
Immunonutrition in Orthopedic and Traumatic Patients

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search
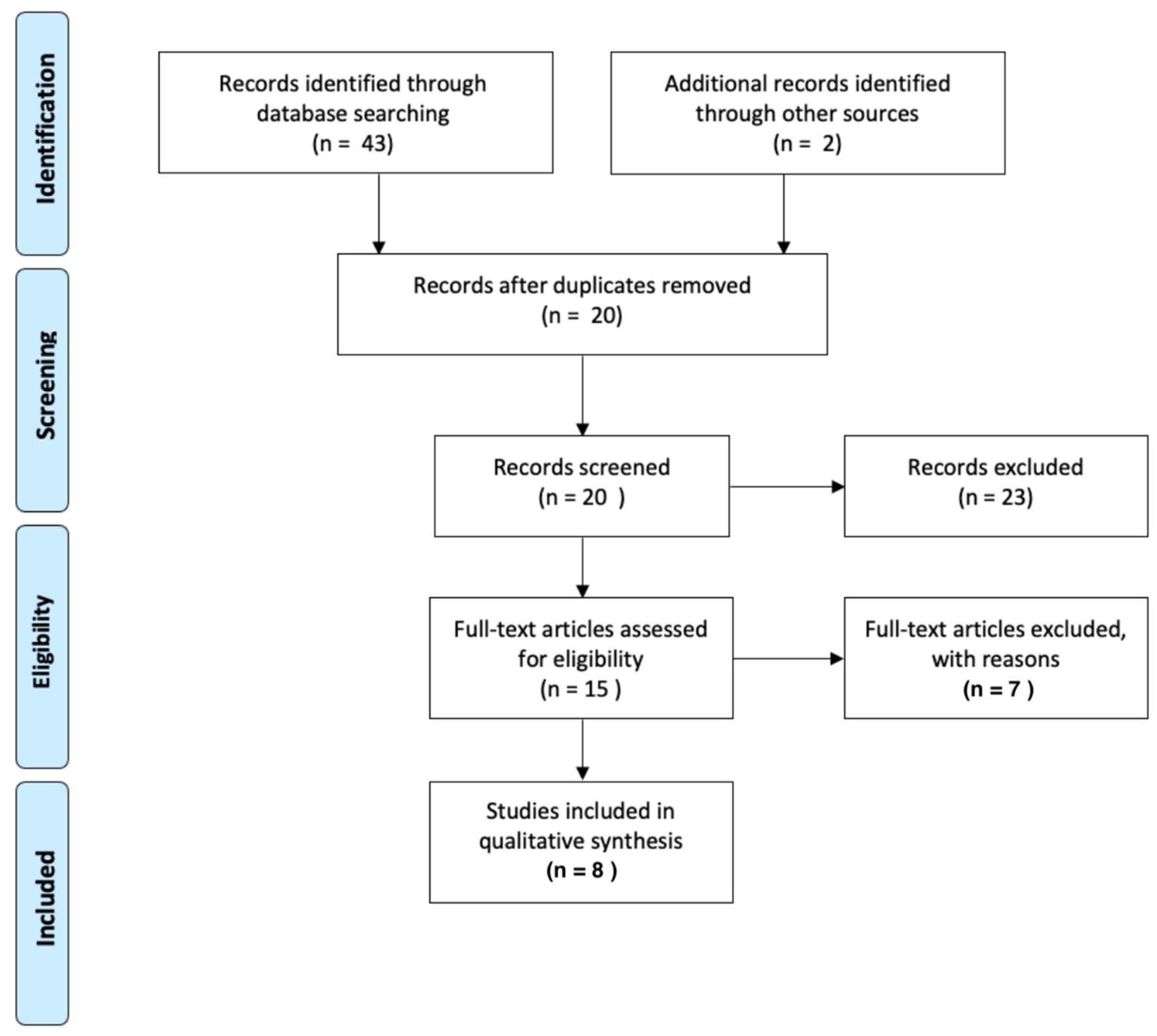
2.3. Study Selection
2.4. Data Collection Process
2.5. Data Extraction
3. Results
3.1. Non-Elective Trauma Orthopedics Studies
3.2. Elective Orthopedic Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Staa, T.P.; Dennison, E.M.; Leufkens, H.G.; Cooper, C. Epidemiology of fractures in England and Wales. Bone 2001, 29, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef] [PubMed]
- Brunner, L.C.; Eshilian-Oates, L.; Kuo, T.Y. Hip fractures in adults. Am. Fam. Physician 2003, 67, 537–542. [Google Scholar]
- Williamson, S.; Landeiro, F.; McConnell, T.; Fulford-Smith, L.; Javaid, M.K.; Judge, A.; Leal, J. Costs of fragility hip fractures globally: A systematic review and meta-regression analysis. Osteoporos. Int. 2017, 28, 2791–2800. [Google Scholar] [CrossRef]
- Bell, J.A.; Emara, A.K.; Barsoum, W.K.; Bloomfield, M.; Briskin, I.; Higuera, C.; Klika, A.K.; Krebs, V.E.; Mesko, N.W.; Molloy, R.M.; et al. Should an Age Cutoff Be Considered for Elective Total Knee Arthroplasty Patients? An Analysis of Operative Success Based on Patient-Reported Outcomes. J. Knee Surg. 2022. [Google Scholar] [CrossRef]
- Bala, A.; Ivanov, D.V.; Huddleston, J.I., 3rd; Goodman, S.B.; Maloney, W.J.; Amanatullah, D.F. The Cost of Malnutrition in Total Joint Arthroplasty. J. Arthroplast. 2020, 35, 926–932.e1. [Google Scholar] [CrossRef]
- Bohl, D.D.; Shen, M.R.; Kayupov, E.; Cvetanovich, G.L.; Della Valle, C.J. Is Hypoalbuminemia Associated With Septic Failure and Acute Infection After Revision Total Joint Arthroplasty? A Study of 4517 Patients From the National Surgical Quality Improvement Program. J. Arthroplast. 2016, 31, 963–967. [Google Scholar] [CrossRef]
- Medina-Contreras, O.; Luvián-Morales, J.; Valdez-Palomares, F.; Flores-Cisneros, L.; Sánchez-López, M.S.; Soto-Lugo, J.H.; Castro-Eguiluz, D. Immunonutrition in cervical cancer: Immune response modula-tion by diet. Rev. Investig. Clin. 2020, 72, 219–230. [Google Scholar] [CrossRef]
- Lorenz, K.J.; Schallert, R.; Daniel, V. Immunonutrition—The influence of early postoperative glutamine supplementation in enteral/parenteral nutrition on immune response, wound healing and length of hospital stay in multiple trauma patients and patients after extensive surgery. GMS Interdiscip. Plast Reconstr. Surg. DGPW 2015, 4, Doc15. [Google Scholar] [CrossRef]
- Braga, M.; Gianotti, L.; Vignali, A.; Carlo, V.D. Preoperative oral arginine and n-3 fatty acid supplementation improves the immunometabolic host response and outcome after colorectal resection for cancer. Surgery 2002, 132, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Weimann, A.; Bastian, L.; Bischoff, W.E.; Grotz, M.; Hansel, M.; Lotz, J.; Trautwein, C.; Tusch, G.; Schlitt, H.J.; Regel, G. Influence of arginine, omega-3 fatty acids and nucleotide-supplemented enteral support on systemic inflammatory response syndrome and multiple organ failure in patients after severe trauma. Nutrition 1998, 14, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Carli, F.; Evans, D.C.; Guilbert, S.; Kozar, R.; Pryor, A.; Thiele, R.H.; Everett, S.; Grocott, M.; Gan, T.J.; et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Nutrition Screening and Therapy Within a Surgical Enhanced Recovery Pathway. Anesth. Analg. 2018, 126, 1883–1895. [Google Scholar] [CrossRef]
- Scott, M.J.; Fawcett, W.J. Oral carbohydrate preload drink for major surgery—The first steps from famine to feast. Anaesthesia. 2014, 69, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Moya, P.; Soriano-Irigaray, L.; Ramirez, J.M.; Garcea, A.; Blasco, O.; Blanco, F.J.; Brugiotti, C.; Miranda, E.; Arroyo, A. Perioperative Standard Oral Nutrition Supplements Versus Immunonutrition in Patients Undergoing Colorectal Resection in an Enhanced Recovery (ERAS) Protocol: A Multicenter Randomized Clinical Trial (SONVI Study). Medicine 2016, 95, e3704. [Google Scholar] [CrossRef]
