
Gastric Emptying of New-World Milk Containing A1 and A2 Β-Casein Is More Rapid as Compared to Milk Containing Only A2 Β-Casein in Lactose Maldigesters: A Randomized, Cross-Over Trial Using Magnetic Resonance Imaging




Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Enrolment, Allocation and Inclusion Criteria
2.2. Exclusion Criteria
2.3. Intervention
2.4. Nutrient Analysis
2.4.1. Analysis of A1 β-Casein/A2 β-Casein Using Liquid Chromatograph Triple Quadrupole Mass Spectrometer (LC-MS/MS)
2.4.2. Sugar Analysis
2.4.3. Protein Analysis
2.4.4. Fat Analysis
2.5. Study Procedure
2.6. Study Ethics
2.7. Image Analysis
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Nutrient Analysis
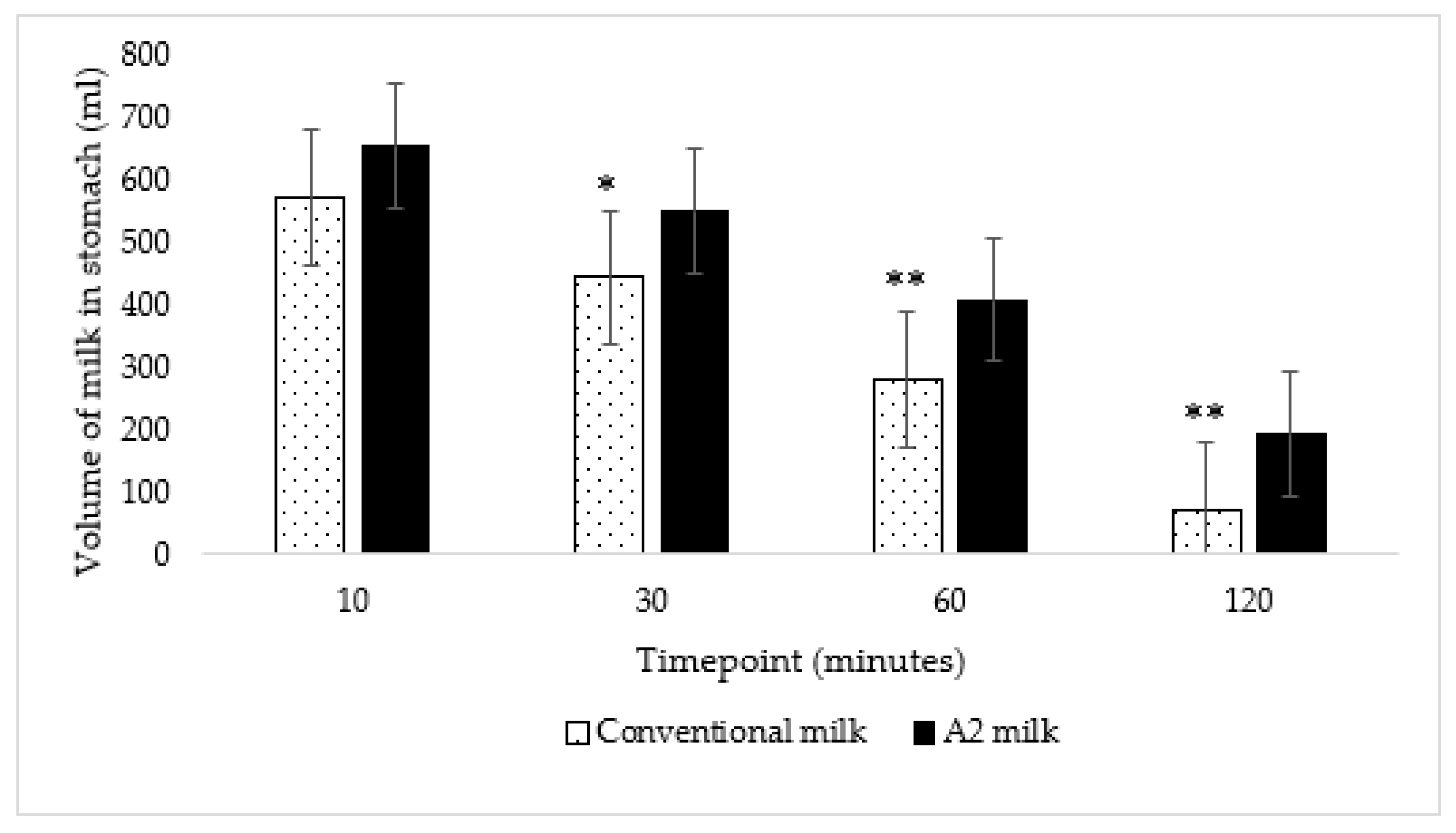
3.3. Gastric Emptying and Transit Volume
3.4. Abdominal Pain
3.5. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Inclusion and Exclusion Criteria for Phone Screening
- Inclusion Criteria:
- Ability/desire to provide informed consent
- Aged 18 to 65 years inclusive at screening
- Milk intolerant and identified as a lactose maldigester while participating in the Milk Protein Study (applicable only for subjects from the previous milk protein study and not applicable for new subjects)
- Current or recent history of intolerance to or avoidance of dairy of at least one month duration (by self-report and self-reported symptoms)
- Willing to return for all study visits and complete all study related procedures
- Able to understand and provide written informed consent in English
- Exclusion Criteria:
- Currently pregnant
- Diagnosed with any of the following disorders known to be associated with abnormal gastrointestinal motility such as gastroparesis, amyloidosis, neuromuscular diseases (including Parkinson’s disease), collagen vascular diseases, alcoholism, uremia, malnutrition or untreated hypothyroidism
- History of surgery that alters the normal function of the gastrointestinal tract including, but not limited to, gastrointestinal bypass surgery, bariatric surgery, gastric banding, vagotomy, fundoplication or pyloroplasty [Note: history of uncomplicated abdominal surgeries such as removal of an appendix more than 12 months prior to screening will not be excluded]
- Past or present: Organ transplant, chronic pancreatitis, pancreatic insufficiency, symptomatic biliary disease, Celiac disease, chronic constipation, diverticulosis, inflammatory bowel disease (IBD), ulcerative colitis (UC), Crohn’s disease (CD), small intestine bacterial overgrowth syndrome (SIBO), gastroparesis, gastro-esophageal reflux disease (GERD), Irritable Bowel Syndrome (IBS) or any other medical condition with symptoms that could confound collection of adverse events
- Active ulcers or history of severe ulcers
- Diabetes mellitus (type 1 and type 2)
- Congestive Heart Failure (CHF)
- Human Immunodeficiency Virus (HIV), Hepatitis B or Hepatitis C
- Recent use of systemic antibiotics, defined as use within 30 days prior to screening
