
Association between Consumption of Dietary Supplements and Chronic Kidney Disease Prevalence: Results of the Korean Nationwide Population-Based Survey

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
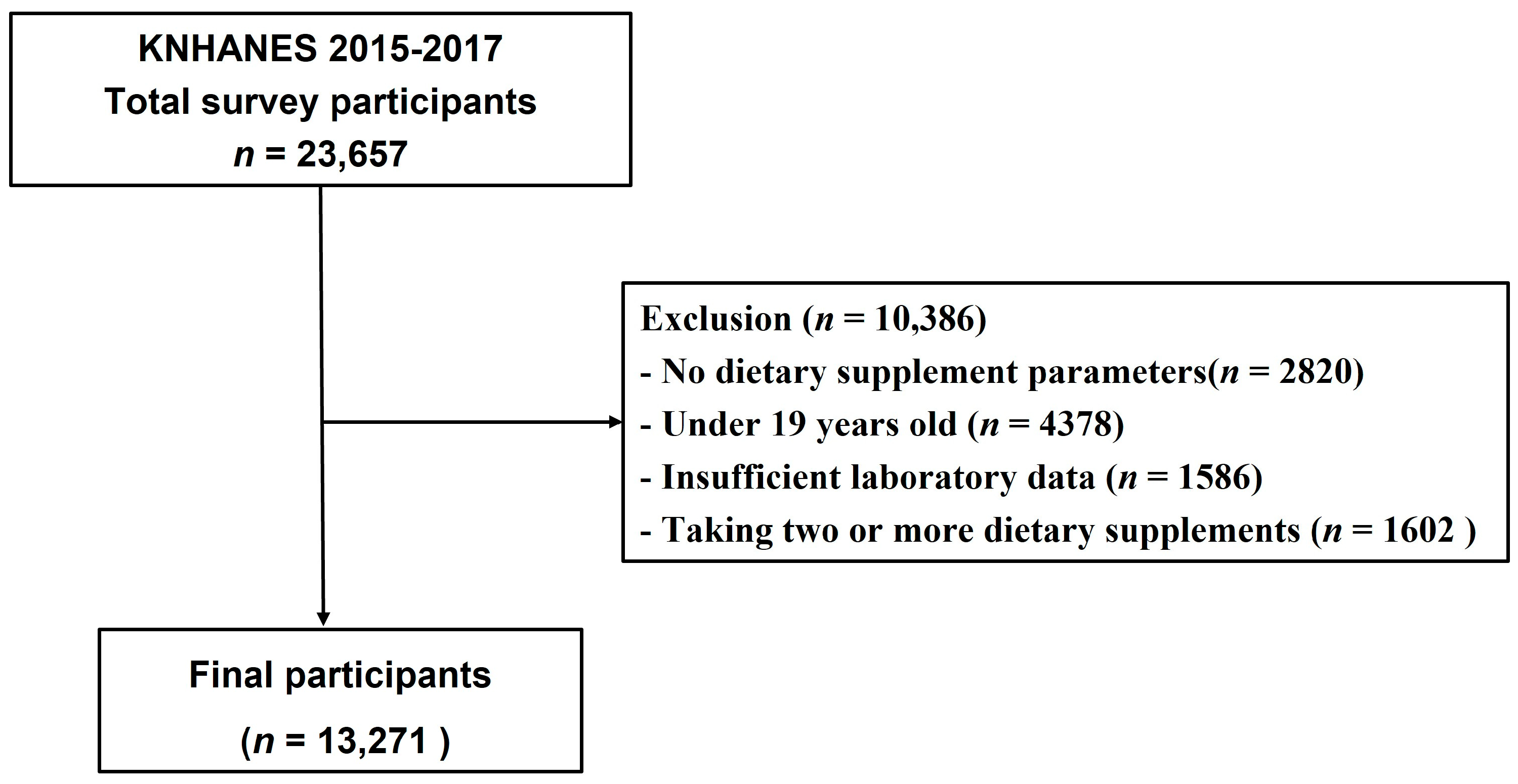
2.1. Data Source and Study Population
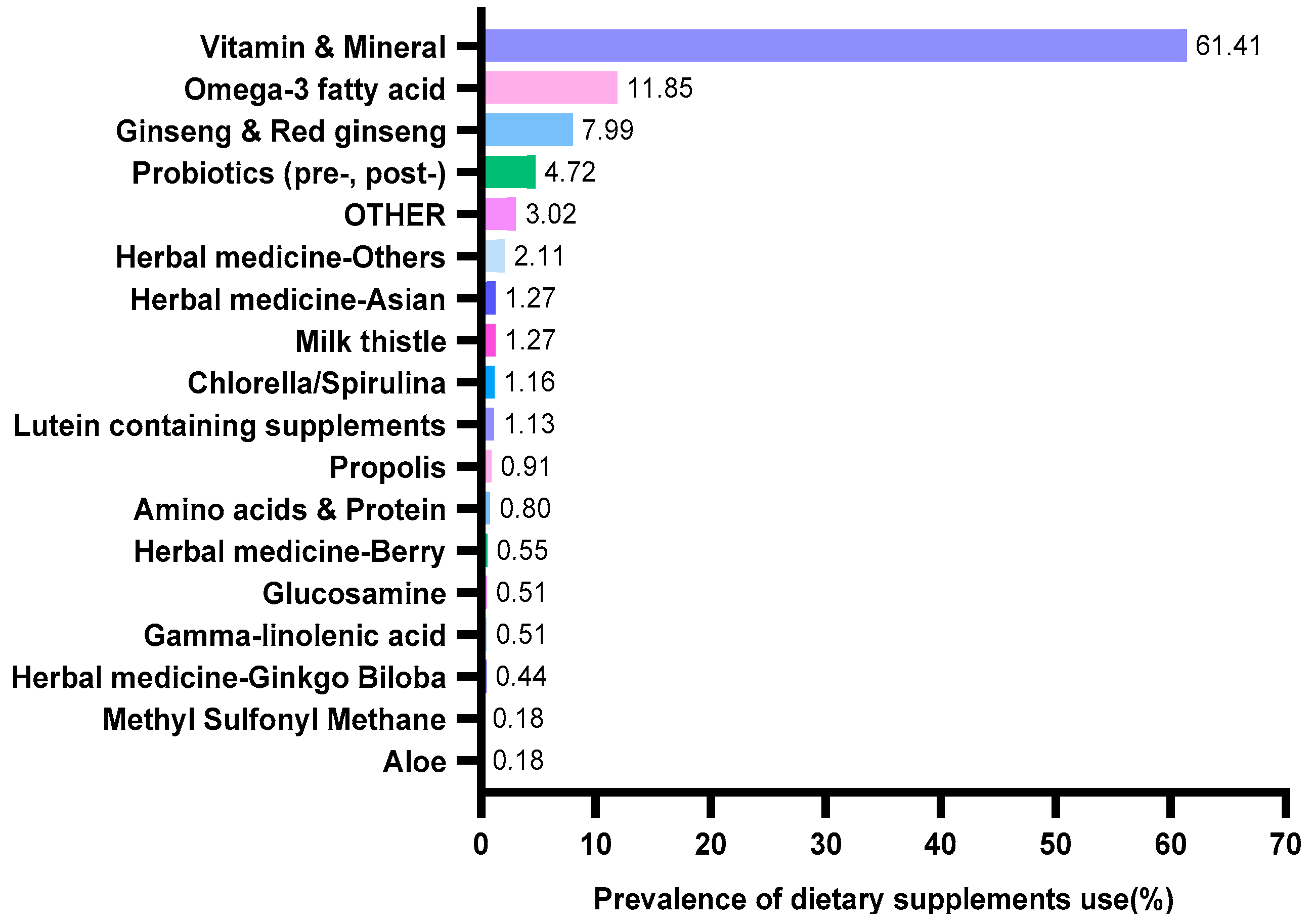
2.2. Different Types of Dietary Supplements
2.3. Assessment of Covariates
2.4. Statistical Analyses
3. Results
3.1. General Characteristics of the Study Subjects
3.2. Association between Different Dietary Supplements and CKD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levin, A.; Tonelli, M.; Bonventre, J.; Coresh, J.; Donner, J.A.; Fogo, A.B.; Fox, C.S.; Gansevoort, R.T.; Heerspink, H.J.L.; Jardine, M.; et al. Global kidney health 2017 and beyond: A roadmap for closing gaps in care, research, and policy. Lancet 2017, 390, 1888–1917. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Tsai, C.C.; Liu, Y.H.; Wu, P.Y.; Huang, J.C.; Chung, T.L.; Su, H.M.; Chen, S.C. Sex Difference in the Associations among Hyperuricemia with New-Onset Chronic Kidney Disease in a Large Taiwanese Population Follow-Up Study. Nutrients 2022, 14, 3832. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Grams, M.E. Epidemiology research to foster improvement in chronic kidney disease care. Kidney Int. 2020, 97, 477–486. [Google Scholar] [CrossRef]
