
Oxidative Stress Induced by Chemotherapy: Evaluation of Glutathione and Its Related Antioxidant Enzyme Dynamics in Patients with Colorectal Cancer


Abstract
:1. Introduction
2. Subjects and Methods
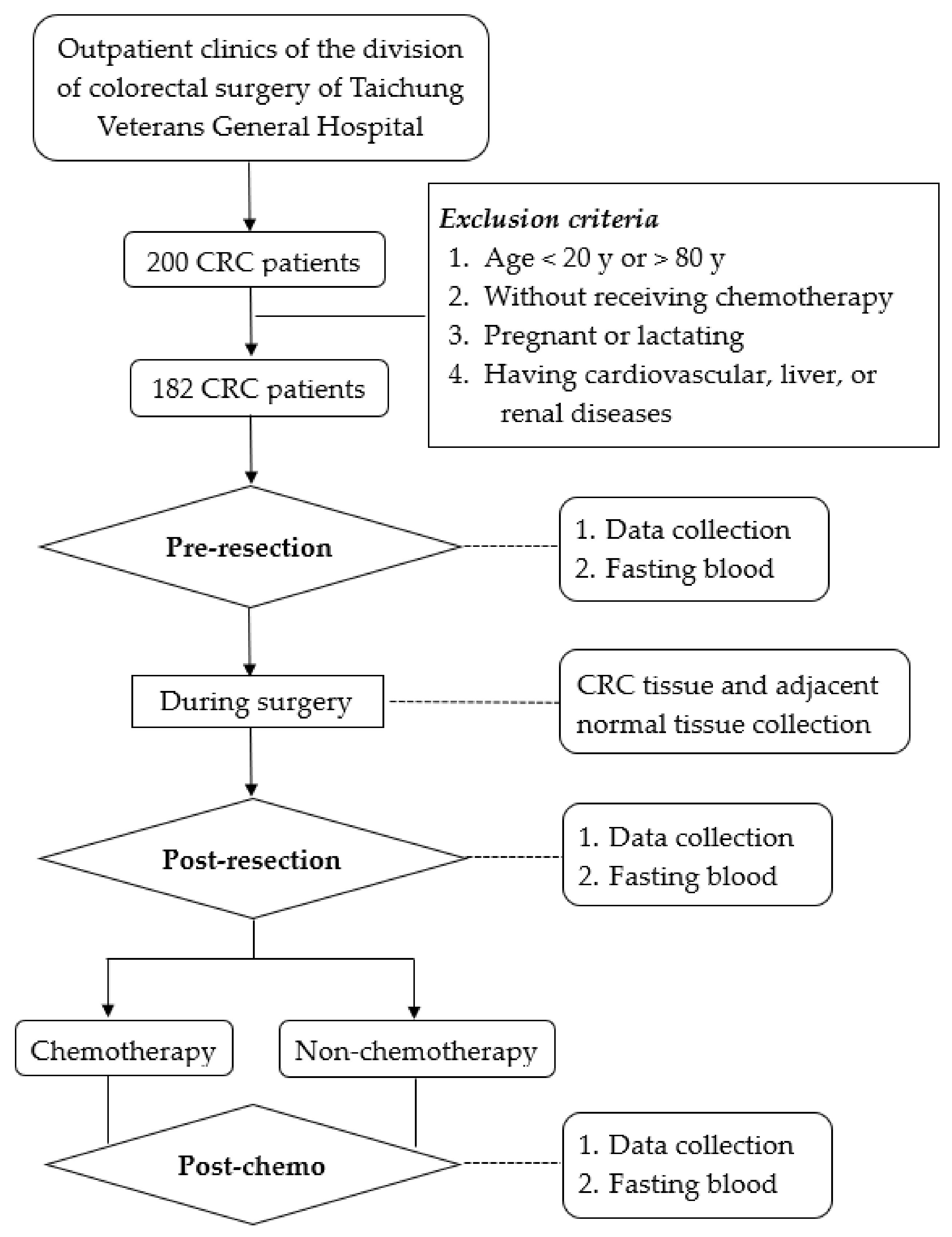
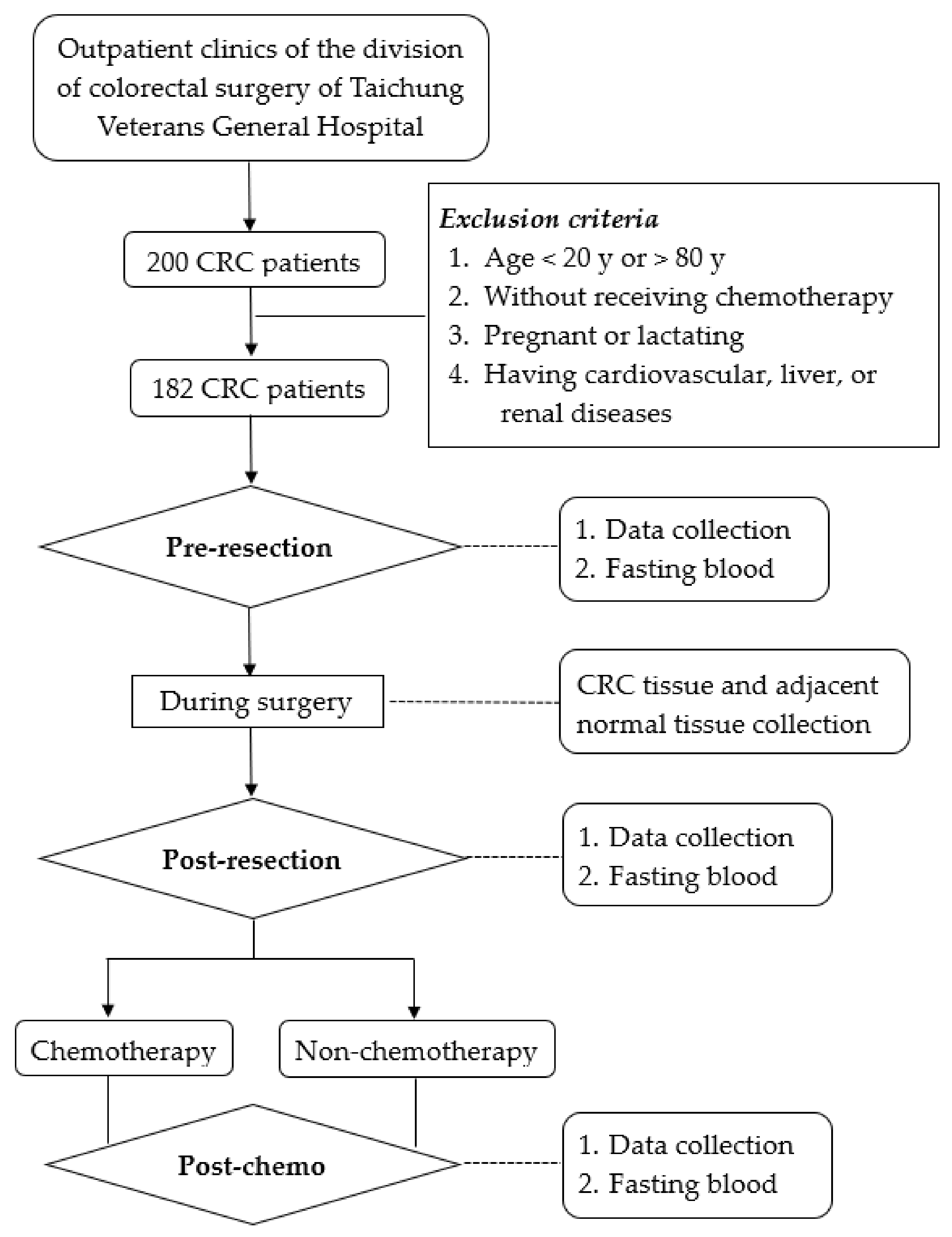
2.1. Study Design and Sample Size Calculation
2.2. Subjects
2.3. Data Collection and Biochemical Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 5-FU | 5-fluorouracil |
| ALT | alanine aminotransferase |
| AOPP | advanced oxidation protein products |
| AST | aspartate aminotransferase |
| CA19-9 | carbohydrate antigen 19-9 |
| CEA | carcinoembryonic antigen |
| CR | complete response |
| CRC | colorectal cancer |
| CRP | C-reactive protein |
| GSH | glutathione |
| GPx | glutathione peroxidase |
| GR | glutathione reductase |
| GSSG | glutathione disulfide |
| GST | glutathione S-transferase |
| MDA | malondialdehyde |
| PD | progressive disease |
| PR | partial response |
| SD | stable disease |
| TEAC | trolox equivalent antioxidant capacity |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Haller, D.G.; O’Connell, M.J.; Cartwright, T.H.; Twelves, C.J.; McKenna, E.F.; Sun, W.; Saif, M.W.; Lee, S.; Yothers, G.; Schmoll, H. Impact of age and medical comorbidity on adjuvant treatment outcomes for stage III colon cancer: A pooled analysis of individual patient data from four randomized, controlled trials. Ann. Oncol. 2015, 26, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Dossa, F.; Acuna, S.A.; Rickles, A.S.; Berho, M.; Wexner, S.D.; Quereshy, F.A.; Baxter, N.N.; Chadi, S.A. Association between adjuvant chemotherapy and overall survival in patients with rectal cancer and pathological complete response after neoadjuvant chemotherapy and resection. JAMA Oncol. 2018, 4, 930–937. [Google Scholar] [CrossRef]
- Polanco, P.M.; Mokdad, A.A.; Zhu, H.; Choti, M.A.; Huerta, S. Association of adjuvant chemotherapy with overall survival in patients with rectal cancer and pathologic complete response following neoadjuvant chemotherapy and resection. JAMA Oncol. 2018, 4, 938–943. [Google Scholar] [CrossRef]
