
Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
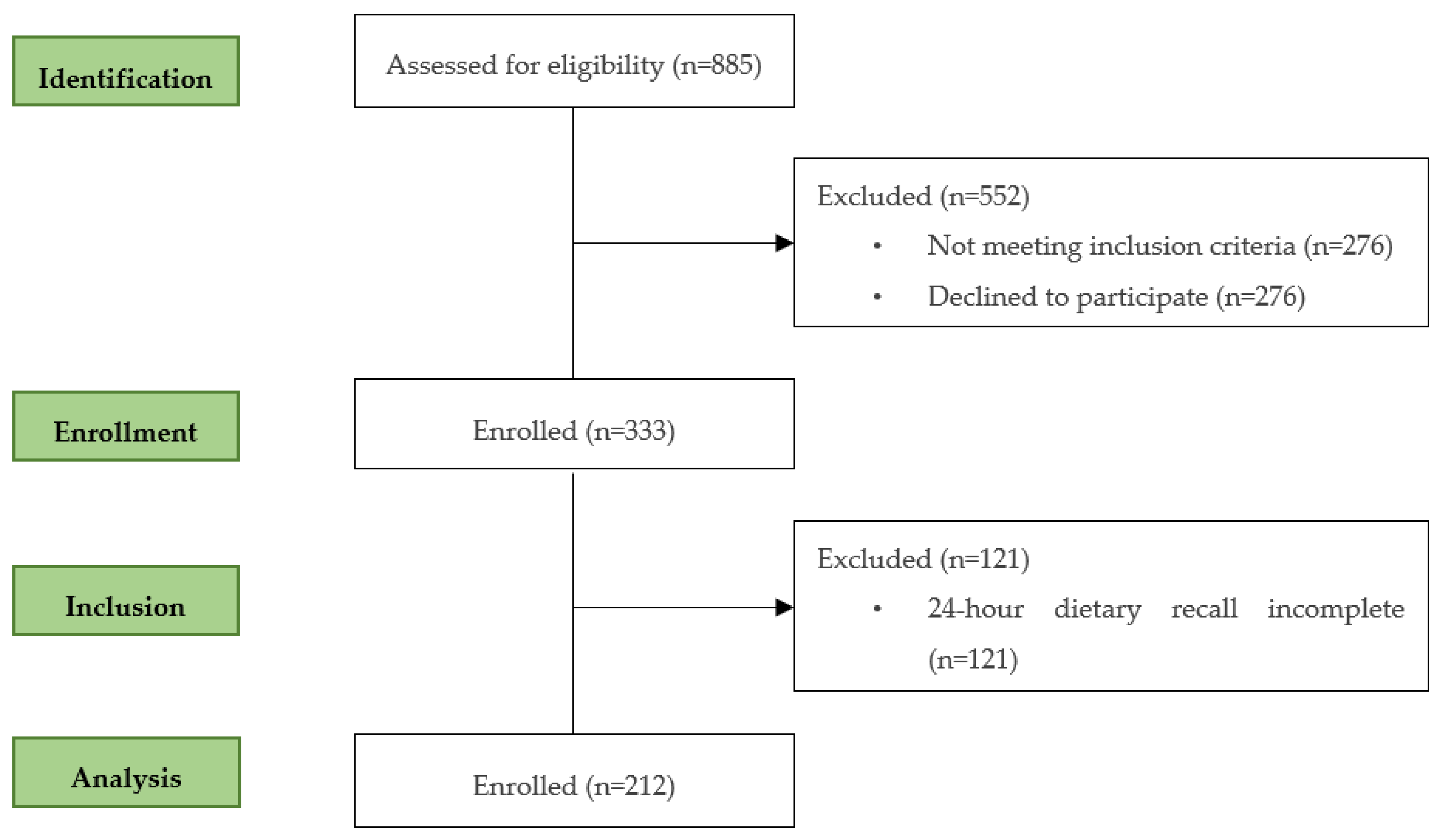
2.1. Study Participants and Design
2.2. Bayley Scales of Infant and Toddler Development
2.3. Dietary Intake
2.4. Food Processing
2.5. Dietary Diversity
2.6. Sociodemographic Data
2.7. Sleep Patterns
2.8. Anthropometry
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Black, M.M.; Walker, S.P.; Fernald, L.C.H.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Naveed, S.; Lakka, T.; Haapala, E.A. An Overview on the Associations between Health Behaviors and Brain Health in Children and Adolescents with Special Reference to Diet Quality. Int. J. Environ. Res. Public. Health 2020, 17, 953. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.W.; Gorski, M.T.; Gruber, S.A.; Kurdziel, L.B.F.; Rimm, E.B. The effect of healthy dietary consumption on executive cognitive functioning in children and adolescents: A systematic review. Br. J. Nutr. 2016, 116, 989–1000. [Google Scholar] [CrossRef]
- Georgieff, M.K.; Ramel, S.E.; Cusick, S.E. Nutritional influences on brain development. Acta Paediatr. 2018, 107, 1310–1321. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Kirolos, A.; Goyheneix, M.; Kalmus Eliasz, M.; Chisala, M.; Lissauer, S.; Gladstone, M.; Kerac, M. Neurodevelopmental, cognitive, behavioural and mental health impairments following childhood malnutrition: A systematic review. BMJ Glob. Health 2022, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Sanefuji, M.; Sonoda, Y.; Ito, Y.; Ogawa, M.; Tocan, V.; Inoue, H.; Ochiai, M.; Shimono, M.; Suga, R.; Senju, A.; et al. Physical growth and neurodevelopment during the first year of life: A cohort study of the Japan Environment and Children’s Study. BMC Pediatr. 2021, 21, 360. [Google Scholar] [CrossRef]
