
- Vanhatalo, A.; Bailey, S.J.; DiMenna, F.J.; Blackwell, J.R.; Wallis, G.A.; Jones, A.M. No effect of acute L-arginine supplementation on O2 cost or exercise tolerance. Eur. J. Appl. Physiol. 2013, 113, 1805–1819. [Google Scholar] [CrossRef]
- Alvares, T.S.; Conte-Junior, C.A.; Silva, J.T.; Paschoalin, V.M. Acute L-Arginine supplementation does not increase nitric oxide production in healthy subjects. Nutr. Metab. 2012, 9, 54. [Google Scholar] [CrossRef]
- Blum, A.; Hathaway, L.; Mincemoyer, R.; Schenke, W.H.; Kirby, M.; Csako, G.; Waclawiw, M.A.; Panza, J.A.; Cannon, R.O., 3rd. Effects of oral L-arginine on endothelium-dependent vasodilation and markers of inflammation in healthy postmenopausal women. J. Am. Coll. Cardiol. 2000, 35, 271–276. [Google Scholar] [CrossRef]
- Tang, J.E.; Lysecki, P.J.; Manolakos, J.J.; MacDonald, M.J.; Tarnopolsky, M.A.; Phillips, S.M. Bolus arginine supplementation affects neither muscle blood flow nor muscle protein synthesis in young men at rest or after resistance exercise. J. Nutr. 2011, 141, 195–200. [Google Scholar] [CrossRef]
- Forbes, S.C.; Bell, G.J. The acute effects of a low and high dose of oral L-arginine supplementation in young active males at rest. Appl. Physiol. Nutr. Metab. 2011, 36, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Maiorana, A.; O’Driscoll, G.; Taylor, R.; Green, D. Exercise and the nitric oxide vasodilator system. Sports Med. 2003, 33, 1013–1035. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Brosnan, J.T.; Brosnan, M.E. Catabolism of arginine and ornithine in the perfused rat liver: Effect of dietary protein and of glucagon. Am. J. Physiol. Endocrinol. Metab. 2000, 278, E516–E521. [Google Scholar] [CrossRef] [PubMed]
- Koifman, B.; Wollman, Y.; Bogomolny, N.; Chernichowsky, T.; Finkelstein, A.; Peer, G.; Scherez, J.; Blum, M.; Laniado, S.; Iaina, A.; et al. Improvement of cardiac performance by intravenous infusion of L-arginine in patients with moderate congestive heart failure. J. Am. Coll. Cardiol. 1995, 26, 1251–1256. [Google Scholar] [CrossRef]
- Yavuz, H.U.; Turnagol, H.; Demirel, A.H. Pre-exercise arginine supplementation increases time to exhaustion in elite male wrestlers. Biol. Sport 2014, 31, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, M.; Brunner, F.; Faulhaber, M.; Hotter, B.; Likar, R. The prolonged intake of L-arginine-L-aspartate reduces blood lactate accumulation and oxygen consumption during submaximal exercise. J. Sport Sci. Med. 2005, 4, 314–322. [Google Scholar]
- Chang, C.K.; Chien, K.M.C.; Chang, J.H.; Huang, M.H.; Liang, Y.C.; Liu, T.H. Branched-chain amino acids and arginine improve performance in two consecutive days of simulated handball games in male and female athletes: A randomized trial. PLoS ONE 2015, 10, e0121866. [Google Scholar] [CrossRef]
- Abel, T.; Knechtle, B.; Perret, C.; Eser, P.; von Arx, P.; Knecht, H. Influence of chronic supplementation of arginine aspartate in endurance athletes on performance and substrate metabolism—A randomized, double-blind, placebo-controlled study. Int. J. Sport Med. 2005, 26, 344–349. [Google Scholar] [CrossRef]
- Kaore, S.N.; Amane, H.S.; Kaore, N.M. Citrulline: Pharmacological perspectives and its role as an emerging biomarker in future. Fundam. Clin. Pharmacol. 2013, 27, 35–50. [Google Scholar] [CrossRef]
- Hwang, P.; Marroquín, F.E.M.; Gann, J.; Andre, T.; McKinley-Barnard, S.; Kim, C.; Morita, M.; Willoughby, D.S. Eight weeks of resistance training in conjunction with glutathione and L-Citrulline supplementation increases lean mass and has no adverse effects on blood clinical safety markers in resistance-trained males. J. Int. Soc. Sport Nutr. 2018, 15, 30. [Google Scholar] [CrossRef]