- Lin, P.C.; Chou, C.L.; Ou, S.H.; Fang, T.C.; Chen, J.S. Systematic Review of Nutrition Supplements in Chronic Kidney Diseases: A GRADE Approach. Nutrients 2021, 13, 469. [Google Scholar] [CrossRef]
- Ronis, M.J.J.; Pedersen, K.B.; Watt, J. Adverse Effects of Nutraceuticals and Dietary Supplements. Annu. Rev. Pharmacol. Toxicol. 2018, 58, 583–601. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.C.K.; Eshetie, T.C.; Gray, S.L.; Marcum, Z.A. Dietary Supplement Use in Middle-aged and Older Adults. J. Nutr. Health Aging 2022, 26, 133–138. [Google Scholar] [CrossRef]
- Wierzejska, R.E. Dietary Supplements-For Whom? The Current State of Knowledge about the Health Effects of Selected Supplement Use. Int. J. Environ. Res. Public Health 2021, 18, 8897. [Google Scholar] [CrossRef]
- Crawford, C.; Brown, L.L.; Costello, R.B.; Deuster, P.A. Select Dietary Supplement Ingredients for Preserving and Protecting the Immune System in Healthy Individuals: A Systematic Review. Nutrients 2022, 14, 4604. [Google Scholar] [CrossRef]
- Kim, M.; Lee, Y.; Park, K. Vitamin and Mineral Supplement Use among Korean Adults: Baseline Data from the Trace Element Study of Korean Adults in Yeungnam Area. Nutrients 2018, 10, 50. [Google Scholar] [CrossRef]