- Anjos, T.; Altmäe, S.; Emmett, P.; Tiemeier, H.; Closa-Monasterolo, R.; Luque, V.; Wiseman, S.; Pérez-García, M.; Lattka, E.; Demmelmair, H.; et al. Nutrition and neurodevelopment in children: Focus on NUTRIMENTHE project. Eur. J. Nutr. 2013, 52, 1825–1842. [Google Scholar] [CrossRef]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the Development of Children’s Eating Behaviours: From Infancy to Adolescence. Can. J. Diet. Pr. Res. 2007, 68, s1–s56. [Google Scholar]
- Rito, A.; Mendes, S.; Baleia, J.; Gregório, M.J. Childhood Obesity Surveillance Initiative: COSI Portugal 2019. Lisb. Inst. Nac. De Saúde Doutor Ricardo Jorge IP 2021. Available online: http://hdl.handle.net/10400.18/7783 (accessed on 1 November 2023).
- World Health Organization. Regional Office for, E. WHO European Childhood Obesity Surveillance Initiative (COSI) Report. on the Fourth Round of Data Collection, 2015–2017; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2021. [Google Scholar]
- Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Alarcão, V.; Guiomar, S.; Mota, J.; Teixeira, P.; Ramos, E.; Rodrigues, S.; et al. Consórcio IAN-AF. Inquérito Alimentar Nacional e de Atividade Física, IAN-AF 2015-2016: Relatório Metodológico; Universidade do Porto: Porto, Portugal, 2017; ISBN 978-989-746-180-4. Available online: www.ian-af.up.pt (accessed on 3 July 2023).
