
Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review



Abstract
1. Introduction
2. Methods
2.1. Study Protocol and Guidance
2.2. Databases Searched and Search Strategy
2.3. Study Selection
2.4. Inclusion/Exclusion of Studies
2.5. Strategy for Data Extraction and Synthesis
2.6. Risk of Bias (RoB) Assessment
3. Results
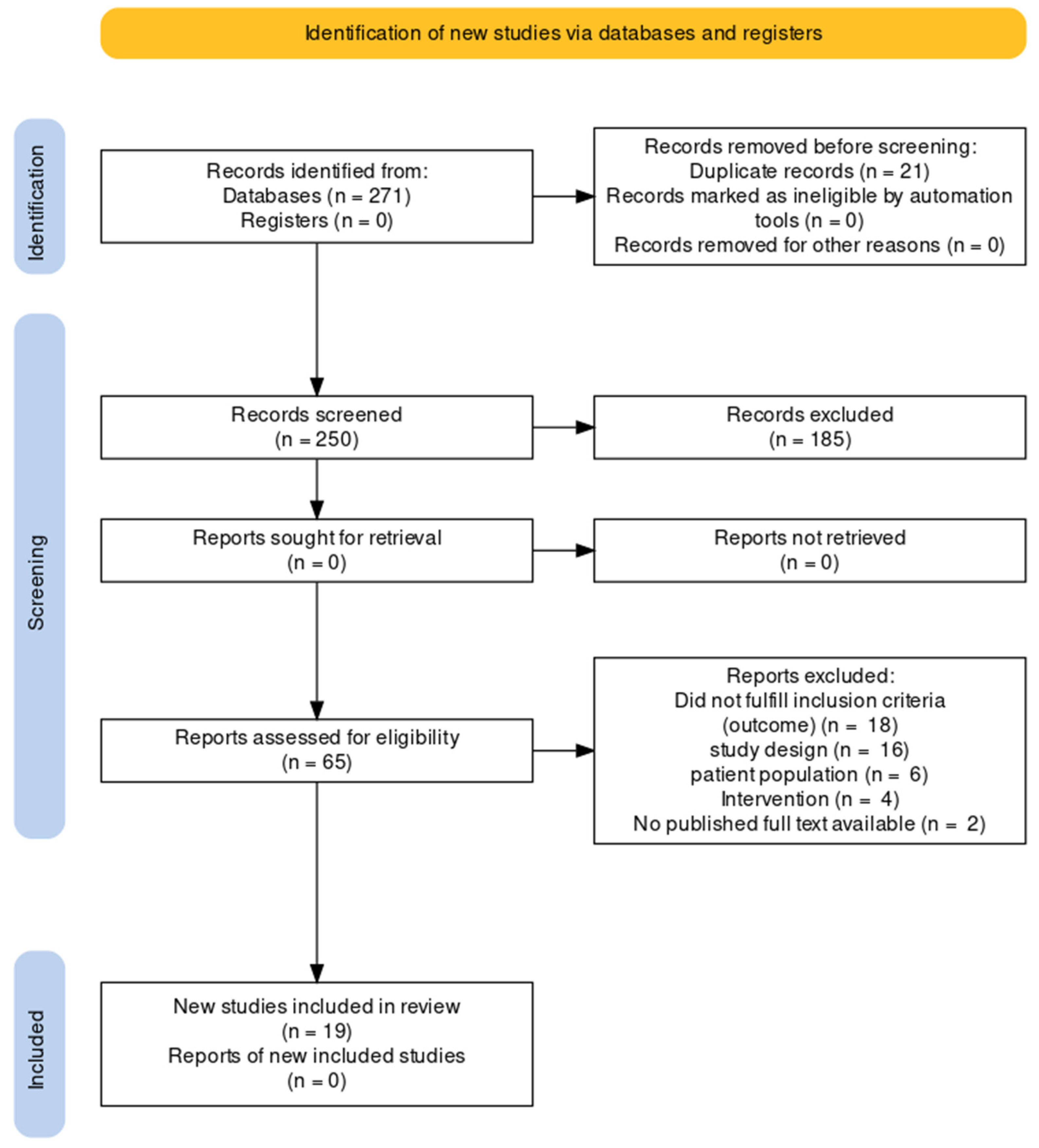
3.1. Search Results
3.2. Study Characteristics
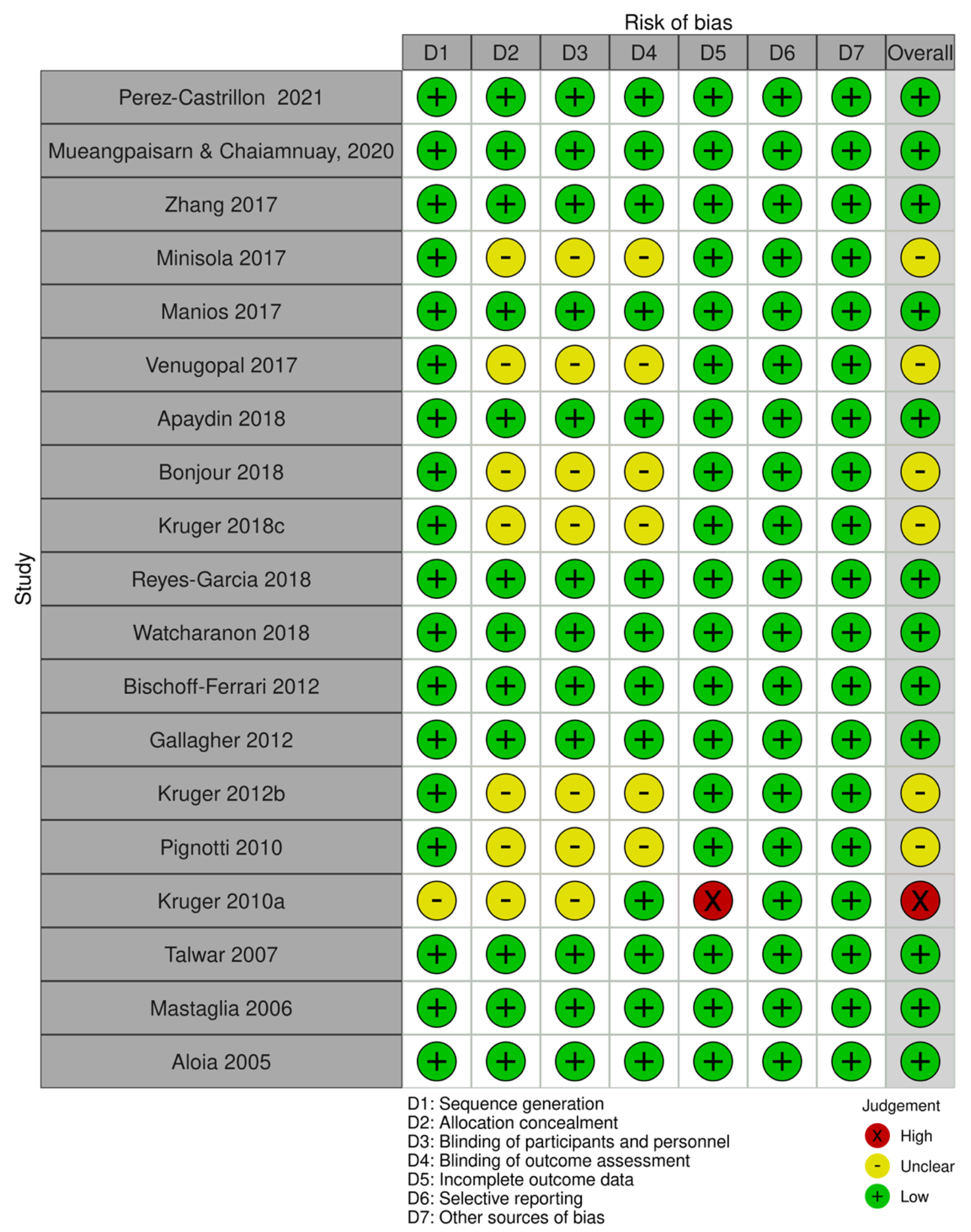
3.3. Risk of Bias
4. Discussion
4.1. The Effect of Treatment Duration and Dose on Vitamin D Status
4.2. The Effects of Type of Vitamin D on Vitamin D Status
4.3. The Effects of Baseline Serum 25(OH)D on Vitamin D Status
4.4. The Effect of Sun Exposure on Vitamin D Status
4.5. The Effect of Lifestyle Habits and Dietary Intake on Vitamin D Status
4.6. Effect of Ethnicity and Genetics
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Lopez-Baena, M.T.; Perez-Roncero, G.; Perez-Lopez, F.; Mezones-Holguin, E.; Chedraui, P. Vitamin D, menopause, and aging: Quo vadis? Climacteric 2020, 23, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Delle Monache, S.; Di Fulvio, P.; Iannetti, E.; Valerii, L.; Capone, L.; Nespoli, M.; Bologna, M.; Angelucci, A. Body mass index represents a good predictor of vitamin D status in women independently from age. Clin. Nutr. 2019, 38, 829–834. [Google Scholar] [CrossRef]
- Feghaly, J.; Johnson, P.; Kalhan, A. Vitamin D and obesity in adults: A pathophysiological and clinical update. Br. J. Hosp. Med. 2020, 81, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Arslanca, T.; Korkmaz, H.; Arslanca, S.; Pehlivanoglu, B.; Celikel, O. The Relationship between Vitamin D and Vasomotor Symptoms During the Postmenopausal Period. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef]
- Riazi, H.; Ghazanfarpour, M.; Taebi, M.; Abdolahian, S. Effect of Vitamin D on the Vaginal Health of Menopausal Women: A Systematic Review. J. Menopausal Med. 2019, 25, 109–116. [Google Scholar] [CrossRef]
- Rad, P.; Tadayon, M.; Abbaspour, M.; Latifi, S.; Rashidi, I.; Delaviz, H. The effect of vitamin D on vaginal atrophy in postmenopausal women. Iran. J. Nurs. Midwifery Res. 2015, 20, 211–215. [Google Scholar]
- Donders, G.G.G.; Ruban, K.; Bellen, G.; Grinceviciene, S. Pharmacotherapy for the treatment of vaginal atrophy. Expert Opin. Pharmacother. 2019, 20, 821–835. [Google Scholar] [CrossRef]
- Jalali-Chimeh, F.; Gholamrezaei, A.; Vafa, M.; Nasiri, M.; Abiri, B.; Darooneh, T.; Ozgoli, G. Effect of Vitamin D Therapy on Sexual Function in Women with Sexual Dysfunction and Vitamin D Deficiency: A Randomized, Double-Blind, Placebo Controlled Clinical Trial. J. Urol. 2019, 201, 987–993. [Google Scholar] [CrossRef]
- Liu, C.; Kuang, X.; Li, K.; Guo, X.; Deng, Q.; Li, D. Effects of combined calcium and vitamin D supplementation on osteoporosis in postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Food Funct. 2020, 11, 10817–10827. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- WHO Scientific Group on the Prevention and Management of Osteoporosis. Prevention and Management of Osteoporosis: Report of a WHO Scientific Group; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Ross, A.C.; Manson, J.; Abrams, S.; Aloia, J.; Brannon, P.; Clinton, S.; Durazo-Arvizu, R.; Gallagher, J.; Gallo, R.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.; Bischoff-Ferrari, H.; Gordon, C.; Hanley, D.; Heaney, R.; Murad, M.; Weaver, C.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Camacho, P.M.; Petak, S.; Binkley, N.; Clarke, B.; Harris, S.; Hurley, D.; Kleerekoper, M.; Lewiecki, E.; Miller, P.; Narula, H.; et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis—2016. Endocr. Pract. 2016, 22 (Suppl. 4), 1111–1118. [Google Scholar] [CrossRef]
- Lips, P.; van Schoor, N.; de Jongh, R. Diet, sun, and lifestyle as determinants of vitamin D status. Ann. N. Y. Acad. Sci. 2014, 1317, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Sollid, S.T.; Hutchinson, M.; Fuskevag, O.; Joakimsen, R.; Jorde, R. Large Individual Differences in Serum 25-Hydroxyvitamin D Response to Vitamin D Supplementation: Effects of Genetic Factors, Body Mass Index, and Baseline Concentration. Results from a Randomized Controlled Trial. Horm. Metab. Res. 2016, 48, 27–34. [Google Scholar] [CrossRef]
- Whiting, S.J.; Bonjour, J.; Payen, F.; Rousseau, B. Moderate amounts of vitamin D3 in supplements are effective in raising serum 25-hydroxyvitamin D from low baseline levels in adults: A systematic review. Nutrients 2015, 7, 2311–2323. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Yalamanchili, V.; Smith, L. The effect of vitamin D supplementation on serum 25(OH)D in thin and obese women. J. Steroid. Biochem. Mol. Biol. 2013, 136, 195–200. [Google Scholar] [CrossRef]
