
Effects of Creatine Supplementation after 20 Minutes of Recovery in a Bench Press Exercise Protocol in Moderately Physically Trained Men

 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
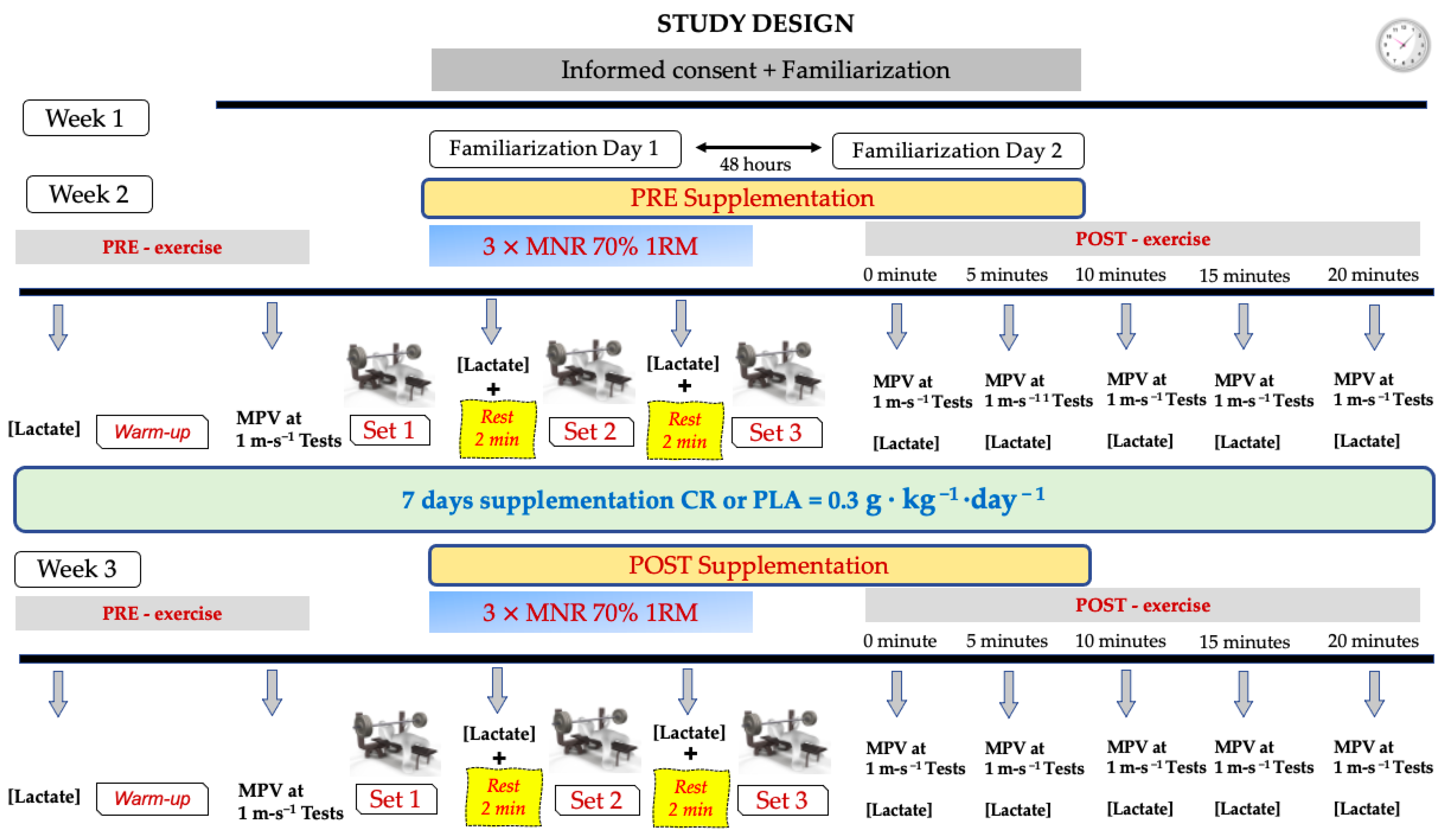
2.1. Study Design
2.2. Participants
2.3. Supplementation
2.4. Procedures
2.4.1. One Repetition Maximum (1RM) Test
2.4.2. 3×Maximum Number of Repetitions (MNR) Exercise Protocol
2.4.3. Blood Lactate Concentrations
2.4.4. Mechanical Fatigue Test
2.4.5. Measurement Equipment
2.4.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buford, T.W.; Kreider, R.B.; Stout, J.R.; Greenwood, M.; Campbell, B.; Spano, M.; Ziegenfuss, T.; Lopez, H.; Landis, J.; Antonio, J. International Society of Sports Nutrition position stand: Creatine supplementation and exercise. J. Int. Soc. Sports Nutr. 2007, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Kreider, R.B.; Jung, Y.P. Creatine supplementation in exercise, sport, and medicine. J. Exerc. Nutr. Biochem. 2011, 15, 53–69. [Google Scholar] [CrossRef]
- Kreider, R.B.; Kalman, D.S.; Antonio, J.; Ziegenfuss, T.N.; Wildman, R.; Collins, R.; Candow, D.G.; Kleiner, S.M.; Almada, A.L.; Lopez, H.L. International Society of Sports Nutrition position stand: Safety and efficacy of creatine supplementation in exercise, sport, and medicine. J. Int. Soc. Sports Nutr. 2017, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Hultman, E.; Söderlund, K.; Timmons, J.A.; Cederblad, G.; Greenhaff, P.L. Muscle creatine loading in men. J. Appl. Physiol. 1996, 81, 232–237. [Google Scholar] [CrossRef]
- Green, A.L.; Hultman, E.; Macdonald, I.A.; Sewell, D.A.; Greenhaff, P.L. Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans. Am. J. Physiol. 1996, 271 Pt 1, E821–E826. [Google Scholar] [CrossRef]
- Harris, R.C.; Soderlund, K.; Hultman, E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin. Sci. 1992, 83, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Balsom, P.D.; Soderlund, K.; Ekblom, B. Creatine in humans with special reference to creatine supplementation. Sports Med. 1994, 18, 268–280. [Google Scholar] [CrossRef]
