
Beneficial Effects of Plant Oils Supplementation on Multiple Sclerosis: A Comprehensive Review of Clinical and Experimental Studies



Abstract
1. Introduction
2. Plants Oil and Multiple Sclerosis
2.1. Pomegranate Seed Oil
2.2. Sesame Oil
2.3. Acer Truncatum Bunge Seed Oil
2.4. Hemp Seed Oil and Evening Primrose Oil
2.5. Coconut Oil
2.6. Walnut Oil
2.7. Essential Oil from Pterodon emarginatus Seeds
2.8. Flaxseed Oil
2.9. Olive Oil
3. Perspectives and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Evans, C.; Beland, S.G.; Kulaga, S.; Wolfson, C.; Kingwell, E.; Marriott, J.; Koch, M.; Makhani, N.; Morrow, S.; Fisk, J.; et al. Incidence and prevalence of multiple sclerosis in the Americas: A systematic review. Neuroepidemiology 2013, 40, 195–210. [Google Scholar] [CrossRef]
- Harbo, H.F.; Gold, R.; Tintoré, M. Sex and gender issues in multiple sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237–248. [Google Scholar] [CrossRef]
- Mahad, D.H.; Trapp, B.D.; Lassmann, H. Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol. 2015, 14, 183–193. [Google Scholar] [CrossRef]
- Katz Sand, I. Classification, diagnosis, and differential diagnosis of multiple sclerosis. Curr. Opin. Neurol. 2015, 28, 193–205. [Google Scholar] [CrossRef]
- Gaby, A. Multiple sclerosis. Glob. Adv. Health Med. 2013, 2, 50–56. [Google Scholar] [CrossRef]
- Green, R.; Cutter, G.; Friendly, M.; Kister, I. Which Symptoms Contribute the Most to Patients’ Perception of Health in Multiple Sclerosis? Mult. Scler. J. Exp. Transl. Clin. 2017, 3, 2055217317728301. [Google Scholar] [CrossRef]
- Penesová, A.; Dean, Z.; Kollár, B.; Havranová, A.; Imrich, R.; Vlček, M.; Rádiková, Ž. Nutritional intervention as an essential part of multiple sclerosis treatment? Physiol. Res. 2018, 67, 521–533. [Google Scholar] [CrossRef]
- Katz Sand, I. The Role of Diet in Multiple Sclerosis: Mechanistic Connections and Current Evidence. Curr. Nutr. Rep. 2018, 7, 150–160. [Google Scholar] [CrossRef]
- Fancy, S.P.; Kotter, M.R.; Harrington, E.P.; Huang, J.K.; Zhao, C.; Rowitch, D.H.; Franklin, R.J. Overcoming remyelination failure in multiple sclerosis and other myelin disorders. Exp. Neurol. 2010, 225, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Procaccini, C.; De Rosa, V.; Pucino, V.; Formisano, L.; Matarese, G. Animal models of Multiple Sclerosis. Eur. J. Pharmacol. 2015, 759, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.P.; Harp, C.T.; Noronha, A.; Miller, S.D. The experimental autoimmune encephalomyelitis (EAE) model of MS: Utility for understanding disease pathophysiology and treatment. Handb. Clin. Neurol. 2014, 122, 173–189. [Google Scholar] [PubMed]
- MS Society of Canada. Medications. 2016. Available online: https://mssociety.ca/managing-ms/treatments/medications (accessed on 21 September 2016).
- Katsavos, S.; Anagnostouli, M. Biomarkers in Multiple Sclerosis: An Up-to-Date Overview. Mult. Scler. Int. 2013, 2013, 340508. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.M. Multiple sclerosis review. Pharm. Ther. 2012, 37, 175–184. [Google Scholar]
- Khan, O.; Filippi, M.; Freedman, M.S.; Barkhof, F.; Dore-Duffy, P.; Lassmann, H.; Trapp, B.; Bar-Or, A.; Zak, I.; Siegel, M.J.; et al. Chronic cerebrospinal venous insufficiency and multiple sclerosis. Ann. Neurol. 2010, 67, 286–290. [Google Scholar] [CrossRef]
- Zamboni, P.; Tesio, L.; Galimberti, S.; Massacesi, L.; Salvi, F.; D’Alessandro, R.; Cenni, P.; Galeotti, R.; Papini, D.; D’Amico, R.; et al. Efficacy and Safety of Extracranial Vein Angioplasty in Multiple Sclerosis: A Randomized Clinical Trial. JAMA Neurol. 2018, 75, 35–43. [Google Scholar] [CrossRef]
- Namjooyan, F.; Ghanavati, R.; Majdinasab, N.; Jokari, S.; Janbozorgi, M. Uses of complementary and alternative medicine in multiple sclerosis. J. Tradit. Complement. Med. 2014, 4, 145–152. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R.; Larocca, M.; Trotta, V.; Mennella, I.; Vitaglione, P.; Ettorre, M.; Graverini, A.; De Santis, A.; Di Monte, E.; et al. Anti-inflammatory nutritional intervention in patients with relapsing-remitting and primary-progressive multiple sclerosis. Exp. Biol. Med. 2016, 241, 620–635. [Google Scholar] [CrossRef]
- Hadgkiss, E.J.; Jelinek, G.A.; Weiland, T.J.; Pereira, N.G.; Marck, C.H.; van der Meer, D.M. The association of diet with quality of life, disability, and relapse rate in an international sample of people with multiple sclerosis. Nutr. Neurosci. 2015, 18, 125–136. [Google Scholar] [CrossRef]
- Lee, D.H.; Gold, R.; Linker, R.A. Mechanisms of oxidative damage in multiple sclerosis and neurodegenerative diseases: Therapeutic modulation via fumaric acid esters. Int. J. Mol. Sci. 2012, 13, 11783–11803. [Google Scholar] [CrossRef]
- Miller, E.D.; Dziedzic, A.; Saluk-Bijak, J.; Bijak, M. A Review of Various Antioxidant Compounds and their Potential Utility as Complementary Therapy in Multiple Sclerosis. Nutrients 2019, 11, 1528. [Google Scholar] [CrossRef] [PubMed]
- Stoiloudis, P.; Kesidou, E.; Bakirtzis, C.; Sintila, S.A.; Konstantinidou, N.; Boziki, M.; Grigoriadis, N. The Role of Diet and Interventions on Multiple Sclerosis: A Review. Nutrients 2022, 14, 1150. [Google Scholar] [CrossRef] [PubMed]
- Bagur, M.J.; Murcia, M.A.; Jiménez-Monreal, A.M.; Tur, J.A.; Bibiloni, M.M.; Alonso, G.L.; Martínez-Tomé, M. Influence of Diet in Multiple Sclerosis: A Systematic Review. Adv. Nutr. 2017, 8, 463–472. [Google Scholar] [CrossRef]
- Esposito, S.; Bonavita, S.; Sparaco, M.; Gallo, A.; Tedeschi, G. The role of diet in multiple sclerosis: A review. Nutr. Neurosci. 2018, 21, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Al Ammar, W.A.; Albeesh, F.H.; Ibrahim, L.M.; Algindan, Y.Y.; Yamani, L.Z.; Khattab, R.Y. Effect of omega-3 fatty acids and fish oil supplementation on multiple sclerosis: A systematic review. Nutr. Neurosci. 2021, 24, 569–579. [Google Scholar] [CrossRef]