- Kratzing, C. Pre-operative nutrition and carbohydrate loading. Proc. Nutr. Soc. 2011, 70, 311–315. [Google Scholar] [CrossRef]
- Serhan, C.N.; Chiang, N.; Van Dyke, T.E. Resolving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators. Nat. Rev. Immunol. 2008, 8, 349–361. [Google Scholar] [CrossRef]
- Houdijk, A.P.; Van Leeuwen, P.A.; Boermeester, M.A.; Van Lambalgen, T.; Teerlink, T.; Flinkerbusch, E.L.; Sauerwein, H.P.; Wesdorp, R.I. Glutamine-enriched enteral diet increases splanchnic blood flow in the rat. Am. J. Physiol. 1994, 267, G1035–G1040. [Google Scholar] [CrossRef]
- Reynolds, J.V.; Daly, J.M.; Shou, J.; Sigal, R.; Ziegler, M.M.; Naji, A. Immunologic effects of arginine supplementation in tumor-bearing and non-tumor-bearing hosts. Ann. Surg. 1990, 211, 202–210. [Google Scholar] [CrossRef]
- Waitzberg, D.L.; Saito, H.; Plank, L.D.; Jamieson, G.G.; Jagannath, P.; Hwang, T.L.; Mijares, J.M.; Bihari, D. Postsurgical infections are reduced with specialized nutrition support. World J. Surg. 2006, 30, 1592–1604. [Google Scholar] [CrossRef]
- Marik, P.E.; Flemmer, M. Immunonutrition in the surgical patient. Minerva Anestesiol. 2012, 78, 336–342. [Google Scholar] [PubMed]
- Daigle, M.E.; Weinstein, A.M.; Katz, J.N.; Losina, E. The cost-effectiveness of total joint arthroplasty: A systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 2012, 26, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.C.; Phillips, S.M.; Wainwright, T.W. What Is the Role of Nutritional Supplements in Support of Total Hip Replacement and Total Knee Replacement Surgeries? A Systematic Review. Nutrients 2018, 10, 820. [Google Scholar] [CrossRef] [PubMed]
- Greene, K.A.; Wilde, A.H.; Stulberg, B.N. Preoperative nutritional status of total joint patients. Relationship to postoperative wound complications. J. Arthroplast. 1991, 6, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Braga, M. The 2015 ESPEN Arvid Wretlind lecture. Evolving concepts on perioperative metabolism and support. Clin. Nutr. 2016, 35, 7–11. [Google Scholar] [CrossRef]
- Hamilton-Reeves, J.M.; Stanley, A.; Bechtel, M.D.; Yankee, T.M.; Chalise, P.; Hand, L.K.; Lee, E.K.; Smelser, W.; Mirza, M.; Wyre, H.; et al. Perioperative Immunonutrition Modulates Inflammatory Response after Radical Cystectomy: Results of a Pilot Randomized Controlled Clinical Trial. J. Urol. 2018, 200, 292–301. [Google Scholar] [CrossRef]
- Celik, J.B.; Gezginc, K.; Ozcelik, K.; Celik, C. The role of immunonutrition in gynecologic oncologic surgery. Eur. J. Gynaecol. Oncol. 2009, 30, 418–421. [Google Scholar]
- Marik, P.E.; Zaloga, G.P. Immunonutrition in critically ill patients: A systematic review and analysis of the literature. Intensive Care Med. 2008, 34, 1980–1990. [Google Scholar] [CrossRef]
- Alito, M.A.; de Aguilar-Nascimento, J.E. Multimodal perioperative care plus immunonutrition versus traditional care in total hip arthroplasty: A randomized pilot study. Nutr. J. 2016, 15, 34. [Google Scholar] [CrossRef]
- Goncalves, T.J.M.; Goncalves, S.; Nava, N.; Jorge, V.C.; Okawa, A.M.; Rocha, V.A.; Forato, L.C.H.; Furuya, V.A.O.; Martins, S.S.; Oksman, D. Perioperative Immunonutrition in Elderly Patients Undergoing Total Hip and Knee Arthroplasty: Impact on Postoperative Outcomes. JPEN J. Parenter. Enteral Nutr. 2021, 45, 1559–1566. [Google Scholar] [CrossRef]
- Kudsk, K.A.; Minard, G.; Croce, M.A.; Brown, R.O.; Lowrey, T.S.; Pritchard, F.E.; Dickerson, R.N.; Fabian, T.C. A randomized trial of isonitrogenous enteral diets after severe trauma. An immune-enhancing diet reduces septic complications. Ann. Surg. 1996, 224, 531–540, discussion 540–533. [Google Scholar] [CrossRef]