- de Moraes, M.M.; Oliveira, B.; Afonso, C.; Santos, C.; Torres, D.; Lopes, C.; Miranda, R.C.; Rauber, F.; Antoniazzi, L.; Levy, R.B.; et al. Dietary Patterns in Portuguese Children and Adolescent Population: The UPPER Project. Nutrients 2021, 13, 3851. [Google Scholar] [CrossRef] [PubMed]
- Albers, C.A.; Grieve, A.J. Test Review: Bayley, N. (2006). Bayley Scales of Infant and Toddler Development–Third Edition. San Antonio, TX: Harcourt Assessment. J. Psychoeduc. Assess. 2007, 25, 180–190. [Google Scholar] [CrossRef]
- Goios, A.; Oliveira, C.A.; Afonso, A.; Amaral, T.; Liz Martins, M. Pesos e Porções de Alimentos, 3rd ed.; Universidade do Porto: Porto, Portugal, 2019. [Google Scholar]
- Monteiro, C.; Cannon, G.; Lawrence, M.; Louzada, M.L.; Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the NOVA Classification System; FAO: Rome, Italy, 2019. [Google Scholar]
- World Health, O. Indicators for Assessing Infant and Young Child Feeding Practices: Part 2: Measurement; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- WHO. Global Nutrition Monitoring Framework: Operational Guidance for Tracking Progress in Meeting Targets for 2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Graffar, M. Une méthode de classification sociale d’échantillons de population. Courrier 1956, 6, 455–459. [Google Scholar]
- McGreavey, J.A.; Donnan, P.T.; Pagliari, H.C.; Sullivan, F.M. The Tayside children’s sleep questionnaire: A simple tool to evaluate sleep problems in young children. Child. Care Health Dev. 2005, 31, 539–544. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- WHO. Training Course on Child Growth Assessment, WHO Child Growth Standards, B Measuring a Child’s Growth; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Riggs, N.R.; Spruijt-Metz, D.; Chou, C.P.; Pentz, M.A. Relationships between executive cognitive function and lifetime substance use and obesity-related behaviors in fourth grade youth. Child. Neuropsychol. 2012, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Haapala, E.A.; Eloranta, A.M.; Venäläinen, T.; Schwab, U.; Lindi, V.; Lakka, T.A. Associations of diet quality with cognition in children–The Physical Activity and Nutrition in Children Study. Br. J. Nutr. 2015, 114, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Blomkvist, E.A.M.; Hillesund, E.R.; Helland, S.H.; Simhan, I.; Øverby, N.C. Diet and Neurodevelopmental Score in a Sample of One-Year-Old Children-A Cross-Sectional Study. Nutrients 2019, 11, 1676. [Google Scholar] [CrossRef]
- Gale, C.R.; Martyn, C.N.; Marriott, L.D.; Limond, J.; Crozier, S.; Inskip, H.M.; Godfrey, K.M.; Law, C.M.; Cooper, C.; Robinson, S.M. Dietary patterns in infancy and cognitive and neuropsychological function in childhood. J. Child. Psychol. Psychiatry 2009, 50, 816–823. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public. Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef]
- Katidi, A.; Vlassopoulos, A.; Noutsos, S.; Kapsokefalou, M. Ultra-Processed Foods in the Mediterranean Diet according to the NOVA Classification System; A Food Level Analysis of Branded Foods in Greece. Foods 2023, 12, 1520. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cornejo, I.; Izquierdo-Gomez, R.; Gómez-Martínez, S.; Padilla-Moledo, C.; Castro-Piñero, J.; Marcos, A.; Veiga, O.L. Adherence to the Mediterranean diet and academic performance in youth: The UP&DOWN study. Eur. J. Nutr. 2016, 55, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Granziera, F.; Guzzardi, M.A.; Iozzo, P. Associations between the Mediterranean Diet Pattern and Weight Status and Cognitive Development in Preschool Children. Nutrients 2021, 13, 3723. [Google Scholar] [CrossRef] [PubMed]