- Torkildsen, O.; Wergeland, S.; Bakke, S.; Beiske, A.G.; Bjerve, K.S.; Hovdal, H.; Midgard, R.; Lilleås, F.; Pedersen, T.; Bjørnarå, B.; et al. ω-3 Fatty Acid Treatment in Multiple Sclerosis (OFAMS Study): A Randomized, Double-Blind, Placebo-Controlled Trial. Arch. Neurol. 2012, 69, 1044–1051. [Google Scholar] [CrossRef]
- Del Campo, C.P.; Tunez, I. Crosstalk between Gut Microbiota and the Central Nervous System in Multiple Sclerosis: Strengths, Weaknesses, Opportunities and Threats Analysis of the Use of an Experimental Model. CNS Neurol. Disord. Drug Targets 2017, 16, 971–973. [Google Scholar] [CrossRef]
- Harbige, L.S.; Layward, L.; Morris-Downes, M.M.; Dumonde, D.C.; Amor, S. The protective effects of omega-6 fatty acids in experimental autoimmune encephalomyelitis (EAE) in relation to transforming growth factor-beta 1 (TGF-beta1) up-regulation and increased prostaglandin E2 (PGE2) production. Clin. Exp. Immunol. 2000, 122, 445–452. [Google Scholar] [CrossRef]
- Salas, J.J.; Sánchez, J.; Ramli, U.S.; Manaf, A.M.; Williams, M.; Harwood, J.L. Biochemistry of lipid metabolism in olive and other oil fruits. Prog. Lipid Res. 2000, 39, 151–180. [Google Scholar] [CrossRef]
- Saresella, M.; Mendozzi, L.; Rossi, V.; Mazzali, F.; Piancone, F.; LaRosa, F.; Marventano, I.; Caputo, D.; Felis, G.E.; Clerici, M. Immunological and Clinical Effect of Diet Modulation of the Gut Microbiome in Multiple Sclerosis Patients: A Pilot Study. Front. Immunol. 2017, 8, 1391. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R. Nutrition facts in multiple sclerosis. ASN Neuro 2015, 7, 1759091414568185. [Google Scholar] [CrossRef]
- Mannucci, P.M.; Jolliet, O.; Meijaard, E.; Slavin, J.; Rasetti, M.; Aleta, A.; Moreno, Y.; Agostoni, C. Sustainable nutrition and the case of vegetable oils to match present and future dietary needs. Front. Public Health 2023, 11, e1106083. [Google Scholar] [CrossRef]
- Santika, T.; Budiharta, S.; Law, E.A.; Struebig, M.; Ancrenaz, M.; Poh, T.M.; Meijaard, E. Does oil palm agriculture help alleviate poverty? A multidimensional counterfactual assessment of oil palm development in Indonesia. World Dev. 2019, 120, 105–117. [Google Scholar] [CrossRef]
- Kýralan, M.; Gölükcü, M.; Tokgöz, H. Oil and Conjugated Linolenic Acid Contents of Seeds from Important Pomegranate Cultivars (Punica granatum, L.) Grown in Turkey. J. Am. Oil Chem. Soc. 2009, 86, 985–990. [Google Scholar] [CrossRef]
- Sassano, G.; Sanderson, P.; Franx, J.; Groot, P.; Straalen, J.; Bassaganya-Riera, J. Analysis of pomegranate seed oil for the presence of jacaric acid. J. Sci. Food Agric. 2009, 89, 1046–1052. [Google Scholar] [CrossRef]
- Viladomiu, M.; Hontecillas, R.; Lu, P.; Bassaganya-Riera, J. Preventive and prophylactic mechanisms of action of pomegranate bioactive constituents. Evid. Based Complement. Alternat. Med. 2013, 2013, 789764. [Google Scholar] [CrossRef]
- Kaseke, T.; Opara, U.L.; Fawole, O.A. Effects of Enzymatic Pretreatment of Seeds on the Physicochemical Properties, Bioactive Compounds, and Antioxidant Activity of Pomegranate Seed Oil. Molecules 2021, 26, 4575. [Google Scholar] [CrossRef]
- Fernandes, L.; Pereira, J.A.; Lopéz-Cortés, I.; Salazar, D.M.; Ramalhosa, E.; Casal, S. Fatty acid, vitamin E and sterols composition of seed oils from nine different pomegranate (Punica granatum L.) cultivars grown in Spain. J. Food Compos. Anal. 2015, 39, 13–22. [Google Scholar] [CrossRef]
- Mollazadeh, H.; Sadeghnia, H.R.; Hoseini, A.; Farzadnia, M.; Boroushaki, M.T. Effects of pomegranate seed oil on oxidative stress markers, serum biochemical parameters and pathological findings in kidney and heart of streptozotocin-induced diabetic rats. Ren. Fail 2016, 38, 1256–1266. [Google Scholar] [CrossRef]
- Harzallah, A.; Hammami, M.; Kępczyńska, M.A.; Hislop, D.C.; Arch, J.R.; Cawthorne, M.A.; Zaibi, M.S. Comparison of potential preventive effects of pomegranate flower, peel and seed oil on insulin resistance and inflammation in high-fat and high-sucrose diet-induced obesity mice model. Arch. Physiol. Biochem. 2016, 122, 75–87. [Google Scholar] [CrossRef]
- Qubty, D.; Frid, K.; Har-Even, M.; Rubovitch, V.; Gabizon, R.; Pick, C.G. Nano-PSO Administration Attenuates Cognitive and Neuronal Deficits Resulting from Traumatic Brain Injury. Molecules 2022, 27, 2725. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M. Pomegranate Protection against Cardiovascular Diseases. Evid. Based Complement. Alternat. Med. 2012, 2012, 382763. [Google Scholar] [CrossRef]
- Petrou, P.; Ginzberg, A.; Binyamin, O.; Karussis, D. Beneficial effects of a nano formulation of pomegranate seed oil, GranaGard, on the cognitive function of multiple sclerosis patients. Mult. Scler. Relat. Disord. 2021, 54, e103103. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Polman, C.H.; Rudick, R.A. The multiple sclerosis functional composite: A clinically meaningful measure of disability. Neurology. 2010, 74, S8–S15. [Google Scholar] [CrossRef]
- Langdon, D.W.; Amato, M.P.; Boringa, J.; Brochet, B.; Foley, F.; Fredrikson, S.; Hämäläinen, P.; Hartung, H.P.; Krupp, L.; Penner, I.K.; et al. Recommendations for a Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS). Mult. Scler. 2012, 18, 891–898. [Google Scholar] [CrossRef]
- Guerra-Vázquez, C.M.; Martínez-Ávila, M.; Guajardo-Flores, D.M.; Antunes-Ricardo, M. Punicic Acid and Its Role in the Prevention of Neurological Disorders: A Review. Foods 2022, 11, 252. [Google Scholar] [CrossRef]
- Estrada-Luna, D.; Carreón-Torres, E.; Bautista-Pérez, R.; Betanzos-Cabrera, G.; Dorantes-Morales, A.; Luna-Luna, M.; Vargas-Barrón, J.; Mejía, A.M.; Fragoso, J.M.; Carvajal-Aguilera, K.; et al. Microencapsulated Pomegranate Reverts High-Density Lipoprotein (HDL)-Induced Endothelial Dysfunction and Reduces Postprandial Triglyceridemia in Women with Acute Coronary Syndrome. Nutrients 2019, 11, 1710. [Google Scholar] [CrossRef]
- Su, N.D.; Liu, X.W.; Kim, M.R.; Jeong, T.S.; Sok, D.E. Protective action of CLA against oxidative inactivation of paraoxonase 1, an antioxidant enzyme. Lipids 2003, 38, 615–622. [Google Scholar] [CrossRef]