- Wainwright, T.W. Enhanced Recovery after Surgery (ERAS) for Hip and Knee Replacement-Why and How It Should Be Implemented Following the COVID-19 Pandemic. Medicina 2021, 57, 81. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W.; Kehlet, H. Fast-track hip and knee arthroplasty—Have we reached the goal? Acta Orthop. 2019, 90, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Glassou, E.N.; Pedersen, A.B.; Hansen, T.B. Risk of re-admission, reoperation, and mortality within 90 days of total hip and knee arthroplasty in fast-track departments in Denmark from 2005 to 2011. Acta Orthop. 2014, 85, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Bastian, L.; Weimann, A.; Bischoff, W.; Meier, P.N.; Grotz, M.; Stan, C.; Regel, G. [Clinical effects of supplemental enteral nutrition solution in severe polytrauma]. Unfallchirurg 1998, 101, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Briassoulis, G.; Filippou, O.; Kanariou, M.; Papassotiriou, I.; Hatzis, T. Temporal nutritional and inflammatory changes in children with severe head injury fed a regular or an immune-enhancing diet: A randomized, controlled trial. Pediatr. Crit. Care Med. 2006, 7, 56–62. [Google Scholar] [CrossRef]
- Rai, V.R.H.; Phang, L.F.; Sia, S.F.; Amir, A.; Veerakumaran, J.S.; Kassim, M.K.A.; Othman, R.; Tah, P.C.; Loh, P.S.; Jailani, M.I.O.; et al. Effects of immunonutrition on biomarkers in traumatic brain injury patients in Malaysia: A prospective randomized controlled trial. BMC Anesthesiol. 2017, 17, 81. [Google Scholar] [CrossRef] [PubMed]
- van Vliet, I.M.Y.; Gomes-Neto, A.W.; de Jong, M.F.C.; Jager-Wittenaar, H.; Navis, G.J. High prevalence of malnutrition both on hospital admission and predischarge. Nutrition 2020, 77, 110814. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.L.; Nielsen, R.L.; Houlind, M.B.; Tavenier, J.; Rasmussen, L.J.H.; Jorgensen, L.M.; Treldal, C.; Beck, A.M.; Pedersen, M.M.; Andersen, O.; et al. Risk of Malnutrition upon Admission and after Discharge in Acutely Admitted Older Medical Patients: A Prospective Observational Study. Nutrients 2021, 13, 2757. [Google Scholar] [CrossRef]
- Leiva Badosa, E.; Badia Tahull, M.; Virgili Casas, N.; Elguezabal Sangrador, G.; Faz Mendez, C.; Herrero Meseguer, I.; Izquierdo Gonzalez, A.; Lopez Urdiales, R.; Oca Burguete, F.J.; Tubau Molas, M.; et al. Hospital malnutrition screening at admission: Malnutrition increases mortality and length of stay. Nutr. Hosp. 2017, 34, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Gu, A.; Malahias, M.A.; Strigelli, V.; Nocon, A.A.; Sculco, T.P.; Sculco, P.K. Preoperative Malnutrition Negatively Correlates with Postoperative Wound Complications and Infection after Total Joint Arthroplasty: A Systematic Review and Meta-Analysis. J. Arthroplast. 2019, 34, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Reddavide, R.; Rotolo, O.; Caruso, M.G.; Stasi, E.; Notarnicola, M.; Miraglia, C.; Nouvenne, A.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F.; et al. The role of diet in the prevention and treatment of Inflammatory Bowel Diseases. Acta Biomed. 2018, 89, 60–75. [Google Scholar] [CrossRef]
- Buzquurz, F.; Bojesen, R.D.; Grube, C.; Madsen, M.T.; Gogenur, I. Impact of oral preoperative and perioperative immunonutrition on postoperative infection and mortality in patients undergoing cancer surgery: Systematic review and meta-analysis with trial sequential analysis. BJS Open 2020, 4, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Zhang, J.; Zhang, L.; Wu, J.; Zhan, Z. Enteral immunonutrition versus enteral nutrition for gastric cancer patients undergoing a total gastrectomy: A systematic review and meta-analysis. BMC Gastroenterol. 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.; Herbert, G.; Atkinson, C.; England, C.; Northstone, K.; Baos, S.; Brush, T.; Chong, A.; Ness, A.; Harris, J.; et al. Pre-admission interventions (prehabilitation) to improve outcome after major elective surgery: A systematic review and meta-analysis. BMJ Open 2021, 11, e050806. [Google Scholar] [CrossRef]
