
Emotional Eating and Changes in High-Sugar Food and Drink Consumption Linked to Psychological Distress and Worries: A Cohort Study from Norway
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Characteristics; Design, Population, Data Collection and Study Sample
2.2. Questionnaire
2.3. Study Variables, Baseline, Clinical and Sociodemographic Factors
2.4. Statistical Analyses
2.5. Ethics
3. Results
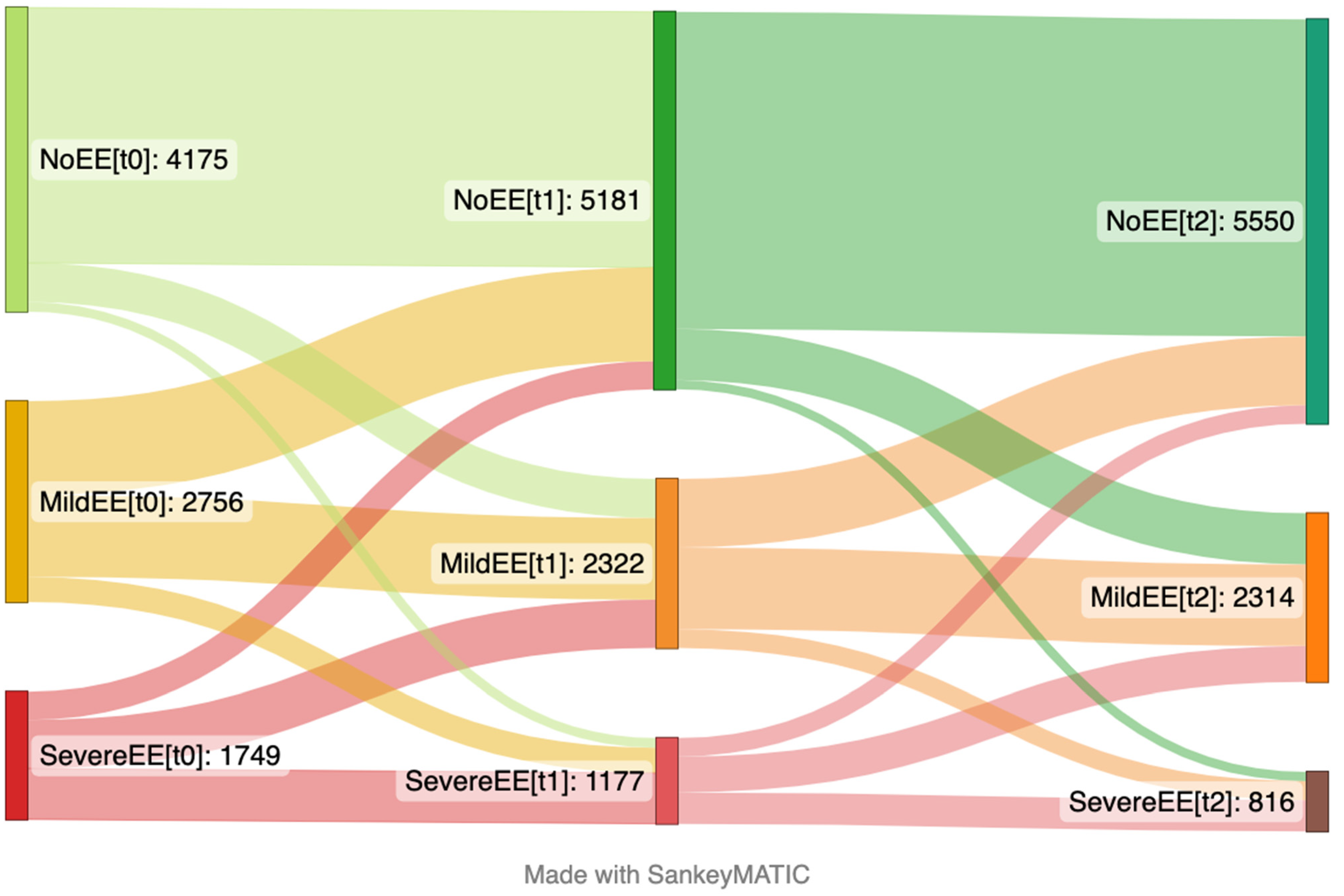
3.1. Emotional Eating at Baseline and over Time
3.2. High-Sugar Food and Drink Intake over Time
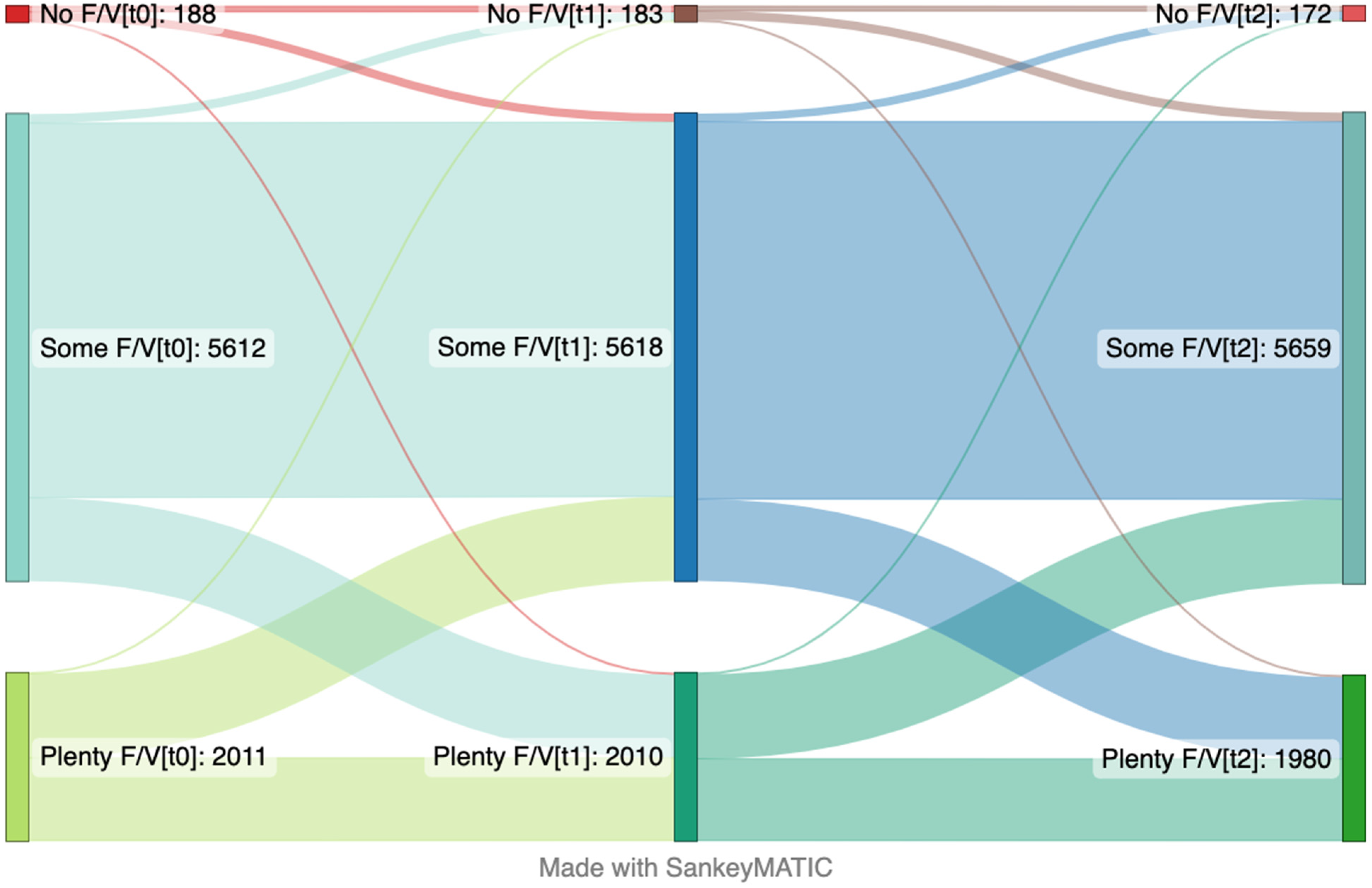
3.3. Servings per Day of Fruits and Vegetables over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Folkman, S.; Lazarus, R.S. Coping as a mediator of emotion. J. Personal. Soc. Psychol. 1988, 54, 466. [Google Scholar] [CrossRef]
- Yeh, M.-L.; Chung, Y.-C.; Hsu, M.-Y.F.; Hsu, C.-C. Quantifying Psychological Distress among Cancer Patients in Interventions and Scales: A Systematic Review. Curr. Pain Headache Rep. 2014, 18, 399. [Google Scholar] [CrossRef]
- Préville, M.; Boyer, R.; Potvin, L.; Perreault, C.; Légaré, G. La Détresse Psychologique: Détermination de la Fiabilité et de la Validité de la Mesure Utilisée dans L’enquête Santé Québec; Santé Québec: Montréal, QC, USA, 1992. [Google Scholar]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed]
- Cecchetto, C.; Aiello, M.; Gentili, C.; Ionta, S.; Osimo, S.A. Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 2021, 160, 105122. [Google Scholar] [CrossRef]
- Awasthi, S.; Ephraim, R. A Cross-Sectional Study on the Correlation between Psychological Distress and Eating Behaviours of Young Adults during the COVID-19 Pandemic. Indian J. Psychiatry 2022, 64 (Suppl. 3), S607. [Google Scholar]