- Any of the following: Worked with metal (grinding, fabrication, etc.) or had an injury to the eye involving a metallic object, e.g., metallic slivers, foreign body, been injured by a metallic object that may NOT have been completely removed (e.g., bullets, shrapnel, BBs), had a reaction to a contrast medium used for MRI or CT, have claustrophobia (fear of closed places), been diagnosed with epilepsy/seizure, any reason for being unable to remain still for long periods of time, cardiac pacemaker, any type of prosthesis (eye, penile), implanted cardiac defibrillator, heart valve prosthesis/stents, aneurysm clip, shunt (spinal/intraventricular), neuro or bone stimulator, wire sutures or surgical staples, insulin or infusion pump, bone/joint pin, screw, nail, plate, implanted drug infusion device, body tattoos, cochlear, otologic or ear implant, tattooed makeup (eyeliner, lip, etc.), prostate radiation seeds, breast tissue expander, IUD (intrauterine device), hearing aids, transdermal medicine patch (Nitro), body piercing(s), any metallic implants or objects or any other reason the participant thinks they would not be a good candidate for MRI
- Any other conditions/issues noted by the study staff and/or principal investigator that would impact participation and/or protocol compliance
References
- Pal, S.; Woodford, K.; Kukuljan, S.; Ho, S. Milk Intolerance, Beta-Casein and Lactose. Nutrients 2015, 7, 7285–7297. [Google Scholar] [CrossRef]
- Phelan, M.; Aherne, A.; FitzGerald, R.J.; O’Brien, N.M. Casein-derived bioactive peptides: Biological effects, industrial uses, safety aspects and regulatory status. Int. Dairy J. 2009, 19, 643–654. [Google Scholar] [CrossRef]
- Kamiński, S.; Cieslińska, A.; Kostyra, E. Polymorphism of bovine beta-casein and its potential effect on human health. J. Appl. Genet. 2007, 48, 189–198. [Google Scholar] [CrossRef]
- Parashar, A.; Saini, R. A1 milk and its controversy-a review. Int. J. Bioassays 2015, 4, 4611–4619. [Google Scholar]
- Sridharan, P.; Chidananda, B.L. The Science of A2 Beta Casein—A Critical Review of Global Data and Outcomes of Indian Study. Indian J. Nutr. 2020, 7, 212. [Google Scholar]
- Formaggioni, P.; Summer, A.; Malacarne, M.; Mariani, P. Milk protein polymorphism: Detection and diffusion of the genetic variants in Bos genus. Ann. Fac. Med. Vet. Univ. Parma. 1999, 19, 127–165. [Google Scholar]
- Noni, I.D. Release of β-casomorphins 5 and 7 during simulated gastro-intestinal digestion of bovine β-casein variants and milk-based infant formulas. Food Chem. 2008, 110, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Noni, I.D.; Cattaneo, S. Occurrence of β-casomorphins 5 and 7 in commercial dairy products and in their digests following in vitro simulated gastrointestinal digestion. Food Chem. 2010, 119, 560–566. [Google Scholar] [CrossRef]
- He, M.; Sun, J.; Jiang, Z.Q.; Yang, Y.X. Effects of cow’s milk beta-casein variants on symptoms of milk intolerance in Chinese adults: A multicentre, randomised controlled study. Nutr. J. 2017, 16, 72. [Google Scholar] [CrossRef]