- Choi, J. The Association between Health Conditions, Consciousness, Involvement, and Knowledge and Dietary Supplement Intake among University Students in South Korea. Int. J. Environ. Res. Public Health 2019, 16, 4028. [Google Scholar] [CrossRef]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 753–779. [Google Scholar] [CrossRef] [PubMed]
- Junarta, J.; Jha, V.; Banerjee, D. Insight into the impact of vitamin D on cardiovascular outcomes in chronic kidney disease. Nephrology 2019, 24, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Tian, N.; Li, L.; Ng, J.K.; Li, P.K. The Potential Benefits and Controversies of Probiotics Use in Patients at Different Stages of Chronic Kidney Disease. Nutrients 2022, 14, 4044. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.J.; Guo, J.; Wang, Q.; Wang, L.; Wang, Y.; Zhang, F.; Huang, W.J.; Zhang, W.; Liu, W.J.; Wang, Y. Probiotics, prebiotics, and synbiotics for the improvement of metabolic profiles in patients with chronic kidney disease: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 577–598. [Google Scholar] [CrossRef]
- The Homepage of Korea National Health and Nutrition Examination Survey. Available online: https://kosis.kr/index/index.do (accessed on 15 May 2022).
- Health Functional Food Code. Available online: https://www.mfds.go.kr/index.do (accessed on 1 May 2022).
