
Virgin Coconut Oil: A Dietary Intervention for Dyslipidaemia in Patients with Diabetes Mellitus

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Participants
2.3. Methods
2.4. Statistical Analysis
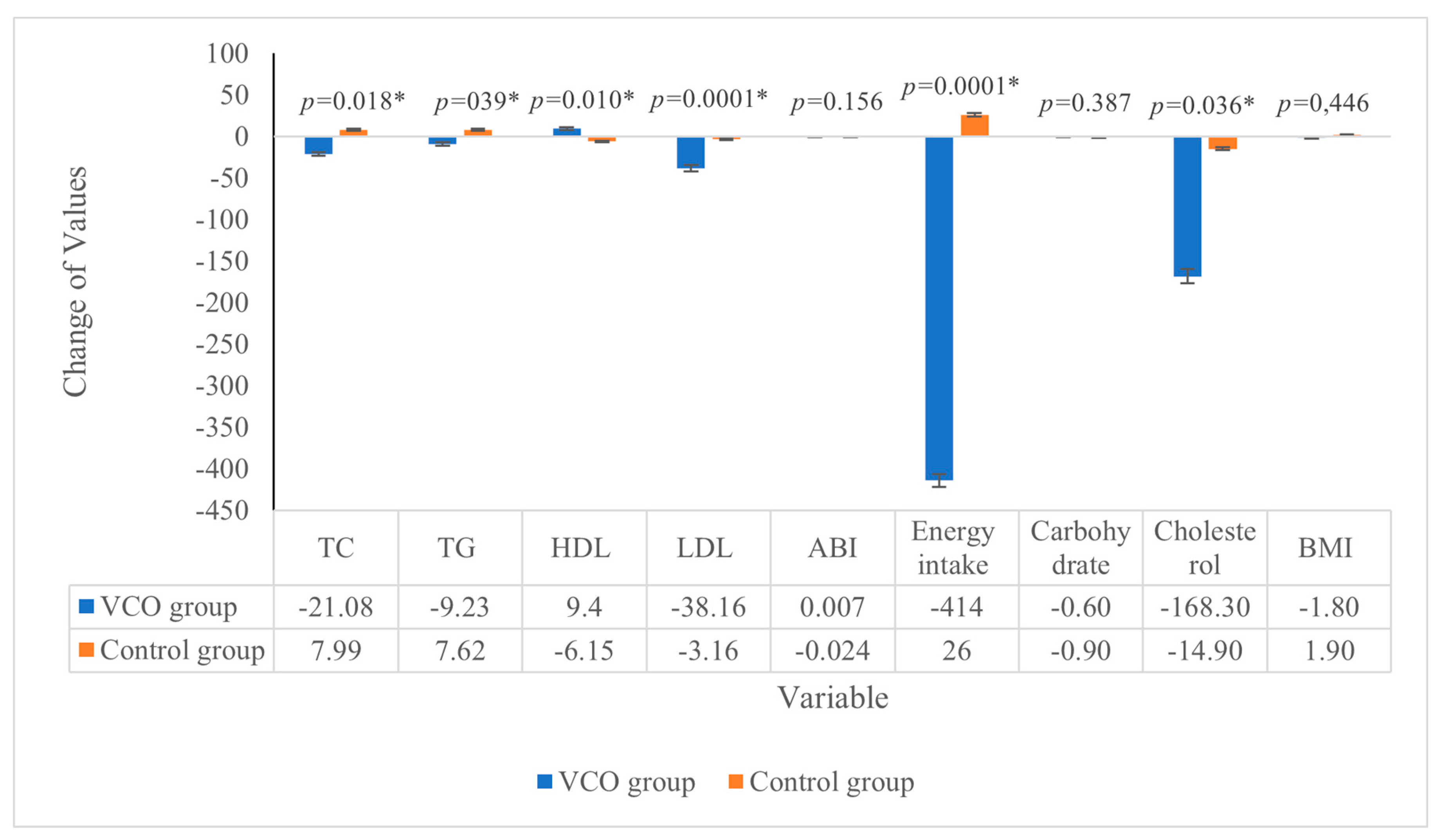
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Classification of Diabetes Mellitus 2019; WHO: Geneva, Switzerland, 2019; pp. 1–13. [Google Scholar]
- Mezil, S.A.; Abed, B.A. Complication of diabetes mellitus. Ann. Rom. Soc. Cell Biol. 2021, 25, 1546–1556. Available online: https://www.researchgate.net/publication/351436982 (accessed on 14 May 2022).