- WHO; United Nations International Children’s Emergency Fund. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Andreas, N.J.; Kampmann, B.; Mehring Le-Doare, K. Human breast milk: A review on its composition and bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Ling, P.R.; Blackburn, G.L. Review of Infant Feeding: Key Features of Breast Milk and Infant Formula. Nutrients 2016, 8, 279. [Google Scholar] [CrossRef] [PubMed]
- Petryk, A.; Harris, S.R.; Jongbloed, L. Breastfeeding and Neurodevelopment: A Literature Review. Infants Young Child. 2007, 20, 120–134. [Google Scholar] [CrossRef]
- Khandpur, N.; Neri, D.A.; Monteiro, C.; Mazur, A.; Frelut, M.L.; Boyland, E.; Weghuber, D.; Thivel, D. Ultra-Processed Food Consumption among the Paediatric Population: An Overview and Call to Action from the European Childhood Obesity Group. Ann. Nutr. Metab. 2020, 76, 109–113. [Google Scholar] [CrossRef]
- Zhao, C.; Guan, H.; Shi, H.; Zhang, J.; Huang, X.; Wang, X. Relationships between dietary diversity and early childhood developmental outcomes in rural China. Matern. Child. Nutr. 2021, 17, e13073. [Google Scholar] [CrossRef]
- Thorne-Lyman, A.L.; Shrestha, M.; Fawzi, W.W.; Pasqualino, M.; Strand, T.A.; Kvestad, I.; Hysing, M.; Joshi, N.; Lohani, M.; Miller, L.C. Dietary Diversity and Child Development in the Far West of Nepal: A Cohort Study. Nutrients 2019, 11, 1799. [Google Scholar] [CrossRef]
- Gould, J.F. Complementary Feeding, Micronutrients and Developmental Outcomes of Children. Nestle Nutr. Inst. Workshop Ser. 2017, 87, 13–28. [Google Scholar] [CrossRef]
- Koletzko, B.; Brands, B.; Grote, V.; Kirchberg, F.F.; Prell, C.; Rzehak, P.; Uhl, O.; Weber, M. Long-Term Health Impact of Early Nutrition: The Power of Programming. Ann. Nutr. Metab. 2017, 70, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Nyaradi, A.; Li, J.; Hickling, S.; Foster, J.; Oddy, W.H. The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front. Hum. Neurosci. 2013, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Frisardi, V.; Panza, F.; Seripa, D.; Imbimbo, B.P.; Vendemiale, G.; Pilotto, A.; Solfrizzi, V. Nutraceutical properties of Mediterranean diet and cognitive decline: Possible underlying mechanisms. J. Alzheimers Dis. 2010, 22, 715–740. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; Ying, Z.; Gomez-Pinilla, F. The interplay between oxidative stress and brain-derived neurotrophic factor modulates the outcome of a saturated fat diet on synaptic plasticity and cognition. Eur. J. Neurosci. 2004, 19, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Larson, L.M.; Young, M.F.; Ramakrishnan, U.; Webb Girard, A.; Verma, P.; Chaudhuri, I.; Srikantiah, S.; Martorell, R. A Cross-Sectional Survey in Rural Bihar, India, Indicates That Nutritional Status, Diet, and Stimulation Are Associated with Motor and Mental Development in Young Children. J. Nutr. 2017, 147, 1578–1585. [Google Scholar] [CrossRef] [PubMed]