- Barkhidarian, B.; Khorshidi, M.; Shab-Bidar, S.; Hashemi, B. Effects of L-citrulline supplementation on blood pressure: A systematic review and meta-analysis. Avicenna J. Phytomed. 2019, 9, 10–20. [Google Scholar] [PubMed]
- Terasawa, N.; Nakada, K. Effect of l-citrulline intake on intermittent short-time high-intensity exercise performance in male collegiate track athletes. J. Phys. Fit. Sport Med. 2019, 8, 147–157. [Google Scholar] [CrossRef]
- Suzuki, T.; Morita, M.; Kobayashi, Y.; Kamimura, A. Oral L-citrulline supplementation enhances cycling time trial performance in healthy trained men: Double-blind randomized placebo-controlled 2-way crossover study. J. Int. Soc. Sport Nutr. 2016, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Esen, O.; Eser, M.C.; Abdioglu, M.; Benesova, D.; Gabrys, T.; Karayigit, R. Eight Days of L-Citrulline or L-Arginine Supplementation Did Not Improve 200-m and 100-m Swimming Time Trials. Int. J. Environ. Res. Public Health 2022, 19, 4462. [Google Scholar] [CrossRef] [PubMed]
- Hickner, R.C.; Tanner, C.J.; Evans, C.A.; Clark, P.D.; Haddock, A.; Fortune, C.; Geddis, H.; Waugh, W.; McCammon, M. L-citrulline reduces time to exhaustion and insulin response to a graded exercise test. Med. Sci. Sport Exerc. 2006, 38, 660–666. [Google Scholar] [CrossRef]
- Cutrufello, P.T.; Gadomski, S.J.; Zavorsky, G.S. The effect of l-citrulline and watermelon juice supplementation on anaerobic and aerobic exercise performance. J. Sport Sci. 2015, 33, 1459–1466. [Google Scholar] [CrossRef]
- Stanelle, S.T.; McLaughlin, K.L.; Crouse, S.F. One Week of L-Citrulline Supplementation Improves Performance in Trained Cyclists. J. Strength Cond. Res. 2020, 34, 647–652. [Google Scholar] [CrossRef]
- Forbes, S.C.; Harber, V.; Bell, G.J. Oral L-arginine before resistance exercise blunts growth hormone in strength trained males. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 236–244. [Google Scholar] [CrossRef]
- Glenn, J.M.; Gray, M.; Wethington, L.N.; Stone, M.S.; Stewart, R.W., Jr.; Moyen, N.E. Acute citrulline malate supplementation improves upper- and lower-body submaximal weightlifting exercise performance in resistance-trained females. Eur. J. Nutr. 2017, 56, 775–784. [Google Scholar] [CrossRef]
- Gonzalez, A.M.; Spitz, R.W.; Ghigiarelli, J.J.; Sell, K.M.; Mangine, G.T. Acute Effect of Citrulline Malate Supplementation on Upper-Body Resistance Exercise Performance in Recreationally Resistance-Trained Men. J. Strength Cond. Res. 2018, 32, 3088–3094. [Google Scholar] [CrossRef]
- da Silva, D.K.; Jacinto, J.L.; de Andrade, W.B.; Roveratti, M.C.; Estoche, J.M.; Balvedi, M.C.W.; de Oliveira, D.B.; da Silva, R.A.; Aguiar, A.F. Citrulline Malate Does Not Improve Muscle Recovery after Resistance Exercise in Untrained Young Adult Men. Nutrients 2017, 9, 1132. [Google Scholar] [CrossRef]
- Trexler, E.T.; Keith, D.S.; Schwartz, T.A.; Ryan, E.D.; Stoner, L.; Persky, A.M.; Smith-Ryan, A.E. Effects of Citrulline Malate and Beetroot Juice Supplementation on Blood Flow, Energy Metabolism, and Performance During Maximum Effort Leg Extension Exercise. J. Strength Cond. Res. 2019, 33, 2321–2329. [Google Scholar] [CrossRef] [PubMed]
- Streeter, D.M.; Trautman, K.A.; Bennett, T.W.; McIntosh, L.E.; Grier, J.W.; Stastny, S.N.; Hackney, K.J. Endothelial, Cardiovascular, and Performance Responses to L-Arginine Intake and Resistance Exercise. Int. J. Exerc. Sci. 2019, 12, 701–713. [Google Scholar]
- Chappell, A.J.; Allwood, D.M.; Johns, R.; Brown, S.; Sultana, K.; Anand, A.; Simper, T. Citrulline malate supplementation does not improve German Volume Training performance or reduce muscle soreness in moderately trained males and females. J. Int. Soc. Sport Nutr. 2018, 15, 42. [Google Scholar] [CrossRef]