- Heaney, R.P.; Davies, K.; Chen, T.; Holick, M.; Barger-Lux, M. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr. 2003, 77, 204–210. [Google Scholar] [CrossRef]
- Kasahara, A.K.; Singh, R.; Noymer, A. Vitamin D (25OHD) Serum Seasonality in the United States. PLoS ONE 2013, 8, e65785. [Google Scholar] [CrossRef] [PubMed]
- Rees, J.R.; Mott, L.; Barry, E.; Baron, J.; Bostick, R.; Figueiredo, J.; Bresalier, R.; Robertson, D.; Peacock, J. Lifestyle and Other Factors Explain One-Half of the Variability in the Serum 25-Hydroxyvitamin D Response to Cholecalciferol Supplementation in Healthy Adults. J. Nutr. 2016, 146, 2312–2324. [Google Scholar] [CrossRef] [PubMed]
- Didriksen, A.; Grimnes, G.; Hutchinson, M.; Kjaergaard, M.; Svartberg, J.; Joakimsen, R.; Jorde, R. The serum 25-hydroxyvitamin D response to vitamin D supplementation is related to genetic factors, BMI, and baseline levels. Eur. J. Endocrinol. 2013, 169, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Yun, F.; Oczak, M.; Wong, B.; Vieth, R.; Cole, D. Common genetic variants of the vitamin D binding protein (DBP) predict differences in response of serum 25-hydroxyvitamin D [25(OH)D] to vitamin D supplementation. Clin. Biochem. 2009, 42, 1174–1177. [Google Scholar] [CrossRef]
- Nimitphong, H.; Saetung, S.; Chanprasertyotin, S.; Chailurkit, L.; Ongphiphadhanakul, B. Changes in circulating 25-hydroxyvitamin D according to vitamin D binding protein genotypes after vitamin D(3) or D(2)supplementation. Nutr. J. 2013, 12, 39. [Google Scholar] [CrossRef]
- Waterhouse, M.; Tran, B.; Armstrong, B.; Baxter, C.; Ebeling, P.; English, D.; Gebski, V.; Hill, C.; Kimlin, M.; Lucas, R.; et al. Environmental, personal, and genetic determinants of response to vitamin D supplementation in older adults. J. Clin. Endocrinol. Metab. 2014, 99, E1332–E1340. [Google Scholar] [CrossRef]
- Looker, A.C.; Pfeiffer, C.; Lacher, D.; Schleicher, R.; Picciano, M.; Yetley, E. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am. J. Clin. Nutr. 2008, 88, 1519–1527. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Chandler, T.J.; Cumpston, J.; Li, M.; Page, T.; Welch, M.J.; Cochrane, V.A. Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: London, UK, 2022; p. 2022. [Google Scholar]
- Aloia, J.F.; Talwar, S.; Pollack, S.; Yeh, J. A randomized controlled trial of vitamin D3 supplementation in African American women. Arch. Intern. Med. 2005, 165, 1618–1623. [Google Scholar] [CrossRef]
- Apaydin, M.; Can, A.; Kizilgul, M.; Beysel, S.; Kan, S.; Caliskan, M.; Demirci, T.; Ozcelik, O.; Ozbek, M.; Cakal, E. The effects of single high-dose or daily low-dosage oral colecalciferol treatment on vitamin D levels and muscle strength in postmenopausal women. BMC Endocr. Disord. 2018, 18, 48. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Stöcklin, E.; Sidelnikov, E.; Willett, W.; Edel, J.; Stähelin, H.; Wolfram, S.; Jetter, A.; Schwager, J.; et al. Oral supplementation with 25(OH)D3 versus vitamin D3: Effects on 25(OH)D levels, lower extremity function, blood pressure, and markers of innate immunity. J. Bone. Miner. Res. 2012, 27, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, J.P.; Dontot-Payen, F.; Rouy, E.; Walrand, S.; Rousseau, B. Evolution of Serum 25OHD in Response to Vitamin D(3)-Fortified Yogurts Consumed by Healthy Menopausal Women: A 6-Month Randomized Controlled Trial Assessing the Interactions between Doses, Baseline Vitamin D Status, and Seasonality. J. Am. Coll. Nutr. 2018, 37, 34–43. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Sai, A.; Templin, T., 2nd; Smith, L. Dose response to vitamin D supplementation in postmenopausal women: A randomized trial. Ann. Intern. Med. 2012, 156, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Kruger, M.C.; Chan, Y.; Lau, L.; Lau, C.; Chin, Y.; Kuhn-Sherlock, B.; Todd, J.; Schollum, L. Calcium and vitamin D fortified milk reduces bone turnover and improves bone density in postmenopausal women over 1 year. Eur. J. Nutr. 2018, 57, 2785–2794. [Google Scholar] [CrossRef]
- Kruger, M.C.; Ha, P.; Todd, J.; Kuhn-Sherlock, B.; Schollum, L.; Ma, J.; Qin, G.; Lau, E. High-calcium, vitamin D fortified milk is effective in improving bone turnover markers and vitamin D status in healthy postmenopausal Chinese women. Eur. J. Clin. Nutr. 2012, 66, 856–861. [Google Scholar] [CrossRef]