- White, J.; Swerdlow, D.; Preiss, D.; Fairhurst-Hunter, Z.; Keating, B.J.; Asselbergs, F.; Sattar, N.; Humphries, S.E.; Hingorani, A.; Holmes, M.V. Association of lipid fractions with risks for coronary artery disease and diabetes. JAMA Cardiol. 2016, 1, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Aday, A.W.; Everett, B.M. Dyslipidemia profiles in patients with peripheral artery disease. Curr. Cardiol. Rep. 2019, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global epidemiology of diabetic foot ulceration: A systematic review and meta-analysis†. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Kanda, E.; Ai, M.; Okazaki, M.; Maeda, Y.; Sasaki, S.; Yoshida, M. The association of very-low-density lipoprotein with ankle-brachial index in peritoneal dialysis patients with controlled serum low-density lipoprotein cholesterol level. BMC Nephrol. 2013, 14, 1. [Google Scholar] [CrossRef]
- Schofield, J.D.; Liu, Y.; Rao-Balakrishna, P.; Malik, R.A.; Soran, H. Diabetes Dyslipidemia. Diabetes Ther. 2016, 7, 203–219. [Google Scholar] [CrossRef]
- Wittlinger, T.; Schwaab, B.; Völler, H.; Bongarth, C.; Heinze, V.; Eckrich, K.; Guha, M.; Richter, M.; Schlitt, A. Efficacy of lipid-lowering therapy during cardiac rehabilitation in patients with diabetes mellitus and coronary heart disease. J. Cardiovasc. Dev. Dis. 2021, 8, 105. [Google Scholar] [CrossRef]
- Margata, L.; Silalahi, J.; Harahap, U.; Satria, D. The effect of hydrolyzed virgin coconut oil on lipid profile and liver enzymes in dyslipidemic rats. Asian J. Pharm. Clin. Res. 2018, 11, 406–409. [Google Scholar] [CrossRef]
- Caesario, J.; Adi, S.; Qurnianingsih, E. The Effect of simvastatin and virgin coconut oil (VCO) combination therapy as triglyceride plasma lowering agent in white dyslipidemic male rat (Rattus norvegicus). Biomol. Health Sci. J. 2021, 4, 85. [Google Scholar] [CrossRef]
- Chinwong, S.; Chinwong, D.; Mangklabruks, A. Daily consumption of virgin coconut oil increases high-density lipoprotein cholesterol levels in healthy volunteers: A randomized crossover trial. Evid.-Based Complement. Altern. Med. 2017, 2017, 7251562. [Google Scholar] [CrossRef]
- Sinaga, F.A.; Samosir, A.S.; Sinaga, R.N.; Ayu, E.; Manalu, N.; A Ginting, A.; Zulaini. Effect of aerobic exercise and supplementation virgin coconut oil on lipid profile. J. Phys. Conf. Ser. 2021, 1811, 1–7. [Google Scholar] [CrossRef]
- Illam, S.P.; Narayanankutty, A.; Raghavamenon, A.C. Polyphenols of virgin coconut oil prevent pro-oxidant mediated cell death. Toxicol. Mech. Methods 2017, 27, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Okpiabhele, A.O.; Nw, E.A.C.; Abu, O.D. Therapeutic Potential of Virgin Coconut Oil in Ameliorating Diabetes Mellitus and Hepatotoxicity Using Rattus Norvegicus as Case Study. Asian J. Biol. Sci. 2018, 11, 138–144. [Google Scholar] [CrossRef]
- Narayanankutty, A.; Palliyil, D.M.; Kuruvilla, K.; Raghavamenon, A.C. Virgin coconut oil reverses hepatic steatosis by restoring redox homeostasis and lipid metabolism in male Wistar rats. J. Sci. Food Agric. 2018, 98, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Famurewa, A.C.; Ejezie, F.E. Polyphenols isolated from virgin coconut oil attenuate cadmium-induced dyslipidemia and oxidative stress due to their antioxidant properties and potential benefits on cardiovascular risk ratios in rats. Avicenna J. Phytomedicine 2018, 8, 73–84. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29387575%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC5787998 (accessed on 17 May 2022).