- Nozawa, H.; Sonoda, H.; Ishii, H.; Emoto, S.; Murono, K.; Kaneko, M.; Sasaki, K.; Nishikawa, T.; Shuno, Y.; Tanaka, T.; et al. Postoperative chemotherapy is associated with prognosis of stage IV colorectal cancer treated with preoperative hemotherapy/chemoradiotherapy and curative resection. Int. J. Color. Dis. 2020, 35, 177–180. [Google Scholar] [CrossRef]
- Zhang, D.; Wang, X.; Zhang, M.; Yin, Y.; Guo, J. Clinical efficacy of chemotherapy in colorectal cancer patients over 80 years old. Int. J. Color. Dis. 2022, 37, 1853–1863. [Google Scholar] [CrossRef]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330–338. [Google Scholar] [CrossRef]
- Mehrzad, V.; Roayaei, M.; Peikar, M.S.; Nouranian, E.; Mokarian, F.; Khani, M.; Farzannia, S. Bevacizumab plus FOLFOX or FOLFIRI regimens on patients with unresectable liver-only metastases of metastatic colorectal cancer. Adv. Biomed. Res. 2016, 5, 10. [Google Scholar]
- Khalil, K.A.; Musallam, H.S.; Hassan, M.A.; Mahmoud, I.A. Triplet (FOLFOXIRI) versus doublet (FOLFOX or FOLFIRI) regimen as first line treatment in metastatic colorectal carcinoma, a prospective phase II, randomized controlled trial. Asian Pac. J. Cancer Prev. 2022, 23, 3421–3429. [Google Scholar] [CrossRef]
- Santiago-Arteche, R.; Muñiz, P.; Cavia-Saiz, M.; Garcia-Giron, C.; García-Gonzalez, M.; Llorente-Ayala, B.; Corral, M.J. Cancer chemotherapy reduces plasma total polyphenols and total antioxidants capacity in colorectal cancer patients. Mol. Biol. Rep. 2012, 39, 9355–9360. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liu, X.; Zhang, C.; Zhu, H.; Xu, Q.; Bu, Y.; Lei, Y. Redox imbalance in the development of colorectal cancer. J. Cancer 2017, 8, 1586–1597. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Bhori, M.; Kasu, Y.A.; Bhat, G.; Marar, T. Antioxidants as precision weapons in war against cancer chemotherapy induced toxicity—Exploring the armoury of obscurity. Saudi Pharm. J. 2018, 26, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Erhola, M.; Kellokumpu-Lehtinen, P.; Metsa-Ketela, T.; Alanko, K.; Nieminen, M.M. Effects of anthracyclin-based chemotherapy on total plasma antioxidant capacity in small cell lung cancer patients. Free Radic. Biol. Med. 1996, 21, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Durken, M.; Herrnring, C.; Finckh, B.; Nagel, S.; Nielsen, P.; Fischer, R.; Berger, H.M.; Moison, R.M.; Pichlmeier, U.; Kohlschütter, B.; et al. Impaired plasma antioxidative defense and increased nontransferrin-bound iron during high-dose chemotherapy and radio-chemotherapy preceding bone marrow transplantation. Free Radic. Biol. Med. 2000, 28, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Thanoon, I.A.J.; Ahmed, F.A.; Jadoaa, K.R. Lipid peroxidation and antioxidant status in post-operative patients with cancer treated with chemotherapy. Zanco. J. Med. Sci. 2018, 14, 64–67. [Google Scholar]
- Kasapović, J.; Pejić, S.; Stojiljković, V.; Todorović, A.; Radošević-Jelić, L.; Saičić, Z.S.; Pajović, S.B. Antioxidant status and lipid peroxidation in the blood of breast cancer patients of different ages after chemotherapy with 5-fluorouracil, doxorubicin and cyclophosphamide. Clin. Biochem. 2010, 43, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Hamza, T.A.; Muhsin, S.A.; Khalil, T.T. Evaluation of malondialdehyde, homocysteine and antioxidant in influence chemotherapy in breast cancer patients. HIV Nurs. 2022, 22, 3759–3762. [Google Scholar] [CrossRef]
- Conklin, K.A. Chemotherapy associated oxidative stress: Impact on chemotherapeutic effectiveness. Integr. Cancer Ther. 2004, 3, 294–300. [Google Scholar] [CrossRef]
- Kennedy, L.; Sandhu, J.K.; Harper, M.E.; Cuperlovic-Culf, M. Role of glutathione in cancer: From mechanisms to therapies. Biomolecules 2020, 10, 1429. [Google Scholar] [CrossRef]
- Chun, K.S.; Joo, S.H. Modulation of Reactive Oxygen Species to Overcome 5-Fluorouracil Resistance. Biomol. Ther. 2022, 30, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zuo, J.; Li, B.; Chen, R.; Luo, K.; Xiang, X.; Lu, S.; Huang, C.; Liu, L.; Tang, J.; et al. Drug-induced oxidative stress in cancer treatments: Angel or devil? Redox Biol. 2023, 63, 102754. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Xiao, C.; Li, Z.; Yang, X. Engineering nanomedicine for glutathione depletion-augmented cancer therapy. Chem. Soc. Rev. 2021, 50, 6013–6041. [Google Scholar] [CrossRef] [PubMed]