- Kruger, M.C.; Schollum, L.; Kuhn-Sherlock, B.; Hestiantoro, A.; Wijanto, P.; Li-Yu, J.; Agdeppa, I.; Todd, J.; Eastell, R. The effect of a fortified milk drink on vitamin D status and bone turnover in post-menopausal women from South East Asia. Bone 2010, 46, 759–767. [Google Scholar] [CrossRef]
- Manios, Y.; Moschonis, G.; Mavrogianni, C.; Heuvel, E.; Singh-Povel, C.; Kiely, M.; Cashman, K. Reduced-fat Gouda-type cheese enriched with vitamin D effectively prevents vitamin D deficiency during winter months in postmenopausal women in Greece. Eur. J. Nutr. 2017, 56, 2367–2377. [Google Scholar] [CrossRef] [PubMed]
- Mastaglia, S.R.; Mautalen, C.; Parisi, M.; Oliveri, B. Vitamin D2 dose required to rapidly increase 25OHD levels in osteoporotic women. Eur. J. Clin. Nutr. 2006, 60, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Minisola, S.; Cianferotti, L.; Biondi, P.; Cipriani, C.; Fossi, C.; Franceschelli, F.; Giusti, F.; Leoncini, G.; Pepe, J.; Bischoff-Ferrari, H.; et al. Correction of vitamin D status by calcidiol: Pharmacokinetic profile, safety, and biochemical effects on bone and mineral metabolism of daily and weekly dosage regimens. Osteoporos. Int. 2017, 28, 3239–3249. [Google Scholar] [CrossRef]
- Mueangpaisarn, P.; Chaiamnuay, S. A randomized double-blinded placebo controlled trial of ergocalciferol 40,000 versus 100,000 IU per week for vitamin D inadequacy in institutionalized postmenopausal women. Aging Clin. Exp. Res. 2020, 32, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Castrillón, J.L.; Dueñas-Laita, A.; Brandi, M.; Jódar, E.; Del Pino-Montes, J.; Quesada-Gómez, J.; Castro, F.C.; Gómez-Alonso, C.; López, L.G.; Martínez, J.O.; et al. Calcifediol is superior to cholecalciferol in improving vitamin D status in postmenopausal women: A randomized trial. J. Bone Miner. Res. 2021, 36, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Pignotti, G.A.P.; Genaro, P.S.; Pinheiro, M.M.; Szejnfeld, V.L.; Martini, L.A. Is a lower dose of vitamin D supplementation enough to increase 25(OH)D status in a sunny country? Eur. J. Nutr. 2010, 49, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Garcia, R.; Mendoza, N.; Palacios, S.; Salas, N.; Quesada-Charneco, M.; Garcia-Martin, A.; Fonolla, J.; Lara-Villoslada, F.; Muñoz-Torres, M. Effects of Daily Intake of Calcium and Vitamin D-Enriched Milk in Healthy Postmenopausal Women: A Randomized, Controlled, Double-Blind Nutritional Study. J. Womens Health 2018, 27, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.A.; Aloia, J.; Pollack, S.; Yeh, J. Dose response to vitamin D supplementation among postmenopausal African American women. Am. J. Clin. Nutr. 2007, 86, 1657–1662. [Google Scholar] [CrossRef]
- Venugopal, Y.; Hatta, S.; Musa, N.; Rahman, S.; Ratnasingam, J.; Paramasivam, S.; Lim, L.; Ibrahim, L.; Choong, K.; Tan, A.; et al. Maintenance vitamin D3 dosage requirements in Chinese women with post menopausal osteoporosis living in the tropics. Asia Pac. J. Clin. Nutr. 2017, 26, 412–420. [Google Scholar]
- Watcharanon, W.; Kaewrudee, S.; Soontrapa, S.; Somboonporn, W.; Srisaenpang, P.; Panpanit, L.; Pongchaiyakul, C. Effects of sunlight exposure and vitamin D supplementation on vitamin D levels in postmenopausal women in rural Thailand: A randomized controlled trial. Complement. Ther. Med. 2018, 40, 243–247. [Google Scholar] [CrossRef]
- Zhang, M.; Zhao, L.; Zhou, Y.; Badr, R.; Watson, P.; Ye, A.; Zhou, B.; Zhang, J.; Deng, H.; Recker, R.; et al. SNP rs11185644 of RXRA gene is identified for dose-response variability to vitamin D3 supplementation: A randomized clinical trial. Sci. Rep. 2017, 7, 40593. [Google Scholar] [CrossRef]
- Kearns, M.D.; Binongo, J.; Watson, D.; Alvarez, J.; Lodin, D.; Ziegler, T.; Tangpricha, V. The effect of a single, large bolus of vitamin D in healthy adults over the winter and following year: A randomized, double-blind, placebo-controlled trial. Eur. J. Clin. Nutr. 2015, 69, 193–197. [Google Scholar] [CrossRef]
- Tjellesen, L.; Hummer, L.; Christiansen, C.; Rodbro, P. Serum concentration of vitamin D metabolites during treatment with vitamin D2 and D3 in normal premenopausal women. Bone Miner 1986, 1, 407–413. [Google Scholar]
- Trang, H.M.; Cole, D.; Rubin, L.; Pierratos, A.; Siu, S.; Vieth, R. Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am. J. Clin. Nutr. 1998, 68, 854–858. [Google Scholar] [CrossRef]
- Armas, L.A.; Hollis, B.; Heaney, R. Vitamin D2 is much less effective than vitamin D3 in humans. J. Clin. Endocrinol. Metab. 2004, 89, 5387–5391. [Google Scholar] [CrossRef] [PubMed]
