
Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire for Children Aged 6–12 in Western China
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Food Frequency Questionnaire (FFQ)
2.4. Twenty-Four Hour Recall
2.5. Food and Nutrient Assessment
2.6. Statistical Analysis
3. Results
3.1. The Characteristics of the Participants
3.2. Reproducibility
3.3. Relative Validity
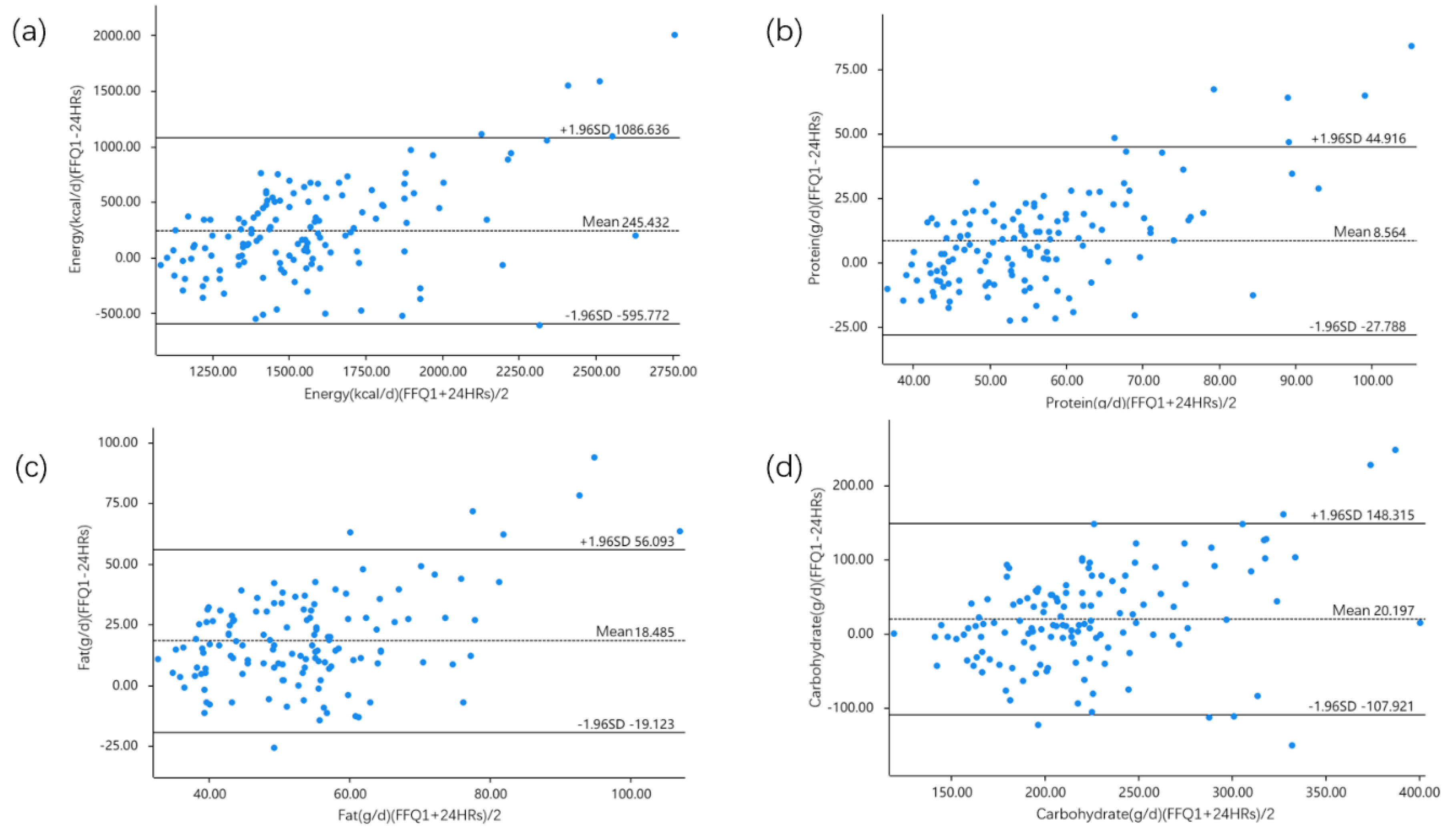
3.4. Bland–Altman Analysis
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nguyen, A.N.; Jen, V.; Jaddoe, V.W.V.; Rivadeneira, F.; Jansen, P.W.; Ikram, M.A.; Voortman, T. Diet quality in early and mid-childhood in relation to trajectories of growth and body composition. Clin. Nutr. 2019, 39, 845–852. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Magenes, V.C.; Pascuzzi, M.C.; Rossi, V.; Sangiorgio, A.; Bosetti, A.; Zuccotti, G.; Mameli, C. The role of pediatric nutrition as a modifiable risk factor for precocious puberty. Life 2021, 11, 1353. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Pawlak, D.B.; Ludwig, D.S. Childhood obesity: Public-health crisis, common sense cure. Lancet 2002, 360, 473–482. [Google Scholar] [CrossRef]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Subar, A.F. Validity of a dietary questionnaire assessed by comparison with multiple weighed dietary records or 24-hour recalls. Am. J. Epidemiol. 2017, 185, 570–584. [Google Scholar] [CrossRef]
- Willett, W. 24-hour recall and diet record methods. In Nutritional Epidemiology, 3rd ed.; Oxford Scholarship Online: New York, NY, USA, 2012; pp. 50–70. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef]
- Willett, W. Food frequency methods. In Nutritional Epidemiology, 3rd ed.; Oxford Scholarship Online: New York, NY, USA, 2012; pp. 71–96. [Google Scholar]
- Sharma, S. Development and use of FFQ among adults in diverse settings across the globe. Proc. Nutr. Soc. 2011, 70, 232–251. [Google Scholar] [CrossRef]
- Mohammadifard, N.; Haghighatdust, F.; Kelishadi, R.; Bahonar, A.; Dianatkhah, M.; Heidari, H.; Maghroun, M.; Dehghan, M. Validity and reproducibility of a semi-quantitative food frequency questionnaire for Iranian adults. Nutr. Diet 2021, 78, 305–314. [Google Scholar] [CrossRef]
- Wong, J.E.; Parnell, W.R.; Black, K.E.; Skidmore, P.M. Reliability and relative validity of a food frequency questionnaire to assess food group intakes in New Zealand adolescents. Nutr. J. 2012, 11, 65. [Google Scholar] [CrossRef]