- Delanaye, P.; Jager, K.J.; Bökenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J. Am. Soc. Nephrol. JASN 2019, 30, 1785–1805. [Google Scholar] [CrossRef]
- Alsaleem, S.A.; Asiri, M.M.; Alsaleem, M.A.; AlShahrani, A.N.; Alamer, K.A.; Mahfouz, A.A. Dietary Supplement Use among Primary Health Care Attendants in Abha City, Southwestern Saudi Arabia. Nutrients 2021, 13, 2968. [Google Scholar] [CrossRef]
- Brown, A.C. An overview of herb and dietary supplement efficacy, safety and government regulations in the United States with suggested improvements. Part 1 of 5 series. Food Chem. Toxicol. 2017, 107, 449–471. [Google Scholar] [CrossRef]
- Xu, W.; Choi, H.K.; Huang, L. State of Panax ginseng Research: A Global Analysis. Molecules 2017, 22, 1518. [Google Scholar] [CrossRef]
- Zhang, H.; Abid, S.; Ahn, J.C.; Mathiyalagan, R.; Kim, Y.J.; Yang, D.C.; Wang, Y. Characteristics of Panax ginseng Cultivars in Korea and China. Molecules 2020, 25, 2635. [Google Scholar] [CrossRef]
- Park, S.H.; Chung, S.; Chung, M.Y.; Choi, H.K.; Hwang, J.T.; Park, J.H. Effects of Panax ginseng on hyperglycemia, hypertension, and hyperlipidemia: A systematic review and meta-analysis. J. Ginseng Res. 2022, 46, 188–205. [Google Scholar] [CrossRef]
- Karunasagara, S.; Hong, G.L.; Park, S.R.; Lee, N.H.; Jung, D.Y.; Kim, T.W.; Jung, J.Y. Korean red ginseng attenuates hyperglycemia-induced renal inflammation and fibrosis via accelerated autophagy and protects against diabetic kidney disease. J. Ethnopharmacol. 2020, 254, 112693. [Google Scholar] [CrossRef]
- Sun, Q.; Meng, Q.T.; Jiang, Y.; Liu, H.M.; Lei, S.Q.; Su, W.T.; Duan, W.N.; Wu, Y.; Xia, Z.Y.; Xia, Z.Y. Protective effect of ginsenoside Rb1 against intestinal ischemia-reperfusion induced acute renal injury in mice. PLoS ONE 2013, 8, e80859. [Google Scholar] [CrossRef] [PubMed]
- Stavro, P.M.; Woo, M.; Leiter, L.A.; Heim, T.F.; Sievenpiper, J.L.; Vuksan, V. Long-term intake of North American ginseng has no effect on 24-hour blood pressure and renal function. Hypertension 2006, 47, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, V.; Plantinga, L.C.; Tuot, D.S.; Hedgeman, E.; Saran, R.; Saydah, S.; Rolka, D.; Powe, N.R. Americans’ use of dietary supplements that are potentially harmful in CKD. Am. J. Kidney Dis. 2013, 61, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yoon, J.H.; Kim, S.S.; Ma, S.K.; Kim, S.W.; Bae, E.H. Panax Ginseng Induces Toxic Hepatitis and Acute Kidney Injury. Chonnam Med. J. 2017, 53, 168–169. [Google Scholar] [CrossRef]
- Paik, D.J.; Lee, C.H. Review of cases of patient risk associated with ginseng abuse and misuse. J. Ginseng Res. 2015, 39, 89–93. [Google Scholar] [CrossRef]
- Mohammadi, S.; Asghari, G.; Emami-Naini, A.; Mansourian, M.; Badri, S. Herbal Supplement Use and Herb-drug Interactions among Patients with Kidney Disease. J. Res. Pharm. Pract. 2020, 9, 61–67. [Google Scholar] [CrossRef]
- Mahmoodpoor, F.; Rahbar Saadat, Y.; Barzegari, A.; Ardalan, M.; Zununi Vahed, S. The impact of gut microbiota on kidney function and pathogenesis. Biomed. Pharmacother. Biomed. Pharmacother. 2017, 93, 412–419. [Google Scholar] [CrossRef]