- Ho, S.; Woodford, K.; Kukuljan, S.; Pal, S. Comparative effects of A1 versus A2 beta-casein on gastrointestinal measures: A blinded randomised cross-over pilot study. Eur. J. Clin. Nutr. 2014, 68, 994–1000. [Google Scholar] [CrossRef]
- Jianqin, S.; Leiming, X.; Lu, X.; Yelland, G.W.; Ni, J.; Clarke, A.J. Effects of milk containing only A2 beta casein versus milk containing both A1 and A2 beta casein proteins on gastrointestinal physiology, symptoms of discomfort, and cognitive behavior of people with self-reported intolerance to traditional cows’ milk. Nutr J. 2016, 15, 35. [Google Scholar] [CrossRef]
- Sheng, X.; Li, Z.; Ni, J.; Yelland, G. Effects of Conventional Milk Versus Milk Containing Only A2 β-Casein on Digestion in Chinese Children: A Randomized Study. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 375–382. [Google Scholar] [CrossRef]
- Ramakrishnan, M.; Eaton, T.K.; Sermet, O.M.; Savaiano, D.A. Milk Containing A2 β-Casein ONLY, as a Single Meal, Causes Fewer Symptoms of Lactose Intolerance than Milk Containing A1 and A2 β-Caseins in Subjects with Lactose Maldigestion and Intolerance: A Randomized, Double-Blind, Crossover Trial. Nutrients 2020, 12, 3855. [Google Scholar] [CrossRef]
- Milan, A.M.; Shrestha, A.; Karlström, H.J.; Martinsson, J.A.; Nilsson, N.J.; Perry, J.K.; Day, L.; Barnett, M.P.G.; Cameron-Smith, D. Comparison of the impact of bovine milk β-casein variants on digestive comfort in females self-reporting dairy intolerance: A randomized controlled trial. Am. J. Clin. Nutr. 2020, 111, 149–160. [Google Scholar] [CrossRef]
- Santiago-Maldonado, I.M.; Phillips, W.T. Frequent occurrence of rapid as well as delayed gastric emptying of a corn flakes and milk meal in clinical patients with gastrointestinal symptoms. Clin. Nucl. Med. 2007, 32, 186–193. [Google Scholar] [CrossRef]
- Cifuentes, J.D.G.; Laique, S.N.; Dornblaser, D.W.; Gabbard, S. Prevalence and Clinical Features of Rapid Gastric Emptying. Am. J. Gastroenterol. 2017, 112, S233–S234. [Google Scholar] [CrossRef]
- de Zwart, I.M.; de Roos, A. MRI for the evaluation of gastric physiology. Eur. Radiol. 2010, 20, 2609–2616. [Google Scholar] [CrossRef]
- Bertoli, D.; Steinkohl, E.; Mark, E.B.; Brock, C.; Drewes, A.M.; Frøkjaer, J.B. Quantification of gastric emptying with magnetic resonance imaging in healthy volunteers: A systematic review. Neurogastroenterol. Motil. 2022, e14371. [Google Scholar] [CrossRef] [PubMed]
- Suarez, F.L.; Savaiano, D.A.; Levitt, M.D. A comparison of symptoms after the consumption of milk or lactose-hydrolyzed milk by people with self-reported severe lactose intolerance. N. Engl. J. Med. 1995, 333, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Mason, B.S.; Slover, H.T. A Gas Chromatographic Method for the Determination of Sugars in Foods. J. Agric. Food Chem. 1971, 19, 551–554. [Google Scholar] [CrossRef]
- Brobst, K.M. Gas-Liquid Chromatography of Trimethylsilyl Derivatives. Methods Carbohydr. Chem. 1972, 6, 3–8. [Google Scholar]
- Official Methods of Analysis of AOAC INTERNATIONAL, 18th ed.; Methods 968.06 and 992.15; AOAC INTERNATIONAL: Gaithersburg, MD, USA, 2005.