- Binyamin, O.; Larush, L.; Frid, K.; Keller, G.; Friedman-Levi, Y.; Ovadia, H.; Abramsky, O.; Magdassi, S.; Gabizon, R. Treatment of a multiple sclerosis animal model by a novel nanodrop formulation of a natural antioxidant. Int. J. Nanomed. 2015, 10, 7165–7174. [Google Scholar] [CrossRef]
- Kim, D.; Park, J.H.; Kweon, D.J.; Han, G.D. Bioavailability of nanoemulsified conjugated linoleic acid for an antiobesity effect. Int. J. Nanomed. 2013, 8, 451–459. [Google Scholar]
- Karlík, M.; Valkovič, P.; Hančinová, V.; Krížová, L.; Tóthová, Ľ.; Celec, P. Markers of oxidative stress in plasma and saliva in patients with multiple sclerosis. Clin. Biochem. 2015, 48, 24–28. [Google Scholar] [CrossRef]
- Ferretti, G.; Bacchetti, T. Peroxidation of lipoproteins in multiple sclerosis. J. Neurol. Sci. 2011, 311, 92–97. [Google Scholar] [CrossRef]
- Leitinger, N. The role of phospholipid oxidation products in inflammatory and autoimmune diseases: Evidence from animal models and in humans. Subcell Biochem. 2008, 49, 325–350. [Google Scholar]
- Mizrahi, M.; Friedman-Levi, Y.; Larush, L.; Frid, K.; Binyamin, O.; Dori, D.; Fainstein, N.; Ovadia, H.; Ben-Hur, T.; Magdassi, S.; et al. Pomegranate seed oil nanoemulsions for the prevention and treatment of neurodegenerative diseases: The case of genetic CJD. Nanomed. Nanotechnol. Biol. Med. 2014, 10, 1353–1363. [Google Scholar] [CrossRef]
- Lu, X.Y.; Han, B.; Deng, X.; Deng, S.Y.; Zhang, Y.Y.; Shen, P.X.; Hui, T.; Chen, R.H.; Li, X.; Zhang, Y. Pomegranate peel extract ameliorates the severity of experimental autoimmune encephalomyelitis via modulation of gut microbiota. Gut Microbes 2020, 12, 1857515. [Google Scholar] [CrossRef]
- Gharby, S.; Harhar, H.; Bouzoubaa, Z.; Asdadi, A.; El Yadini, A.; Charrouf, Z. Chemical characterization and oxidative stability of seeds and oil of sesame grown in Morocco. J. Saudi Soc. Agric. Sci. 2017, 16, 105–111. [Google Scholar] [CrossRef]
- Ramesh, B.; Saravanan, R.; Pugalendi, K.V. Influence of sesame oil on blood glucose, lipid peroxidation, and antioxidant status in streptozotocin diabetic rats. J. Med. Food 2005, 8, 377–381. [Google Scholar] [CrossRef]
- Hsu, C.C.; Huang, H.C.; Wu, P.T.; Tai, T.W.; Jou, I.M. Sesame oil improves functional recovery by attenuating nerve oxidative stress in a mouse model of acute peripheral nerve injury: Role of Nrf-2. J. Nutr. Biochem. 2016, 38, 102–106. [Google Scholar] [CrossRef]
- Faraji, F.; Hashemi, M.; Ghiasabadi, A.; Davoudian, S.; Talaie, A.; Ganji, A.; Mosayebi, G. Combination therapy with interferon beta-1a and sesame oil in multiple sclerosis. Complement. Ther. Clin. Pract. 2019, 45, 275–279. [Google Scholar] [CrossRef]
- Narasimhulu, C.A.; Selvarajan, K.; Litvinov, D.; Parthasarathy, S. Anti-atherosclerotic and anti-inflammatory actions of sesame oil. J. Med. Food 2015, 18, 11–20. [Google Scholar] [CrossRef]
- Jiang, H.R.; Milovanović, M.; Allan, D.; Niedbala, W.; Besnard, A.G.; Fukada, S.Y.; Alves-Filho, J.C.; Togbe, D.; Goodyear, C.S.; Linington, C.; et al. IL-33 attenuates EAE by suppressing IL-17 and IFN-γ production and inducing alternatively activated macrophages. Eur. J. Immunol. 2012, 42, 1804–1814. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Lin, Y. Interferon-γ inhibits central nervous system myelination through both STAT1-dependent and STAT1-independent pathways. J. Neurosci. Res. 2010, 88, 2569–2577. [Google Scholar] [CrossRef]
- Guinness, N.M.; Dungan, L.S.; Lynch, M.A.; Mills, K.H. Interferon-gamma-producing natural killer cells are patho-genic in experimental autoimmune encephalomyelitis by promoting M1 macrophage activation and VLA-4 expression on CD4+ T cells. J. Neuroimmunol. 2014, 275, 119–120. [Google Scholar] [CrossRef]
- Tyler, A.F.; Mendoza, J.P.; Firan, M.; Karandikar, N.J. CD8(+) T Cells Are Required For Glatiramer Acetate Therapy in Autoimmune Demyelinating Disease. PLoS ONE 2013, 8, e66772. [Google Scholar] [CrossRef]
- Javan, M.R.; Zamani, M.R.; Aslani, S.; Dargahi Abbasabad, G.; Beirami Khalaj, M.; Serati-Nouri, H. Cytokine Modulatory Effects of Sesamum Indicum Seeds Oil Ameliorate Mice with Experimental Autoimmune Encephalomyelitis. Arch. Asthma Allergy Immunol. 2017, 1, 086–093. [Google Scholar]
- O’Neill, E.J.; Day, M.J.; Wraith, D.C. IL-10 is essential for disease protection following intranasal peptide administration in the C57BL/6 model of EAE. J. Neuroimmunol. 2006, 178, 1–8. [Google Scholar] [CrossRef]
- Staykova, M.A.; Fordham, S.A.; Bartell, G.J.; Cowden, W.B.; Willenborg, D.O. Nitric oxide contributes to the resistance of young SJL/J mice to experimental autoimmune encephalomyelitis. J. Neuroimmunol. 2006, 176, 1–8. [Google Scholar] [CrossRef]
- Mosayebi, G.; Ghazavi, A.; Salehi, H.; Payani, M.A.; Khazae, M.R. Effect of sesame oil on the inhibition of experimental autoimmune encephalomyelitis in C57BL/6 mice. Pak. J. Biol. Sci. 2007, 10, 1790–1796. [Google Scholar] [CrossRef]
- Song, W.; Zhang, K.; Xue, T.; Han, J.; Peng, F.; Ding, C.; Lin, F.; Li, J.; Sze, F.T.A.; Gan, J.; et al. Cognitive improvement effect of nervonic acid and essential fatty acids on rats ingesting Acer truncatum Bunge seed oil revealed by lipidomics approach. Food Funct. 2022, 13, 2475–2490. [Google Scholar] [CrossRef]
- Amminger, G.P.; Schäfer, M.R.; Klier, C.M.; Slavik, J.M.; Holzer, I.; Holub, M.; Goldstone, S.; Whitford, T.J.; McGorry, P.D.; Berk, M. Decreased nervonic acid levels in erythrocyte membranes predict psychosis in help-seeking ultra-high-risk individuals. Mol. Psychiatry 2012, 17, 1150–1152. [Google Scholar] [CrossRef]
- Liang, Y.; Kong, F.; Ma, X.; Shu, Q. Inhibitory Effect of Acer truncatum Bunge Seed Coat Extract on Fatty Acid Synthase, Differentiation and Lipid Accumulation in 3T3-L1 Adipocytes. Molecules 2022, 27, 1324. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, T.; Hong, X.Y.; Liu, J.J.; Yang, X.F.; Liu, G.P. Acer truncatum Seed Oil Alleviates Learning and Memory Impairments of Aging Mice. Front. Cell Dev. Biol. 2021, 9, 680386. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.C.; Gilmore, W.; Ting, J.P.; Matsushima, G.K. Cuprizone induces similar demyelination in male and female C57BL/6 mice and results in disruption of the estrous cycle. J. Neurosci. Res. 2010, 88, 391–402. [Google Scholar] [CrossRef]