- Kanekiyo, S.; Takeda, S.; Iida, M.; Nishiyama, M.; Kitahara, M.; Shindo, Y.; Tokumitsu, Y.; Tomochika, S.; Tsunedomi, R.; Suzuki, N.; et al. Efficacy of perioperative immunonutrition in esophageal cancer patients undergoing esophagectomy. Nutrition 2019, 59, 96–102. [Google Scholar] [CrossRef]
- Efstathopoulos, N.; Bathrellos, E.; Giamarellos-Bourboulis, E.J.; Lazarettos, J.; Papalois, A.; Grecka, P.; Nikolaou, V. N-6 polyunsaturated fatty acids confer hemodynamic stability in an experimental model of multiple trauma. Prostaglandins. Leukot Essent. Fat. Acids 2005, 72, 357–362. [Google Scholar] [CrossRef]
- Svetikiene, M.; Ringaitiene, D.; Vezeliene, J.; Isajevas, V.; Trybe, D.; Vicka, V.; Malickaite, R.; Jurgauskiene, L.; Norkuniene, J.; Serpytis, M.; et al. The efficacy of early postoperative enteral immunonutrition on T-lymphocyte count: A randomised control study in low-risk cardiac surgery patients. Clin. Nutr. 2021, 40, 372–379. [Google Scholar] [CrossRef]
- Rinonapoli, G.; Gregori, P.; Di Matteo, B.; Impieri, L.; Ceccarini, P.; Manfreda, F.; Campofreda, G.; Caraffa, A. Stem cells application in meniscal tears: A systematic review of pre-clinical and clinical evidence. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7754–7764. [Google Scholar] [CrossRef]
- Marano, L.; Porfidia, R.; Pezzella, M.; Grassia, M.; Petrillo, M.; Esposito, G.; Braccio, B.; Gallo, P.; Boccardi, V.; Cosenza, A.; et al. Clinical and immunological impact of early postoperative enteral immunonutrition after total gastrectomy in gastric cancer patients: A prospective randomized study. Ann. Surg. Oncol 2013, 20, 3912–3918. [Google Scholar] [CrossRef] [PubMed]
- Abunnaja, S.; Cuviello, A.; Sanchez, J.A. Enteral and parenteral nutrition in the perioperative period: State of the art. Nutrients 2013, 5, 608–623. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, M.; Chiabrando, J.G.; Vescovo, G.M.; Bressi, E.; Del Buono, M.G.; Carbone, S.; Koenig, R.A.; Van Tassell, B.W.; Abbate, A.; Biondi-Zoccai, G.; et al. Impact of Different Doses of Omega-3 Fatty Acids on Cardiovascular Outcomes: A Pairwise and Network Meta-analysis. Curr. Atheroscler. Rep. 2020, 22, 45. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.W.; Zhou, L.; Liu, Z.Z.; Pei, D.P.; Fan, W.Q.; Ning, W. A Systematic Review and Meta-Analysis of the Effects of Perioperative Immunonutrition in Gastrointestinal Cancer Patients. Nutr. Cancer 2021, 73, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-León, A.M.; Lapuente, M.; Estruch, R.; Casas, R. Clinical Advances in Immunonutrition and Atherosclerosis: A Review. Front. Immunol. 2019, 10, 837. [Google Scholar] [CrossRef]
- Eneroth, M.; Olsson, U.B.; Thorngren, K.G. Nutritional supplementation decreases hip fracture-related complications. Clin. Orthop. Relat. Res. 2006, 451, 212–217. [Google Scholar] [CrossRef]
- Cederholm, T.; Hedström, M. Nutritional treatment of bone fracture. Current. Opin. Clin. Nutr. Metab. Care 2005, 8, 377–381. [Google Scholar] [CrossRef]
- Calori, G.M.; Albisetti, W.; Agus, A.; Iori, S.; Tagliabue, L. Risk factors contributing to fracture non-unions. Injury 2007, 38, S11–S18. [Google Scholar] [CrossRef]
- Nicholson, J.A.; Dowrick, A.S.; Liew, S.M. Nutritional status and short-term outcome of hip arthroplasty. J. Orthop. Surg. 2012, 20, 331–335. [Google Scholar] [CrossRef]


{kind=link}
| Study | Year | Case Formula | Control Formula | Type of Study | Trauma/Surgery | Number of Patients |