- Brosnan, M.E.; Brosnan, J.T. The role of dietary creatine. Amino Acids 2016, 48, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Mizuta, C.; Uda, K.; Ishida, K.; Mizuta, K.; Sona, S.; Compaan, D.M.; Ellington, W.R. Evolution and divergence of the genes for cytoplasmic, mitochondrial, and flagellar creatine kinases. J. Mol. Evol. 2004, 59, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Bertin, M.; Pomponi, S.M.; Kokuhuta, C.; Iwasaki, N.; Suzuki, T.; Ellington, W.R. Origin of the genes for the isoforms of creatine kinase. Gene 2007, 392, 273–282. [Google Scholar] [CrossRef]
- Sahlin, K.; Harris, R.C. The creatine kinase reaction: A simple reaction with functional complexity. Amino Acids 2011, 40, 1363–1367. [Google Scholar] [CrossRef] [PubMed]
- Wyss, M.; Kaddurah-Daouk, R. Creatine and creatinine metabolism. Physiol. Rev. 2000, 80, 1107–1213. [Google Scholar] [CrossRef] [PubMed]
- Ostojic, S.M.; Forbes, S.C. Perspective: Creatine, a conditionally essential nutrient: Building the case. Adv. Nutr. 2022, 13, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Balsom, P.D.; Ekblom, B.; Söerlund, K.; Sjödin, B.; Hultman, E. Creatine supplementation and dynamic high-intensity intermittent exercise. Scand. J. Med. Sci. Sports 1993, 3, 143–149. [Google Scholar] [CrossRef]
- Greenhaff, P.L.; Casey, A.; Short, A.H.; Harris, R.; Soderlund, K.; Hultman, E. Influence of Oral Creatine Supplementation of Muscle Torque during Repeated Bouts of Maximal Voluntary Exercise in Man. Clin. Sci. 1993, 84, 565–571. [Google Scholar] [CrossRef]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.E.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E.; et al. ISSN exercise & sports nutrition review update: Research & recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 38. [Google Scholar]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common questions and misconceptions about creatine supplementation: What does the scientific evidence really show? J. Int. Soc. Sports Nutr. 2021, 18, 13. [Google Scholar] [CrossRef]
- Bemben, M.G.; Lamont, H.S. Creatine supplementation and exercise performance: Recent findings. Sports Med. 2005, 35, 107–125. [Google Scholar] [CrossRef]
- Australian Institute of Sport. ABCD Classification System. 2021. Available online: https://www.ais.gov.au/nutrition/supplements/group_a (accessed on 27 December 2022).