- Rodriguez, C.A.; Smith, E.R.; Villamor, E.; Zavaleta, N.; Respicio-Torres, G.; Contreras, C.; Perea, S.; Jimenez, J.; Tintaya, K.; Lecca, L.; et al. Development and validation of a food frequency questionnaire to estimate intake among children and adolescents in urban Peru. Nutrients 2017, 9, 1112. [Google Scholar] [CrossRef]
- Oviedo-Solís, C.I.; Monterrubio-Flores, E.A.; Cediel, G.; Denova-Gutiérrez, E.; Barquera, S. Relative validity of a semi-quantitative food frequency questionnaire to estimate dietary intake according to the NOVA classification in Mexican children and adolescents. J. Acad. Nutr. Diet 2022, 122, 1129–1140. [Google Scholar] [CrossRef]
- Huybrechts, I.; Miglio, R.; Mistura, L.; Grioni, S.; Pozzebon, I.; Odorifero, C.; Borea, R.; Gitto, A.; Terrafino, M.; Scipioni, M.; et al. Relative validity of an Italian EPIC food Frequency questionnaire for dietary factors in children and adolescents. A Rizzoli orthopedic institute study. Nutrients 2021, 13, 1245. [Google Scholar] [CrossRef]
- Ding, Y.; Li, F.; Hu, P.; Ye, M.; Xu, F.; Jiang, W.; Yang, Y.; Fu, Y.; Zhu, Y.; Lu, X.; et al. Reproducibility and relative validity of a semi-quantitative food frequency questionnaire for the Chinese lactating mothers. Nutr. J. 2021, 20, 20. [Google Scholar] [CrossRef]
- Zhang, H.; Qiu, X.; Zhong, C.; Zhang, K.; Xiao, M.; Yi, N.; Xiong, G.; Wang, J.; Yao, J.; Hao, L.; et al. Reproducibility and relative validity of a semi-quantitative food frequency questionnaire for Chinese pregnant women. Nutr. J. 2015, 14, 56. [Google Scholar] [CrossRef]
- Liu, D.; Ju, H.; Yang, Z.Y.; Zhang, Q.; Gao, J.F.; Gong, D.P.; Guo, D.D.; Luo, S.Q.; Zhao, W.H. Food frequency questionnaire for Chinese children aged 12–17 years: Validity and reliability. Biomed. Environ. Sci. 2019, 32, 486–495. [Google Scholar] [CrossRef]
- Ma, Y.; Tan, J.; Tan, Z.; Shang, L. Validity and reliability of semiquantitative food frequency questionnaires for assessing nutrient intake among preschool children in Northwest China. J. Healthc. Eng. 2022, 2022, 1677252. [Google Scholar] [CrossRef]
- The Chinese Nutrition Society. Dietary Guidelines for Chinese School-Age Children; People’s Medical Publishing House Press: Beijing, China, 2022. [Google Scholar]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition; Peiking University Medical Press: Beijing, China, 2019. [Google Scholar]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition; Peiking University Medical Center Press: Beijing, China, 2002. [Google Scholar]