- Alghamdi, S.A. Potential antidiabetic and antioxidant effects of coconut oil on streptozotocin-induced diabetes in male Sprague-Dawley rats. Int. J. Pharm. Phytopharm. Res. 2019, 9, 68–76. Available online: www.eijppr.com (accessed on 17 May 2022).
- Maidin, N.Q.H.; Ahmad, N. Protective and antidiabetic effects of virgin coconut oil (VCO) on blood glucose concentrations in alloxan induced diabetic rats. Int. J. Pharm. Pharm. Sci. 2015, 7, 57–60. [Google Scholar]
- Rahmawati; Wiyani, L.; Aladin, A.; Putra, B.; Muliani. Antidiabetic effect of the virgin coconut oil and the virgin coconut oil emulsions. Syst. Rev. Pharm. 2020, 11, 243–246. [Google Scholar]
- Lasari, S.D.; Syafrizayanti; Tjong, D.H.; Purwati, E.; Syukur, S. The Effect of Virgin Coconut Oil (Vco) as an antidiabetic and on lipid profile in alloxan–induced white male mice (Mus Musculus). Int. Res. J. Pharm. 2019, 10, 5–9. [Google Scholar] [CrossRef]
- Mitic-Culafic, D.; Djurasevic, S.; Todorovic, Z.; Knezevic-Vukcevic, J.; Djordjevic, J.; Nikolic, B. Effect of virgin coconut oil on caecal microbiota composition in alloxan-induced diabetic rats. IOP Conf. Ser. Earth Environ. Sci. 2019, 333, 012080. [Google Scholar] [CrossRef]
- Sampson, M.; Ling, C.; Sun, Q.; Harb, R.; Ashmaig, M.; Warnick, R.; Sethi, A.; Fleming, J.K.; Otvos, J.D.; Meeusen, J.W.; et al. A New Equation for Calculation of Low-Density Lipoprotein Cholesterol in Patients with Normolipidemia and/or Hypertriglyceridemia. JAMA Cardiol. 2020, 5, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.-T.; Sharp, S.J.; Finikarides, L.; Afzal, I.; Lentjes, M.; Luben, R.; Forouhi, N.G. Randomised trial of coconut oil, olive oil or butter on blood lipids and other cardiovascular risk factors in healthy men and women. BMJ Open 2018, 8, e020167. [Google Scholar] [CrossRef] [PubMed]
- Lwanga, S.K.; Lameshow, S. Sample Size Determination in Health Studies: A Practical Manual; World Health Organization: Geneva, Switzerland, 1991; pp. 9–10. 28p, Available online: https://apps.who.int/iris/bitstream/handle/10665/40062/9241544058_%28p1-p22%29.pdf?sequence=1&isAllowed=y (accessed on 28 December 2022).
- Barone Gibbs, B.; Dobrosielski, D.A.; Althouse, A.D.; Stewart, K.J. The effect of exercise training on ankle-brachial index in type 2 diabetes. Atherosclerosis 2013, 230, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Rohman, A.; Irnawati; Erwanto, Y.; Lukitaningsih, E.; Rafi, M.; Fadzilah, N.A.; Windarsih, A.; Sulaiman, A.; Zakaria, Z. Virgin coconut oil: Extraction, physicochemical properties, biological activities and its authentication analysis. Food Rev. Int. 2021, 37, 46–66. [Google Scholar] [CrossRef]
- Amelia, R.; Harahap, J.; Yunanda, Y.; Wijaya, H.; Fujiati, I.I.; Yamamoto, Z. Early detection of macrovascular complications in type 2 diabetes mellitus in Medan, North Sumatera, Indonesia: A cross-sectional study. F1000Research 2021, 10, 808. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.T.A.; Tran, G.B.; Le, T.D.; Phan, U.T.X. The effect of different free fatty acid fractions from hydrolyzed virgin coconut oil on changes of lipid profile and liver morphology induced by high fat diet: An in vivo study. J. Teknol. 2022, 84, 145–152. [Google Scholar] [CrossRef]
- Kumar, V.M.; Vasudevan, D.M.; Sundaram, K.R.; Krishnan, S.; Chandrasekhar, R.; Mathew, N.; Nandakumar, S. Effect of virgin coconut oil on lipid profile and other CVD risk factors. Indian J. Nutr. 2022, 9, 1–5. Available online: https://www.opensciencepublications.com/wp-content/uploads/IJN-2395-2326-9-257.pdf (accessed on 1 January 2023).