- Farney, T.M.; Bliss, M.V.; Hearon, C.M.; Salazar, D.A. The Effect of Citrulline Malate Supplementation on Muscle Fatigue Among Healthy Participants. J. Strength Cond. Res. 2019, 33, 2464–2470. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Gouspillou, G.; Carvalho, L.P.; Marcangeli, V.; El Hajj Boutros, G.; Dulac, M.; Noirez, P.; Morais, J.A.; Gaudreau, P.; Aubertin-Leheudre, M. Effect of High-Intensity Interval Training Combined with L-Citrulline Supplementation on Functional Capacities and Muscle Function in Dynapenic-Obese Older Adults. J. Clin. Med. 2018, 7, 561. [Google Scholar] [CrossRef] [PubMed]
- Kanaley, J.A. Growth hormone, arginine and exercise. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 50–54. [Google Scholar] [CrossRef]
- Manini, T.M.; Yarrow, J.F.; Buford, T.W.; Clark, B.C.; Conover, C.F.; Borst, S.E. Growth hormone responses to acute resistance exercise with vascular restriction in young and old men. Growth Horm. IGF Res. 2012, 22, 167–172. [Google Scholar] [CrossRef]
- Ghigo, E.; Arvat, E.; Valente, F.; Nicolosi, M.; Boffano, G.M.; Procopio, M.; Bellone, J.; Maccario, M.; Mazza, E.; Camanni, F. Arginine reinstates the somatotrope responsiveness to intermittent growth hormone-releasing hormone administration in normal adults. Neuroendocrinology 1991, 54, 291–294. [Google Scholar] [CrossRef]
- Zajac, A.; Poprzecki, S.; Zebrowska, A.; Chalimoniuk, M.; Langfort, J. Arginine and ornithine supplementation increases growth hormone and insulin-like growth factor-1 serum levels after heavy-resistance exercise in strength-trained athletes. J. Strength Cond. Res. 2010, 24, 1082–1090. [Google Scholar] [CrossRef]
- Chromiak, J.A.; Antonio, J. Use of amino acids as growth hormone-releasing agents by athletes. Nutrition 2002, 18, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Lambert, M.I.; Hefer, J.A.; Millar, R.P.; Macfarlane, P.W. Failure of commercial oral amino acid supplements to increase serum growth hormone concentrations in male body-builders. Int. J. Sport Nutr. 1993, 3, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Wax, B.; Kavazis, A.N.; Webb, H.E.; Brown, S.P. Acute L-arginine alpha ketoglutarate supplementation fails to improve muscular performance in resistance trained and untrained men. J. Int. Soc. Sport Nutr. 2012, 9, 17. [Google Scholar] [CrossRef]
- Hurst, H.T.; Sinclair, J.K.; Beenham, M. Influence of Absolute versus relative L-arginine Dosage on 1 km and 16.1 km time trial performance in trained cyclists. J. Sci. Cycl. (JSC) 2014, 3, 2–8. [Google Scholar]
- Greer, B.K.; Jones, B.T. Acute arginine supplementation fails to improve muscle endurance or affect blood pressure responses to resistance training. J. Strength Cond. Res. 2011, 25, 1789–1794. [Google Scholar] [CrossRef] [PubMed]
- Gough, L.A.; Sparks, S.A.; McNaughton, L.R.; Higgins, M.F.; Newbury, J.W.; Trexler, E.; Faghy, M.A.; Bridge, C.A. A critical review of citrulline malate supplementation and exercise performance. Eur. J. Appl. Physiol. 2021, 121, 3283–3295. [Google Scholar] [CrossRef] [PubMed]
- Chappell, A.J.; Allwood, D.M.; Simper, T.N. Citrulline Malate Fails to Improve German Volume Training Performance in Healthy Young Men and Women. J. Diet. Suppl. 2020, 17, 249–260. [Google Scholar] [CrossRef]
- Wegierska, A.E.; Charitos, I.A.; Topi, S.; Potenza, M.A.; Montagnani, M.; Santacroce, L. The Connection Between Physical Exercise and Gut Microbiota: Implications for Competitive Sports Athletes. Sports Med. 2022, 52, 2355–2369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Participants | BP Status | Formulation | Dose | Duration | Results |
| Pahlavani et al. (2017) [92] | 52 healthy males (Arg: 21.32 ± 4.59 y pla: 20.40 ± 4.04 y) | Normotensive | L-Arginine | 2 g/day | 45 days | FBS, TG, LDL, Cholesterol ↓ HDL ↑ SBP, DBP ↔ |