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Lombard, M.J.; Steyn, N.P.; Charlton, K.E.; Senekal, M. Application and interpretation of multiple statistical tests to evaluate validity of dietary intake assessment methods. Nutr. J. 2015, 14, 40. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Willett, W.C. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Hu, X.; Li, L.; Ouyang, Y.; Hu, H.; Guan., F.; Wang, H.; Wang, L.; Li, Y.; Zhang, B.; Guo, C.; et al. Trends of overweight and obesity among children and adolescents aged 7–17 in 16 provinces of China from 2000 to 2018. Wei Sheng Yan Jiu 2022, 51, 568–573. [Google Scholar] [CrossRef]
- Preston, A.M.; Palacios, C.; Rodríguez, C.A.; Vélez-Rodríguez, R.M. Validation and reproducibility of a semi-quantitative food frequency questionnaire for use in Puerto Rican children. Puerto Rico Health Sci. J. 2011, 30, 58–64. [Google Scholar] [PubMed]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Grubb, D.A.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire: Use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Andrellucchi, A.; Henríquez-Sánchez, P.; Sánchez-Villegas, A.; Peña-Quintana, L.; Mendez, M.; Serra-Majem, L. Dietary assessment methods for micronutrient intake in infants, children and adolescents: A systematic review. Br. J. Nutr. 2009, 102 (Suppl. S1), S87–S117. [Google Scholar] [CrossRef] [PubMed]
- Mai, T.M.T.; Tran, Q.C.; Nambiar, S.; Pols, J.C.V.; Gallegos, D. Development and validation of the Vietnamese children’s short dietary questionnaire to evaluate food groups intakes and dietary practices among 9–11-year-olds children in urban Vietnam. Nutrients 2022, 14, 3996. [Google Scholar] [CrossRef]
- Marques Rde, M.; de Oliveira, A.C.; Teles, S.A.; Stringuini, M.L.; Fornés, N.S.; Gardenghi, G. Relative validity and reproducibility of a quantitative food frequency questionnaire for adolescents with type 1 diabetes: Validity of a food frequency questionnaire. Int. J. Endocrinol. 2014, 2014, 976508. [Google Scholar] [CrossRef]
- Xia, W.; Sun, C.; Zhang, L.; Zhang, X.; Wang, J.; Wang, H.; Wu, L. Reproducibility and relative validity of a food frequency questionnaire developed for female adolescents in Suihua, North China. PLoS ONE 2011, 6, e19656. [Google Scholar] [CrossRef] [PubMed]
- Notario-Barandiaran, L.; Freire, C.; García-de-la-Hera, M.; Compañ-Gabucio, L.M.; Torres-Collado, L.; González-Palacios, S.; Mundo, A.; Molina, M.; Fernández, M.F.; Vioque, J. Reproducibility and validity of a food frequency questionnaire for dietary assessment in adolescents in a self-reported way. Nutrients 2020, 12, 2081. [Google Scholar] [CrossRef]
- Truthmann, J.; Mensink, G.B.; Richter, A. Relative validation of the KiGGS food frequency questionnaire among adolescents in Germany. Nutr. J. 2011, 10, 133. [Google Scholar] [CrossRef]