- Wax, B.; Kerksick, C.M.; Jagim, A.R.; Mayo, J.J.; Lyons, B.C.; Kreider, R.B. Creatine for Exercise and Sports Performance, with Recovery Considerations for Healthy Populations. Nutrients 2021, 13, 1915. [Google Scholar] [CrossRef]
- Izquierdo, M.; Ibañez, J.; González-Badillo, J.J.; Gorostiaga, E.M. Effects of creatine supplementation on muscle power, endurance, and sprint performance. Med. Sci. Sports Exerc. 2002, 34, 332–343. [Google Scholar] [CrossRef]
- Bazzucchi, I.; Felici, F.; Sacchetti, M. Effect of short-term creatine supplementation on neuromuscular function. Med. Sci. Sports Exerc. 2009, 41, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Naclerio, F.; Allgrove, J.; Jimenez, A. Creatine supplementation with specific view to exercise/sports performance: An update. J. Int. Soc. Sports Nutr. 2012, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Atter, T.; Georg, K.P. Oral creatine supplementation improves multiple sprint performance in elite ice-hockey players. J. Sports Med. Phys. Fit. 1999, 39, 189–196. [Google Scholar] [CrossRef]
- Cottrell, G.T.; Coast, J.R.; Herb, R.A. Effect of recovery interval on multiple-bouts print cycling performance after acute creatine supplementation. J. Strength Cond. Res. 2002, 16, 109–116. [Google Scholar] [PubMed]
- Griffen, C.; Rogerson, D.; Ranchordas, M.; Ruddock, A. Effects of Creatine and Sodium Bicarbonate Coingestion on Multiple Indices of Mechanical Power Output during Repeated Wingate Tests in Trained Men. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 298–306. [Google Scholar] [CrossRef]
- Crisafulli, D.L.; Buddhadev, H.H.; Brilla, L.R.; Chalmers, G.R.; Suprak, D.N.; Juan, J.G.S. Creatine-electrolyte supplementation improves repeated sprint cycling performance: A double blind randomized control study. J. Int. Soc. Sports Nutr. 2018, 15, 21. [Google Scholar] [CrossRef]
- Aaserud, R.; Gramvik, P.; Olsen, S.R.; Jensen, J. Creatine supplementation delay son set of fatigue during repeated bouts of sprint running. Scand. J. Med. Sci. Sports 1998, 8, 247–251. [Google Scholar] [CrossRef]
- Mujika, I.; Padilla, S.; Ibañez, J.; Izquierdo, M.; Gorostiaga, E. Creatine supplementation and sprint performance in soccer players. Med. Sci. Sports Exerc. 2000, 32, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Deminice, R.; Rosa, F.T.; Franco, G.S.; Jordao, A.A.; de Freitas, E.C. Effects of creatine supplementation on oxidative stress and inflammatory markers after repeated-sprint exercise in humans. Nutrients 2013, 29, 1127–1132. [Google Scholar] [CrossRef]
- Bogdanis, G.C.; Nevill, M.E.; Aphamis, G.; Stavrinou, P.S.; Jenkins, D.G.; Giannaki, C.D.; Lakomy, H.K.A.; Williams, C. Effects of Oral Creatine Supplementation on Power Output during Repeated Treadmill Sprinting. Nutrients 2022, 14, 1140. [Google Scholar] [CrossRef] [PubMed]