| Suzuki et al. (2019) [42] | 24 male soccer players (19.0 ± 0.2 y) | Normotensive | Arg + Cit | both 1.2 g/day each | 6 days | Plasma post-exercise NOx, Cit, Arg ↑ Perception of physical exertion ↑ |
| Figueroa et al. (2010) [91] | 17 healthy young males (22 ± 1 y) | Normotensive | L-Citrulline | 6 g/day | 4 weeks | bSBP, aSBP, aPP ↓ |
| Figueroa et al. (2016) [90] | 16 overweight/obese healthy males (24 ± 2 y) | Normotensive | L-Citrulline | 6 g/day | 2 weeks | aSBP, aPP, AIx during IHG ↓ aDBP, MAP, AIx during PEMI ↓ aSBP, DBP, aPP, an baPWV during PEMI + CPT ↓ (resting) Attenuated the increase in aSBP and AIx during IHG and reduced MAP aDBP |
| Figueroa et al. (2013) [85] | 12 postmenopausal women (57 ± 1 y) | Hypertensive | Watermelon Extract | 6 g/day | 6 weeks | (Resting) baPWV, aSBP, aDBP, aSBP2 ↓ (Resting) Alx ↔ |
| Figueroa et al. (2011) [86] | 9 middle-aged adults (4 M, 5 F) (54 ± 3 y) | Pre-hypertensive | Watermelon Extract | 2.7 g/day | 6 weeks | (Resting) bPP, aSBP, aPP, Alx ↓ |
| Figueroa et al. (2012) [82] | 14 middle-aged adults (3 M, 11 F) (58 ± 1 y) | Pre-hypertensive | Watermelon Extract | 2.7 g/day | 6 weeks | (Resting) ankle SBP, DBP, MAP ↓ (Resting) bSBP, bDBP, bMAP ↓ (Resting) carotid Alx ↓ |
| Massa et al. (2016) [87] | 40 prehypertensive and hypertensive (21 M, 19 F) (Cit: 48.7 ± 1, Pla: 47.4 ± 1) | Pre-hypertensive | Watermelon Extract | 6 g/day | 6 weeks | (Resting) bSBP and bDBP ↓ (Resting) cardiac autonomic function ↔ |
| Maharaj et al. (2022) [16] | 25 postmenopausal women (14 Cit, 11 Pla) (Cit: 61 ± 6 y, Pla: 64 ± 6 y) | Hypertensive | L-Citrulline | 10 g/day | 4 weeks | Serum L-ARG levels and brachial artery FMD ↑ (Resting) aortic DBP and MAP ↓ |
| Kang et al. (2023) [93] | 24 postmenopausal women (13 Cit, 11 Pla) (Cit: 62 ± 2 y, Pla: 63 ± 1 y) | Hypertensive | L-Citrulline | 10 g/day | 4 weeks | Superficial femoral artery FMD ↑ |
| Study | Participants | Exercise | Exercise Protocol | BP Status | Supplement Timing | Formulation | Dose | Duration | Results |
| Bailey et al. (2010) [32] | 9 healthy males (26.0 ± 6.0 y) | aerobic exercise (cycle MIE, HIE) | MIE intensity: 80% GET HIE intensity: (power output at the VO2peak—power output at the GET) × 70% + power output at the GET Supplement 1 day: 2 × 6 min MIE, supplement 2 day: 1 × 6 min MIE + 1 × 6 min HIE, supplement 3 day: 1 × 6 min MIE + HIE until no longer able to perform the exercise | Normotensive | 1 h before exercise | L-Arginine | 6 g | Cross-over acute | Plasma NO2 ↑, SBP ↓ (MIE) VO2 ↑ (HIE) VO2 slow component amplitude ↓, Extended the time to exhaustion |
| Bailey et al. (2015) [75] | 10 healthy adult males (19.0 ± 1.0 y) | aerobic exercise (cycle MIE, HIE) | During the first laboratory visit, subjects completed a ramp incremental cycle test on an electronically braking cycle ergometer (Lode Excalibur Sport, Groningen, The Netherlands). Initially, subjects performed 3 min of baseline cycling at 0 W; then the work rate was increased by 30 W/min until the limit of tolerance. Subjects rode their bikes at their own pace (70–90 rpm). | Normotensive | 60 min before exercise | L-Arginine L-Citrulline | Arg 6 g/day or Cit 6 g/day | Cross-over 7 days | (Cit) BP ↓, VO2 kinetic, endurance exercise performance ↑ |
| Bailey et al. (2016) [73] | 8 healthy, recreationally active males (22 ± 2 y) | - | 3 min of baseline cycling at 20 W. A passive recovery of 5 min separated the transitions. The moderate-intensity steps were each of 4 min. First visit and on day 14 of the period, they cycled at a severe-intensity constant-work-rate (70% Δ) until exhaustion. On day 16 of the period, subjects cycled for 6 min at a severe-intensity constant-work-rate (70% Δ) followed immediately by a 30 s all-out effort. The resistance on the pedals was set using the linear mode of the Lode ergometer so that the subjects would attain the power output calculated to be 50% Δ if they attained their preferred cadence. | Normotensive | 75 min before test | Watermelon juice | ~3.4 g/day | 2 weeks | (resting) aSBP and MAP ↑ |