- Park, Y.; Dodd, K.W.; Kipnis, V.; Thompson, F.E.; Potischman, N.; Schoeller, D.A.; Baer, D.J.; Midthune, D.; Troiano, R.P.; Bowles, H.; et al. Comparison of self-reported dietary intakes from the automated self-administered 24-h recall, 4-d food records, and food-frequency questionnaires against recovery biomarkers. Am. J. Clin. Nutr. 2018, 107, 80–93. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Male (n = 68) | Female (n = 65) | ap-Value |
|---|---|---|---|---|
| Age (years, mean ± SD) | 9.3 ± 0.9 | 9.5 ± 0.7 | 9.1 ± 1.0 | 0.05 |
| 6–9 years | 65 (48.9) | 28 (41.2) | 37 (56.9) | 0.07 |
| 9–12 years | 68 (51.1) | 40 (58.8) | 28 (43.1) | |
| Height (cm, mean ± SD) | 139.3 ± 8.5 | 141.2. ± 9.2 | 137.3 ± 7.4 | <0.01 |
| Weight (kg, mean ± SD) | 35.1 ± 9.4 | 37.7 ± 10.1 | 32.4 ± 7.8 | <0.01 |
| b Body mass index (BMI) (kg/m2, mean ± SD) | 18.0 ± 3.3 | 18.7 ± 3.7 | 17.2 ± 2.6 | 0.07 |
| Underweight (n, %) | 6 (4.5) | 3 (4.4) | 3 (4.6) | 0.23 |
| Normal weight (n, %) | 83 (62.4) | 37 (54.4) | 46 (70.8) | |
| Overweight (n, %) | 23 (17.3) | 14 (20.6) | 9 (13.8) | |
| Obese (n, %) | 21 (15.8) | 14 (20.6) | 7 (10.8) | |
| Father’s education level (n, %) | ||||
| Junior high school or below | 66 (49.6) | 38 (55.9) | 28 (43.0) | 0.06 |
| Senior high school | 29 (21.8) | 17 (25.0) | 12 (18.5) | |
| University degree or above | 38 (28.6) | 13 (19.1) | 25 (38.5) | |
| Mother’s education level (n, %) | ||||
| Junior high school or below | 58 (43.6) | 33 (48.5) | 25 (38.5) | 0.32 |
| Senior high school | 32 (24.1) | 17 (25.0) | 15 (23.0) | |
| University degree or above | 43 (32.3) | 18 (26.5) | 25 (38.5) | |
| c Average family income (n, %) | ||||
| ≤5000 | 11 (8.3) | 7 (10.3) | 4 (6.2) | 0.27 |
| 5001–10,000 | 77 (57.9) | 42 (61.8) | 35 (53.8) | |
| >10,000 | 45 (33.8) | 19 (27.9) | 26 (40.0) |
| Food Groups (g/day) | Median (P25, P75) | ap-Value | Correlation Coefficient | Agreement (%) | d K | ||||
|---|---|---|---|---|---|---|---|---|---|
| FFQ1 | FFQ2 | b rs | c ri | Same Quartile | Same or Adjacent Quartile | Extreme Quartile | |||
| Cereals and potatoes | 243 (193, 276) | 218 (182, 279) | 0.03 | 0.69 ** | 0.71 ** | 52.6 | 83.4 | 2.3 | 0.62 |
| Meat | 72 (51, 107) | 76 (49, 113) | 0.50 | 0.67 ** | 0.72 ** | 56.4 | 71.7 | 1.5 | 0.67 |
| Aquatic products | 7 (2, 12) | 7 (3, 13) | 0.71 | 0.52 ** | 0.40 ** | 46.6 | 83.4 | 5.3 | 0.49 |
| Eggs | 26 (11, 42) | 26 (11, 42) | 0.40 | 0.77 ** | 0.40 ** | 72.2 | 91.7 | 1.5 | 0.75 |
| Milk and milk products | 123 (77, 201) | 121 (68, 204) | 0.53 | 0.84 ** | 0.85 ** | 69.9 | 94.0 | 0.8 | 0.80 |