- Feng, Z.; Wang, T.; Dong, S.; Jiang, H.; Zhang, J.; Raza, H.K.; Lei, G. Association between gut dysbiosis and chronic kidney disease: A narrative review of the literature. J. Int. Med. Res. 2021, 49, 3000605211053276. [Google Scholar] [CrossRef]
- Kim, M.G.; Yang, J.; Jo, S.K. Intestinal microbiota and kidney diseases. Kidney Res. Clin. Pract. 2021, 40, 335–343. [Google Scholar] [CrossRef]
- Yang, J.; Lim, S.Y.; Ko, Y.S.; Lee, H.Y.; Oh, S.W.; Kim, M.G.; Cho, W.Y.; Jo, S.K. Intestinal barrier disruption and dysregulated mucosal immunity contribute to kidney fibrosis in chronic kidney disease. Nephrol Dial Transpl. 2019, 34, 419–428. [Google Scholar] [CrossRef]
- Ramezani, A.; Raj, D.S. The gut microbiome, kidney disease, and targeted interventions. J. Am. Soc. Nephrol. 2014, 25, 657–670. [Google Scholar] [CrossRef]
- Wang, I.K.; Yen, T.H.; Hsieh, P.S.; Ho, H.H.; Kuo, Y.W.; Huang, Y.Y.; Kuo, Y.L.; Li, C.Y.; Lin, H.C.; Wang, J.Y. Effect of a Probiotic Combination in an Experimental Mouse Model and Clinical Patients with Chronic Kidney Disease: A Pilot Study. Front. Nutr. 2021, 8, 661794. [Google Scholar] [CrossRef]
- Zhu, H.; Cao, C.; Wu, Z.; Zhang, H.; Sun, Z.; Wang, M.; Xu, H.; Zhao, Z.; Wang, Y.; Pei, G.; et al. The probiotic L. casei Zhang slows the progression of acute and chronic kidney disease. Cell Metab. 2021, 33, 1926–1942. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Johnson, D.W.; Morrison, M.; Pascoe, E.M.; Coombes, J.S.; Forbes, J.M.; Szeto, C.C.; McWhinney, B.C.; Ungerer, J.P.; Campbell, K.L. Synbiotics Easing Renal Failure by Improving Gut Microbiology (SYNERGY): A Randomized Trial. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, A.; Zarrati Mojarrad, M.; Bahmani, F.; Taghizadeh, M.; Ramezani, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Esmaillzadeh, A.; Asemi, Z. Probiotic supplementation in diabetic hemodialysis patients has beneficial metabolic effects. Kidney Int. 2017, 91, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Yang, J.; Ji, G.E.; Park, M.S.; Seong, Y.; Oh, S.W.; Kim, M.G.; Cho, W.Y.; Jo, S.K. The effect of probiotic supplementation on systemic inflammation in dialysis patients. Kidney Res. Clin. Pract. 2022, 41, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Jhee, J.H.; Kee, Y.K.; Park, S.; Kim, H.; Park, J.T.; Han, S.H.; Kang, S.W.; Yoo, T.H. High-protein diet with renal hyperfiltration is associated with rapid decline rate of renal function: A community-based prospective cohort study. Nephrol. Dial. Transplant. 2020, 35, 98–106. [Google Scholar] [CrossRef]
- Vukovic, V.; Hantikainen, E.; Raftopoulou, A.; Gögele, M.; Rainer, J.; Domingues, F.S.; Pramstaller, P.P.; Garcia-Larsen, V.; Pattaro, C. Association of dietary proteins with serum creatinine and estimated glomerular filtration rate in a general population sample: The CHRIS study. J. Nephrol. 2022, 36, 103–114. [Google Scholar] [CrossRef]
- Kim, E.; Chung, S.; Hwang, J.-T.; Park, Y.J. 2020 Korean Dietary Reference Intakes for Protein: Estimation of protein requirements and the status of dietary protein intake in the Korean population. J. Nutr. Health 2022, 55, 10–20. [Google Scholar] [CrossRef]