- Tripkovic, L.; Lambert, H.; Hart, K.; Smith, C.; Bucca, G.; Penson, S.; Chope, G.; Hypponen, E.; Berry, J.; Vieth, R.; et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2012, 95, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Houghton, L.A.; Vieth, R. The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am. J. Clin. Nutr. 2006, 84, 694–697. [Google Scholar] [CrossRef] [PubMed]
- Hollis, B.W. Comparison of equilibrium and disequilibrium assay conditions for ergocalciferol, cholecalciferol and their major metabolites. J. Steroid. Biochem. 1984, 21, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, I.; Berlin, T.; Ewerth, S.; Bjorkhem, I. 25-Hydroxylase activity in subcellular fractions from human liver. Evidence for different rates of mitochondrial hydroxylation of vitamin D2 and D3. Scand. J. Clin. Lab. Investig. 1986, 46, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Stamp, T.C. Intestinal absorption of 25-hydroxycholecalciferol. Lancet 1974, 2, 121–123. [Google Scholar] [CrossRef]
- Haddad, J.G., Jr.; Rojanasathit, S. Acute administration of 25-hydroxycholecalciferol in man. J. Clin. Endocrinol. Metab. 1976, 42, 284–290. [Google Scholar] [CrossRef]
- Barger-Lux, M.J.; Heaney, R.; Dowell, S.; Chen, T.; Holick, M. Vitamin D and its major metabolites: Serum levels after graded oral dosing in healthy men. Osteoporos. Int. 1998, 8, 222–230. [Google Scholar] [CrossRef]
- Francis, R.M.; Peacock, M.; Storer, J.; Davies, A.; Brown, W.; Nordin, B. Calcium malabsorption in the elderly: The effect of treatment with oral 25-hydroxyvitamin D3. Eur. J. Clin. Investig. 1983, 13, 391–396. [Google Scholar] [CrossRef]
- Hahn, T.J.; Halstead, L.; Teitelbaum, S.; Hahn, B. Altered mineral metabolism in glucocorticoid-induced osteopenia. Effect of 25-hydroxyvitamin D administration. J. Clin. Investig. 1979, 64, 655–665. [Google Scholar] [CrossRef]
- Peacock, M.; Liu, G.; Carey, M.; McClintock, R.; Ambrosius, W.; Hui, S.; Johnston, C. Effect of calcium or 25OH vitamin D3 dietary supplementation on bone loss at the hip in men and women over the age of 60. J. Clin. Endocrinol. Metab. 2000, 85, 3011–3019. [Google Scholar] [PubMed]
- Sosa, M.; Lainez, P.; Arbelo, A.; Navarro, M. The effect of 25-dihydroxyvitamin D on the bone mineral metabolism of elderly women with hip fracture. Rheumatology 2000, 39, 1263–1268. [Google Scholar] [CrossRef]
- Stamp, T.C.; Haddad, J.G.; Twigg, C.A. Comparison of oral 25-hydroxycholecalciferol, vitamin D, and ultraviolet light as determinants of circulating 25-hydroxyvitamin D. Lancet 1977, 1, 1341–1343. [Google Scholar] [CrossRef] [PubMed]
- Broe, K.E.; Chen, T.; Weinberg, J.; Bischoff-Ferrari, H.; Holick, M.; Kiel, D. A higher dose of vitamin d reduces the risk of falls in nursing home residents: A randomized, multiple-dose study. J. Am. Geriatr. Soc. 2007, 55, 234–239. [Google Scholar] [CrossRef]
- Viljakainen, H.T.; Palssa, A.; Karkkainen, M.; Jakobsen, J.; Lamberg-Allardt, C. How much vitamin D3 do the elderly need? J. Am. Coll. Nutr. 2006, 25, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Seamans, K.; Cashman, K.; Kiely, M. An updated systematic review and meta-analysis of the efficacy of vitamin D food fortification. J. Nutr. 2012, 142, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef]
- Tang, J.C.Y.; Nicholls, H.; Piec, I.; Washbourne, C.; Dutton, J.; Jackson, S.; Greeves, J.; Fraser, W. Reference intervals for serum 24,25-dihydroxyvitamin D and the ratio with 25-hydroxyvitamin D established using a newly developed LC-MS/MS method. J. Nutr. Biochem. 2017, 46, 21–29. [Google Scholar] [CrossRef]
- Zhou, R.; Chun, R.; Lisse, T.; Garcia, A.; Xu, J.; Adams, J.; Hewison, M. Vitamin D and alternative splicing of RNA. J. Steroid Biochem. Mol. Biol. 2015, 148, 310–317. [Google Scholar] [CrossRef]
- Wicherts, I.S.; Boeke, A.; van der Meer, I.; van Schoor, N.; Knol, D.; Lips, P. Sunlight exposure or vitamin D supplementation for vitamin D-deficient non-western immigrants: A randomized clinical trial. Osteoporos. Int. 2011, 22, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Abd-Alrahman, S.; Panigrahy, A.; Al-Saleh, Y.; Aljohani, N.; Al-Attas, O.; Khattak, M.; Alokail, M. Efficacy of Vitamin D interventional strategies in saudi children and adults. J. Steroid. Biochem. Mol. Biol. 2018, 180, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Moradi, S.; Shahdadian, F.; Mohammadi, H.; Rouhani, M. A comparison of the effect of supplementation and sunlight exposure on serum vitamin D and parathyroid hormone: A systematic review and meta-analysis. Crit. Rev. Food. Sci. Nutr. 2020, 60, 1881–1889. [Google Scholar] [CrossRef] [PubMed]