| Soy and soy products | 9 (6, 12) | 8 (4, 11) | 0.02 | 0.60 ** | 0.55 ** | 50.4 | 85.0 | 3.0 | 0.57 |
| Vegetables | 214 (140, 334) | 230 (143, 337) | 0.83 | 0.30 ** | 0.44 ** | 34.6 | 74.4 | 8.3 | 0.27 |
| Fruits | 164 (109, 286) | 204 (112, 356) | <0.01 | 0.63 ** | 0.50 ** | 48.9 | 84.2 | 0.8 | 0.59 |
| Nuts | 4 (2, 10) | 4 (1, 12) | 0.47 | 0.45 ** | 0.45 ** | 40.6 | 77.4 | 6.0 | 0.38 |
| Snacks | 8 (4, 16) | 11 (6, 19) | 0.03 | 0.56 ** | 0.48 ** | 51.1 | 84.2 | 3.0 | 0.56 |
| Beverages | 52 (34, 122) | 78 (34, 154) | 0.02 | 0.38 ** | 0.20 * | 36.1 | 72.9 | 7.5 | 0.35 |
| Oil | 17 (11, 21) | 14 (10, 21) | 0.17 | 0.52 ** | 0.54 ** | 56.4 | 73.7 | 0.0 | 0.49 |
| Energy and Nutrients | Median (P25, P75) | ap-Value | Correlation Coefficient | Agreement (%) | d K | ||||
|---|---|---|---|---|---|---|---|---|---|
| FFQ1 | FFQ2 | b rs | c ri | Same Quartile | Same or Adjacent Quartile | Extreme Quartile | |||
| Energy (kcal/day) | 1623.3 (1400.2, 1877.8) | 1610.1 (1319.6, 1952.5) | 0.83 | 0.65 ** | 0.63 ** | 52.6 | 88.7 | 1.5 | 0.65 |
| Protein (g/day) | 57.2 (47.4, 67.8) | 56.8 (45.5, 68.9) | 0.97 | 0.66 ** | 0.68 ** | 48.9 | 89.5 | 1.5 | 0.64 |
| Fat (g/day) | 59.0 (51.3, 70.1) | 58.2 (47.0, 72.0) | 0.20 | 0.60 ** | 0.72 ** | 41.3 | 84.2 | 2.3 | 0.53 |
| Carbohydrate (g/day) | 223.7 (182.1, 267.4) | 223.0 (177.8, 276.7) | 0.73 | 0.65 ** | 0.58 ** | 53.4 | 89.5 | 2.3 | 0.62 |
| Dietary fiber (g/day) | 12.1 (9.2, 16.2) | 12.4 (8.3, 17.0) | 0.86 | 0.52 ** | 0.52 ** | 40.6 | 78.9 | 2.3 | 0.47 |
| Cholesterol(mg/day) | 275.5 (200.2, 408.8) | 276.5 (184.1, 413.2) | 0.61 | 0.82 ** | 0.52 ** | 60.1 | 94.0 | 0.8 | 0.73 |
| Vitamin A (μgRAE/day) | 401.9 (294.3, 521.7) | 360.8 (283.5, 520.4) | 0.44 | 0.47 ** | 0.37 ** | 36.8 | 82.7 | 4.5 | 0.46 |
| Vitamin E (mg/day) | 19.2 (15.4, 23.5) | 19.2 (17.8, 23.4) | 0.63 | 0.58 ** | 0.61 ** | 45.9 | 81.9 | 2.3 | 0.52 |
| Thiamin (mg/day) | 0.8 (0.7, 1.0) | 0.8 (0.7, 1.0) | 0.33 | 0.55 ** | 0.61 ** | 43.6 | 81.9 | 2.3 | 0.53 |
| Riboflavin (mg/day) | 0.9 (0.7, 1.1) | 0.9 (0.7, 1.1) | 0.67 | 0.57 ** | 0.52 ** | 48.1 | 83.4 | 2.3 | 0.56 |
| Vitamin B6 (mg/day) | 0.7 (0.5, 0.9) | 0.7 (0.5, 1.0) | 0.76 | 0.53 ** | 0.51 ** | 42.9 | 80.4 | 3.8 | 0.48 |
| Vitamin B12 (μg/day) | 1.5 (1.1, 2.0) | 1.5 (1.1, 2.0) | 0.30 | 0.68 ** | 0.61 ** | 53.4 | 89.5 | 2.3 | 0.66 |
| Vitamin C (mg/day) | 97.8 (59.4, 138.5) | 94.9 (58.4, 162.0) | 0.53 | 0.50 ** | 0.51 ** | 39.1 | 78.9 | 2.3 | 0.46 |
| Pantothenic acid(mg/day) | 2.0 (1.5, 2.9) | 2.2 (1.4, 3.3) | 0.35 | 0.46 ** | 0.42 ** | 42.9 | 79.7 | 3.8 | 0.47 |