- Ko, G.J.; Obi, Y.; Tortorici, A.R.; Kalantar-Zadeh, K. Dietary protein intake and chronic kidney disease. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Oba, R.; Kanzaki, G.; Sasaki, T.; Okabayashi, Y.; Haruhara, K.; Koike, K.; Kobayashi, A.; Yamamoto, I.; Tsuboi, N.; Yokoo, T. Dietary Protein Intake and Single-Nephron Glomerular Filtration Rate. Nutrients 2020, 12, 2549. [Google Scholar] [CrossRef]
- Nunes, S.; Vieira, P.; Gomes, P.; Viana, S.D.; Reis, F. Blueberry as an Attractive Functional Fruit to Prevent (Pre)Diabetes Progression. Antioxidants 2021, 10, 1162. [Google Scholar] [CrossRef] [PubMed]
- El Morsy, E.M.; Ahmed, M.A.; Ahmed, A.A. Attenuation of renal ischemia/reperfusion injury by açaí extract preconditioning in a rat model. Life Sci. 2015, 123, 35–42. [Google Scholar] [CrossRef]
- Nair, A.R.; Elks, C.M.; Vila, J.; Del Piero, F.; Paulsen, D.B.; Francis, J. A blueberry-enriched diet improves renal function and reduces oxidative stress in metabolic syndrome animals: Potential mechanism of TLR4-MAPK signaling pathway. PLoS ONE 2014, 9, e111976. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Sun, Z.; Zeng, Y.; Luo, M.; Yang, J. Molecular Mechanism and Health Role of Functional Ingredients in Blueberry for Chronic Disease in Human Beings. Int. J. Mol. Sci. 2018, 19, 2785. [Google Scholar] [CrossRef] [PubMed]
- Belmonte-Herrera, B.H.; Domínguez-Avila, J.A.; Wall-Medrano, A.; Ayala-Zavala, J.F.; Preciado-Saldaña, A.M.; Salazar-López, N.J.; López-Martínez, L.X.; Yahia, E.M.; Robles-Sánchez, R.M.; González-Aguilar, G.A. Lesser-Consumed Tropical Fruits and Their by-Products: Phytochemical Content and Their Antioxidant and Anti-Inflammatory Potential. Nutrients 2022, 14, 3663. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Yu, E.Y.T.; Chan, L.; Mok, A.H.Y.; Wang, Y.; Chan, E.W.Y.; Wong, I.C.K.; Lam, C.L.K. Comparative Risks of Nonsteroidal Anti-Inflammatory Drugs on CKD. Clin. J. Am. Soc. Nephrol. CJASN 2021, 16, 898–907. [Google Scholar] [CrossRef]
- Gooch, K.; Culleton, B.F.; Manns, B.J.; Zhang, J.; Alfonso, H.; Tonelli, M.; Frank, C.; Klarenbach, S.; Hemmelgarn, B.R. NSAID use and progression of chronic kidney disease. Am. J. Med. 2007, 120, 280.e281–e287. [Google Scholar] [CrossRef]
- Are Berries High in Potassium? Available online: https://tastylicious.com/berries-potassium/ (accessed on 17 December 2022).
- Kovesdy, C.P.; Matsushita, K.; Sang, Y.; Brunskill, N.J.; Carrero, J.J.; Chodick, G.; Hasegawa, T.; Heerspink, H.L.; Hirayama, A.; Landman, G.W.D.; et al. Serum potassium and adverse outcomes across the range of kidney function: A CKD Prognosis Consortium meta-analysis. Eur. Heart J. 2018, 39, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Inaba, M. Potassium Metabolism and Management in Patients with CKD. Nutrients 2021, 13, 1751. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Non-Dietary Supplement Users (n = 10,519) | Dietary Supplements Users (n = 2752) | p | |||
|---|---|---|---|---|---|
| n (or MEAN) | % (or STD) | n (or MEAN) | % (or STD) | ||
| Sex | <0.0001 | ||||
| Male | 4744 | (45.10) | 1051 | (38.19) | |
| Female | 5775 | (54.90) | 1701 | (61.81) | |
| Age | 50.63 | ±17.26 | 53.73 | ±15.68 | <0.0001 † |
| BMI | 23.97 | ±3.61 | 23.85 | ±3.38 | 0.112 |
| Education | <0.0001 | ||||