- Chel, V.G.; Ooms, M.; Popp-Snijders, C.; Pavel, S.; Schothorst, A.; Meulemans, C.; Lips, P. Ultraviolet irradiation corrects vitamin D deficiency and suppresses secondary hyperparathyroidism in the elderly. J. Bone Miner. Res. 1998, 13, 1238–1242. [Google Scholar] [CrossRef]
- Vieth, R.; Bischoff-Ferrari, H.; Boucher, B.; Dawson-Hughes, B.; Garland, C.; Heaney, R.; Holick, M.; Hollis, B.; Lamberg-Allardt, C.; McGrath, J.; et al. The urgent need to recommend an intake of vitamin D that is effective. Am. J. Clin. Nutr. 2007, 85, 649–650. [Google Scholar] [CrossRef]
- Trivedi, D.P.; Doll, R.; Khaw, K. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: Randomised double blind controlled trial. BMJ 2003, 326, 469. [Google Scholar] [CrossRef]
- Chapuy, M.C.; Pamphile, R.; Paris, E.; Kempf, C.; Schlichting, M.; Arnaud, S.; Garnero, P.; Meunier, P. Combined calcium and vitamin D3 supplementation in elderly women: Confirmation of reversal of secondary hyperparathyroidism and hip fracture risk: The Decalyos II study. Osteoporos. Int. 2002, 13, 257–264. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.; Lu, Z.; Sauter, E. Vitamin D and skin physiology: A D-lightful story. J. Bone Miner. Res. 2007, 22 (Suppl. 2), V28–V33. [Google Scholar] [CrossRef]
- Klenk, J.; Rapp, K.; Denkinger, M.; Nagel, G.; Nikolaus, T.; Peter, R.; Koenig, W.; Bohm, B.; Rothenbacher, D. Seasonality of vitamin D status in older people in Southern Germany: Implications for assessment. Age Ageing 2013, 42, 404–408. [Google Scholar] [CrossRef]
- Macdonald, H.M. Contributions of sunlight and diet to vitamin D status. Calcif. Tissue Int. 2013, 92, 163–176. [Google Scholar] [CrossRef]
- Mason, C.; Xiao, L.; Imayama, I.; Duggan, C.; Bain, C.; Foster-Schubert, K.; Kong, A.; Campbell, K.; Wang, C.; Neuhouser, M.; et al. Effects of weight loss on serum vitamin D in postmenopausal women. Am. J. Clin. Nutr. 2011, 94, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Mistry, V.; Vukovich, M.; Hogie-Lorenzen, T.; Hollis, B.; Specker, B. Bioavailability of vitamin D from fortified process cheese and effects on vitamin D status in the elderly. J. Dairy Sci. 2005, 88, 2295–2301. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention and Comparators (Dose, Frequency, and Length of Intervention) | Outcome | Baseline Mean (SD) | Outcome Mean (SD) | p Value | Outcome Measure | Findings |
|---|---|---|---|---|---|---|
| (Pérez-Castrillón et al., 2021) [44] Spain and Italy | ||||||
| Calcifediol 0.226 mg/month for four months, then eight months placebo | 25(OH)D3 (ng/mL) | 12.8 (3.9) | 29.7 (8.6) | <0.0001 | Chemiluminescence immunoassay, the intra-assay coefficient of variation (CV) was 2.34, and the inter-assay coefficient of variation was 5.06% | Calcifediol is more effective than cholecalciferol in increasing serum 25(OH)D levels. |
| Cholecalciferol 25,000 IU/month for 52 weeks | 13.2 (3.7) | 23.8 (5.0) | ||||
| Calcifediol 0.226 mg/month for four months, then eight months placebo | Free 25(OH)D (pg/mL) | 3.8 (1.1) | 7.6 (2.5) | |||
| Cholecalciferol 25,000 IU/month for 52 weeks | 4.0 (1.1) | 6.5 (1.6) | ||||
| (Mueangpaisarn and Chaiamnuay, 2020) [43] Thailand | ||||||
| Vitamin D 40,000 IU/week for 12 weeks | 25(OH)D3 (ng/mL) | 19.4 (6.2) | 34.5 (9.1) | <0.001 | Electroluminescence immunoassay, the intra-assay coefficient of variability was 3.65, and the inter-assay coefficient of variability was 4.10 | Higher doses were more effective at raising serum 25(OH)D compared to the low dose |
| Vitamin D 100,000 IU/week for 12 weeks | 19.1 (6.5) | 51.7 (19.3) | ||||
| (Watcharanon et al., 2018) [49] Thailand | ||||||
| Vitamin D2 20,000 IU/week for 12 weeks | 25(OH)D3 (ng/mL) | 29.98 (6.35) | 32.44 (7.33) | <0.01 | Electroluminescence immunoassay with a coefficient variation of 3.7–4.5% | A combination of both vitamin D and sun exposure is more effective in raising serum 25(OH)D levels than sun exposure only in postmenopausal women |
| Sunlight exposure for 12 weeks | 32.30 (6.97) | 29.68 (6.28) | ||||
| (Reyes-Garcia et al., 2018) [46] Spain | ||||||
| Semi-skimmed milk calcium 180 mg/100 mL and vitamin D 120 IU/100 mL + Fructooligosaccharides (FOS) 5 g/L | 25(OH)D3 (ng/mL) | 21.4 (6.7) | 26.6 (6.4) | <0.001 | Chemiluminescence immunoassay | Daily intake of calcium and vitamin D-fortified milk significantly improves vitamin D status in postmenopausal Thai women |