- Lopez-Moreno, M.; Lopez, M.T.I.; Miguel, M.; Garces-Rimon, M. Physical and psychological effects related to food habits and lifestyle changes derived from COVID-19 home confinement in the spanish population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- Caso, D.; Guidetti, M.; Capasso, M.; Cavazza, N. Finally, the chance to eat healthily: Longitudinal study about food consumption during and after the first COVID-19 lockdown in Italy. Food Qual. Prefer. 2022, 95, 104275. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- Lau, J.T.; Yang, X.; Tsui, H.Y.; Kim, J.H. Impacts of SARS on health-seeking behaviors in general population in Hong Kong. Prev. Med. 2005, 41, 454–462. [Google Scholar] [CrossRef]
- Machín, L.; Aschemann-Witzel, J.; Patiño, A.; Moratorio, X.; Bandeira, E.; Curutchet, M.R.; Martínez, J.; Bove, I.; Molina, V.; Giménez, A.; et al. Barriers and Facilitators to Implementing the Uruguayan Dietary Guidelines in Everyday Life: A Citizen Perspective. Health Educ. Behav. 2018, 45, 511–523. [Google Scholar] [CrossRef]
- Vidal, L.; Brunet, G.; Curutchet, M.R.; Girona, A.; Pardiñas, V.; Guerra, D.; Platero, E.; Machado, L.; González, F.; Gugliucci, V.; et al. Is COVID-19 a threat or an opportunity for healthy eating? An exploration of the factors that moderate the impact of the pandemic on eating habits in Uruguay. Appetite 2021, 167, 105651. [Google Scholar] [CrossRef] [PubMed]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Falissard, B. Eating disorders: Interactions between human nutrition research and food behaviours. Trends Food Sci. Technol. 2007, 18, 281–284. [Google Scholar] [CrossRef]
- Barnhart, W.R.; Braden, A.L.; Price, E. Emotion regulation difficulties interact with negative, not positive, emotional eating to strengthen relationships with disordered eating: An exploratory study. Appetite 2021, 158, 105038. [Google Scholar] [CrossRef] [PubMed]
- Yau, Y.H.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar]
- Camilleri, G.M.; Méjean, C.; Kesse-Guyot, E.; Andreeva, V.A.; Bellisle, F.; Hercberg, S.; Péneau, S. The Associations between Emotional Eating and Consumption of Energy-Dense Snack Foods Are Modified by Sex and Depressive Symptomatology. J. Nutr. 2014, 144, 1264–1273. [Google Scholar] [CrossRef]