- Lv, H.; Zhen, C.; Liu, J.; Yang, P.; Hu, L.; Shang, P. Unraveling the Potential Role of Glutathione in Multiple Forms of Cell Death in Cancer Therapy. Oxid. Med. Cell Longev. 2019, 2019, 3150145. [Google Scholar] [CrossRef] [PubMed]
- Tormos, C.; Javier Chaves, F.; Garcia, M.J.; Garrido, F.; Jover, R.; O’Connor, J.E.; Iradi, A.; Oltra, A.; Oliva, M.R.; Sáez, G.T. Role of glutathione in the induction of apoptosis and c-fos and c-jun mRNAs by oxidative stress in tumor cells. Cancer Lett. 2004, 10, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Gana, C.C.; Hanssen, K.M.; Yu, D.M.T.; Flemming, C.L.; Wheatley, M.S.; Conseil, G.; Cole, S.P.C.; Norris, M.D.; Haber, M.; Fletcher, J.I. MRP1 modulators synergize with buthionine sulfoximine to exploit collateral sensitivity and selectively kill MRP1-expressing cancer cells. Biochem. Pharmacol. 2019, 168, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Upadhya, S.; Upadhya, S.; Mohan, S.K.; Vanajakshamma, K.; Kunder, M.; Mathias, S. Oxidant-antioxidant status in colorectal cancer patients-before and after treatment. Indian J. Clin. Biochem. 2004, 19, 80–83. [Google Scholar] [CrossRef]
- Chiang, F.F.; Chao, T.H.; Huang, S.C.; Cheng, C.H.; Tseng, Y.Y.; Huang, Y.C. Cysteine regulates oxidative stress and glutathione-related antioxidative capacity before and after colorectal tumor resection. Int. J. Mol. Sci. 2022, 23, 9581. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer. 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Lakemeyer, L.; Sander, S.; Wittau, M.; Henne-Bruns, D.; Kornmann, M.; Lemke, J. Diagnostic and prognostic value of CEA and CA19-9 in colorectal cancer. Diseases 2021, 17, 21. [Google Scholar] [CrossRef]
- Zińczuk, J.; Maciejczyk, M.; Zaręba, K.; Romaniuk, W.; Markowski, A.; Kędra, B.; Zalewska, A.; Pryczynicz, A.; Matowicka-Karna, J.; Guzińnska-Ustymowicz, K. Antioxidant barrier, redox status, and oxidative damage to biomolecules in patients with colorectal cancer. Can malondialdehyde and catalase be markers of colorectal cancer advancement? Biomolecules 2019, 9, 637. [Google Scholar] [CrossRef] [PubMed]