- Grindstaff, P.D.; Kreider, R.; Bishop, R.; Wilson, M.; Wood, L.; Alexander, C.; Almada, A. Effects of creatine supplementation on repetitive sprint performance and body composition in competitive swimmers. Int. J. Sport Nutr. 1997, 7, 330–346. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Kraermer, W.J.; Bush, J.A.; Boetes, M.; Incledon, T.; Clark, K.L.; Lynch, J.M. Creatine supplementation enhances muscular performance during high-intensity resistance exercise. J. Am. Diet. Assoc. 1997, 97, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Warber, J.P.; Tharion, W.J.; Patton, J.F.; Champagne, C.M.; Mitotti, P.; Lieberman, H.R. The effect of creatine monohydrate supplementation on ob- stacle course and multiple bench press performance. J. Strength Cond. Res. 2002, 16, 500–508. [Google Scholar] [PubMed]
- Hernández-Lougedo, J.; Heredia-Elvar, J.R.; Maicas-Pérez, L.; Cañuelo-Márquez, A.M.; Rozalén-Bustín, M.; de Jesús Franco, F.; Garnacho-Castaño, M.V.; García-Fernández, P.; Maté-Muñoz, J.L. Neuromuscular Fatigue and Metabolic Stress during the 15 Minutes of Rest after Carrying Out a Bench Press Exercise Protocol. Biology 2022, 11, 1435. [Google Scholar] [CrossRef] [PubMed]
- Maté-Muñoz, J.L.; Budurin, M.; González-Lozano, S.; Heredia-Elvar, J.R.; Cañuelo-Márquez, A.M.; Barba-Ruiz, M.; Muriarte, D.; Garnacho-Castaño, M.V.; Hernández-Lougedo, J.; García-Fernández, P. Physiological Responses at 15 Minutes of Recovery after a Session of Functional Fitness Training in Well-Trained Athletes. Int. J. Environ. Res. Public Health 2022, 19, 8864. [Google Scholar] [CrossRef] [PubMed]
- Pallarés, J.G.; López-Samanes, A.; Fernández-Elías, V.E.; Aguado-Jiménez, R.; Ortega, J.F.; Gómez, C.; Ventura, R.; Segura, J.; Mora-Rodríguez, R. Pseudoephedrine and circadian rhythm interaction on neuromuscular performance. Scand. J. Med. Sci. Sport 2015, 25, e603–e612. [Google Scholar] [CrossRef]
- Moses, L.E.; Oakford, R.Y. Tables of Random Permutations; Standford University Press: Standford, CA, USA, 1963. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- Sánchez-Medina, L.; Pérez, C.E.; González-Badillo, J.J. Importance of the propulsive phase in strength assessment. Int. J. Sports Med. 2010, 31, 123–129. [Google Scholar] [CrossRef]
- Heredia-Elvar, J.R.; Hernández-Lougedo, J.; Maicas-Pérez, L.; Notario-Alonso, R.; Garnacho-Castaño, M.V.; García-Fernández, P.; Maté-Muñoz, J.L. Reproducibility and Applicability of Traditional Strength Training Prescription Recommendations. Biology 2022, 11, 851. [Google Scholar] [CrossRef]
- Sánchez-Medina, L.; González-Badillo, J.J. Velocity loss as an indicator of neuromuscular fatigue during resistance training. Med. Sci. Sports Exerc. 2011, 43, 1725–1734. [Google Scholar] [CrossRef] [PubMed]