|---|---|---|---|---|---|---|
| Kudsk et al. [31] | 1996 | [IED]Immun-Aid, McGaw, Inc., Irvine, CA | Promote [Ross Laboratories, Columbus, OH] and Casec [Mead-Johnson Nutritionals, Evansville, IN] | Prospective | Emergency abdominal surgery (celiotomy) | 35 |
| Weimann et al. [12] | 1998 | IMPACT, Sandoz Nutrition, Beme, Switzerland | Sandoz Nutrition, Beme, Switzerland | Prospective | Emergency thorax and abdominal surgery (celiotomy) | 32 |
| Bastian et al. [36] | 1998 | Sandoz Nutrition, Berna | Unspecified isocaloric and isonitrogenic | Prospective | No-surgery/emergency thorax and abdominal surgery (celiotomy) | 29 |
| Briassoulis et al. [37] | 2006 | Stresson (N.V.NUTRICIA, Zoetermeer, The Netherlands) | Tentrini (N.V.NUTRICIA) | Prospective | Mechanically ventilated children with severe head injury | 40 |
| Lorenz et al. [10] | 2015 | Not specified enteral parenteral isocaloric nutrition with glutamine supplementation | Not specified | Prospective | Extensive ear, nose, and throat tumor surgery and multiple-trauma patients | 22 |
| Rai et al. [38] | 2017 | Neomune | Fresubin HP energy | Prospective | Moderate to severe head injuries requiring enteral nutrition. Surgical and non-surgical patients | 36 |
| Study | Follow-Up | Route | Feeding Protocol | Results |
|---|---|---|---|---|
| Kudsk et al. [31] | Hospital stay | Jejunostomy | 200 mL/die. | Hospital stay, infectious complications, hospital costs, and antibiotic usage were significantly higher in the group not fed with an immune-enhanced diet. |
| Weimann et al. [12] | Hospital stay | Nasoduodenal tube or jejunostomy | A quantity of 25 mL/h for 18 h per die, stopping for the night between 12:00 PM and 6:00 AM. The feeding rate increased by 25 mL/h from day to day, up to a final rate of 150 mL/h. Simultaneously with enteral nutrition, patients were also fed parenterally until complete enteral coverage of the caloric requirements of 35–40 kcal per kg. | Significantly fewer days of Systemic Inflammatory Response Syndrome (SIRS) per patient and lower scores for the Multiple Organ Failure (MOF) score were observed; outcome and hospital stay were not influenced. |
| Bastian et al. [36] | Hospital stay | Nasoduodenal tube or jejunostomy | 561 ± 266 mL mean/die. | Significant reduction of Systemic Inflammatory Response Syndrome (SIRS), no impact on mortality, intensive care unit, or hospital stay. |
| Briassoulis et al. [37] | Hospital stay | Nasogastric tube | Hourly amount protocol for the children: energy intake equal to 0.50%, 100%, 125%, 150%, and 150% of the Predicted Basal Metabolic Rate (PBMR) on days 1–5, respectively. Enteral feeding was increased during the first five days, eventually reaching 150% of the PBMR. | Significantly lower interleukin-8 levels and positive gastric cultures. No differences were found in nosocomial infections, length of stay, length of mechanical ventilation, or survival. |
| Lorenz et al. [10] | Hospital stay | Enteral not specified | Not specified. | Decreased septic complications, length of hospital stays, length of intensive care unit, and time for wound healing. A small cohort of patients and little data reported. |
| Rai et al. [38] | Six months | Nasogastric tube | The target calorie for each patient was determined by the clinician working alongside the dietitian using the Harris–Benedict equation, which measures resting energy expenditure. Enteral feeding was commenced at an initial rate of 20 mL/h and increased by 20 mL/h every 6 h until the target calorie was reached. | IL-6 levels were significantly reduced, whereas glutathione levels were significantly higher following feeding with immunonutrition. Only inflammatory blood curves are analyzed, not clinical or economic benefits. |
| Study | Formula | Control |
|---|---|---|