| Vanhatalo et al. (2013) [110] | 18 males recreationally active (22 ± 3 y) | aerobic exercise (treadmill) | Ramp incremental running tests on a motorized treadmill | Normotensive | 95 min before exercise protocol | L-Arginine | 6 g | Acute | NOx and O2 cost of exercise or exercise tolerance ↔ |
| Bailey et al. (2015) [75] | 10 males recreationally active (19 ± 1 y) | aerobic exercise | Cycle ergometer; 3 “step” exercise tests: 2 moderate-intensity step tests followed by 1 severe-intensity exercise bout. Moderate-intensity step tests were completed to assess VO2 economy in the absence of a VO2 kinetics and cycling intensity step tests were completed to assess VO2 presence of a VO2 slow component | Normotensive | 90 min before exercise protocol | L-Citrulline or L-Arginine | Cit 6 g/day Arg 6 g/day | 7 days | L-Arg for both L-Arg and L-Cit ↑, Nitrite for L-Arg ↑, Mean arterial pressure ↓, Tolerance during severe exercise ↑, Lowered the VO2 mean response time ↓, Total amount of work completed in the exercise performance test with L-Cit supple but not with L-Arg ↑ |
| Bailey et al. (2016) [73] | 8 males recreationally active (22 ± 2 y) | aerobic exercise | ‘Step’ exercise tests including one moderate-intensity step test followed by one high-intensity exercise bout | Normotensive | 75 min before exercise protocol | Watermelon juice | 300 mL/day (provided ~3.4 g/day L-Cit) | L-Arg, L-Cit, nitrite, skeletal muscle oxygenation index during moderate-intensity exercise ↑, Resting blood pressure ↑ Time-to-exhaustion during severe-intensity exercise ↔ | |
| Pahlavani et al. (2017) [92] | 56 male soccer players (20.85 ± 4.29 y) | aerobic exercise (Harvard Step Test) | Harvard Step Test: repeated steps 30 times per 1 min using 50 cm platform, total of 5 min | Normotensive | evening | L-Arginine | 2 g/day | 45 days | VO2max ↑ BMI, BFM, LBM ↔ |
| Forbes et al. (2013) [108] | 15 male trained cyclists (28 ± 5 y) | aerobic exercise (cycle) | VO2max test on cycle ergometer—graded, incremental exercise to volitional exhaustion | Normotensive | 60 min before exercise protocol | L-Arginine | 0.075 g/kg | Acute | L-Arg ↑, NOx, GH, cardiorespiratory parameter measured ↔ |
| Yavuz et al. (2014) [118] | 9 male trained wrestlers (24.7 ± 3.8 y) | aerobic exercise (cycle) | Maximal incremental exercise on cycle ergometer starting at 60–70 rpm (increase by 30 watts at every 3 min) | Normotensive | 60 min before exercise | L-Arginine | 1.5 g/10kg | Acute | Time to exhaustion ↑, Lactate ↔ |
| Suzuki et al. (2019) [42] | 20 male soccer players (19.0 ± 0.2 y) | aerobic exercise | PWC 75% HRmax, three stages of load (25, 75 and 125 W) for 3 min each (total, 9 min) | Normotensive | 60 min before exercise protocol | L-Arginine and L-Citrulline | Arg 1.2 g and Cit 1.2 g/day | 7 days | Power output, L-Cit, L-Arg, NOx ↑, RPE ↓ |
| Pérez-Guisado and Jakeman (2010) [50] | 41 healthy males (29.8 ± 7.64 y) | anaerobic exercise | The pectoral workout protocol comprised 16 sets in the following order: 4 sets of flat barbell bench presses (80% 1RM weight for the flat bench press), 4 sets of incline barbell bench presses (80% 1RM weight for the flat bench press), 4 sets of incline flies (60% 1RM weight for the flat bench press), and 4 sets of flat barbell bench presses (80% 1RM weight for the flat bench press). The speed of each rep was 3-4 s Rest for 1 min between sets and for 2 min between each exercise. The training program was the same during the 2-week study period | Normotensive | 60 min before test | Citrulline malate | 8 g | Cross-over acute | The number of repetitions ↑ Muscle soreness ↓ |