| Semi-skimmed milk calcium 180 mg/100 mL and vitamin D 120 IU/100 mL + Fructooligosaccharides (FOS) 5 g/L | 22.3 (9.4) | 25.2 (6.2) | ||||
| Calcium 120 mg/100 mL and vitamin D 30 IU/100 mL | 21.8 (7.1) | 22.6 (7) | ||||
| (Kruger et al., 2018) [37] Malaysia | ||||||
| Vitamin D 15 ug/day + calcium 1200 mg | 25(OH)D3 (nmol/L) | 62.3 (1.89) | 74.8 (2.74) | <0.001 | Liquid chromatography–mass spectrometry | Daily intake of calcium and vitamin D-fortified milk significantly improves vitamin D status in postmenopausal Chinese women |
| Regular milk powder, 428 mg calcium | 64.8 (18.89) | 63.1 (2.87) | ||||
| (Bonjour et al., 2018) [35] Brazil | ||||||
| Vitamin D3-fortified yogurt 5 ug/day for 16 weeks, followed by eight weeks without product | 25(OH)D3 (nmol/L) | 36.5 (14.6) | 52.6 (17) | 0.008 | Enzyme-linked immunosorbent assay (ELISA) and electroluminescence immunoassay. The intra-assay and inter-assay variations were less than 7% for both. | A dose-dependent improvement in serum 25(OH)D with fortified yogurt and an inversely baseline-dependent increase in serum 25(OH)D |
| Vitamin D3-fortified yogurt 10 ug/day for 16 weeks, followed by eight weeks without product | 35.9 (14.8) | 58.9 (19.9) | 0.0008 | |||
| Regular dietary habits | 36.4 (15.8) | 49.5 (18.8) | ||||
| (Apaydin et al., 2018) [33] Turkey | ||||||
| Vitamin D3 800 IU/day for 12 weeks | 25(OH)D3 (nmol/L) | 24.2 (10.9) | 57.6 (11.7) | <0.001 | Chemiluminescence immunoassay | A single high oral dose of vitamin D is more effective than a daily low dose in raising serum 25(OH)D |
| Oral vitamin D3 single dose 300,000 IU | 25.4 (10.9) | 49.4 (17.9) | ||||
| (Venugopal et al., 2017) [48] Malaysia | ||||||
| Oral cholecalciferol 50,000 IU/monthly for 12 weeks | 25(OH)D3 (nmol/L) | 90.2 (23.1) | 96 (24.1) | 0.057 | Electro-chemiluminescence immunoassay (ECLIA). Intra-assay coefficient of variation, mean of 38.8 nmol/L −12.2% and mean of 169.5 nmol/L −2.2% | Both doses can safely maintain vitamin D sufficiency. Higher doses were required with baseline serum levels of <75 nmol/L |
| Oral cholecalciferol 25,000 IU/monthly for 12 weeks | 91.2 (24.6) | 107.1 (22.7) | ||||
| (Minisola et al., 2017) [42] Italy | ||||||
| Oral calcidiol 20 ug/day for 12 weeks | 25(OH)D3 (nmol/L) | 15.1 (7.4) | 49.3 (19.5) | <0.0001 | Liquid chromatography–mass-spectrometry. Intra-assay coefficient variation <5% and intra-assay <6% | Calcidiol in all dosage schemes significantly increased serum 25(OH)D in postmenopausal women and can be considered an alternative to cholecalciferol |
| Oral calcidiol 40 ug/day for 12 weeks | 16.8 (6.6) | 74.8 (22.5) | ||||
| Oral calcidiol 125 ug/week for 12 weeks | 16.4 (9.7) | 46.4 (15) | ||||
| (Manios et al., 2017) [40] Greece | ||||||
| Vitamin D3-enriched Gouda-type cheese 5.7 ug/day for eight weeks | 25(OH)D3 (nmol/L) | 47.3 (15.2) | 52.5 (12) | <0.001 | Chemiluminescence immunoassay. Intra-assay 8.9% and inter-assay 12.8% | Supplementation was sufficient in raising serum 23(OH)D levels throughout the winter season |
| Non-enriched reduced-fat cheese for eight weeks | 42.9 (17.7) | 38.3 (18.9) | ||||
| (Zhang et al., 2017) [50] China | ||||||
| Cholecalciferol 1100 IU/day + calcium 1500 mg/day for 52 weeks | 25(OH)D3 (nmol/L) reported as changes in mean 25(OH)D | 74.1 (18.5) | 24.31 (17.02) | <0.0001 | Radioimmunoassay | Polymorphisms in CYP2R1 and GC genes may be associated with differences in response to supplements in postmenopausal Caucasian women. |
| Calcium 1500 mg/day for 52 weeks | 73.4 (21.6) | −1.02 (11.12) | ||||
| Cholecalciferol 2000 IU/day + calcium 1500 mg/day for 52 weeks | 80.1 (25.5) | 31.92 (43.96) | ||||
| Control placebo | 80.8 (31.7) | 0.36 (41.17) | ||||
| (Gallagher et al., 2012) [36] USA | ||||||
| Vitamin D3 for 52 weeks | ||||||
| 400 IU/day | 25(OH)D3 (nmol/L) | 37.8 (10.8) | Serum concentrations were reported as a dose-response mixed-effect model | <0.001 | Radioimmunoassay, the inter-assay variation was 10.3% for 32.5 ng/mL and 12.7% for 70 ng/mL | Low doses of vitamin D3 of 600 IU and 800 IU/day were effective in raising serum 25(OH)D levels to greater than 50 nmol/L in postmenopausal women |
| 800 IU/day | 39.0 (9.5) | |||||
| 1600 IU/day | 37.4 (10.2) | |||||
| 2400 IU/day | 38.2 (10.1) | |||||
| 3200 IU/day | 39.8 (8.2) | |||||
| 4000 IU/day | 37.2 (9.2) | |||||
| 4800 IU/day | 38.6 (9.1) | |||||
| (Bischoff-Ferrari et al., 2012) [34] Switzerland | ||||||