- Konttinen, H.; Männistö, S.; Sarlio-Lähteenkorva, S.; Silventoinen, K.; Haukkala, A. Emotional eating, depressive symptoms and self-reported food consumption. A population-based study. Appetite 2010, 54, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; King, J.M.; Prinyawiwatkul, W. A review of measurement and relationships between food, eating behavior and emotion. Trends Food Sci. Technol. 2014, 36, 15–28. [Google Scholar] [CrossRef]
- Bemanian, M.; Mæland, S.; Blomhoff, R.; Rabben, Å.K.; Arnesen, E.K.; Skogen, J.C.; Fadnes, L.T. Emotional Eating in Relation to Worries and Psychological Distress Amid the COVID-19 Pandemic: A Population-Based Survey on Adults in Norway. Int. J. Environ. Res. Public Health 2020, 18, 130. [Google Scholar] [CrossRef]
- Al-Musharaf, S. Prevalence and Predictors of Emotional Eating among Healthy Young Saudi Women during the COVID-19 Pandemic. Nutrients 2020, 12, 2923. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Huo, S.; Ma, Y.; Ke, Y.; Wang, P.; Zhao, A. Emotional Eating in Pregnant Women during the COVID-19 Pandemic and Its Association with Dietary Intake and Gestational Weight Gain. Nutrients 2020, 12, 2250. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, H.; Sharps, M.; Cunliffe, L.; van den Tol, A. Eating in the lockdown during the COVID 19 pandemic; Self-reported changes in eating behaviour, and associations with BMI, eating style, coping and health anxiety. Appetite 2021, 161, 105082. [Google Scholar] [CrossRef] [PubMed]
- Cypryańska, M.; Nezlek, J.B. Anxiety as a mediator of relationships between perceptions of the threat of COVID-19 and coping behaviors during the onset of the pandemic in Poland. PLoS ONE 2020, 15, e0241464. [Google Scholar] [CrossRef]
- Bergen I Endring COVID19 Studien—BiE Studien. Available online: https://www.uib.no/igs/135092/bergen-i-endring-covid19-studien-bie-studien# (accessed on 1 December 2021).