- Marnett, L.J. Lipid peroxidation-DNA damage by malondialdehyde. Mutat. Res. 1999, 424, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Koçer, M.; Nazıroğlu, M. Effects of 5-fluorouracil on oxidative stress and calcium levels in the blood of patients with newly diagnosed colorectal cancer. Biol. Trace Elem. Res. 2013, 155, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rajappa, M.; Satyam, A.; Sharma, M. Oxidant/anti-oxidant dynamics in patients with advanced cervical cancer: Correlation with treatment response. Mol. Cell Biochem. 2010, 41, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Guan, S.; Luo, J.; Yuan, J.; Yan, J.; Yang, C.; Tong, Q. Levels of oxidative stress in patients with neoadjuvant chemotherapy for gastric cancer: Correlation with treatment response. Front. Oncol. 2023, 13, 1192192. [Google Scholar] [CrossRef] [PubMed]
- Skrzydlewska, E.; Sulkowski, S.; Koda, M.; Zalewski, B.; Kanczuga-Koda, L.; Sulkowska, M. Lipid peroxidation and antioxidant status in colorectal cancer. World J. Gastroenterol. 2005, 11, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Rainis, T.; Maor, I.; Lanir, A.; Shnizer, S.; Lavy, A. Enhanced oxidative stress and leucocyte activation in neoplastic tissues of the colon. Dig. Dis. Sci. 2007, 52, 526–530. [Google Scholar] [CrossRef]
- Kekec, Y.; Paydas, S.; Tuli, A.; Zorludemir, S.; Sakman, G.; Seydaoglu, G. Antioxidant enzyme levels in cases with gastrointestinal cancer. Eur. J. Intern. Med. 2009, 20, 403–406. [Google Scholar] [CrossRef]
- Kim, A.D.; Zhang, R.; Han, X.; Kang, K.A.; Piao, M.J.; Maeng, Y.H.; Chang, W.Y.; Hyun, J.W. Involvement of glutathione and glutathione metabolizing enzymes in human colorectal cancer cell lines and tissues. Mol. Med. Rep. 2015, 12, 4314–4319. [Google Scholar] [CrossRef]
- Veljković, A.; Stanojević, G.; Branković, B.; Pavlović, D.; Stojanović, I.; Cvetković, T. Parameters of oxidative stress in colon cancer tissue. Acta. Med. Median. 2016, 55, 32–37. [Google Scholar] [CrossRef]
- Zaidieh, T.; Smith, J.R.; Ball, K.E.; An, Q. ROS as a novel indicator to predict anticancer drug efficacy. BMC Cancer 2019, 19, 1224. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Chemotherapy (n = 48) | Non-Chemotherapy (n = 43) | ||||