| Vitamin D3 800 IU/day For 16 weeks | 25(OH)D3 (nmol/L) | 14.18 (3.61) | 30.99 (1.59) | <0.0001 | Liquid chromatography coupled to tandem mass spectrometry detection (HPLC-MS/MS) | Oral supplementation with (25(OH)D3 metabolite) at doses of 20 ug/day is safe and resulted in a rapid and prolonged increase in 25(OH)D levels compared with vitamin D3 |
| 25(OH)D3 (HyD) 800 IU/day for16 weeks | 12.28 (4.08) | 69.47 (1.58) | ||||
| Vitamin D3 5600 IU/week for 16 weeks | 1,25(OH)2D (pmol/L) | 38.61 (12.10) | 40.50 (2.91) | 0.004 | ||
| 25(OH)D3 (HyD) 5600 IU/week for16 weeks | 33.02 (13.63) | 53.06 (2.76) | ||||
| (Kruger et al., 2012) China | ||||||
| Calcium 900 mg and vitamin D-fortified milk 6.4 ug/day for 12 weeks | 25(OH)D3 (nmol/L) | 33.13 (15.5) | (33.13–39.49) | <0.001 | Electroluminescence immunoassay. Intra-assay coefficient variation is 5.1%, and inter-assay is 4.8% | High-calcium vitamin D-fortified milk was effective and significantly improved vitamin D status in postmenopausal Chinese women |
| Powdered control rice-based drink | 29.27 (12.03) | (29.27–28.21) | ||||
| (Kruger et al., 2010) [39] | ||||||
| High-calcium vitamin D-fortified milk—9.6 ug/day for 16 weeks (Indonesia) | 25(OH)D3 (nmol/L) | 45.06 (2.01) | - | <0.001 | Electroluminescence immunoassay | High-calcium vitamin D-fortified milk was effective and significantly improved vitamin D status in two groups of Southeast Asian postmenopausal women |
| Powdered control rice-based drink | 43.33 (2.01 | - | ||||
| High-calcium vitamin D-fortified milk—9.6 ug/day for 16 weeks (Philippines) | 62.0 (2.87) | - | ||||
| Powdered control rice-based drink | 59.23 (2.87) | - | ||||
| (Pignotti et al., 2010) [45] Brazil | ||||||
| Vitamin D3 400 IU/day + 600 mg calcium for 12 weeks | 25(OH)D3 (nmol/L) | 46.67 (13.97) | 59.47 (17.5) | 0.023 | Radioimmunoassay. Inter-assay coefficient variation 12% | Supplementation with 400 IU/day was not enough to raise serum concentrations of 25(OH)D to levels considered optimal for bone turnover in postmenopausal osteoporotic women |
| General orientation on a healthy diet | 52.87 (21.40) | 58.8 (24.72) | - | |||
| (Talwar et al., 2007) [47] USA | ||||||
| Vitamin D3 800 IU/day for 24 months | 25(OH)D (nmol/L) | 46.9 (20.6) | 65.9 (22.4) | <0.0001 | Radioimmunoassay. Inter-assay coefficient variation 7% | Supplementation with 2000 IU/day oral vitamin D3 was sufficient to raise serum 25(OH)D concentrations to >50 nmol/L in Black African American postmenopausal women |
| Control | 43.2 (16.8) | 41.6 (18.1) | - | |||
| Vitamin D3 800 IU/day for 24 months | 1,25(OH)2D (pmol/L) | 121.3 (39.2) | 107.6 (33.6) | - | ||
| Control | 119.2 (39.2) | 87.4 (33.6) | - | |||
| (Mastaglia et al., 2006) [41] Argentina | ||||||
| Oral drops of vitamin D2—5000 IU/Day for 12 weeks | 25(OH)D (nmol/L) | 42.0 (23.7–45.0) | 7.5 (66.2–156.2) | <0.001 | Radioimmunoassay. Intra-assay coefficient variation 7.6%, and inter-assay 19% | Vitamin D2 was effective at raising serum 25(OH)D levels to 85 nmol/L in postmenopausal osteoporotic women |
| Oral drops of vitamin D2—10,000 IU/Day for 12 weeks | 32.5 (27.5–37.5) | 97.7 (79.3–123.1) | ||||
| Control (placebo) | 45.0 (31.2–61.2) | 55.0 (72.5–68) | <0.01 | |||
| (Aloia et al., 2005) [32] USA | ||||||
| Vitamin D3 800 IU/day + calcium 1500 mg/day for 24 months, then 2000 IU for another 12 months | 25(OH)D (ng/mL) | 19.3 (8.36) | 34.8 | <0.001 | Radioimmunoassay | Supplementation with 20 ug/day oral vitamin D3 was sufficient to raise serum 25(OH)D concentrations to a mean of 89.9 nmol/L in Black African American postmenopausal women |
| Control (placebo) | 17.2 (6.64) | - | - | |||
| Vitamin D3 800 IU/day + calcium 1500 mg/day for 24 months, then 2000 IU for another 12 months | 1,25(OH)2D (pmol/L) | 46.5 (15.2) | - | - | ||
| Control (placebo) | 45.7 (15.10) | - | - | |||
| Trial | Population | Sample Size | Drop out (n) | Adverse Events | Compliance Rate | Compliance Assessment |
|---|---|---|---|---|---|---|
| (Bonjour et al., 2018 [35] | Healthy postmenopausal women | 140 | 7 | - | 93−100% | Completed a questionnaire regarding adherence and acceptability in a dairy. Adherence was measured by returning yogurt lids |
| (Reyes-Garcia et al., 2018) [46] | Healthy postmenopausal women | 461 | 94 | Adverse events not reported | 80% | By a food frequency questionnaire at baseline, 12 months, and end of the study |
| (Kruger et al., 2018) [37] | Healthy Chinese Malaysian postmenopausal women | 121 | 23 | Adverse events not reported | 86–90% | Phone calls were made to monitor milk consumption, and each subject was provided with a monthly diary to record their intake daily |