| Folate (μg/day) | 215.8 (151.7, 275.6) | 194.3 (147.6, 280.9) | 0.30 | 0.53 ** | 0.49 ** | 39.8 | 80.5 | 3.0 | 0.47 |
| Niacin (mg/day) | 12.7 (10.6, 15.8) | 12.8 (10.5, 17.0) | 0.74 | 0.59 ** | 0.66 ** | 44.4 | 84.2 | 2.3 | 0.55 |
| Calcium (mg/day) | 441.1 (362.6, 583.0) | 443.8 (336.9, 581.5) | 0.80 | 0.60 ** | 0.49 ** | 51.9 | 85.0 | 1.5 | 0.60 |
| Phosphorus (mg/day) | 932.8 (784.4, 1103.9) | 933.3 (775.5, 1139.3) | 0.90 | 0.64 ** | 0.65 ** | 42.1 | 89.5 | 2.3 | 0.60 |
| Potassium (mg/day) | 1891.9 (1454.5, 2258.6) | 1901.7 (1421.2, 2469.6) | 0.70 | 0.56 ** | 0.57 ** | 45.1 | 83.5 | 2.3 | 0.54 |
| Sodium (mg/day) | 874.9 (659.8, 1119.3) | 870.6 (611.7, 1072.7) | 0.09 | 0.59 ** | 0.61 ** | 45.9 | 84.2 | 2.3 | 0.55 |
| Magnesium (mg/day) | 263.5 (214.4, 324.4) | 259.2 (207.8, 338.4) | 0.96 | 0.56 ** | 0.56 ** | 47.4 | 81.9 | 3.0 | 0.52 |
| Iron (mg/day) | 14.1 (11.5, 17.0) | 13.6 (10.8, 17.5) | 0.64 | 0.62 ** | 0.60 ** | 44.4 | 85.7 | 1.5 | 0.58 |
| Iodine (μg/day) | 71.0 (54.2, 94.1) | 62.4 (47.5, 93.4) | <0.01 | 0.60 ** | 0.54 ** | 41.3 | 87.2 | 2.3 | 0.57 |
| Zinc (mg/day) | 7.8 (6.5, 9.4) | 7.9 (6.3, 9.7) | 0.85 | 0.60 ** | 0.64 ** | 44.4 | 81.2 | 2.3 | 0.52 |
| Selenium (μg/day) | 29.3 (24.0, 35.7) | 30.0 (22.6, 36.6) | 0.37 | 0.72 ** | 0.75 ** | 53.4 | 89.5 | 1.5 | 0.66 |
| Copper (mg/day) | 1.2 (0.9, 1.6) | 1.2 (0.9, 1.7) | 0.39 | 0.60 ** | 0.59 ** | 43.6 | 82.7 | 1.5 | 0.54 |
| Manganese (mg/day) | 3.8 (3.2, 4.7) | 3.8 (3.1, 4.7) | 0.78 | 0.64 ** | 0.66 ** | 45.9 | 84.2 | 2.3 | 0.56 |
| Food Groups (g/day) | Median (P25, P75) | ap- Value | Correlation Coefficient | Agreement (%) | d K | ||||
|---|---|---|---|---|---|---|---|---|---|
| FFQ1 | 24HR | b rs | c re-adj | Same Quartile | Same or Adjacent Quartile | Extreme Quartile | |||
| Cereals and potatoes | 243 (193, 276) | 262 (212, 304) | <0.01 | 0.35 ** | 0.21 * | 30.8 | 72.2 | 5.3 | 0.29 |
| Meat | 72 (51, 107) | 62 (38, 94) | <0.01 | 0.24 ** | 0.24 ** | 28.6 | 69.2 | 6.0 | 0.23 |
| Aquatic products | 7 (2, 12) | 0.5 (0, 1.4) | <0.01 | 0.15 | 0.15 | 37.6 | 75.2 | 9.8 | 0.12 |
| Eggs | 26 (11, 42) | 31 (17, 49) | 0.02 | 0.17 * | 0.12 | 30.8 | 67.7 | 11.3 | 0.14 |
| Milk and milk products | 123 (77, 201) | 76 (0, 133) | <0.01 | 0.37 ** | 0.37 ** | 36.8 | 77.4 | 4.5 | 0.37 |
| Soy and soy products | 9 (6, 12) | 14 (7.6, 20) | <0.01 | 0.36 ** | 0.30 ** | 33.1 | 77.4 | 5.3 | 0.33 |
| Vegetables | 214 (140, 334) | 184 (137, 235) | <0.01 | 0.16 | 0.13 | 28.6 | 77.4 | 7.5 | 0.26 |
| Fruits | 164 (109, 286) | 81 (43, 132) | <0.01 | 0.32 ** | 0.26 ** | 34.6 | 71.4 | 8.3 | 0.24 |