- Official Methods of Analysis of AOAC INTERNATIONAL, 18th ed.; Methods 989.05, 932.05, 986.25, 945.48B; AOAC INTERNATIONAL: Gaithersburg, MD, USA, 2005.
- Declaration of Helsinki 2008. World Medical Association. Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/doh-oct2008/ (accessed on 15 January 2023).
- Dixon, J.R., Jr. The International Conference on Harmonization Good Clinical Practice guideline. Qual. Assur. 1998, 6, 65–74. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Woolrich, M.W.; Beckmann, C.F.; Behrens, T.E.; Johansen-Berg, H.; Bannister, P.R.; De Luca, M.; Drobnjak, I.; Flitney, D.E.; et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 2004, 23, S208–S219. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.D.; Thompson, D.G.; McIntyre, A.; Burnham, W.R.; Walker, E. Effect of codeine and loperamide on upper intestinal transit and absorption in normal subjects and patients with postvagotomy diarrhoea. Gut 1988, 29, 312–318. [Google Scholar] [CrossRef]
- Keller, J.; Layer, P. The Pathophysiology of Malabsorption. Viszeralmedizin 2014, 30, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.P.; McNabb, W.C.; Roy, N.C.; Woodford, K.B.; Clarke, A.J. Dietary A1 β-casein affects gastrointestinal transit time, dipeptidyl peptidase-4 activity, and inflammatory status relative to A2 β-casein in Wistar rats. Int. J. Food Sci. Nutr. 2014, 65, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Brantl, V.; Teschemacher, H.; Bläsig, J.; Henschen, A.; Lottspeich, F. Opioid activities of beta-casomorphins. Life Sci. 1981, 28, 1903–1909. [Google Scholar] [CrossRef] [PubMed]
- Teschemacher, H.; Koch, G.; Brantl, V. Milk protein-derived opioid receptor ligands. Biopolymers 1997, 43, 99–117. [Google Scholar] [CrossRef]
- Teschemacher, H. Opioid receptor ligands derived from food proteins. Curr. Pharm. Des. 2003, 9, 1331–1344. [Google Scholar] [CrossRef]
- Giribaldi, M.; Lamberti, C.; Cirrincione, S.; Giuffrida, M.G.; Cavallarin, L. A2 Milk and BCM-7 Peptide as Emerging Parameters of Milk Quality. Front. Nutr. 2022, 9, 842375. [Google Scholar] [CrossRef]
- Daniel, H.; Vohwinkel, M.; Rehner, G. Effect of casein and beta-casomorphins on gastrointestinal motility in rats. J. Nutr. 1990, 120, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Holzer, P. Opioids and opioid receptors in the enteric nervous system: From a problem in opioid analgesia to a possible new prokinetic therapy in humans. Neurosci. Lett. 2004, 361, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Akbarali, H.I.; Dewey, W.L. Gastrointestinal motility, dysbiosis and opioid-induced tolerance: Is there a link? Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 323–324. [Google Scholar] [CrossRef] [PubMed]
- Peuhkuri, K.; Vapaatalo, H.; Nevala, R.; Korpela, R. Influence of the pharmacological modification of gastric emptying on lactose digestion and gastrointestinal symptoms. Aliment. Pharmacol. Ther. 1999, 13, 81–86. [Google Scholar] [CrossRef]
- Lapides, R.A.; Savaiano, D.A. Gender, Age, Race and Lactose Intolerance: Is There Evidence to Support a Differential Symptom Response? A Scoping Review. Nutrients 2018, 10, 1956. [Google Scholar] [CrossRef]
- Cunningham, K.M.; Daly, J.; Horowitz, M.; Read, N.W. Gastrointestinal adaptation to diets of differing fat composition in human volunteers. Gut 1991, 32, 483–486. [Google Scholar] [CrossRef] [PubMed]
- How to Buy Dairy Products. Prepared by Food Safety and Quality Service. United States Department of Agriculture. Available online: https://naldc.nal.usda.gov/download/CAT87214663/PDF#:~:text=For%20shipment%20in%20interstate%20com,municipality%20where%20it%20is%20sold.&text=Lowfat%20milk%20has%20between%200.5,is%20fortified%20with%20vitamin%20A (accessed on 28 November 2022).