| Kudsk et al. [31] | Water, Corn Maltodextrin, Sodium Caseinate, Soy Protein Isolate, Soy Oil, Sugar. Less than 0.5% of Medium Chain Triglycerides, Safflower Oil, Natural and Artificial Flavors, Calcium Citrate, Potassium Chloride, Magnesium Phosphate, Potassium Citrate, Calcium Phosphate, Soy Lecithin, Choline Chloride, Ascorbic Acid, Taurine, l-Carnitine, DL Alpha-Tocopheryl Acetate, Ferrous Sulfate, Zinc Sulfate, Manganese Sulfate, Niacinamide, Calcium Pantothenate, Copper Sulfate, Riboflavin, Thiamine Hydrochloride, Pyridoxine Hydrochloride, Vitamin A Palmitate, Beta-Carotene, Chromium Chloride, Folic Acid, Potassium Iodide, Sodium Molybdate, Sodium Selenate, Phylloquinone, Biotin, Vitamin D3, and Vitamin B12 | Water, Corn Maltodextrin, Sodium Caseinate, Soy Protein Isolate, Soy Oil, and Sugar |
| Weimann et al. [12] | Water, Sugar, Calcium Caseinate (Milk), Sodium Caseinate, l-Arginine, Refined Fish Oil (anchovy and sardine) and less than 2% of Corn Oil, Citric Acid, Medium Chain Triglycerides, Maltodextrin, Natural and Artificial Flavor, Yeast Extract, Potassium Citrate, Potassium Chloride, Calcium Phosphate, Magnesium Phosphate, Salt, Magnesium Chloride, Cellulose Gel, Cellulose Gum, Choline Chloride, Sodium Ascorbate, Sucralose (Sweetener), Carrageenan, Zinc Sulfate, Ferrous Sulfate, D Alpha-Tocopherol, Niacinamide, Soybean Oil, DL Alpha-Tocopheryl Acetate, Calcium Pantothenate, Copper Gluconate, Manganese Sulfate, Vitamin A Palmitate, Pyridoxine Hydrochloride, Riboflavin, Thiamine Hydrochloride, Beta-Carotene, Folic Acid, Potassium Iodide, Sodium Selenite, Sodium Molybdate, Chromium Chloride, Vitamin K1, Biotin, Vitamin D3, and Vitamin B1 | Sugar, Whey (Milk) Protein, Maltodextrin, l-Arginine, Fish Oil, Minerals (Potassium Dihydrogen Phosphate, Ferrous Sulphate, Zinc Sulfate, Potassium Iodide, Copper Gluconate, Chromium Trichloride, Manganese Sulfate, Sodium Selenite, Sodium Molybdate, and Sodium Fluoride), Partially hydrolyzed Guar gum fire, Medium Chain Triglycerides Oil, Corn Oil, Acidity regulator (Citric Acid), Flavors (Mango, Grapefruit, and Passion fruit), Ribonucleic Acid Sodium Salt, Vitamins (C, E, B5, A, D, Niacin, B6, B1, B2, K, Folic Acid, and d-Biotin), Stabilizer (Xanthan gum), Choline Bitartrate, Emulsifier (Soy Lecithin), Colors (Beta Carotene and Beetroot Red), Antioxidants (l-Ascorbyl Palmitate and Tocopherol Rich-extract). Gluten free |
| Bastian et al. [36] | Water, Sugar, Calcium Caseinate (Milk), Sodium Caseinate, l-Arginine, Refined Fish Oil (anchovy and sardine) and less than 2% of Corn Oil, Citric Acid, Medium Chain Triglycerides, Maltodextrin, Natural and Artificial Flavor, Yeast Extract, Potassium Citrate, Potassium Chloride, Calcium Phosphate, Magnesium Phosphate, Salt, Magnesium Chloride, Cellulose Gel, Cellulose Gum, Choline Chloride, Sodium Ascorbate, Sucralose (Sweetener), Carrageenan, Zinc Sulfate, Ferrous Sulfate, D Alpha-Tocopherol, Niacinamide, Soybean Oil, DL Alpha-Tocopheryl Acetate, Calcium Pantothenate, Copper Gluconate, Manganese Sulfate, Vitamin A Palmitate, Pyridoxine Hydrochloride, Riboflavin, Thiamine Hydrochloride, Beta-Carotene, Folic Acid, Potassium Iodide, Sodium Selenite, Sodium Molybdate, Chromium Chloride, Vitamin K1, Biotin, Vitamin D3, and Vitamin B12 | Not specified |
| Briassoulis et al. [37] | Nitrogen, Casein l-Arginine, l-Glutamine, Sugar, Lactose, Polysaccharides, Saturates, Mono unsaturates, Polyunsaturated Linoleic acid, Alpha-Linolenic acid, Docosahexaenoic acid, Eicosapentaenoic acid, Sodium, Potassium, Calcium, Phosphate, Magnesium, Vitamin E, Carotenoids, Taurine, Carnitine, Selenium, Zinc, and Copper | Water, Maltodextrin, Fructose, Potassium Citrate, Sodium Citrate, Acidity Regulator (Citric Acid), Flavoring, and Sweeteners (Acesulfame K and Sodium Saccharin) |