| Mor et al. (2018) [43] | 28 male active football players (18–30 y) | anaerobic exercise (RAST) | Running anaerobic sprint test (RAST): 6 × 35 m sprints at 10 s rest | Normotensive | 3 g before training (1 g before breakfast and 2 g 30 min before training) and 3 g after training (2 g 1 h after training and 1 g before sleep) rest day 3 g (2 g before breakfast and 1 g before sleep) | L-Arginine | 6 g or 3 g | 14 days | BMI, recovery HR, AST, ALT, LDH ↓ anaerobic performance ↔ rapid reduction recovery LA |
| Terasawa and Nakada (2019) [125] | 9 male track athletes (20.9 ± 1.6 y) | anaerobic exercise | Wingate test, using cycle ergometer, was adopted as the intermittent short-time high intensity exercise | Normotensive | 60 min before exercise protocol | L-Citrulline | 3 g/day | 7 days | L-Cit group; ↓ RPE, ↔ Lactate, ↑ NOx, ↑ mean power output, ↑ pedaling speed, ↑ VO2 |
| Sanchez-Gonzalez et al. (2013) [84] | 16 young, healthy male adults (23 ± 3 y) | isometric handgrip (IHG) exercise | Normotensive | L-Citrulline | 100 mg/kg | 2 weeks | CI and IHG increases in bSBP, aSBP and Alx ↓ | ||
| Forbes et al. (2014) [131] | 14 males resistance trained (25 ± 4 y) | resistance exercise | Resistance exercise (3 sets of 8 exercises, 10 repetitions at ~75% 1RM) | Normotensive | 60 min before exercise protocol | L-Arginine | 0.075 g/kg | Acute | L-Arg ↑, GH ↓, RPE ↔ |
| Meirelles and Matsuura (2018) [109] | 12 males resistance trained (27 ± 3 y) | resistance exercise | Maximal dynamic strength in the bench press and knee extension (one-repetition maximum [1RM] test) | Normotensive | 60 min before exercise protocol | L-Arginine | 6 g | Acute | NOx, in strength exercises ↔ |
| Bendahan et al. (2002) [55] | 18 sedentary males symptomatic of fatigue (31 ± 9 y) | resistance exercise | Finger flexions performed at 1.5 s intervals lifting a 6 kg weight for 3 min Performed: 2 × before ingestion CM 3 × during ingestion CM 1 × after ingestion CM | Normotensive | Citrulline Malate | 6 g/day | 15 days | Power (w) ↑ Delta change in pH per unit of power ↓, Rate of oxidative ATP production (%EC) ↑, Rate of PCr resynthesis (mmol/min) ↑ | |
| Pérez-Guisado and Jakeman (2010) [50] | 41 resistance trained males (30 ±8 y) | resistance exercise | 4 sets at 80% 1RM until failure before and again after a pectoral training workout 1-min rest between sets, Barbell bench press | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Bench press total reps ↑, Total reps ↑ Muscle soreness following 24h, 48h ↓ |
| Wax et al. (2015) [52] | 12 resistance trained males (22 ±1 y) | resistance exercise | 5 sets at 60% 1RM until failure 3-min rest between sets, Leg press, hack squat, leg extension | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Leg press total reps ↑, Hack squat total reps ↑, Leg extension total reps ↑ Blood lactate, HR, SBP, DBP ↔ |
| Wax et al. (2016) [51] | 14 resistance trained males (23 ±2 y) | resistance exercise | 3 sets until failure 3-min rest between sets, Chin-up, Reverse chin-up, Push-up | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Chin-up total reps ↑, Reverse chin-up total reps ↑, Push-up total reps ↑ Blood lactate, HR, SBP ↔, DBP ↓ |
| Glenn et al. (2017) [132] | 15 resistance trained females (23± 3 y) | resistance exercise | 6 sets at 80% 1RM until failure 1-min rest between sets, Bench press, Leg press | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Bench press total reps ↑, Leg press total reps ↑ Bench press RPE ↓ Leg press RPE, bench press HR, leg press HR ↔ |