- Xue, Y.; Zhu, X.; Yan, W.; Zhang, Z.; Cui, E.; Wu, Y.; Li, C.; Pan, J.; Yan, Q.; Chai, X.; et al. Dietary Supplementation with Acer truncatum Oil Promotes Remyelination in a Mouse Model of Multiple Sclerosis. Front. Neurosci. 2022, 16, 860280. [Google Scholar] [CrossRef]
- Callaway, J.C. Hempseed as a nutritional resource: An overview. Euphytica 2004, 140, 65–72. [Google Scholar] [CrossRef]
- Islam, M.; Rajagukguk, Y.V.; Siger, A.; Tomaszewska-Gras, J. Assessment of Hemp Seed Oil Quality Pressed from Fresh and Stored Seeds of Henola Cultivar Using Differential Scanning Calorimetry. Foods 2022, 12, 135. [Google Scholar] [CrossRef]
- Okuyama, H.; Kobayashi, T.; Watanabe, S. Dietary fatty acids—The N-6/N-3 balance and chronic elderly diseases. Excess linoleic acid and relative N-3 deficiency syndrome seen in Japan. Prog. Lipid Res. 1996, 35, 409–457. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P.; Leaf, A.; Salem, N., Jr. Workshop statement on the essentiality of and recommended dietary intakes for Omega-6 and Omega-3 fatty acids. Prostaglandins Leukot. Essent. Fat. Acids 2000, 63, 119–121. [Google Scholar] [CrossRef]
- Matthäus, B.; Brühl, L. Virgin hemp seed oil: An interesting niche product. Eur. J. Lipid Sci. Technol. 2008, 110, 655–661. [Google Scholar] [CrossRef]
- Vitorović, J.; Joković, N.; Radulović, N.; Mihajilov-Krstev, T.; Cvetković, V.J.; Jovanović, N.; Mitrović, T.; Aleksić, A.; Stanković, N.; Bernstein, N. Antioxidant Activity of Hemp (Cannabis sativa L.) Seed Oil in Drosophila melanogaster Larvae under Non-Stress and H2O2-Induced Oxidative Stress Conditions. Antioxidants 2021, 10, 830. [Google Scholar] [CrossRef] [PubMed]
- Claro-Cala, C.M.; Grao-Cruces, E.; Toscano, R.; Millan-Linares, M.C.; Montserrat-de la Paz, S.; Martin, M.E. Acyclic Diterpene Phytol from Hemp Seed Oil (Cannabis sativa L.) Exerts Anti-Inflammatory Activity on Primary Human Monocytes-Macrophages. Foods 2022, 11, 2366. [Google Scholar] [CrossRef]
- Christie, W.W. The analysis of evening primrose oil. Ind. Crops Prod. 1999, 10, 73–83. [Google Scholar] [CrossRef]
- Ben-Nun, A.; Mendel, I.; Bakimer, R.; Fridkis-Hareli, M.; Teitelbaum, D.; Arnon, R.; Sela, M.; Kerlero de Rosbo, N. The autoimmune reactivity to myelin oligodendrocyte glycoprotein (MOG) in multiple sclerosis is potentially pathogenic: Effect of copolymer 1 on MOG-induced disease. J. Neurol. 1996, 243, S14–S22. [Google Scholar] [CrossRef] [PubMed]
- Rezapour-Firouzi, S.; Seyed, R.; Farhoudi, M.; Ebrahimi-Mamagha, M.; Baradaran, B.; Sadeghihokmabad, E.; Mostafaei, S.; Torbati, M.A. Regulation of Lipid-dependent Membrane Enzymes by Hot Nature Diet with Co-Supplemented Hemp Seed, Evening Primrose Oils Intervention in Multiple Sclerosis Patients. J. Pure Appl. Microbiol. 2013, 7, 2891–2901. [Google Scholar]
- Van Meeteren, M.E.; Teunissen, C.E.; Dijkstra, C.D.; van Tol, E.A. Antioxidants and polyunsaturated fatty acids in multiple sclerosis. Eur. J. Clin. Nutr. 2005, 59, 1347–1361. [Google Scholar] [CrossRef]
- Rezapour-Firouzi, S.; Mohammadian, M.; Sadeghzadeh, M.; Mazloomi, E. Effects of co-administration of rapamycin and evening primrose/hemp seed oil supplement on immunologic factors and cell membrane fatty acids in experimental autoimmune encephalomyelitis. Gene 2020, 759, 144987. [Google Scholar] [CrossRef]
- Mitchell, M.D. Biochemistry of the prostaglandins. Baillieres Best Pract. Res. Clin. Obstet. Gynaecol. 1992, 6, 687–706. [Google Scholar] [CrossRef]
- Horrobin, D.F. Multiple sclerosis: The rational basis for treatment with colchicine and evening primrose oil. Med. Hypotheses 1979, 5, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Rezapour-Firouzi, S.; Kheradmand, F.; Shahabi, S.; Tehrani, A.A.; Mazloomi, E.; Mohammadzadeh, A. Regulatory effects of hemp seed/evening primrose oil supplement in comparison with rapamycin on the expression of the mammalian target of rapamycin-complex 2 and interleukin-10 genes in experimental autoimmune encephalomyelitis. Res. Pharm. Sci. 2019, 14, 36–45. [Google Scholar] [PubMed]
- Lisi, L.; Navarra, P.; Cirocchi, R.; Sharp, A.; Stigliano, E.; Feinstein, D.L.; Dello Russo, C. Rapamycin reduces clinical signs and neuropathic pain in a chronic model of experimental autoimmune encephalomyelitis. J. Neuroimmunol. 2012, 243, 43–51. [Google Scholar] [CrossRef]
- Majdinasab, N.; Namjoyan, F.; Taghizadeh, M.; Saki, H. The effect of evening primrose oil on fatigue and quality of life in patients with multiple sclerosis. Neuropsychiatr. Dis. Treat. 2018, 14, 1505–1512. [Google Scholar] [CrossRef]
- Salem, M.L.; El-Naggar, R. Immunomodulatory and antitumor effects of simultaneous treatment of mice with ω3 and ω6 polyunsaturated fatty acids. Union Arab. Biol. 2000, 14, 489–505. [Google Scholar]
- Rezapour-Firouzi, S.; Arefhosseini, S.R.; Ebrahimi-Mamaghani, M.; Baradaran, B.; Sadeghihokmabad, E.; Torbati, M.; Mostafaei, S.; Chehreh, M.; Zamani, F. Activity of liver enzymes in multiple sclerosis patients with Hot-nature diet and co-supplemented hemp seed, evening primrose oils intervention. Complement. Ther. Med. 2014, 22, 986–993. [Google Scholar] [CrossRef]
- Rezapour-Firouzi, S.; Arefhosseini, S.R.; Mehdi, F.; Mehrangiz, E.M.; Baradaran, B.; Sadeghihokmabad, E.; Mostafaei, S.; Fazljou, S.M.; Torbati, M.A.; Sanaie, S.; et al. Immunomodulatory and therapeutic effects of Hot-nature diet and co-supplemented hemp seed, evening primrose oils intervention in multiple sclerosis patients. Complement. Ther. Med. 2013, 21, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.Y.; Xu, J.; Jensen, M.D.; Simonyi, A. Phospholipase A2 in the central nervous system: Implications for neurodegenerative diseases. J. Lipid Res. 2004, 45, 205–213. [Google Scholar] [CrossRef]