- Peña García-Orea, G.; Belando-Pedreño, N.; Merino-Barrero, J.A.; Heredia-Elvar, J.R. Validation of an opto-electronic instrument for the measurement of execution velocity in squat exercise. Sports Biomech. 2021, 6, 706–719. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, L.R.; Thompson, D.; Philips, G.; Backx, K.; Crickmore, L. A comparison of the Lactate Pro, Accusport, Analox GM7 and Kodak Ektachem lactate analysers in normal, hot and humid conditions. Int. J. Sports Med. 2002, 23, 130–135. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.R.; Norris, S.R.; Smith, D.J. Comparison of the Lactate Pro and the YSI 1500 Sport Blood Lactate analyzers. Int. J. Appl. Sports Sci. 2004, 16, 22–30. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage: London, UK, 2013; pp. 473–474. [Google Scholar]
- Earnest, C.P.; Snell, P.G.; Rodriguez, R.; Almada, A.L.; Mitchell, T.L. The effect of creatine monohydrate ingestion on anaerobic power indices, muscular strength and body composition. Acta Physiol. Scand. 1995, 153, 207–209. [Google Scholar] [CrossRef]
- Rossiter, H.B.; Cannell, E.R.; Jakeman, P.M. The effect of oral creatine supplementation on the 1000-m performance of competitive rowers. J. Sports Sci. 1996, 14, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Kreider, R.B.; Ferreira, M.; Wilson, M.; Grindstaff, P.; Plisk, S.; Reinardy, J.; Cantler, E.; Almada, A.L. Effects of creatine supplementation on body composition, strength, and sprint performance. Med. Sci. Sports Exerc. 1998, 30, 73–82. [Google Scholar] [CrossRef]
- Yquel, R.; Arsac, L.; Thiaudière, E.; Canioni, P.; Manier, G. Effect of creatine supplementation on phosphocreatine resynthesis, inorganic phosphate accumulation and pH during intermittent maximal exercise. J. Sports Sci. 2002, 20, 427–437. [Google Scholar] [CrossRef]
- Fitts, R. Cellular. mechanisms of muscle fatigue. Physiol. Rev. 1994, 74, 49–94. [Google Scholar] [CrossRef] [PubMed]
- Ahmun, R.P.; Tong, R.J.; Grimshaw, P.N. The effects of acute creatine supplementation on multiple sprint cycling and running performance in rugby players. J. Strength Cond. Res. 2005, 19, 92–97. [Google Scholar]
- Balsom, P.D.; Söderlund, K.; Sjödin, B.; Ekblom, B. Skeletal Muscle Metabolism During Short Duration High-Intensity Exercise: Influence of Creatine Supplementation. Acta Physiol. Scand. 1995, 154, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-Y.; Seo, B.-D.; Choi, P.-A. Influence of taekwondo as security martial arts training on anaerobic threshold, cardiorespiratory fitness, and blood lactate recovery. J. Phys. Ther. Sci. 2014, 26, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Bogdanis, G.C.; Nevill, M.E.; Boobis, L.H.; Lakomy, H.K. Contribution of Phosphocreatine and Aerobic Metabolism to Energy Supply During Repeated Sprint Exercise. J. Appl. Physiol. 1996, 80, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Whiters, R.T.; Sherman, W.M.; Clark, D.G.; Esselbach, P.C.; Nolan, S.R.; Mackay, M.H.; Brinkman, M. Muscle metabolism during 30, 60 and 90 s of maximal cycling on an air-braked ergometer. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 63, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Bogdanis, G.C.; Nevill, M.E.; Boobis, L.H.; Lakomy, H.K.A.; Nevill, A.M. Recovery of power output and muscle metabolites following 30 s of maximal sprint cycling in man. J. Physiol. 1995, 482, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Gaitanos, C.G.; Williams, C.; Boobis, L.H.; Brooks, S. Human muscle metabolism during intermittent maximal exercise. J. Appl. Physiol. 1993, 75, 712–719. [Google Scholar] [CrossRef]