| Gonzalez et al. (2018) [133] | 12 recreational resistance trained males (21 ± 2 y) | resistance exercise | 5 sets × 15 reps at 75% 1RM 2-min rest between sets, Barbell bench press | Normotensive | 40 min before test | Citrulline Malate | 8 g | Acute | Total reps, peak power, mean power, fatigue index ↔ RPE, muscle thickness, subjective feelings of focus, energy, fatigue, and muscle pump ↔ |
| da Silva et al. (2017) [134] | 9 recreational active males (24 ± 3 y) | resistance exercise | 1 set at 100% of 10RM machine leg press machine hack squat | Normotensive | 1 h before test | Citrulline Malate | 6 g | Acute | Total no. Reps ↔ RPE, lactate, creatine kinase, muscle soreness, testosterone-cortisol, electromyography ↔ |
| Trexler et al. (2019) [135] | 27 recreationally active males (22 ± 4 y) | resistance exercise | Maximal concentric leg extensions 5 sets × 30 reps | Normotensive | 2 h before test | Citrulline Malate | 8 g | Acute | NOx, blood flow, metabolic efficiency, hormonal response ↔ |
| Hwang et al. (2018) [123] | 75 resistance trained males (21 ± 2 y) | resistance exercise | 1RM testing: free weight bench press angled leg press performed at baseline, 4, and 8 weeks of training | Normotensive | Citrulline Malate | 2 g/day | 8 weeks | Bench press 4 weeks, 8 weeks ↔, Angled leg press 4 weeks, 8 weeks ↔ Body mass, fat mass, body water ↔, Lean mass ↑ at week 4 | |
| Stanelle et al. (2020) [130] | 10 male cyclists (24 ± 3 y) | compound | Simulated 40-km TT on a cycle ergometer, and supramaximal sprint repeat task (six 1-min sprints at 120% of maximal power) | Normotensive | 120 min before exercise protocol | L-Citrulline | 6 g/day | 7 days | TT time ↔, average power output, HR and RPE ↑ |
| Glenn et al. (2017) [132] | 15 females (23.0 ± 3.0 y) | resistance exercise | 1RM measurement (plate-loaded, flat barbell bench press and a plate-loaded, leg press) | Normotensive | 60 min before exercise | Citrulline Malate | 8 g | Acute | Upper-body repetitions, lower-body total repetitions ↑ upper-body RPE ↓, HR ↔ |
| Esen et al. (2022) [127] | 15 trained/developmental (5 females) swimmers and triathletes (25.0 ± 7.0 y) | 200 m and 100 m freestyle swimming | Swimming Time Trials protocol (200 m and 100 m). 10 min after the warm-up, participants completed a 200 m freestyle TT. The participants recovered in a seated position for 30 min and were only allowed to drink water, which was recorded and precisely replicated on the 2nd trial. After 30 min recovery, a 100 m TT was performed. All TTs were started from a diving box and timed with a stopwatch. | Normotensive | L-Arginine or L-Citrulline | 8 g/day | 8 days | NOx, 200 m and 100 m swimming, BLa ↔ | |
| Cutrufello et al. (2015) [129] | Mixed athletes (11 M, 11 F) (20.6 ± 1.2 y) | aerobic exercise | Chest press; maximum number of repetitions at 80% 1RM for 5 sets with a 30 s rest period between each set. Bruce protocol on treadmill | Normotensive | 60 and 120 min before exercise protocol | L-Citrulline | 6 g | Acute | Number of repetitions, time to exhaustion, VO2max ↔ |
| Streeter et al. (2019) [136] | 30 healthy, physically active participants (20.4 ± 1.8 y) (15 M, 15 F) | acute resistance exercise (isokinetic dynamometer) | 5 × 10 maximal isokinetic extension repetitions of the elbow joint at 90° | Normotensive | 55 min before exercise | L-Arginine | 3 g | Acute | Elbow extension and flexion, FMD, BP, HRV ↔ |
| Chappell et al. (2018) [137] | 15 recreational resistance trained adults (11 M, 4 F) (24 ± 2 y) | resistance exercise | 10 sets × 10 reps 70% of Concentric force max 1-min rest between sets, Leg curl – knee extensor and flexor strength | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Total Reps, Isometric force max, Concentric force max, Eccentric force max ↔ Blood lactate ↔, Quadriceps muscle soreness ↑ |