|---|---|---|---|---|---|---|
| Pre-Resection | Post-Resection | Post-Chemo | Pre-Resection | Post-Resection | Post-Chemo | |
| Age (y) | 59.33 ± 1.62 | 59.12 ± 1.71 | ||||
| Male/Female | 26/22 | 23/20 | ||||
| Weight (kg) | 63.41 ± 2.42 a | 60.15 ± 2.45 b | 64.72 ± 2.53 a | 63.96 ± 1.86 a | 61.99 ± 1.89 b | 65.46 ± 2.04 a |
| Serum ALT (U/L) | 20.19 ± 1.90 b | 23.52 ± 2.31 b | 29.96 ± 3.31 a,† | 23.29 ± 3.87 | 30.70 ± 6.98 | 23.07 ± 2.69 |
| Serum AST (U/L) | 23.50 ± 1.78 b | 25.25 ± 1.85 b | 32.08 ± 1.91 a,† | 22.20 ± 2.05 | 23.05 ± 2.10 | 24.23 ± 1.96 |
| Serum creatinine (mg/dL) | 0.85 ± 0.03 b | 0.83 ± 0.04 b,** | 0.92 ± 0.04 a | 0.89 ± 0.04 b | 0.93 ± 0.04 a,b | 0.93 ± 0.04 a |
| C-reactive protein (mg/dL) | 1.08 ± 0.30 a,b | 1.46 ± 0.39 b | 0.37 ± 0.17 a | 0.80 ± 0.22 | 0.68 ± 0.14 | 0.33 ± 0.14 |
| Serum albumin (g/dL) | 4.07 ± 0.06 b | 4.17 ± 0.05 b | 4.32 ± 0.05 a,† | 4.13 ± 0.08 c | 4.30 ± 0.06 b | 4.45 ± 0.05 a |
| CEA (ng/mL) | 77.35 ± 47.57 b | 83.75 ± 61.52 a | 4.36 ± 1.03 a | 27.33 ± 11.33 | 10.09 ± 5.09 | 7.26 ± 3.18 |
| CA 19-9 (U/mL) | 288.93 ± 263.34 a | 124.0 ± 95.25 b | 18.01 ± 4.30 a | 73.59 ± 54.67 | 17.56 ± 5.53 | 17.35 ± 3.52 |
| Stage at diagnosis (n, %) Stage 0 Stage I Stage II Stage III Stage IV | – 0 0 32, 66.7% 16, 33.3% | 3, 7% 8, 18.6% 11, 25.6% 13, 30.2% 8, 18.6% | ||||
| Tumor location (n, %) Ascending colon Transverse colon Descending colon Sigmoid colon Rectum | 10, 20.8% 1, 2.1% 8, 16.7% 14, 29.2% 15, 31.3% | 8, 18.6% 1, 2.3% 3, 6.3% 11, 22.9% 20, 41.7% | ||||
| Concurrent chemoradiotherapy before tumor resection (n, %) | 8, 16.7% | – | ||||
| Histological grading (n, %) Well-differentiated Moderately differentiated Moderately to poorly differentiated Poorly differentiated | 1, 2.1% 40, 86.3% 2, 4.2% 5, 10.4% | 1, 2.3% 41, 95.3% 0 1, 2.3% | ||||
| Chemotherapy type (n, %) Single therapy Double therapy Triple therapy | 8, 16.7% 35, 72.9% 5, 10.4% | – – – | ||||
| Parameters | Chemotherapy (n = 48) | Non-Chemotherapy (n = 43) | ||||
|---|---|---|---|---|---|---|
| Pre-Resection | Post-Resection | Post-Chemo | Pre-Resection | Post-Resection | Post-Chemo | |