- Leroy, J.L.; Olney, D.; Ruel, M. Tubaramure, a Food-Assisted Integrated Health and Nutrition Program in Burundi, Increases Maternal and Child Hemoglobin Concentrations and Reduces Anemia: A Theory-Based Cluster-Randomized Controlled Intervention Trial. J. Nutr. 2016, 146, 1601–1608. [Google Scholar] [CrossRef]
- Aboud, F.E.; Yousafzai, A.K. Very Early Childhood Development. In Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2); Black, R.E., Laxminarayan, R., Temmerman, M., Walker, N., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2016. [Google Scholar] [CrossRef]
- Lassek, W.D.; Gaulin, S.J. Sex differences in the relationship of dietary Fatty acids to cognitive measures in american children. Front. Evol. Neurosci. 2011, 3, 5. [Google Scholar] [CrossRef]
- Stea, T.H.; Torstveit, M.K. Association of lifestyle habits and academic achievement in Norwegian adolescents: A cross-sectional study. BMC Public Health 2014, 14, 829. [Google Scholar] [CrossRef]
- Markham, J.A.; Mullins, S.E.; Koenig, J.I. Periadolescent maturation of the prefrontal cortex is sex-specific and is disrupted by prenatal stress. J. Comp. Neurol. 2013, 521, 1828–1843. [Google Scholar] [CrossRef]
- Patton, G.C.; Viner, R. Pubertal transitions in health. Lancet 2007, 369, 1130–1139. [Google Scholar] [CrossRef]
- Koolschijn, P.C.M.P.; Crone, E.A. Sex differences and structural brain maturation from childhood to early adulthood. Dev. Cogn. Neurosci. 2013, 5, 106–118. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Girls (n = 110) | Boys (n = 102) | Total (n = 212) | p-Value | |
|---|---|---|---|---|
| Age (months), mean ± SD | 23.61 ± 6.13 | 23.94 ± 6.56 | 23.77 ± 6.33 | 0.704 1 |
| TEI (kcal/day), median (25th–75th) | 1030.01 (912.52–1192.41) | 1100.34 (975.97–1281.30) | 1077.33 (930.94–1236.42) | 0.111 1 |
| Breastfeeding a, n (%) | 19 (17.3) | 12 (11.8) | 31 (14.6) | 0.257 2 |
| Infant formula b, n (%) | 25 (22.7) | 23 (22.5) | 48 (22.6) | 0.975 2 |
| Sleeping time (hours), mean ± SD | 10.31 ± 0.82 | 10.28 ± 0.63 | 10.30 ± 0.72 | 0.793 1 |
| Mother education, n (%) | 0.607 2 | |||
| Basic/High School | 43 (39.4) | 36 (36.0) | 79 (37.8) | |
| University | 66 (66.6) | 64 (64.0) | 130 (62.2) | |
| Bayley cognitive score, mean ± SD | 10.04 ± 2.72 | 9.56 ± 2.60 | 9.81 ± 2.67 | 0.193 1 |
| Bayley’s cognitive categories, n (%) | 0.448 2 | |||
| Below median cognitive scaled score (score < 10) | 45 (40.9) | 47 (46.1) | 92 (43.4) | |
| Above median cognitive scaled score (score ≥ 10) | 65 (59.1) | 55 (53.9) | 120 (56.6) |
| Girls (n = 110) | Boys (n = 102) | Total (n = 212) | p-Value | |
|---|---|---|---|---|
| NOVA classification (% kcal TEI) Including infant formulas | ||||
| NOVA 1, mean ± SD | 58.15 ± 13.02 | 55.95 ± 12.60 | 57.09 ± 12.83 | 0.219 1 |
| NOVA 2, mean ± SD | 8.20 ± 3.56 | 7.54 ± 3.16 | 7.89 ± 3.38 | 0.163 1 |
| NOVA 3, mean ± SD | 13.15 ± 7.69 | 11.23 ± 7.69 | 12.22 ± 7.73 | 0.076 1 |
| NOVA 4, mean ± SD | 20.44 ± 13.93 | 25.29 ± 14.73 | 22.78 ± 14.49 | 0.016 1 |
| NOVA classification (% kcal TEI) Excluding infant formulas | ||||
| NOVA 1, mean ± SD | 61.11 ± 11.91 | 59.43 ± 11.77 | 60.31 ± 11.85 | 0.304 1 |
| NOVA 2, median (25th–75th) | 8.62 (5.90–10.89) | 8.00 (6.00–10.20) | 8.26 (5.94–10.45) | 0.321 3 |