| Farney et al. (2019) [138] | 12 recreationally trained adults (6 M, 6 F) (24 ± 4 y) | resistance exercise | 1 set × 15 reps at 180° sec, Leg extension | Normotensive | 1 h before test | Citrulline Malate | 8 g | Acute | Total Reps, Peak torque, Peak power, Fatigue index ↔ Lactate, Heart rate ↔ |
| Wong et al. (2016) [89] | 41 postmenopausal overweight or obese females (WBVT + pla: 58.0 ± 4.0 y, Cit: 58.0 ± 4.0 y, WBVT + Cit: 58.0 ± 3.0 y) | whole-body vibration training | Consisted of static and dynamic squats with a 90° knee angle (considering 180° as full knee extension), semi-squats with 120° knee angle, wide-stance semi-squats, and calf raises. The training volume was increased progressively over the 8-week training period by increasing the intensity of vibration (25–40 Hz of frequency and 1–2 mm of amplitude), duration of the exercise set (30–60 s), number of sets (1–5), and total duration of the training session (11–60 min) and decreasing the duration of rest periods (60–30 s) between sets. | Normotensive | before breakfast and before sleeping | L-Citrulline | 6 g/day | –8 weeks | AP, Brachial and aortic BP, BP, Alx, Alx@75 ↓ NOx ↑ |
| Buckinx et al. (2018) [139] | 56 dynapenic-obese elderly (26 Cit, 30 Pla) (Cit: 65.7 ± 4.2 y, Pla: 68.1 ± 4.2 y) | high-intensity interval training | 30 min exercise session 5 min warm-up at low intensity (50–60% maximal heart rate and/or a score between 8 and 12 on the Borg scale) 20-min HIIT of multiples 30 s sprints at a high intensity (80–85% maximal heart rate or Borg’ scale > 17) alternating with sprints of 90 s at a moderate intensity (65% maximal heart rate or Borg’scale score 13–16) 5 min cool-down (50–60% maximal heart rate and/or a Borg’ scale score 8–12) | Normotensive | every day during lunch meals | L-Citrulline | 10 g/day | 12 weeks | upper limbs muscle strength ↑ walking speed ↑ |
| Kang et al. (2022) [93] | 24 postmenopausal women (13 Cit, 11 Pla) (Cit: 62 ± 2 y, Pla: 63 ± 1 y) | slow velocity low-intensity resistance training | slow velocity low-intensity resistance training 4 lower body exercises (leg press, leg extension, leg curl, and calf raise) lasting approximately 25 min per session, 3 times a week Intensity: 40% and 50% of the estimated 1RM for the first and second 2 weeks All exercise movements with a slow speed contraction (3 s concentric and 3 s eccentric) using a metronome for 3 sets of 15 repetitions with 1–3 min of rest between sets | Hypertensive | a daily dose of 10 g taking 6 pills in the morning and 7 at night | L-Citrulline | 10 g/day | 4 weeks | leg lean mass and curl strength ↑ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-Y.; Kim, S.-W.; Seo, J.; Jung, Y.P.; Kim, H.; Kim, A.-J.; Kim, S.; Lim, K. Dietary Arginine and Citrulline Supplements for Cardiovascular Health and Athletic Performance: A Narrative Review. Nutrients 2023, 15, 1268. https://doi.org/10.3390/nu15051268
Park H-Y, Kim S-W, Seo J, Jung YP, Kim H, Kim A-J, Kim S, Lim K. Dietary Arginine and Citrulline Supplements for Cardiovascular Health and Athletic Performance: A Narrative Review. Nutrients. 2023; 15(5):1268. https://doi.org/10.3390/nu15051268
Chicago/Turabian StylePark, Hun-Young, Sung-Woo Kim, Jisoo Seo, Yanghoon P. Jung, Hyunji Kim, Ah-Jin Kim, Sonwoo Kim, and Kiwon Lim. 2023. "Dietary Arginine and Citrulline Supplements for Cardiovascular Health and Athletic Performance: A Narrative Review" Nutrients 15, no. 5: 1268. https://doi.org/10.3390/nu15051268
APA StylePark, H.-Y., Kim, S.-W., Seo, J., Jung, Y. P., Kim, H., Kim, A.-J., Kim, S., & Lim, K. (2023). Dietary Arginine and Citrulline Supplements for Cardiovascular Health and Athletic Performance: A Narrative Review. Nutrients, 15(5), 1268. https://doi.org/10.3390/nu15051268