- Kalyvas, A.; Baskakis, C.; Magrioti, V.; Constantinou-Kokotou, V.; Stephens, D.; López-Vales, R.; Lu, J.Q.; Yong, V.W.; Dennis, E.A.; Kokotos, G.; et al. Differing roles for members of the phospholipase A2 superfamily in experimental autoimmune encephalomyelitis. Brain 2009, 132, 1221–1235. [Google Scholar] [CrossRef]
- Cunningham, T.J.; Yao, L.; Oetinger, M.; Cort, L.; Blankenhorn, E.P.; Greenstein, J.I. Secreted phospholipase A2 activity in experimental autoimmune encephalomyelitis and multiple sclerosis. J. Neuroinflam. 2006, 3, 26. [Google Scholar] [CrossRef][Green Version]
- Rezapour-Firouzi, S.; Arefhosseini, S.R.; Farhoudi, M.; Ebrahimi-Mamaghani, M.; Rashidi, M.R.; Torbati, M.A.; Baradaran, B. Association of Expanded Disability Status Scale and Cytokines after Intervention with Co-supplemented Hemp Seed, Evening Primrose Oils and Hot-natured Diet in Multiple Sclerosis Patients. BioImpacts 2013, 3, 43–47. [Google Scholar] [PubMed]
- DebMandal, M.; Mandal, S. Coconut (Cocos nucifera L.: Arecaceae): In health promotion and disease prevention. Asian Pac. J. Trop. Med. 2011, 4, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Clegg, M.E. They say coconut oil can aid weight loss, but can it really. Eur. J. Clin. Nutr. 2017, 71, 1139–1143. [Google Scholar] [CrossRef]
- Famurewa, A.C.; Aja, P.M.; Maduagwuna, E.K.; Ekeleme-Egedigwe, C.A.; Ufebe, O.G.; Azubuike-Osu, S.O. Antioxidant, and anti-inflammatory effects of virgin coconut oil supplementation abrogate acute chemotherapy oxidative nephrotoxicity induced by anticancer drug methotrexate in rats. Biomed. Pharmacother. 2017, 96, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Gandotra, S.; Kour, J.; Van Der Waag, A. Efficacy of adjunctive extra virgin coconut oil use in moderate to severe Alzheimer’s disease. Int. J. Sch. Cogn. Psychol. 2014, 1, 10000108. [Google Scholar]
- Platero, J.L.; López-Rodríguez, M.M.; García-Pardo, P.; de la Rubia Ortí, J.E. Possible Benefits of Coconut Oil in Multiple Sclerosis. Ann. Food Process. Preserv. 2018, 3, 1024. [Google Scholar]
- Vitor, R.J.S., 2nd; Tochinai, R.; Sekizawa, S.I.; Kuwahara, M. Favorable Effects of Virgin Coconut Oil on Neuronal Damage and Mortality after a Stroke Incidence in the Stroke-Prone Spontaneously Hypertensive Rat. Life 2022, 12, 1857. [Google Scholar] [CrossRef] [PubMed]
- Cuerda-Ballester, M.; Proaño, B.; Alarcón-Jimenez, J.; de Bernardo, N.; Villaron-Casales, C.; Lajara Romance, J.M.; de la Rubia Ortí, J.E. Improvements in gait and balance in patients with multiple sclerosis after treatment with coconut oil and epigallocatechin gallate. A pilot study. Food Funct. 2023, 14, 1062–1071. [Google Scholar] [CrossRef]
- Page, K.A.; Williamson, A.; Yu, N.; McNay, E.C.; Dzuira, J.; McCrimmon, R.J.; Sherwin, R.S. Medium-chain fatty acids improve cognitive function in intensively treated type 1 diabetic patients and support in vitro synaptic transmission during acute hypoglycemia. Diabetes 2009, 58, 1237–1244. [Google Scholar] [CrossRef]
- Lim, S.; Chesser, A.S.; Grima, J.C.; Rappold, P.M.; Blum, D.; Przedborski, S.; Tieu, K. D-β-hydroxybutyrate is protective in mouse models of Huntington’s disease. PloS ONE 2011, 6, e24620. [Google Scholar] [CrossRef]
- Kashiwaya, Y.; Bergman, C.; Lee, J.H.; Wan, R.; King, M.T.; Mughal, M.R.; Okun, E.; Clarke, K.; Mattson, M.P.; Veech, R.L. A ketone ester diet exhibits anxiolytic and cognition-sparing properties and lessens amyloid and tau pathologies in a mouse model of Alzheimer’s disease. Neurobiol. Aging 2013, 34, 1530–1539. [Google Scholar] [CrossRef]
- Lu, Y.; Yang, Y.Y.; Zhou, M.W.; Liu, N.; Xing, H.Y.; Liu, X.X.; Li, F. Ketogenic diet attenuates oxidative stress and inflammation after spinal cord injury by activating Nrf2 and suppressing the NF-κB signaling pathways. Neurosci. Lett. 2018, 683, 13–18. [Google Scholar] [CrossRef]
- Bock, M.; Karber, M.; Kuhn, H. Ketogenic diets attenuate cyclooxygenase and lipoxygenase gene expression in multiple sclerosis. EBioMedicine 2018, 36, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Platero, J.L.; Cuerda-Ballester, M.; Ibáñez, V.; Sancho, D.; Lopez-Rodríguez, M.M.; Drehmer, E.; Ortí, J.E.R. The Impact of Coconut Oil and Epigallocatechin Gallate on the Levels of IL-6, Anxiety and Disability in Multiple Sclerosis Patients. Nutrients 2020, 12, 305. [Google Scholar] [CrossRef] [PubMed]
- Gao, P.; Liu, R.J.; Jin, Q.Z.; Wang, X.G. Comparison of different processing methods of iron walnut oils (Juglans sigillata): Lipid yield, lipid compositions, minor components, and antioxidant capacity. Eur. J. Lipid. Sci. Technol. 2018, 120, 1800151. [Google Scholar] [CrossRef]
- Muthaiyah, B.; Essa, M.M.; Lee, M.; Chauhan, V.; Kaur, K.; Chauhan, A. Dietary supplementation of walnuts improves memory deficits and learning skills in transgenic mouse model of Alzheimer’s disease. J. Alzheimers Dis. 2014, 42, 1397–1405. [Google Scholar] [CrossRef]
- Liao, J.; Nai, Y.; Feng, L.; Chen, Y.; Li, M.; Xu, H. Walnut oil prevents scopolamine-induced memory dysfunction in a mouse model. Molecules 2020, 25, 1630. [Google Scholar] [CrossRef]
- Ganji, A.; Farahani, I.; Palizvan, M.R.; Ghazavi, A.; Ejtehadifar, M.; Ebrahimimonfared, M.; Shojapour, M.; Mosayebi, G. Therapeutic effects of walnut oil on the animal model of multiple sclerosis. Nutr. Neurosci. 2019, 22, 215–222. [Google Scholar] [CrossRef]
- Dutra, R.C.; Fava, M.B.; Alves, C.C.; Ferreira, A.P.; Barbosa, N.R. Antiulcerogenic and anti-inflammatory activities of the essential oil from Pterodon emarginatus seeds. J. Pharm. Pharmacol. 2009, 61, 243–250. [Google Scholar] [CrossRef]
- Martín, R.; Hernández, M.; Córdova, C.; Nieto, M.L. Natural triterpenes modulate immune-inflammatory markers of experimental autoimmune encephalomyelitis: Therapeutic implications for multiple sclerosis. Br. J. Pharmacol. 2012, 166, 1708–1723. [Google Scholar] [CrossRef]
- Coelho, M.G.; Sabino, K.C.; Dalmau, S.R. Immunomodulatory effects of sucupira (Pterodon pubescens) seed infusion on collagen-induced arthritis. Clin. Exp. Rheumatol. 2004, 22, 213–218. [Google Scholar]