| (Manios et al., 2017) [40] | Healthy postmenopausal women | 80 | 1 | - | 97.50% | Bi-weekly meetings and telephone communication. Participants were provided with a diary to record their intake daily |
| (Kruger et al., 2012) [38] | Healthy Chinese postmenopausal women | 63 | 5 | Two events; one of constipation and stomach discomfort and one of cancer (unrelated to the intervention) | 98% | Phone calls were made to monitor milk consumption, and each subject was provided with a monthly diary to record their intake daily |
| Kruger et al., 2010 [39] | Healthy Asian postmenopausal women | 120 | 3 | Two events of lactose intolerance and one of gastrointestinal discomfort | 98–99.6% | Participants were provided with a diary to record their intake daily |
| (Pérez-Castrillón et al., 2021) [44] | White postmenopausal women with (32) and without osteoporosis (266) | 303 | 5 | Nine adverse events were reported (not specified) | - | Dietary calcium consumption at baseline, 4, 8, and 12 months was assessed using an adapted version of a validated questionnaire |
| (Mueangpaisarn and Chaiamnuay, 2020) [43] | Asian postmenopausal women with vitamin D deficiency | 94 | 9 | Three adverse events: constipation; chest pain, and one hip fracture | >80% | Did not report |
| (Watcharanon et al., 2018) [49] | Healthy Asian postmenopausal women | 52 | - | None | - | Did not report |
| (Apaydin et al., 2018) [33] | Healthy postmenopausal women | 60 | - | - | - | Did not report |
| (Venugopal et al., 2017) [48] | Chinese Malaysian postmenopausal osteoporotic women | 90 | - | - | - | The study intervention was administered monthly at the clinic under the direct supervision of the investigator |
| (Minisola et al., 2017) [42] | Postmenopausal women with vitamin D deficiency | 87 | Four events: three reported flu and one hypercalcemia possibly related to the intervention | - | Compliance was recorded at each of the study time points (not specified how) | |
| (Zhang et al., 2017) [50] | Non-Hispanic White postmenopausal women | 2207 | - | - | - | By bottle weight. Empty and full bottles were weighed, and then the resulting subtraction was divided by the number of tablets in the bottle |
| (Gallagher et al., 2012) [36] | Healthy postmenopausal White women with vitamin D insufficiency | 163 | 16 | Three events: one hypercalciuria, one myocardial infarction, and one congestive heart failure | 86–90% | By counting pills |
| (Bischoff-Ferrari et al., 2012) [34] | Healthy White postmenopausal women | 20 | - | By capsule count at each study visit and by measuring the serum concentration of 25(OH)D at the end of the study | ||
| (Pignotti et al., 2010) [45] | Caucasian postmenopausal osteoporotic women | 64 | 6 | - | - | Dietary intake was collected through 3-day food record and checked and calculated by nutrition software (Nutrition Data System for Research, University of Minnesota) |
| (Talwar et al., 2007) [47] | Healthy Black African-American postmenopausal women | 208 | - | Eight severe hypercalcemia events, none of which was considered to be related to the study intervention | 87% | Food frequency questionnaire at each visit to assess calcium intake |
| (Mastaglia et al., 2006) [41] | Postmenopausal osteoporotic women | 45 | 45/7 | Three cases of hypercalciuria | 89–92% | By pill counts and drop counts in each box and vial returned at each monthly visit |
| (Aloia et al., 2005) [32] | Healthy Black African-American postmenopausal women | 208 | 19 | 222 adverse events were reported over the study period of three years | - | Food frequency questionnaire at each visit to assess calcium intake |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassanein, M.M.; Huri, H.Z.; Baig, K.; Abduelkarem, A.R. Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review. Nutrients 2023, 15, 685. https://doi.org/10.3390/nu15030685
Hassanein MM, Huri HZ, Baig K, Abduelkarem AR. Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review. Nutrients. 2023; 15(3):685. https://doi.org/10.3390/nu15030685
Chicago/Turabian StyleHassanein, Mohammed M., Hasniza Zaman Huri, Kauser Baig, and Abduelmula R. Abduelkarem. 2023. "Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review" Nutrients 15, no. 3: 685. https://doi.org/10.3390/nu15030685
APA StyleHassanein, M. M., Huri, H. Z., Baig, K., & Abduelkarem, A. R. (2023). Determinants and Effects of Vitamin D Supplementation in Postmenopausal Women: A Systematic Review. Nutrients, 15(3), 685. https://doi.org/10.3390/nu15030685