- Almutairi, R.; Basson, A.R.; Wearsh, P.; Cominelli, F.; Rodriguez-Palacios, A. Validity of food additive maltodextrin as placebo and effects on human gut physiology: Systematic review of placebo-controlled clinical trials. Eur. J. Nutr. 2022, 61, 2853–2871. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | (M ± SD) (n = 50) | 95%CI |
|---|---|---|
| Age (years) | 22.40 ± 3.31 | 21.46–23.34 |
| Weight (kg) | 76.89 ± 9.78 | 74.11–79.67 |
| Height (m) | 1.79 ± 0.06 | 1.77–1.80 |
| BMI (kg·m−2) | 24.02 ± 2.33 | 23.36–24.68 |
| RSR (kg at 1RM·kg body mass−1) | 1.06 ± 0.20 | 1.00–1.11 |
| 1RM (kg) | 80.76 ± 16.59 | 76.05–85.47 |
| MPV 1RM (m·s−1) | 0.17 ± 0.07 | 0.15–0.19 |
| PRE Suppl | POST Suppl | PRE Suppl | POST Suppl | PRE Suppl | POST Suppl | ||
|---|---|---|---|---|---|---|---|
| Group | MPVrep Best (m·s−1) (M ± SD, 95% CI) | MPVrep Best (m·s−1) (M ± SD, 95% CI) | MPVrep Last (m·s−1) (M ± SD, 95% CI) | MPVrep Last (m·s−1) (M ± SD, 95% CI) | % loss MPV Set (M ± SD, 95% CI) | % loss MPV Set (M ± SD, 95% CI) | |
| CREATINE | 0.62 ± 0.09 | 0.63 ± 0.07 | 0.14 ± 0.04 | 0.15 ± 0.04 | −77.94 ± 5.82 | −75.81 ± 6.49 | |
| SET 1 | 0.58–0.66 | 0.60–0.66 | 0.12–0.16 | 0.13–0.17 | −80.87–−75.01 | −78.61–−73.01 | |
| PLACEBO | 0.60 ± 0.11 | 0.61 ± 0.08 | 0.15 ± 0.05 | 0.16 ± 0.05 | –74.11 ± 8.50 | –73.88 ± 7.41 | |
| 0.56–0.64 | 0.58–0.64 | 0.14–0.17 | 0.14–0.17 | −77.04–−71.19 | −76.68–−71.08 | ||
| CREATINE | 0.42 ± 0.07 | 0.40 ± 0.06 | 0.17 ± 0.04 | 0.16 ± 0.04 | −59.25 ± 10.36 * | −59.16 ± 9.15 | |
| SET 2 | 0.39–0.45 | 0.38–0.42 | 0.15–0.19 | 0.14–0.18 | −63.37–−55.12 | –63.03–−55.29 | |
| PLACEBO | 0.44 ± 0.07 | 0.43 ± 0.06 | 0.14 ± 0.05 | 0.16 ± 0.05 | −67.20 ± 10.15 | −63.16 ± 10.07 | |
| 0.41–0.47 | 0.40–0.45 | 0.13–0.16 | 0.14–0.18 | −71.32–−63.07 | −67.03–−59.29 | ||
| CREATINE | 0.35 ± 0.05 | 0.34 ± 0.05 | 0.17 ± 0.06 | 0.16 ± 0.06 | −52.32 ± 15.77 | −53.40 ± 20.99 | |
| SET 3 | 0.33–0.37 | 0.32–0.36 | 0.15–0.19 | 0.13–0.18 | −58.69–−45.96 | −60.27–−46.5 | |
| PLACEBO | 0.37 ± 0.06 | 0.36 ± 0.05 | 0.16 ± 0.5 | 0.15 ± 0.04 | −53.89 ± 15.88 | −58.52 ± 12.01 | |
| 0.34–0.39 | 0.34–0.38 | 0.14–0.18 | 0.13–0.17 | −69.75–−78.17 | −65.40–−51.65 |
| PRE Suppl | POST Suppl | |||||
|---|---|---|---|---|---|---|
| Group | Lactate (mmol·L−1) (M ± SD, 95% CI) | Lactate (mmol·L−1) (M ± SD, 95% CI | p Time ηp2 SP | p Group ηp2 SP | p Group × Time ηp2 SP | |
| Pre-exercise | CREATINE | 1.3 ± 0.3 | 1.4 ± 0.3 | 0.054 0.075 0.492 | 0.780 0.002 0.059 | 0.513 0.009 0.099 |
| 1.2–1.5 | 1.3–1.6 | |||||
| PLACEBO | 1.3 ± 0.3 | 1.5 ± 0.5 | ||||
| 1.2–1.5 | 1.3–1.6 | |||||
| SET 1 | CREATINE | 4.9 ± 1.2 | 4.8 ± 0.9 | 0.993 0.000 0.050 | 0.675 0.004 0.070 | 0.838 0.001 0.055 |
| 4.3–5.4 | 4.4–5.3 | |||||