| Less than elementary school graduation | 2280 | (23.00) | 580 | (22.14) | |
| Middle School graduation | 998 | (10.07) | 277 | (10.57) | |
| High School graduation | 3221 | (32.50) | 750 | (28.63) | |
| College graduate or higher | 3412 | (34.43) | 1013 | (38.66) | |
| Smoking status | <0.0001 | ||||
| Smoker | 1943 | (18.81) | 351 | (12.94) | |
| Ex-smoker | 2241 | (21.69) | 573 | (21.12) | |
| Non-smoker | 6148 | (59.50) | 1789 | (65.94) | |
| Drinking status | <0.0001 | ||||
| Never | 1220 | (11.80) | 341 | (12.56) | |
| Less than once a month | 3438 | (33.25) | 1002 | (36.89) | |
| 1–4 times a month | 3341 | (32.31) | 867 | (31.92) | |
| ≥5 times a month | 2341 | (22.64) | 506 | (18.63) | |
| Physical activity | 0.311 | ||||
| <2 days/week | 9097 | (91.70) | 2391 | (91.09) | |
| ≥2 days/week | 823 | (8.30) | 234 | (8.91) | |
| Diabetes | 0.843 | ||||
| No | 9319 | (90.33) | 2439 | (90.20) | |
| Yes | 998 | (9.67) | 265 | (9.80) | |
| Hypertension | <0.0001 | ||||
| No | 7845 | (76.02) | 1957 | (72.35) | |
| Yes | 2474 | (23.98) | 748 | (27.65) | |
| CKD | 0.851 | ||||
| No | 9940 | (94.50) | 2598 | (94.40) | |
| Yes | 579 | (5.50) | 154 | (5.60) | |
| SBP | 119.06 | ±16.95 | 118.95 | ±16.74 | 0.762 |
| DBP | 75.19 | ±10.20 | 74.76 | ±9.96 | 0.048 |
| Cr | 0.84 | ±0.36 | 0.82 | ±0.26 | 0.001 † |
| FBG | 101.69 | ±26.69 | 101.15 | ±24.15 | 0.541 † |
| TG | 136.70 | ±116.63 | 133.19 | ±95.17 | 0.216 † |
| CKD (n = 733) | No CKD (n = 12,538) | ||||
|---|---|---|---|---|---|
| n | % | n | % | p | |
| Aloe | >0.999 | ||||
| Yes | 0 | (0.00) | 5 | (100.00) | |
| No | 733 | (5.53) | 12533 | (94.47) | |
| Amino acids and Protein | 0.031 | ||||
| Yes | 4 | (18.18) | 18 | (81.82) | |
| No | 729 | (5.50) | 12,520 | (94.50) | |
| Chlorella/Spirulina | 0.696 | ||||
| Yes | 2 | (6.25) | 30 | (93.75) | |
| No | 731 | (5.52) | 12,508 | (94.48) | |
| Gamma-linolenic acid | >0.999 | ||||
| Yes | 0 | (0.00) | 14 | (100.00) | |
| No | 733 | (5.53) | 12,524 | (94.47) | |
| Ginseng and Red ginseng | 0.009 | ||||
| Yes | 21 | (9.55) | 199 | (90.45) | |
| No | 712 | (5.46) | 12,339 | (94.54) | |
| Glucosamine | 0.549 | ||||
| Yes | 1 | (7.14) | 13 | (92.86) | |
| No | 732 | (5.52) | 12,525 | (94.48) | |
| Herbal medicine (plant extract) Asian | 0.720 | ||||
| Yes | 2 | (5.71) | 33 | (94.29) | |
| No | 731 | (5.52) | 12,505 | (94.48) | |
| Herbal medicine (plant extract) Berry | 0.046 | ||||
| Yes | 3 | (20.00) | 12 | (80.00) | |
| No | 730 | (5.51) | 12,526 | (94.49) | |
| Herbal medicine (plant extract) Ginkgo Biloba | >0.999 | ||||
| Yes | 0 | (0.00) | 12 | (100.00) | |
| No | 733 | (5.53) | 12,526 | (94.47) | |
| Herbal medicine (plant extract) Others | 0.378 | ||||
| Yes | 1 | (1.72) | 57 | (98.28) | |
| No | 732 | (5.54) | 12,481 | (94.46) | |
| Lutein containing supplements | 0.689 | ||||
| Yes | 2 | (6.45) | 29 | (93.55) | |
| No | 731 | (5.52) | 12,509 | (94.48) | |
| Methyl Sulfonyl Methane | >0.999 | ||||
| Yes | 0 | (0.00) | 5 | (100.00) | |
| No | 733 | (5.53) | 12,533 | (94.47) | |
| Milk thistle | 0.262 | ||||
| Yes | 0 | (0.00) | 35 | (100.00) | |
| No | 733 | (5.54) | 12,503 | (94.46) | |
| Omega-3 fatty acid | 0.050 | ||||