| MDA (μmol/L) | 1.0 ± 0.03 b | 1.05 ± 0.04 b | 1.28 ± 0.05 a | 0.97 ± 0.03 b | 1.06 ± 0.05 a,b | 1.22 ± 0.06 a |
| AOPP (μmol/L) | 380.67 ± 20.77 b | 523.0 ± 36.71 a | 463.64 ± 30.28 a,b | 385.73 ± 28.82 | 444.41 ± 35.77 | 460.96 ± 30.85 |
| GSH (μmol/L) | 55.74 ± 4.66 a | 89.69 ± 8.14 b | 54.87 ± 4.81 a,† | 73.47 ± 8.52 | 97.07 ± 8.06 | 79.78 ± 5.19 |
| GSSG (μmol/L) | 429.34 ± 13.24 c,* | 522.97 ± 14.76 b | 458.14 ± 15.18 a,† | 468.78 ± 12.64 b | 552.20 ± 12.64 a | 585.48 ± 13.21 a |
| GPx (nmol/mL/min) | 193.01 ± 10.07 c,* | 238.16 ± 9.65 b | 275.92 ± 10.15 a,† | 159.51 ± 8.62 b | 232.19 ± 9.93 a | 232.53 ± 11.01 a |
| GR (nmol/mL/min) | 58.50 ± 2.79 b | 69.74 ± 3.01 a | 73.88 ± 2.43 a,† | 57.17 ± 3.67 | 63.93 ± 2.31 | 64.87 ± 3.04 |
| GST (nmol/mL/min) | 16.91 ± 2.49 b | 26.19 ± 2.93 a | 28.27 ± 4.25 a | 19.54 ± 2.26 b | 32.75 ± 3.82 a | 23.81 ± 2.81 a,b |
| TEAC (μmol/L) | 3811.91 ± 53.52 b | 4382.70 ± 53.24 a | 4461.64 ± 56.79 a,† | 3891.11 ± 49.89 c | 4428.65 ± 70.91 b | 4259.38 ± 54.30 a |
| Parameters | Chemotherapy (n = 48) | Non-Chemotherapy (n = 43) | ||
|---|---|---|---|---|
| Tumor Tissue | Adjacent Normal Tissue | Tumor Tissue | Adjacent Normal Tissue | |
| MDA (μmol/g protein) | 0.20 ± 0.03 | 0.23 ± 0.04 | 0.23 ± 0.05 | 0.28 ± 0.09 |
| AOPP (μmol/g protein) | 109.39 ± 5.60 a,* | 89.50 ± 4.47 b | 136.27 ± 6.56 a | 83.57 ± 4.21 b |
| GSH (μmol/g protein) | 6.91 ± 2.11 * | 5.14 ± 0.72 ** | 11.31 ± 1.41 a | 7.27 ± 0.64 b |
| GSSG (μmol/g protein) | 152.65 ± 12.45 a,* | 120.18 ± 8.30 b,** | 191.94 ± 18.61 a | 137.25 ± 6.54 b |
| GPx (nmol/min/g protein) | 117.48 ± 6.34 a | 97.97 ± 5.20 b | 139.20 ± 9.50 a | 77.89 ± 5.25 b |
| GR (nmol/min/g protein) | 129.30 ± 8.94 | 113.06 ± 7.60 | 156.32 ± 12.55 a | 116.64 ± 8.44 b |
| GST (nmol/min/g protein) | 25.91 ± 1.69 a | 21.42 ± 1.68 b | 31.70 ± 2.49 a | 25.46 ± 1.77 b |
| TEAC (μmol/g protein) | 484.54 ± 32.80 | 436.24 ± 20.55 ** | 450.94 ± 21.51 a | 363.84 ± 22.77 b |
| MDA (μmol/L) | ||||||
|---|---|---|---|---|---|---|
| Chemotherapy (n = 48) | Non-Chemotherapy (n = 43) | |||||
| Pre-Resection | Post-Resection | Post-Chemo | Pre-Resection | Post-Resection | Post-Chemo | |
| GSH (μmol/L) | −0.187 | −0.041 | 0.412 ** | −0.159 | −0.182 | −0.184 |