| Nuts | 4 (2, 10) | 3 (0, 6) | <0.01 | 0.05 | 0.07 | 26.3 | 65.4 | 9.8 | 0.05 |
| Snacks | 8 (4, 16) | 5 (0, 21) | 0.09 | 0.15 | 0.15 | 30.1 | 64.7 | 12.3 | 0.14 |
| Beverages | 52 (34, 122) | 25 (0, 67) | <0.01 | 0.02 | 0.02 | 37.0 | 75.5 | 8.2 | 0.06 |
| Oil | 17 (11, 21) | 11 (9, 13) | <0.01 | 0.11 | 0.13 | 30.9 | 70.7 | 7.5 | 0.13 |
| Energy and Nutrients | Median (P25, P75) | ap-Value | Correlation Coefficient | |||
|---|---|---|---|---|---|---|
| FFQ1 | 24HR | b rs | c re-adj | d r de-att | ||
| Energy (kcal/day) | 1623.3 (1400.2, 1877.8) | 1425.0 (1235.0, 1604.0) | <0.01 | 0.44 ** | - | 0.48 ** |
| Protein (g/day) | 57.2 (47.4, 67.8) | 50.6 (44.4, 57.0) | <0.01 | 0.37 ** | 0.30 ** | 0.42 ** |
| Fat (g/day) | 59.0 (51.3, 70.1) | 44.0 (34.4, 52.1) | <0.01 | 0.31 ** | 0.28 ** | 0.36 ** |
| Carbohydrate (g/day) | 223.7 (182.1, 267.4) | 204.1 (177.7, 240.6) | <0.01 | 0.45 ** | 0.36 ** | 0.48 ** |
| Dietary fiber (g/day) | 12.1 (9.2, 16.2) | 8.3 (7.0, 9.7) | <0.01 | 0.35 ** | 0.28 ** | 0.39 ** |
| Cholesterol(mg/day) | 275.5 (200.2, 408.8) | 243.0 (194.0, 356.5) | 0.24 | 0.22 * | 0.18 * | 0.26 ** |
| Vitamin A (μgRAE/day) | 401.9 (294.3, 521.7) | 219.0 (165.0, 273.5) | <0.01 | 0.08 | 0.02 | 0.09 |
| Vitamin E (mg/day) | 19.2 (15.4, 23.5) | 16.7 (14.2, 16.6) | <0.01 | 0.21 * | 0.22 * | 0.25 ** |
| Thiamin (mg/day) | 0.8 (0.7, 1.0) | 0.8 (0.6, 0.9) | 0.001 | 0.25 ** | 0.22 * | 0.29 ** |
| Riboflavin (mg/day) | 0.9 (0.7, 1.1) | 0.7 (0.5, 0.8) | <0.01 | 0.33 ** | 0.30 ** | 0.38 ** |
| Vitamin C (mg/day) | 97.8 (59.4, 138.5) | 55.7 (41.1, 76.9) | <0.01 | 0.21 * | 0.15 | 0.25 ** |
| Folate (μg/day) | 215.8 (151.7, 275.6) | 84.2 (68.4, 106.7) | <0.01 | 0.33 ** | 0.31 ** | 0.38 ** |
| Niacin (mg/day) | 12.7 (10.6, 15.8) | 11.3 (9.7, 12.9) | <0.01 | 0.26 ** | 0.20 * | 0.30 ** |
| Calcium (mg/day) | 441.1 (362.6, 583.0) | 328.0 (277.9, 428.5) | <0.01 | 0.39 ** | 0.32 ** | 0.44 ** |
| Phosphorus (mg/day) | 932.8 (784.4, 1103.9) | 754.0 (672.0, 856.5) | <0.01 | 0.35 ** | 0.33 ** | 0.40 ** |
| Potassium (mg/day) | 1891.9 (1454.5, 2258.6) | 1334.0 (1172.0, 1509.5) | <0.01 | 0.21 * | 0.12 | 0.24 ** |
| Sodium (mg/day) | 874.9 (659.8, 1119.3) | 491.4 (370.5, 654.0) | <0.01 | 0.28 ** | 0.17 * | 0.33 ** |
| Magnesium (mg/day) | 263.5 (214.4, 324.4) | 235.0 (212.0, 264.5) | <0.01 | 0.32 ** | 0.28 ** | 0.36 ** |
| Iron (mg/day) | 14.1 (11.5, 17.0) | 13.7 (12.1, 15.4) | 0.80 | 0.29 ** | 0.22 * | 0.32 ** |
| Iodine (μg/day) | 71.0 (54.2, 94.1) | 35.6 (25.8, 52.6) | <0.01 | 0.20 * | 0.07 | 0.23 ** |
| Zinc (mg/day) | 7.8 (6.5, 9.4) | 7.2 (6.4, 7.9) | <0.01 | 0.29 ** | 0.26 ** | 0.33 ** |