- Perry, V.H.; Nicoll, J.A.; Holmes, C. Microglia in neurodegenerative disease. Nat. Rev. Neurol. 2010, 6, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Alberti, T.B.; Marcon, R.; Bicca, M.A.; Raposo, N.R.; Calixto, J.B.; Dutra, R.C. Essential oil from Pterodon emarginatus seeds ameliorates experimental autoimmune encephalomyelitis by modulating Th1/Treg cell balance. J. Ethnopharmacol. 2014, 155, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wang, L.; Li, D.; Li, S.; Necati Özkan, N. Characteristics of flaxseed oil from two different flax plants. Int. J. Food Prop. 2011, 14, 1286–1296. [Google Scholar] [CrossRef]
- Jangale, N.M.; Devarshi, P.P.; Dubal, A.A.; Ghule, A.E.; Koppikar, S.J.; Bodhankar, S.L.; Chougale, A.D.; Kulkarni, M.J.; Harsulkar, A.M. Dietary flaxseed oil and fish oil modulates expression of antioxidant and inflammatory genes with alleviation of protein glycation status and inflammation in liver of streptozotocin-nicotinamide induced diabetic rats. Food Chem. 2013, 141, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Kaithwas, G.; Majumdar, D.K. In vitro antioxidant and in vivo antidiabetic, antihyperlipidemic activity of linseed oil against streptozotocin-induced toxicity in albino rats. Eur. J. Lipid. Sci. Technol. 2012, 114, 1237–1245. [Google Scholar] [CrossRef]
- Ogawa, T.; Sawane, K.; Ookoshi, K.; Kawashima, R. Supplementation with Flaxseed Oil Rich in Alpha-Linolenic Acid Improves Verbal Fluency in Healthy Older Adults. Nutrients 2023, 15, 1499. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, A.; Talei, S.; Hassanzadeh, N.; Mokhtari, T.; Akbari, M.; Malek, F.; Jameie, S.B.; Sadeghi, Y.; Hassanzadeh, G. The Neuroprotective Effects of Flaxseed Oil Supplementation on Functional Motor Recovery in a Model of Ischemic Brain Stroke: Upregulation of BDNF and GDNF. Acta Med. Iran. 2017, 55, 785–792. [Google Scholar]
- Jelinek, G.A.; Hadgkiss, E.J.; Weiland, T.J.; Pereira, N.G.; Marck, C.H.; van der Meer, D.M. Association of fish consumption and Ω3 supplementation with quality of life, disability and disease activity in an international cohort of people with multiple sclerosis. Int. J. Neurosci. 2013, 123, 792–800. [Google Scholar] [CrossRef]
- Seidita, A.; Soresi, M.; Giannitrapani, L.; Di Stefano, V.; Citarrella, R.; Mirarchi, L.; Cusimano, A.; Augello, G.; Carroccio, A.; Iovanna, J.L.; et al. The clinical impact of an extra virgin olive oil enriched mediterranean diet on metabolic syndrome: Lights and shadows of a nutraceutical approach. Front. Nutr. 2022, 9, 980429. [Google Scholar] [CrossRef]
- Conterno, L.; Martinelli, F.; Tamburini, M.; Fava, F.; Mancini, A.; Sordo, M.; Pindo, M.; Martens, S.; Masuero, D.; Vrhovsek, U.; et al. Measuring the impact of olive pomace enriched biscuits on the gut microbiota and its metabolic activity in mildly hypercholesterolaemic subjects. Eur. J. Nutr. 2019, 58, 63–81. [Google Scholar] [CrossRef]
- Prieto, I.; Hidalgo, M.; Segarra, A.B.; Martínez-Rodríguez, A.M.; Cobo, A.; Ramírez, M.; Abriouel, H.; Gálvez, A.; Martínez-Cañamero, M. Influence of a diet enriched with virgin olive oil or butter on mouse gut microbiota and its correlation to physiological and biochemical parameters related to metabolic syndrome. PLoS ONE 2018, 13, e0190368. [Google Scholar] [CrossRef]
- Liehr, M.; Mereu, A.; Pastor, J.J.; Quintela, J.C.; Staats, S.; Rimbach, G.; Ipharraguerre, I.R. Olive oil bioactives protect pigs against experimentally induced chronic inflammation independently of alterations in gut microbiota. PLoS ONE 2017, 12, e0174239. [Google Scholar] [CrossRef] [PubMed]
- Llorente-Cortés, V.; Estruch, R.; Mena, M.P.; Ros, E.; González, M.A.; Fitó, M.; Lamuela-Raventós, R.M.; Badimon, L. Effect of Mediterranean diet on the expression of pro-atherogenic genes in a population at high cardiovascular risk. Atherosclerosis 2010, 208, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Riolo, R.; De Rosa, R.; Simonetta, I.; Tuttolomondo, A. Olive Oil in the Mediterranean Diet and Its Biochemical and Molecular Effects on Cardiovascular Health through an Analysis of Genetics and Epigenetics. Int. J. Mol. Sci. 2022, 23, 16002. [Google Scholar] [CrossRef]
- Khalatbary, A.R. Olive oil phenols and neuroprotection. Nutr. Neurosci. 2013, 16, 243–249. [Google Scholar] [CrossRef]
- Lozano-Castellón, J.; López-Yerena, A.; Rinaldi de Alvarenga, J.F.; Romero Del Castillo-Alba, J.; Vallverdú-Queralt, A.; Escribano-Ferrer, E.; Lamuela-Raventós, R.M. Health-promoting properties of oleocanthal and oleacein: Two secoiridoids from extra-virgin olive oil. Crit. Rev. Food Sci. Nutr. 2020, 60, 2532–2548. [Google Scholar] [CrossRef]
- Angeloni, C.; Malaguti, M.; Barbalace, M.C.; Hrelia, S. Bioactivity of Olive Oil Phenols in Neuroprotection. Int. J. Mol. Sci. 2017, 18, 2230. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Miranda, B.; Gallardo, I.; Melliou, E.; Cabero, I.; Álvarez, Y.; Hernández, M.; Magiatis, P.; Hernández, M.; Nieto, M.L. Treatment with the Olive Secoiridoid Oleacein Protects against the Intestinal Alterations Associated with EAE. Int. J. Mol. Sci. 2023, 24, 4977. [Google Scholar] [CrossRef] [PubMed]
- Gorzynik-Debicka, M.; Przychodzen, P.; Cappello, F.; Kuban-Jankowska, A.; Marino Gammazza, A.; Knap, N.; Wozniak, M.; Gorska-Ponikowska, M. Potential Health Benefits of Olive Oil and Plant Polyphenols. Int. J. Mol. Sci. 2018, 19, 686. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Christoph, M.; Hoffmann, G. Effects of Olive Oil on Markers of Inflammation and Endothelial Function-A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 7651–7675. [Google Scholar] [CrossRef]
- Carito, V.; Ceccanti, M.; Tarani, L.; Ferraguti, G.; Chaldakov, G.N.; Fiore, M. Neurotrophins’ Modulation by Olive Polyphenols. Curr. Med. Chem. 2016, 23, 3189–3197. [Google Scholar] [CrossRef] [PubMed]
- Jongen, P.J.; Ter Horst, A.T.; Brands, A.M. Cognitive impairment in multiple sclerosis. Minerva Med. 2012, 103, 73–96. [Google Scholar] [PubMed]