- Kvaløy, K.; Melhus, M.; Silviken, A.; Brustad, M.; Sørlie, T.; Broderstad, A.R. Disordered eating in Sami and non-Sami Norwegian populations: The SAMINOR 2 clinical survey. Public Health Nutr. 2018, 21, 1094–1105. [Google Scholar] [CrossRef]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Zierle-Ghosh, A.; Jan, A. Physiology, Body Mass Index. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hill, D.; Conner, M.; Clancy, F.; Moss, R.; Wilding, S.; Bristow, M.; O’Connor, D.B. Stress and eating behaviours in healthy adults: A systematic review and meta-analysis. Health Psychol. Rev. 2022, 16, 280–304. [Google Scholar] [CrossRef]
- Hewagalamulage, S.D.; Lee, T.K.; Clarke, I.J.; Henry, B.A. Stress, cortisol, and obesity: A role for cortisol responsiveness in identifying individuals prone to obesity. Domest. Anim. Endocrinol. 2016, 56, S112–S120. [Google Scholar] [CrossRef]
- Dallman, M.F.; la Fleur, S.E.; Pecoraro, N.C.; Gomez, F.; Houshyar, H.; Akana, S.F. Minireview: Glucocorticoids—Food Intake, Abdominal Obesity, and Wealthy Nations in 2004. Endocrinology 2004, 145, 2633–2638. [Google Scholar] [CrossRef]
- Hannibal, K.E.; Bishop, M.D. Chronic stress, cortisol dysfunction, and pain: A psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys. Ther. 2014, 94, 1816–1825. [Google Scholar] [CrossRef]
- Salazar-Fernandez, C.; Palet, D.; Haeger, P.A.; Mella, F.R. The perceived impact of COVID-19 on comfort food consumption over time: The mediational role of emotional distress. Nutrients 2021, 13, 1910. [Google Scholar] [CrossRef] [PubMed]
- Strand, B.H.; Dalgard, O.S.; Tambs, K.; Rognerud, M. Measuring the mental health status of the Norwegian population: A comparison of the instruments SCL-25, SCL-10, SCL-5 and MHI-5 (SF-36). Nord. J. Psychiatry 2003, 57, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.M.; Norekvål, T.M.; Oterhals, K.; Fadnes, L.T.; Mæland, S.; Pakpour, A.H.; Breivik, K. Psychometric properties of the Norwegian version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2022, 20, 1446–1464. [Google Scholar] [CrossRef] [PubMed]
- Skogen, J.C.; Nilsen, T.S.; Aasan, B.E.V.; Nes, R.B.; Aarø, L.E.; Vedaa, Ø. Fylkeshelseundersøkelsen I Nordland 2020: Framgangsmåte og Utvalgte Resultater; Folkehelseinstituttet: Oslo, Norway, 2020. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Age | 18–30 | 30–40 | 40–50 | 50–60 | 60–70 | 70+ |
|---|---|---|---|---|---|---|
| Female (%) | 2200 (64) | 2530 (60) | 2768 (58) | 2950 (56) | 2133 (50) | 1363 (45) |
| BMI categories * (%) | ||||||
| Underweight | 114 (4) | 58 (1) | 31 (1) | 36 (1) | 38 (1) | 32 (1) |
| Normal | 2038 (64) | 1285 (55) | 1500 (48) | 525 (42) | 43 (39) | 3 (21) |
| Overweight | 739 (23) | 1278 (32) | 1673 (37) | 2103 (43) | 1717 (43) | 1154 (41) |
| Obese | 298 (9) | 516 (13) | 704 (16) | 808 (16) | 553 (14) | 285 (10) |
| Living with ≥1 adult (s) | 2911 (85) | 3415 (81) | 3887 (81) | 4235 (80) | 3044 (72) | 1821 (60) |
| Own children (<18y) in house | 811 (24) | 2595 (61) | 3486 (73) | 1565 (30) | 334 (8) | 247 (8) |