| NOVA 3, mean ± SD | 13.63 ± 7.96 | 11.37 ± 7.92 | 12.54 ± 8.00 | 0.039 1 |
| NOVA 4, mean ± SD | 16.55 ± 12.05 | 21.15 ± 12.44 | 18.77 ± 12.42 | 0.007 1 |
| Dietary diversity score, mean ± SD | 4.99 ± 0.79 | 5.07 ± 0.76 | 4.91 ± 0.81 | 0.257 2 |
| Dietary diversity categories, n (%) | ||||
| Below median score (<5) | 79 (37.3) | 37 (33.6) | 42 (41.2) | |
| Above median score (≥5) | 133 (62.7) | 73 (66.4) | 60 (58.8) |
| NOVA Classification: aOR (95%CI) | NOVA 1 Above Median Cognitive Scaled Score Crude Model | p-Value | NOVA 1 Above Median Cognitive Scaled Score Adjusted Model | p-Value |
|---|---|---|---|---|
| Model 1 | ||||
| All participants | 1.04 (1.01; 1.06) | 0.004 | 1.05 (1.01; 1.09) | 0.036 |
| Girls | 1.04 (1.01; 1.08) | 0.015 | 1.06 (1.01; 1.11) | 0.018 |
| Boys | 1.03 (0.99; 1.06) | 0.134 | 1.03 (0.99; 1.07) | 0.208 |
| Model 2 | ||||
| All participants | 1.02 (1.00; 1.05) | 0.034 | 1.03 (1.00; 1.06) | 0.037 |
| Girls | 1.04 (1.01; 1.08) | 0.008 | 1.06 (1.01; 1.11) | 0.024 |
| Boys | 1.00 (0.97; 1.03) | 0.956 | 1.02 (0.98; 1.07) | 0.299 |
| Model 3 | ||||
| All participants | 1.04 (1.01; 1.06) | 0.004 | 1.03 (1.00; 1.06) | 0.032 |
| Girls | 1.04 (1.01; 1.08) | 0.015 | 1.05 (1.00; 1.11) | 0.033 |
| Boys | 1.03 (0.99; 1.06) | 0.134 | 1.02 (0.98; 1.07) | 0.239 |
| Model 4 | ||||
| All participants | 1.02 (1.00; 1.05) | 0.034 | 1.03 (1.00; 1.06) | 0.041 |
| Girls | 1.04 (1.01; 1.08) | 0.008 | 1.05 (1.00; 1.11) | 0.043 |
| Boys | 1.00 (0.97; 1.03) | 0.956 | 1.02 (0.98; 1.06) | 0.338 |
| Minimum Dietary Diversity: aOR (95%CI) | Food Diversity Above Median Cognitive Scaled Score Crude Model | p-Value | Food Diversity Above Median Cognitive Scaled Score Adjusted Model | p-Value |
|---|---|---|---|---|
| Model 1 | ||||
| All participants | 1.47 (0.84; 2.58) | 0.177 | 1.28 (0.65; 2.49) | 0.476 |
| Girls | 2.26 (1.01; 5.06) | 0.048 | 3.15 (1.05; 9.48) | 0.041 |
| Boys | 0.94 (0.43; 2.08) | 0.887 | 0.61 (0.23; 1.63) | 0.329 |
| Model 2 | ||||
| All participants | 1.47 (0.84; 2.58) | 0.177 | 1.24 (0.63; 2.43) | 0.533 |
| Girls | 2.26 (1.01; 5.06) | 0.048 | 3.18 (1.12; 9.08) | 0.030 |
| Boys | 0.94 (0.43; 2.08) | 0.887 | 0.65 (0.25; 1.70) | 0.382 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cunha-Rodrigues, M.; Rosário, R.; Duarte, A.; Silva, M.J.; Augusto, C.; Rodrigues, M.; Padrão, P.; Moreira, P. Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project. Nutrients 2023, 15, 5105. https://doi.org/10.3390/nu15245105
Cunha-Rodrigues M, Rosário R, Duarte A, Silva MJ, Augusto C, Rodrigues M, Padrão P, Moreira P. Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project. Nutrients. 2023; 15(24):5105. https://doi.org/10.3390/nu15245105
Chicago/Turabian StyleCunha-Rodrigues, Micaela, Rafaela Rosário, Ana Duarte, Maria José Silva, Cláudia Augusto, Mónica Rodrigues, Patrícia Padrão, and Pedro Moreira. 2023. "Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project" Nutrients 15, no. 24: 5105. https://doi.org/10.3390/nu15245105
APA StyleCunha-Rodrigues, M., Rosário, R., Duarte, A., Silva, M. J., Augusto, C., Rodrigues, M., Padrão, P., & Moreira, P. (2023). Neurodevelopment and Dietary Intake in Toddlers—A Cross-Sectional Study from the Healthy Children 2021 Project. Nutrients, 15(24), 5105. https://doi.org/10.3390/nu15245105