| Lorenz et al. [10] | Not specified: enteral parenteral isocaloric nutrition with glutamine supplementation | Not specified |
| Rai et al. [38] | Maltodextrin, Sodium Caseinate, Medium chain Triglycerides Oil, Dry Omega-3, Arginine, Fructose, Poly Dextrose, Corn Oil, Glutamine, Citric Acid Anhydrous (Acidity Regulator), Trehalose (Sweetener), Potassium Chloride, Dicalcium Phosphate 2-hydrate, Choline Bitartrate, Mono- and Diglycerides of Fatty Acids (Emulsifier), Calcium Carbonate, Beta-Carotene 1%, Magnesium Oxide, Potassium Acetate, Sodium Ascorbate (Vitamin C), De-oiled Enzyme-Modified Soy Lecithin (Emulsifier), DL Alpha-Tocopherol Acetate (Vitamin E-Acetate 50%), Sodium Ferrous Citrate, Calcium Chloride Dihydrate, Taurine, Carnitine, Zinc Sulfate Heptahydrate, Biotin 1%, Niacin, Vitamin B12 0.1%, Dry Vitamin A (175,000 IU/g), Vitamin E (Mixed Tocopherols Concentrate) (Antioxidant), Calcium Pantothenate (Vitamin B5), Manganese Sulfate Monohydrate, Copper Sulfate Pentahydrate, Thiamine HCl (Vitamin B1), Pyridoxine HCl (Vitamin B6), Selenium Glycinate Complex 1.0%, Molybdenum Glycinate Chelate 2.5%, Chromium Nicotinate Glycinate Chelate 2.5%, Riboflavin (Vitamin B2), Dry Vitamin D3 (200,000 IU/g), Folic Acid (Vitamin M), Potassium Iodide, and Vitamin K1 powder 50% | Water, Maltodextrin, Milk protein, Medium chain Triglycerides, Vegetable Oils (Soya Oil and Linseed Oil), Potassium Citrate, Fish Oil, Potassium Chloride, Sodium Chloride, Calcium Chloride, Sodium Citrate, Vitamin C, Choline Chloride, Magnesium Oxide, Calcium Phosphate, Acidity Regulator (E330), Magnesium Citrate, Emulsifier (E471), Zinc Sulphate, iron Pyrophosphate, Iron Sulphate, Niacin, Vitamin E, Manganese Chloride, Pantothenic Acid, Sodium Fluoride, Vitamin B2, Copper Sulphate, Vitamin B6, Vitamin B1, Vitamin A, Beta-Carotene, Folic Acid, Sodium Molybdate, Potassium Iodide, Chromium Chloride, Sodium Selenite, Vitamin K1, Biotin, Vitamin D3, and Vitamin B12 |
| Study | kcal | Volume |
|---|---|---|
| Kudsk et al. [31] | Immun-Aid = 1040 kcal Promote and Casec = 1000 kcal | Not specified |
| Weimann et al. [12] | IMPACT Sandoz Nutrition = 101 kcal × 100 mL Sandoz Nutrition = 101 kcal × 100 mL | 35 ± 40 kcal/kg body weight/day |
| Bastian et al. [36] | IMPACT Sandoz Nutrition = 101 kcal × 100 mL Not specified control = 101 kcal × 100 mL | 35 ± 40 kcal/kg body weight/day |
| Briassoulis et al. [37] | Stresson = 100 kcal × 100 mL Tentrini = 125 kcal × 100 mL | According to the predicted basal metabolic rate |
| Lorenz et al. [10] | Not specified | |
| Rai et al. [38] | Neomune = 1503 kcal Fresubin® HP energy = 1502 kcal | About 1000 mL in both groups |
| Study | Scoring System |
|---|---|
| Kudsk et al. [31] | ISS ≥ 21 ATI ≥ 25 GCS ≥ 7 |
| Weimann et al. [12] | ISS-test: 39.6 ± 11.4 ISS-control: 40.5 ± 9.2 APACHE II-test: 6.5 ± 3.1 APACHE II-control: 9.8 ± 6.3 |
| Bastian et al. [36] | ISS-test: 39.6 ± 11.4 ISS-control: 40.5 ± 9.2 APACHE II-test: 6.5 ± 3.1 APACHE II-control: 9.8 ± 6.3 PTS-test: 38.8 ± 12.5 PTS-control: 40.8 ± 15.5 |
| Briassoulis et al. [37] | PRISM: 13.2 ± 1 PRISM-control: 12.4 ± 1 TISS: 32.5 ± 4 TISS-control: 28.4 ± 3.7 GCS: 6.1 ± 0.4 GCS-control: 6.3 ± 0.6 |
| Lorenz et al. [10] | ISS, GCS, APACHE 11, MOF, SOFA, and SAPS values not cited |
| Rai et al. [38] | GCS from moderate to severe (3–12) |
| Study | Year | Formula | Control Formula | Type of Study | Surgery | Number of Patients | Age | Sex |
|---|---|---|---|---|---|---|---|---|
| Alito et al. [29] | 2016 | ACERTO protocol | Impact-Nestlé, Brazil | Prospective Pilot | Elective total hip arthroplasty | 32 | 58 years; range, 26–85 years | 50% women |
| Gonçalves et al. [30] | 2021 | ONS with impact immunonutrients (Nestlé Health Science, Epalinges, Switzerland) | Not specified | Retrospective cohort | Elective total hip and knee arthroplasties in elderly patients | 3015 | 72.6 ± 6.9 years | 81.2% women |