| Educational level | ||||||
| Primary school | 414 (13) | 150 (4) | 182 (4) | 272 (5) | 358 (9) | 375 (13) |
| High school/trade school | 1177 (36) | 773 (19) | 932 (20) | 1604 (31) | 1346 (32) | 959 (32) |
| College/University | 1694 (52) | 3155 (77) | 3510 (76) | 3265 (64) | 2469 (59) | 1661 (55) |
| Employed prior to COVID-19 (%) | 2178 (64) | 3548 (84) | 4175 (87) | 4550 (86) | 2415 (57) | 201 (7) |
| Household income (%) | ||||||
| Low | 1041 (36) | 522 (13) | 462 (10) | 364 (8) | 234 (6) | 314 (13) |
| Medium | 1098 (38) | 1944 (49) | 2259 (51) | 1800 (38) | 1262 (35) | 1204 (50) |
| High | 734 (26) | 1464 (37) | 1678 (38) | 2536 (54) | 2109 (59) | 886 (37) |
| Substantial worries (%) | ||||||
| Economy-related worries | 998 (29) | 514 (22) | 561 (17) | 207 (16) | 12 (10) | <5 (7) |
| Health-related worries | 1889 (55) | 2089 (49) | 2181 (46) | 2507 (48) | 1559 (37) | 887 (29) |
| High psychological distress (%) | 1403 (41) | 1211 (29) | 935 (20) | 823 (16) | 475 (11) | 247 (8) |
| Estimates Presented as Coefficients (with 95% Confidence Intervals) | ||
|---|---|---|
| Fixed Effects | Time Trend (Per Year) | |
| Age | ||
| 18–29 | 0 (reference) | 0 (reference) |
| 30–39 | 0.048 (0.038; 0.058) | −0.015 (−0.024; −0.006) |
| 40–49 | 0.033 (0.023; 0.043) | −0.015 (−0.023; −0.006) |
| 50–59 | 0.024 (0.015; 0.033) | −0.007 (−0.016; 0.001) |
| 60–69 | −0.001 (−0.011; 0.009) | −0.002 (−0.011; 0.006) |
| 70+ | −0.031 (−0.042; −0.020) | 0.014 (0.004; 0.023) |
| Sex | ||
| Male | 0 (reference) | 0 (reference) |
| Female | 0.055 (0.050; 0.061) | −0.021 (−0.025; −0.016) |
| Living with other adult(s) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | −0.02 (−0.03; −0.01) | 0.001 (0.000; 0.018) |
| Living with own children (<18 years of age) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | 0.000 (−0.007; 0.006) | 0.040 (0.034; 0.046) |
| Health-related worries | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | 0.018 (0.013; 0.023) | −0.009 (−0.014; −0.004) |
| Worries related to economy | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | 0.044 (0.037; 0.051) | −0.001 (−0.009; 0.007) |
| Psychological distress (0 = no to 1 = extreme) | 0.63 (0.61; 0.65) | −0.18 (−0.20; −0.17) |
| Estimates Presented as Coefficients (with 95% Confidence Intervals) | ||
|---|---|---|
| Fixed Effects | Time Trend (Per Year) | |
| Age | ||
| 18–29 | 0 (reference) | 0 (reference) |
| 30–39 | −0.033 (−0.043; −0.024) | 0.001 (−0.006; 0.008) |
| 40–49 | −0.062 (−0.071; −0.053) | −0.003 (−0.010; 0.003) |
| 50–59 | −0.105 (−0.114; −0.096) | −0.004 (−0.011; 0.002) |
| 60–69 | −0.139 (−0.148; −0.130) | −0.003 (−0.009; 0.004) |
| 70+ | −0.151(−0.162; −0.141) | 0.004 (−0.003; 0.011) |
| Sex | ||
| Male | 0 (reference) | 0 (reference) |
| Female | −0.020 (−0.025; −0.015) | −0.009 (−0.012; −0.006) |
| Living with other adult(s) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | 0.011 (0.005; 0.016) | −0.003 (−0.010; 0.004) |
| Living with own children (<18 y/o) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | 0.029 (0.023; 0.034) | −0.038 (−0.043; −0.033) |