| Yes | 26 | (7.98) | 300 | (92.02) | |
| No | 707 | (5.46) | 12,238 | (94.54) | |
| Probiotics (pre-, post-) | 0.017 | ||||
| Yes | 1 | (0.77) | 129 | (99.23) | |
| No | 732 | (5.57) | 12,409 | (94.43) | |
| Propolis | >0.999 | ||||
| Yes | 1 | (4.00) | 24 | (96.00) | |
| No | 732 | (5.53) | 12,514 | (94.47) | |
| Vitamin and Mineral | 0.470 | ||||
| Yes | 87 | (5.15) | 1603 | (94.85) | |
| No | 646 | (5.58) | 10,935 | (94.42) | |
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Amino acids and Protein | 3.817 | (1.288–11.306) | 0.016 | 2.199 | (0.699–6.915) | 0.178 | 2.291 | (0.723–7.257) | 0.159 |
| Ginseng and Red ginseng | 1.829 | (1.159–2.886) | 0.010 | 1.338 | (0.825–2.169) | 0.238 | 1.35 | (0.817–2.232) | 0.241 |
| Herbal medicine (plant extract) Berry | 4.290 | (1.208–15.235) | 0.024 | 4.598 | (1.123–18.821) | 0.034 | 4.809 | (1.077–21.473) | 0.040 |
| Probiotics (pre-, post-) | 0.132 | (0.018–0.941) | 0.043 | 0.207 | (0.028–1.510) | 0.120 | 0.237 | (0.032–1.741) | 0.157 |
| Omega-3 fatty acid | 1.500 | (0.998–2.256) | 0.051 | 1.015 | (0.666–1.547) | 0.945 | 1.019 | (0.655–1.584) | 0.933 |
| Chlorella/Spirulina | 1.141 | (0.272–4.783) | 0.857 | 1.186 | (0.262–5.364) | 0.825 | 1.151 | (0.244–5.420) | 0.859 |
| Glucosamine | 1.317 | (0.172–10.076) | 0.791 | 0.528 | (0.067–4.187) | 0.546 | 0.591 | (0.074–4.723) | 0.620 |
| Herbal medicine (plant extract) Asian | 1.037 | (0.249–4.330) | 0.960 | 0.820 | (0.188–3.585) | 0.792 | 1.121 | (0.254–4.940) | 0.880 |
| Herbal medicine (plant extract) Others | 0.300 | (0.042–2.164) | 0.233 | 0.628 | (0.085–4.630) | 0.648 | 0.759 | (0.102–5.625) | 0.787 |
| Lutein containing supplements | 1.180 | (0.281–4.956) | 0.821 | 1.287 | (0.287–5.769) | 0.741 | 1.424 | (0.292–6.939) | 0.662 |
| Propolis | 0.713 | (0.096–5.273) | 0.740 | 0.879 | (0.110–7.008) | 0.903 | 1.233 | (0.151–10.073) | 0.845 |
| Vitamin and Mineral | 0.919 | (0.730–1.156) | 0.470 | 0.907 | (0.714–1.153) | 0.426 | 0.980 | (0.762–1.260) | 0.874 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, Y.; Lee, H.; Son, S.; Oh, S.; Jo, S.-K.; Cho, W.; Kim, M.-G. Association between Consumption of Dietary Supplements and Chronic Kidney Disease Prevalence: Results of the Korean Nationwide Population-Based Survey. Nutrients 2023, 15, 822. https://doi.org/10.3390/nu15040822
Fang Y, Lee H, Son S, Oh S, Jo S-K, Cho W, Kim M-G. Association between Consumption of Dietary Supplements and Chronic Kidney Disease Prevalence: Results of the Korean Nationwide Population-Based Survey. Nutrients. 2023; 15(4):822. https://doi.org/10.3390/nu15040822
Chicago/Turabian StyleFang, Yina, Hwasun Lee, Serhim Son, Sewon Oh, Sang-Kyung Jo, Wonyong Cho, and Myung-Gyu Kim. 2023. "Association between Consumption of Dietary Supplements and Chronic Kidney Disease Prevalence: Results of the Korean Nationwide Population-Based Survey" Nutrients 15, no. 4: 822. https://doi.org/10.3390/nu15040822
APA StyleFang, Y., Lee, H., Son, S., Oh, S., Jo, S.-K., Cho, W., & Kim, M.-G. (2023). Association between Consumption of Dietary Supplements and Chronic Kidney Disease Prevalence: Results of the Korean Nationwide Population-Based Survey. Nutrients, 15(4), 822. https://doi.org/10.3390/nu15040822