- Chatzikostopoulos, T.; Tsolaki, M.; Wozniak, G.; Basgiouraki, E.; Saoulidis, I.; Michmizos, D.; Koutsouraki, E. The Effects of Early-Harvest Extra Virgin Olive Oil on Cognition and Mental Health of Primary (PPMS) or Secondary (SPMS) Progressive Multiple Sclerosis Patients. Glob. J. Med. Res. 2022, 22, RC455.4.L67. [Google Scholar]
- Berr, C.; Portet, F.; Carriere, I.; Akbaraly, T.N.; Feart, C.; Gourlet, V.; Combe, N.; Barberger-Gateau, P.; Ritchie, K. Olive oil and cognition: Results from the three-city study. Dement. Geriatr. Cogn. Disord. 2009, 28, 357–364. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y.; Tang, M.X.; Mayeux, R.; Luchsinger, J.A. Mediterranean diet and risk for Alzheimer’s disease. Ann. Neurol. 2006, 59, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Kostas, A.; Siakavellas, S.I.; Kosmidis, C.; Takou, A.; Nikou, J.; Maropoulos, G.; Vlachogiannakos, J.; Papatheodoridis, G.V.; Papaconstantinou, I.; Bamias, G. Fecal calprotectin measurement is a marker of short-term clinical outcome and presence of mucosal healing in patients with inflammatory bowel disease. World J. Gastroenterol. 2017, 23, 7387–7396. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, G.; Kyprou, M.; Tsolaki, M. The Effect of Cretan High Phenolic Olive Oil on Fecal Calprotectin Levels in the Course of Multiple Sclerosis. EC Neurol. 2020, 12, 65–79. [Google Scholar]
- Adamczyk-Sowa, M.; Galiniak, S.; Żyracka, E.; Grzesik, M.; Naparło, K.; Sowa, P.; Bartosz, G.; Sadowska-Bartosz, I. Oxidative Modification of Blood Serum Proteins in Multiple Sclerosis after Interferon Beta and Melatonin Treatment. Oxid. Med. Cell. Longev. 2017, 7905148. [Google Scholar] [CrossRef]
- Escribano, B.M.; Medina-Fernández, F.J.; Aguilar-Luque, M.; Agüera, E.; Feijoo, M.; Garcia-Maceira, F.I.; Lillo, R.; Vieyra-Reyes, P.; Giraldo, A.I.; Luque, E.; et al. Lipopolysaccharide Binding Protein and Oxidative Stress in a Multiple Sclerosis Model. Neurotherapeutics 2017, 14, 199–211. [Google Scholar] [CrossRef]
- Conde, C.; Escribano, B.M.; Luque, E.; Feijóo, M.; Caballero-Villarraso, J.; Valdelvira, M.E.; Ochoa-Sepúlveda, J.J.; Lillo, R.; Paz, E.; Santamaría, A.; et al. Extra-Virgin Olive Oil Modifies the Changes Induced in Non-Nervous Organs and Tissues by Experimental Autoimmune Encephalomyelitis Models. Nutrients 2019, 11, 2448. [Google Scholar] [CrossRef]
- Stojanović, I.; Šavikin, K.; Đedović, N.; Živković, J.; Saksida, T.; Momčilović, M.; Koprivica, I.; Vujičić, M.; Stanisavljević, S.; Miljković, Đ.; et al. Pomegranate peel extract ameliorates autoimmunity in animal models of multiple sclerosis and type 1 diabetes. J. Funct. Foods 2017, 35, 522–530. [Google Scholar] [CrossRef]
- Rafiee, S.; Faryabi, R.; Yargholi, A.; Zareian, M.A.; Hawkins, J.; Shivappa, N.; Shirbeigi, L. Effects of Sesame Consumption on Inflammatory Biomarkers in Humans: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid. Based Complement. Altern. Med. eCAM 2021, 2021, 6622981. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Plant Oil | Authors (Country) | Design of Study | Dosage | Duration of Study | Effects | Possible Mechanisms of Action and Principle Active Compounds |
|---|---|---|---|---|---|---|
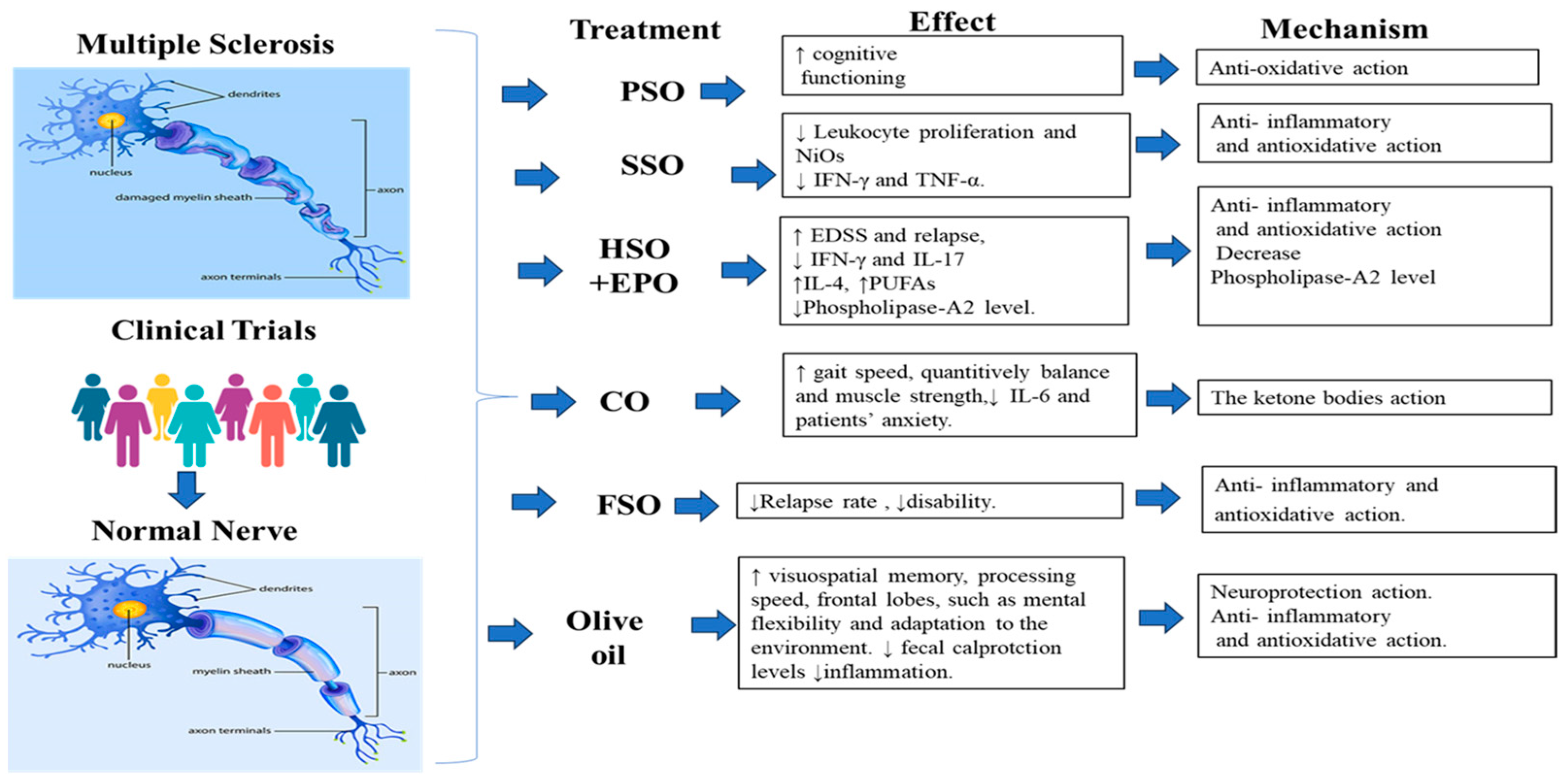
| Pomegranate Seed Oil (PSO) | Petrou et al. [45] (Jerusalem) | Clinical trial with 30 MS patients, placebo pills containing soybean oil then additional PSO | Not mentioned | 9 months | ↑ cognitive functioning | Anti-oxidative action of PSO nanoemulsion and its main active ingredient punicic acid |
| Sesame seed oil (SSO) | Faraji et al. [62] (Iran) | Clinical trial, control treated with 30 μg/week. | 30 μg/week of interferon beta-1a + 0.5 mL/kg/day of oral sesame oil | 6 months | ↓ Leukocyte proliferation and Nitric oxide ↓ IFN-γ and TNF-α | Anti- inflammatory and antioxidative action |
| Hemp seed oil and Evening primrose oil (HSO + EPO) | Majdinasab et al. [94] (Iran) | Clinical trial with 52 MS patients, with placebo Control | 3 Months | Antioxidants and Inflammatory action. | ||
| Rezapour-Firouzi et al., [96] (Iran) | Clinical trial, Placebo control of olive oil Each group has 20 patients. | 6 Months | ↑ Clinical improvements in expended disability status scale and relapse rate in MS Also, ↓ pro-inflammatory cytokines IL-17. | Antioxidant activity Inflammatory functions and cytokines production | ||
| Rezapour-Firouzi et al., [97] (Iran) | Clinical trial, Placebo control of olive oil Each group has 23 patients. | 1 g oral capsule containing EPO every 12 h for 3 months. | 6 Months | ↑ in red blood cells PUFAs and ↓ Phospholipase-A2 level. | Decrease Phospholipase-A2 level. | |
| Rezapour-Firouzi et al., [98] (Iran) | Clinical trial, Placebo control of olive oil Each group has 23 patients. | A combination of HSO and EPO with 9/1 ratio AT 18–21 g/day (6–7 g, three times daily) | 6 Months | ↑ extended disability status score. | ||
| Rezapour-Firouzi et al., [87] (Iran) | Clinical trial, Placebo control of olive oil Each group has 20 patients. | A combination of HSO and EPO with 9/1 ratio AT 18–21 g/day (6–7 g, three times daily) | 6 Months | ↓ Pro-inflammatory cytokines of IFN-γ and IL-17 and ↑IL-4. | ↓ Pro-inflammatory and ↑ in anti-inflammatory cytokines. | |
| Coconut oil (CO) | Cuerda-Ballester et al., [109] (Spain) | Clinical trial of 27 MS patients, Placebo Control of 26 patients. | 60 mL of extra virgin CO supplemented with EGCG. | 4-month | ↑ improvement in gait speed, quantitively balance and muscle strength. | The ketone bodies that may formed from EVCO metabolism balance. |
| Platero et al., [115] (Spain) | Clinical trial of 24 MS patients and with Placebo Control of 27 patients. | 60 mL of extra virgin coconut oil supplemented with epigallocatechin gallate (EGCG)at 800 mg. | 4 Months | ↓ in serum concentration of IL-6 and patients’ anxiety. ↑ Improvement in patients’ functionality. | The ketone bodies that may formed from CO metabolism balance. | |