| PLACEBO | 4.7 ± 1.5 | 4.8 ± 1.2 | ||||
| 4.2–5.3 | 4.4–5.2 | |||||
| SET 2 | CREATINE | 5.7 ± 1.0 | 6.0 ± 0.7 | 0.320 0.021 0.167 | 0.760 0.002 0.060 | 0.602 0.006 0.081 |
| 5.1–6.2 | 5.6–6.3 | |||||
| PLACEBO | 5.9 ± 1.6 | 5.9 ± 1.0 | ||||
| 5.3–6.4 | 5.6–6.3 | |||||
| SET 3 | CREATINE | 6.8 ± 1.5 | 7.0 ± 1.4 | 0.081 0.062 0.416 | 0.691 0.003 0.068 | 0.486 0.010 0.106 |
| 6.2–7.4 | 6.4–7.5 | |||||
| PLACEBO | 6.5 ± 1.5 | 7.0 ± 1.4 | ||||
| 5.9–7.1 | 6.4–7.5 | |||||
| CREATINE | 6.2 ± 1.0 | 6.8 ± 1.8 | 0.035 * 0.091 0.565 | 0.202 0.034 0.245 | 0.213 0.033 0.236 | |
| 5 min Post-exercise | 5.7–6.7 | 6.2–7.4 | ||||
| PLACEBO | 6.0 ± 1.3 | 6.1 ± 1.2 | ||||
| 5.5–6.5 | 5.5–6.7 | |||||
| 10 min Post-exercise | CREATINE | 5.1 ± 1.1 | 5.9 ± 1.1 | 0.002 * 0.175 0.879 | 0.043 * 0.082 0.529 | 0.028 * 0.097 0.604 |
| 4.6–5.5 | 5.5–6.3 | |||||
| PLACEBO | 4.8 ± 1.3 | 5.0 ± 1.0 | ||||
| 4.3–5.3 | 4.6–5.4 | |||||
| 15 min Post-exercise | CREATINE | 4.1 ± 0.6 | 5.1 ± 1.7 | <0.001 * 0.258 0.980 | 0.043 * 0.083 0.532 | 0.038 * 0.087 0.552 |
| 3.8–4.4 | 4.6–5.7 | |||||
| PLACEBO | 3.9 ± 1.0 | 4.3 ± 0.9 | ||||
| 3.6–4.2 | 3.7–4.8 | |||||
| 20 min Post-exercise | CREATINE | 3.7 ± 1.0 | 4.4 ± 2.0 | 0.281 0.024 0.187 | 0.040 * 0.085 0.545 | 0.027 * 0.098 0.609 |
| 3.3–4.1 | 3.8–5.0 | |||||
| PLACEBO | 3.6 ± 0.8 | 3.3 ± 0.8 | ||||
| 3.2–3.9 | 2.7–3.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maicas-Pérez, L.; Hernández-Lougedo, J.; Heredia-Elvar, J.R.; Pedauyé-Rueda, B.; Cañuelo-Márquez, A.M.; Barba-Ruiz, M.; Lozano-Estevan, M.d.C.; García-Fernández, P.; Maté-Muñoz, J.L. Effects of Creatine Supplementation after 20 Minutes of Recovery in a Bench Press Exercise Protocol in Moderately Physically Trained Men. Nutrients 2023, 15, 657. https://doi.org/10.3390/nu15030657
Maicas-Pérez L, Hernández-Lougedo J, Heredia-Elvar JR, Pedauyé-Rueda B, Cañuelo-Márquez AM, Barba-Ruiz M, Lozano-Estevan MdC, García-Fernández P, Maté-Muñoz JL. Effects of Creatine Supplementation after 20 Minutes of Recovery in a Bench Press Exercise Protocol in Moderately Physically Trained Men. Nutrients. 2023; 15(3):657. https://doi.org/10.3390/nu15030657
Chicago/Turabian StyleMaicas-Pérez, Luis, Juan Hernández-Lougedo, Juan Ramón Heredia-Elvar, Blanca Pedauyé-Rueda, Ana María Cañuelo-Márquez, Manuel Barba-Ruiz, María del Carmen Lozano-Estevan, Pablo García-Fernández, and José Luis Maté-Muñoz. 2023. "Effects of Creatine Supplementation after 20 Minutes of Recovery in a Bench Press Exercise Protocol in Moderately Physically Trained Men" Nutrients 15, no. 3: 657. https://doi.org/10.3390/nu15030657
APA StyleMaicas-Pérez, L., Hernández-Lougedo, J., Heredia-Elvar, J. R., Pedauyé-Rueda, B., Cañuelo-Márquez, A. M., Barba-Ruiz, M., Lozano-Estevan, M. d. C., García-Fernández, P., & Maté-Muñoz, J. L. (2023). Effects of Creatine Supplementation after 20 Minutes of Recovery in a Bench Press Exercise Protocol in Moderately Physically Trained Men. Nutrients, 15(3), 657. https://doi.org/10.3390/nu15030657