- Loung, F.S.; Silalahi, J.; Suryanto, D. Antibacterial activity of enzymatic hydrolyzed of virgin coconut oil and palm kernel oil against staphylococcus aureus, Salmonella thypi and Escherichia coli. Int. J. PharmTech Res. 2014, 6, 628–633. [Google Scholar]
- Ali, K.M.; Wonnerth, A.; Huber, K.; Wojta, J. Cardiovascular disease risk reduction by raising HDL cholesterol—Current therapies and future opportunities. Br. J. Pharmacol. 2012, 167, 1177–1194. [Google Scholar] [CrossRef]
- Vogel, C.É.; Crovesy, L.; Rosado, E.L.; Soares-Mota, M. Effect of coconut oil on weight loss and metabolic parameters in men with obesity: A randomized controlled clinical trial. Food Funct. 2020, 11, 6588–6594. [Google Scholar] [CrossRef]
- Panth, N.; Abbott, K.A.; Dias, C.B.; Wynne, K.; Garg, M.L. Differential effects of medium- and long-chain saturated fatty acids on blood lipid profile: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2018, 108, 675–687. [Google Scholar] [CrossRef] [PubMed]
- Iswendi, I.; Iryani, I.; Putra, R.F. Effect of virgin coconut oil from green coconut on high-density lipoprotein (HDL) levels in blood serum of white mice. EKSAKTA J. Sci. Data Anal. 2021, 2, 162–168. [Google Scholar] [CrossRef]
- van Schalkwijk, D.B.; Pasman, W.J.; Hendriks, H.F.J.; Verheij, E.R.; Rubingh, C.M.; van Bochove, K.; Vaes, W.H.J.; Adiels, M.; Freidig, A.P.; de Graaf, A.A. Dietary medium chain fatty acid supplementation leads to reduced VLDL lipolysis and uptake rates in comparison to linoleic acid supplementation. PLoS ONE 2014, 9, e100376. [Google Scholar] [CrossRef] [PubMed]
- Chambers, K.F.; Day, P.E.; Aboufarrag, H.T.; Kroon, P.A. Polyphenol effects on cholesterol metabolism via bile acid biosynthesis, CYP7A1: A review. Nutrients 2019, 11, 2588. [Google Scholar] [CrossRef] [PubMed]
- Akinnuga, A.M.; Jeje, S.O.; Bamidele, O.; Sunday, V.E. Dietary consumption of virgin coconut oil ameliorates lipid profiles in diabetic rats. J. Physiol. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Metin, Z.E.; Bilgic, P.; Metin, M.M.T.; Akkoca, M. Comparing acute effects of extra virgin coconut oil and extra virgin olive oil consumption on appetite and food intake in normal-weight and obese male subjects. PLoS ONE 2022, 17, e0274663. [Google Scholar] [CrossRef]
- Valente, F.X.; Cândido, F.G.; Lopes, L.L.; Dias, D.M.; Carvalho, S.D.L.; Pereira, P.F.; Bressan, J. Effects of coconut oil consumption on energy metabolism, cardiometabolic risk markers, and appetitive responses in women with excess body fat. Eur. J. Nutr. 2018, 57, 1627–1637. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | Intervention Group (n = 68) | Control Group (n = 68) | p-Values |
|---|---|---|---|
| Mean (s.d.) | Mean (s.d.) | ||
| Age (years) | 63.06 (8.4) | 48.00 (8.1) | <0.0001 *,a |
| Sex (% male) | 53.2 | 52.3% | 0.034 a |
| BMI (kg/m2) | 26.0 (3.5) | 26.7 (4.1) | 0.715 a |