- 2% Reduced Fat Milk. Food Data Central. United States Department of Agriculture. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-details/1872476/nutrients (accessed on 28 November 2022).
- 2% Reduced Fat Milk. Food Data Central. United States Department of Agriculture. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-details/1905877/nutrients (accessed on 28 November 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age, mean (range); years | 27 (19–42) |
| Bodyweight, mean (range); kg | 62 (40–91) |
| Height, mean (range); cm | 164 (150–185) |
| BMI, mean (range); kg/m2 | 23 (18–27) |
| Male/female, n/n | 3/7 |
| Asian | 3 |
| Caucasian | 6 |
| Unknown or not reported | 1 |
| Hispanic | 2 |
| Non-Hispanic | 8 |
| Nutrient | A2 Milk or Old-World Milk | Conventional Milk or New-World Milk |
|---|---|---|
| Protein (g/serving) | 3.14 | 3.30 |
| Fat (g/serving) | 2.10 | 1.90 |
| Lactose (g/serving) | 4.70 | 4.60 |
| Carbohydrate (g/serving) | 4.70 | 4.60 |
| Calories (kcal/serving) | 0.0541 | 0.0500 |
| A1 β-casein protein (%) | 0.00 | 75.00 |
| A2 β-casein protein (%) | 100.00 | 25.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramakrishnan, M.; Zhou, X.; Dydak, U.; Savaiano, D.A. Gastric Emptying of New-World Milk Containing A1 and A2 Β-Casein Is More Rapid as Compared to Milk Containing Only A2 Β-Casein in Lactose Maldigesters: A Randomized, Cross-Over Trial Using Magnetic Resonance Imaging. Nutrients 2023, 15, 801. https://doi.org/10.3390/nu15040801
Ramakrishnan M, Zhou X, Dydak U, Savaiano DA. Gastric Emptying of New-World Milk Containing A1 and A2 Β-Casein Is More Rapid as Compared to Milk Containing Only A2 Β-Casein in Lactose Maldigesters: A Randomized, Cross-Over Trial Using Magnetic Resonance Imaging. Nutrients. 2023; 15(4):801. https://doi.org/10.3390/nu15040801
Chicago/Turabian StyleRamakrishnan, Monica, Xiaopeng Zhou, Ulrike Dydak, and Dennis A. Savaiano. 2023. "Gastric Emptying of New-World Milk Containing A1 and A2 Β-Casein Is More Rapid as Compared to Milk Containing Only A2 Β-Casein in Lactose Maldigesters: A Randomized, Cross-Over Trial Using Magnetic Resonance Imaging" Nutrients 15, no. 4: 801. https://doi.org/10.3390/nu15040801
APA StyleRamakrishnan, M., Zhou, X., Dydak, U., & Savaiano, D. A. (2023). Gastric Emptying of New-World Milk Containing A1 and A2 Β-Casein Is More Rapid as Compared to Milk Containing Only A2 Β-Casein in Lactose Maldigesters: A Randomized, Cross-Over Trial Using Magnetic Resonance Imaging. Nutrients, 15(4), 801. https://doi.org/10.3390/nu15040801