| Study | Follow-Up | Route | Feeding Protocol | Results |
|---|---|---|---|---|
| Alito et al. [29] | Hospital stay | Oral intake | 600 mL per day | Reduction in length of hospital stay and postoperative acute inflammatory response. |
| Gonçalves et al. [30] | 3 months | Oral intake | 600 mL per day | Shorter length of hospital stay and a lower rate of infectious complications compared to the control group. A 55% reduction in the chance of infectious complications and mean hospitalization was 42% lower in the immunonutrition group. Additionally, the immunonutrition group reduced the chance of secondary outcomes, such as non-infectious complications and the need for blood transfusion, by 50–76% in an adjusted logistic regression model, respectively. |
| Study | Formula | Control |
|---|---|---|
| Alito et al. [29] | Proteins 23% (77% Calcium Caseinate and 23% arginine); Carbohydrates 52% (100% Maltodextrin); Lipids 25% (68% Fish Oil, 20% Medium-chain Triglycerides, and 12% Corn Oil); Vitamins and Electrolytes | Water, Maltodextrin, Milk Proteins, Vegetable Oils (Palm and Sunflower), Minerals (Potassium Citrate, Calcium Chloride, Magnesium Citrate, Trisodium Citrate, Potassium Phosphate, Sodium Chloride, Potassium Chloride, Zinc Sulphate, Ferrous Sulphate, Copper Gluconate, Manganese Sulphate, Sodium Fluoride, Sodium Molybdate, Chromium Chloride, Sodium Selenite, and Potassium Iodide), l-Arginine, Fish Oil, Yeast Extract Rich In Nucleotides (RNA), Emulsifier (Soy Lecithin), Choline Bitartrate, Vitamins (C, E, Pantothenic Acid, Niacin, B1, B6, B2, A, D, B12, K, Folic Acid, and Biotin), Acidity Regulator (E330), Antioxidants (E301 and E307), and Color (Beta-Carotene) |
| Gonçalves et al. [30] | Water, Sugar, Calcium Caseinate (Milk), Sodium Caseinate, l-arginine, Refined Fish Oil (Anchovy and Sardine) and less than 2% of Corn Oil, Citric Acid, Medium-chain Triglycerides, Maltodextrin, Natural and Artificial Flavor, Yeast Extract, Potassium Citrate, Potassium Chloride, Calcium Phosphate, Magnesium Phosphate, Salt, Magnesium Chloride, Cellulose Gel, Cellulose Gum, Choline Chloride, Sodium Ascorbate, Sucralose (Sweetener), Carrageenan, Zinc Sulfate, Ferrous Sulfate, D Alpha-Tocopherol, Niacinamide, Soybean Oil, DL Alpha-Tocopheryl Acetate, Calcium Pantothenate, Copper Gluconate, Manganese Sulfate, Vitamin A Palmitate, Pyridoxine Hydrochloride, Riboflavin, Thiamine Hydrochloride, Beta-Carotene, Folic Acid, Potassium Iodide, Sodium Selenite, Sodium Molybdate, Chromium Chloride, Vitamin K1, Biotin, Vitamin D3, and Vitamin B12 | Not specified |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gregori, P.; Franceschetti, E.; Basciani, S.; Impieri, L.; Zampogna, B.; Matano, A.; Manzi, C.; Carbone, L.; Marano, L.; Papalia, R. Immunonutrition in Orthopedic and Traumatic Patients. Nutrients 2023, 15, 537. https://doi.org/10.3390/nu15030537
Gregori P, Franceschetti E, Basciani S, Impieri L, Zampogna B, Matano A, Manzi C, Carbone L, Marano L, Papalia R. Immunonutrition in Orthopedic and Traumatic Patients. Nutrients. 2023; 15(3):537. https://doi.org/10.3390/nu15030537
Chicago/Turabian StyleGregori, Pietro, Edoardo Franceschetti, Susanna Basciani, Lorenzo Impieri, Biagio Zampogna, Alfredo Matano, Carlo Manzi, Ludovico Carbone, Luigi Marano, and Rocco Papalia. 2023. "Immunonutrition in Orthopedic and Traumatic Patients" Nutrients 15, no. 3: 537. https://doi.org/10.3390/nu15030537
APA StyleGregori, P., Franceschetti, E., Basciani, S., Impieri, L., Zampogna, B., Matano, A., Manzi, C., Carbone, L., Marano, L., & Papalia, R. (2023). Immunonutrition in Orthopedic and Traumatic Patients. Nutrients, 15(3), 537. https://doi.org/10.3390/nu15030537