| Health-related worries | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | 0.004 (0.000; 0.009) | 0.001 (−0.003; 0.005) |
| Worries related to personal economy | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | 0.008 (0.002; 0.014) | 0.004 (−0.002; 0.010) |
| Psychological distress (0 = no to 1 = extreme) | 0.11 (0.10; 0.13) | −0.014 (−0.025; −0.003) |
| Effect Estimates Coefficients (with 95% Confidence Intervals) | ||
|---|---|---|
| Constant/Fixed Effects | Time Trend (Per Year) | |
| Age | ||
| 18–30 | 0 (reference) | 0 (reference) |
| 30–40 | 0.006 (−0.004; 0.016) | 0.007 (−0.002; 0.017) |
| 40–50 | −0.007 (−0.017; 0.003) | 0.009 (−0.001; 0.019) |
| 50–60 | 0.010 (0.000; 0.020) | 0.006 (−0.001; 0.019) |
| 60–70 | 0.030 (0.020; 0.041) | 0.004 (−0.003; 0.013) |
| 70+ | 0.049 (0.037; 0.060) | −0.0005 (−0.011; 0.010) |
| Sex | ||
| Male | 0 (reference) | 0 (reference) |
| Female | 0.045 (0.039; 0.051) | −0.002 (−0.067; 0.030) |
| Living with other adult(s) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | 0.008 (0.001; 0.060) | −0.001 (−0.007; 0.003) |
| Living with own children (<18 years) | ||
| No | 0 (reference) | 0 (reference) |
| Yes | 0.001 (−0.006; 0.008) | −0.005 (−0.012; 0.002) |
| Health-related worries | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | −0.001 (−0.007; 0.005) | 0.002 (−0.003; 0.008) |
| Worries related to personal economy | ||
| None or some | 0 (reference) | 0 (reference) |
| Substantial | 0.011 (0.004; 0.019) | −0.005 (−0.014; 0.004) |
| Psychological distress (0 = no to 1 = extreme) | −0.040 (−0.057; −0.022) | 0.022 (0.006; 0.038) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javadi Arjmand, E.; Bemanian, M.; Vold, J.H.; Skogen, J.C.; Sandal, G.M.; Arnesen, E.K.; Mæland, S.; Fadnes, L.T. Emotional Eating and Changes in High-Sugar Food and Drink Consumption Linked to Psychological Distress and Worries: A Cohort Study from Norway. Nutrients 2023, 15, 778. https://doi.org/10.3390/nu15030778
Javadi Arjmand E, Bemanian M, Vold JH, Skogen JC, Sandal GM, Arnesen EK, Mæland S, Fadnes LT. Emotional Eating and Changes in High-Sugar Food and Drink Consumption Linked to Psychological Distress and Worries: A Cohort Study from Norway. Nutrients. 2023; 15(3):778. https://doi.org/10.3390/nu15030778
Chicago/Turabian StyleJavadi Arjmand, Elaheh, Mitra Bemanian, Jørn Henrik Vold, Jens Christoffer Skogen, Gro Mjeldheim Sandal, Erik K. Arnesen, Silje Mæland, and Lars Thore Fadnes. 2023. "Emotional Eating and Changes in High-Sugar Food and Drink Consumption Linked to Psychological Distress and Worries: A Cohort Study from Norway" Nutrients 15, no. 3: 778. https://doi.org/10.3390/nu15030778
APA StyleJavadi Arjmand, E., Bemanian, M., Vold, J. H., Skogen, J. C., Sandal, G. M., Arnesen, E. K., Mæland, S., & Fadnes, L. T. (2023). Emotional Eating and Changes in High-Sugar Food and Drink Consumption Linked to Psychological Distress and Worries: A Cohort Study from Norway. Nutrients, 15(3), 778. https://doi.org/10.3390/nu15030778