| Selenium (μg/day) | 29.3 (24.0, 35.7) | 27.7 (23.7, 32.8) | 0.16 | 0.31 ** | 0.18 * | 0.36 ** |
| Copper (mg/day) | 1.2 (0.9, 1.6) | 1.0 (0.9, 1.2) | <0.01 | 0.19 * | 0.10 | 0.22 * |
| Manganese (mg/day) | 3.8 (3.2, 4.7) | 3.6 (3.1, 4.2) | 0.001 | 0.44 ** | 0.35 ** | 0.47 ** |
| Energy and Nutrients | Agreement by Quartile (%) | a K | b Agreement by LoA (%) | ||
|---|---|---|---|---|---|
| Same Quartile | Same or Adjacent Quartile | Extreme Quartile | |||
| Energy | 38.3 | 75.9 | 4.5 | 0.38 | 95.5 |
| Protein | 31.6 | 69.9 | 3.8 | 0.35 | 95.5 |
| Fat | 35.3 | 75.2 | 6.8 | 0.31 | 95.5 |
| Carbohydrate | 39.1 | 77.4 | 5.3 | 0.38 | 94.7 |
| Dietary fiber | 33.8 | 75.2 | 8.3 | 0.28 | 94.0 |
| Cholesterol | 23.3 | 74.4 | 9.0 | 0.21 | 94.7 |
| Vitamin A | 28.6 | 63.2 | 9.8 | 0.08 | 93.2 |
| Vitamin E | 25.6 | 66.9 | 8.3 | 0.15 | 96.2 |
| Thiamin | 30.8 | 71.4 | 9.0 | 0.23 | 94.7 |
| Riboflavin | 30.1 | 74.4 | 6.0 | 0.31 | 94.7 |
| Vitamin C | 29.3 | 66.9 | 7.5 | 0.18 | 95.5 |
| Folate | 27.8 | 76.7 | 5.3 | 0.33 | 97.0 |
| Niacin | 32.3 | 69.2 | 5.3 | 0.26 | 94.7 |
| Calcium | 39.8 | 75.9 | 4.4 | 0.39 | 94.0 |
| Phosphorus | 34.6 | 72.9 | 3.0 | 0.36 | 95.5 |
| Potassium | 26.3 | 70.7 | 9.8 | 0.16 | 94.7 |
| Sodium | 31.6 | 72.9 | 6.8 | 0.27 | 94.0 |
| Magnesium | 30.8 | 70.7 | 6.0 | 0.26 | 97.0 |
| Iron | 30.8 | 72.2 | 6.8 | 0.26 | 94.7 |
| Iodine | 30.1 | 66.2 | 10.5 | 0.11 | 98.5 |
| Zinc | 34.6 | 72.9 | 9.0 | 0.26 | 96.2 |
| Selenium | 36.8 | 73.7 | 6.8 | 0.30 | 94.7 |
| Copper | 30.8 | 63.9 | 10.5 | 0.10 | 96.2 |
| Manganese | 38.3 | 78.9 | 5.3 | 0.41 | 96.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, Y.; Deng, H.; Lu, M.; Cheng, Y.; Mi, B.; Xiao, Y.; Zhou, J. Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire for Children Aged 6–12 in Western China. Nutrients 2023, 15, 856. https://doi.org/10.3390/nu15040856
Qin Y, Deng H, Lu M, Cheng Y, Mi B, Xiao Y, Zhou J. Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire for Children Aged 6–12 in Western China. Nutrients. 2023; 15(4):856. https://doi.org/10.3390/nu15040856
Chicago/Turabian StyleQin, Yujie, Hongyang Deng, Mengnan Lu, Yue Cheng, Baibing Mi, Yanfeng Xiao, and Jing Zhou. 2023. "Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire for Children Aged 6–12 in Western China" Nutrients 15, no. 4: 856. https://doi.org/10.3390/nu15040856
APA StyleQin, Y., Deng, H., Lu, M., Cheng, Y., Mi, B., Xiao, Y., & Zhou, J. (2023). Reproducibility and Validity of a Semi-Quantitative Food Frequency Questionnaire for Children Aged 6–12 in Western China. Nutrients, 15(4), 856. https://doi.org/10.3390/nu15040856