| GSSG (μmol/L) | −0.069 | 0.014 | 0.445 ** | 0.074 | −0.074 | 0.089 |
| GPx (nmol/mL/min) | −0.172 | −0.133 | −0.087 | 0.347 | −0.069 | −0.172 |
| GR (nmol/mL/min) | 0.186 | 0.071 | 0.042 | 0.106 | 0.086 | 0.106 |
| GST (nmol/mL/min) | −0.168 | −0.283 | 0.202 | 0.231 | 0.128 | 0.052 |
| TEAC (μmol/L) | −0.090 | −0.394 ** | 0.081 | 0.105 | −0.275 | 0.428 * |
| AOPP (μmol/L) | ||||||
| Chemotherapy (n = 48) | Non-chemotherapy (n = 43) | |||||
| Pre-resection | Post-resection | Post-chemo | Pre-resection | Post-resection | Post-chemo | |
| GSH (μmol/L) | 0.151 | 0.356 * | −0.323 * | 0.435 * | −0.278 | −0.167 |
| GSSG (μmol/L) | 0.146 | 0.228 | −0.341 * | 0.248 | −0.497 ** | −0.235 |
| GPx (nmol/mL/min) | 0.251 | 0.079 | 0.249 | −0.153 | −0.068 | −0.009 |
| GR (nmol/mL/min) | 0.045 | 0.208 | 0.319 * | 0.248 | 0.050 | −0.352 |
| GST (nmol/mL/min) | −0.064 | 0.100 | −0.185 | 0.070 | −0.111 | −0.132 |
| TEAC (μmol/L) | 0.076 | 0.117 | 0.211 | 0.028 | 0.229 | −0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, F.-F.; Huang, S.-C.; Yu, P.-T.; Chao, T.-H.; Huang, Y.-C. Oxidative Stress Induced by Chemotherapy: Evaluation of Glutathione and Its Related Antioxidant Enzyme Dynamics in Patients with Colorectal Cancer. Nutrients 2023, 15, 5104. https://doi.org/10.3390/nu15245104
Chiang F-F, Huang S-C, Yu P-T, Chao T-H, Huang Y-C. Oxidative Stress Induced by Chemotherapy: Evaluation of Glutathione and Its Related Antioxidant Enzyme Dynamics in Patients with Colorectal Cancer. Nutrients. 2023; 15(24):5104. https://doi.org/10.3390/nu15245104
Chicago/Turabian StyleChiang, Feng-Fan, Shih-Chien Huang, Pei-Ting Yu, Te-Hsin Chao, and Yi-Chia Huang. 2023. "Oxidative Stress Induced by Chemotherapy: Evaluation of Glutathione and Its Related Antioxidant Enzyme Dynamics in Patients with Colorectal Cancer" Nutrients 15, no. 24: 5104. https://doi.org/10.3390/nu15245104
APA StyleChiang, F.-F., Huang, S.-C., Yu, P.-T., Chao, T.-H., & Huang, Y.-C. (2023). Oxidative Stress Induced by Chemotherapy: Evaluation of Glutathione and Its Related Antioxidant Enzyme Dynamics in Patients with Colorectal Cancer. Nutrients, 15(24), 5104. https://doi.org/10.3390/nu15245104