| Energy intakes (kilocalories/day) | 1768 (346.7) | 1452 (462.9) | <0.0001 *,a |
| Carbohydrates intake (% of energy) | 43.3 (7.4) | 45.7 (6.7) | 0.525 b |
| Cholesterol intake (mg/day) | 373.6 (8.2) | 298.1 (7.6) | 0.528 b |
| Total cholesterol (mg/dL) | 247.69 (8.95) | 231,85 (8.69) | 0.167 a |
| Triglyceride (mg/dL) | 192.77 (3.27) | 135.46 (3.80) | 0.087 a |
| HDL (mg/dL) | 39.92 (1.44) | 47.15 (2.11) | 0.064 a |
| LDL (mg/dL) | 179.62 (7.75) | 156.31 (6.19) | 0.110 b |
| Ankle brachial index | 0.958 (0.09) | 0.987 (0.08) | 0.756 a |
| Variables | VCO Group | Control Group | ||||
|---|---|---|---|---|---|---|
| Mean at Baseline (s.d) | Mean at End-Point (s.d) | p-Values | Mean at Baseline (s.d) | Mean at End-Point (s.d) | p-Values | |
| Total cholesterol (mg/dL) | 247.69 (8.95) | 226.61 (8.05) | 0.127 a | 231.85 (8.69) | 239.84 (7.63) | 0.327 a |
| Triglyceride (mg/dL) | 192.77 (3.27) | 183.54 (4.96) | 0.88 a | 135.46 (3.80) | 143.08 (5.94) | 0.203 a |
| HDL (mg/dL) | 39.92 (1.44) | 49.32 (2.31) | 0.031 a,* | 47.15 (2.11) | 41.00 (2.67) | 0.062 a |
| LDL (mg/dL) | 179.62 (7.75) | 141.46 (7.15) | 0.002 b,* | 156.31 (6.19) | 153.15 (7.43) | 0.797 b |
| Ankle–brachial index | 0.958 (0.09) | 0.965 (0.06) | 0.653 a | 0.987 (0.08) | 0.963 (0.04) | 0.627 a |
| Energy intakes (kilocalories/day) | 1768 (346.7) | 1354 (257.9) | 0.046 a | 1452 (462.9) | 1478 (340.7) | 0.098 a |
| Carbohydrates intake (% of energy) | 43.3 (7.4) | 42.7 (7.2) | 0.374 a | 45.7 (6.7) | 44.8 (8.1) | 0.326 b |
| Cholesterol intake (mg/day) | 373.6 (8.2) | 205.3 (8.8) | 0.023 b | 298.1 (7.6) | 283.2 (6.9) | 0.376 b |
| BMI (kg/m2) | 26.0 (3.5) | 24.2 (4.2) | 0.284 a | 26.7 (4.1) | 28.6 (5.9) | 0.198 a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Setyawati, A.; Sangkala, M.S.; Malasari, S.; Jafar, N.; Sjattar, E.L.; Syahrul, S.; Rasyid, H. Virgin Coconut Oil: A Dietary Intervention for Dyslipidaemia in Patients with Diabetes Mellitus. Nutrients 2023, 15, 564. https://doi.org/10.3390/nu15030564
Setyawati A, Sangkala MS, Malasari S, Jafar N, Sjattar EL, Syahrul S, Rasyid H. Virgin Coconut Oil: A Dietary Intervention for Dyslipidaemia in Patients with Diabetes Mellitus. Nutrients. 2023; 15(3):564. https://doi.org/10.3390/nu15030564
Chicago/Turabian StyleSetyawati, Andina, Moh Syafar Sangkala, Silvia Malasari, Nuurhidayat Jafar, Elly L Sjattar, Syahrul Syahrul, and Haerani Rasyid. 2023. "Virgin Coconut Oil: A Dietary Intervention for Dyslipidaemia in Patients with Diabetes Mellitus" Nutrients 15, no. 3: 564. https://doi.org/10.3390/nu15030564
APA StyleSetyawati, A., Sangkala, M. S., Malasari, S., Jafar, N., Sjattar, E. L., Syahrul, S., & Rasyid, H. (2023). Virgin Coconut Oil: A Dietary Intervention for Dyslipidaemia in Patients with Diabetes Mellitus. Nutrients, 15(3), 564. https://doi.org/10.3390/nu15030564