| Flaxseed oil (FSO) | Jelinek et al., [130] (Australia) | Surveyed study with MS patients through Web 2.0 platforms, including social media. | last 12 months. | A large cohort of 2469 people with MS disease | ↓ Relapse rate was seen at large level (over 52%) for those MS patients who are taking FSO in univariate analysis. ↓ of disability. | anti-inflammatory and antioxidant action of PUFAs |
| Olive oil | Chatzikostopoulos et al. [146] (Greece) | Clinical trials With 30 MS patient 20 for intervention and 10 controls | Three tablespoons of EVOO/day | 6 Months to one year | ↑ Improvement visuospatial memory, processing speed and improvement in functions related to the frontal lobes, such as mental flexibility and adaptation to the environment when compared to control patients. | Neuroprotection action. |
| Greta Wozniak et al. [150] (Cyprus) | Clinical trials with RRMS patients 10 patients for treatment and 5 patients as control. | 50 mL of EVOO/day, Control patients did not take any oil. | 2–4 months | ↓ Reduction in fecal calprotectin levels after 2 and 4 months of administration, ↓ inflammation in the treated group. | ↓ Inflammation by decreasing the fecal calprotectin due to the presence of t polyphenols in the oil. |
| Plant Oil | Author (Country) Reference Number | Design of Study | Dosage | Duration of Study | Effects | Possible Mechanisms of Action and Principle Active Compounds |
|---|---|---|---|---|---|---|
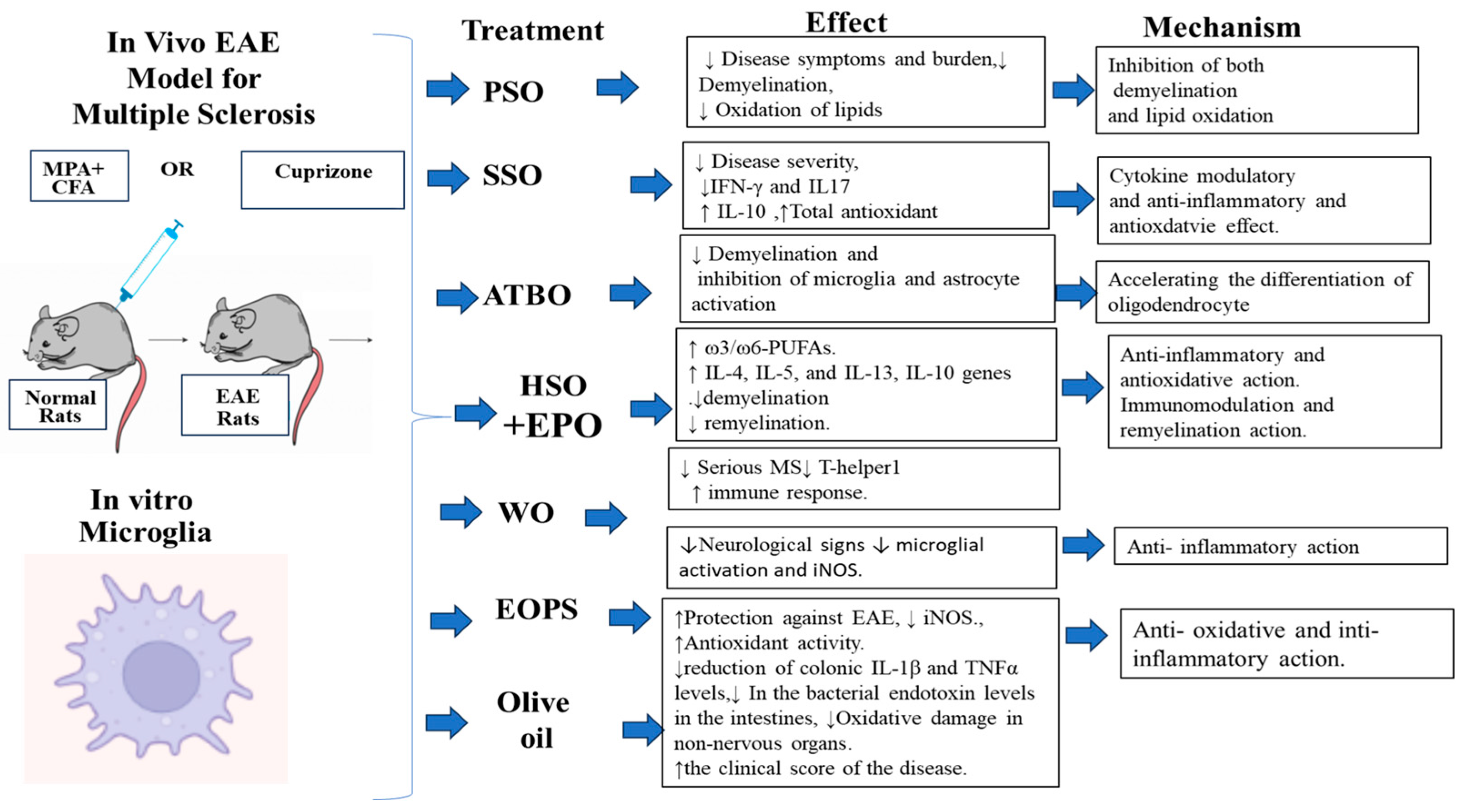
| Pomegranate Seed Oil (PSO) | Binyamin et al. [52] (Jerusalem) | EAE model of MS in female mice | PSO as nanoemulsion by gavage and PSO with diet at 25 or 75 mL/kg of the diet. | 10 days | ↓ Disease symptoms and burden, ↓ Demyelination, ↓ Oxidation of lipids in the brains of EAE mice. | Inhibition of both demyelination and lipid oxidation |
| Sesame seed oil (SSO) | Javan et al., [68] (Iran) | EAE model of MS in female mice | 4 mL/kg/day) injected intraperitoneally. Control was injected with 4 mL phosphate buffer intraperitoneally. | 20 days | ↓ Disease severity, ↓ IFN-γ and IL17 ↑ IL-10 | Cytokine modulatory and anti-inflammatory effect. |
| Mosayebi, et al., [71] (Iran) | EAE model of MS in male mice | 4 mL/kg/day) injected intraperitoneally (10 mice). | 25 days | ↓ Clinical symptoms of EAE, ↑ Total antioxidant capacity. | Inhibition of oxidative stress | |
| Acer truncatum Bunge seed oil (ATBO) | Xue et al., [77] (China) | Cuprizone induced mice as a MS model | 4% ATBO of the diet. | 2 Weeks | ↓ Demyelination and inhibition of microglia and astrocyte activation in vitro. | Accelerating the differentiation of oligodendrocyte precursor cells to mature oligodendrocytes in vitro. |
| Hemp seed oil and Evening primrose oil (HSO + EPO) | Rezapour -Firouzi et al., [89] (Iran) | EAE model of MS in female mice | Oral EPO/HSO (50 λ/mouse) | 2 weeks | ↑ The percentage of essential fatty acids and ω3/ω6-PUFAs. ↑ The expression levels of IL-4, IL-5 and IL-13 genes No demyelination in the brain and spinal cord sections of the EPO/HSO treated mice. | Antioxidants and PUFAs presented in both oils are the responsible compounds for the effect through anti-inflammatory and antioxidative action. |
| Rezapour-Firouzi et al., [92] (Iran) | EAE model of MS in female mice | A combination of HSO and EPO at λ/mouse | 28 days after | ↓ of MS diseases in EAE. ↑ the expression of IL-10 gene, ↓ cell infiltration and promote remyelination. | Immunomodulation and remyelination activities. | |
| Walnut oil (WO) | Ganji et al., [118] (Iran) | EAE model of MS in female mice | Gavage daily with 5 mL of WO/kg b.w phosphate buffered saline. | 21 days | ↓ Serious MS Sickness, ↓ T-helper1 activity and ↑ improvement of immune response | Anti-inflammatory mechanisms |
| Essential oil from Pterodon emarginatus seeds (EOPS) | Alberti et al., [124] (Brazil) | EAE model of MS in mice and in vitro using microglia macrophages cells of the central nervous system | Oral treatment of E0PS dissolved in Tween 80 and 0.9% NaCl at 50–100 mg/kg. | 25 days | ↓ Neurological signs and the development of MS diseases in EAE animals ↓ microglial activation and expression of iNOS. | Inhibition of microglial activation and reduce the expression of pro-inflammatory mediators and reduce the oxidative stress. |
| Olive Oil | Gutiérrez-Miranda et al., [141] (Greece) | EAE model of MS in female mice | Treated mice with olive oil were injected intraperitoneally With 10 mg/kg/day | 24 days | ↑Protection against EAE ↓ superoxide anion and lipid oxidation products in colon, ↑ Antioxidant activity. ↓ reduction in colonic IL-1 β and TNFα levels. | Anti-oxidative and inti-inflammatory mechanisms. |
| Conde et al. [151] (Spain) | EAE model of MS in rats | 10% of the calorie intake (in terms of weight) is EVOO with a gastric catheter. | 51 days | ↓ In the bacterial endotoxin levels in the intestines, ↓ Oxidative damage in non-nervous organs. ↑ the clinical score of the disease. | Anti-oxidative damage. in the EAE model |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Naqeb, G.; Kalmpourtzidou, A.; De Giuseppe, R.; Cena, H. Beneficial Effects of Plant Oils Supplementation on Multiple Sclerosis: A Comprehensive Review of Clinical and Experimental Studies. Nutrients 2023, 15, 4827. https://doi.org/10.3390/nu15224827
Al-Naqeb G, Kalmpourtzidou A, De Giuseppe R, Cena H. Beneficial Effects of Plant Oils Supplementation on Multiple Sclerosis: A Comprehensive Review of Clinical and Experimental Studies. Nutrients. 2023; 15(22):4827. https://doi.org/10.3390/nu15224827
Chicago/Turabian StyleAl-Naqeb, Ghanya, Aliki Kalmpourtzidou, Rachele De Giuseppe, and Hellas Cena. 2023. "Beneficial Effects of Plant Oils Supplementation on Multiple Sclerosis: A Comprehensive Review of Clinical and Experimental Studies" Nutrients 15, no. 22: 4827. https://doi.org/10.3390/nu15224827
APA StyleAl-Naqeb, G., Kalmpourtzidou, A., De Giuseppe, R., & Cena, H. (2023). Beneficial Effects of Plant Oils Supplementation on Multiple Sclerosis: A Comprehensive Review of Clinical and Experimental Studies. Nutrients, 15(22), 4827. https://doi.org/10.3390/nu15224827